
An Endoscope Image Enhancement Algorithm Based on Image Decomposition

Abstract
:1. Introduction
2. Dataset Introduction
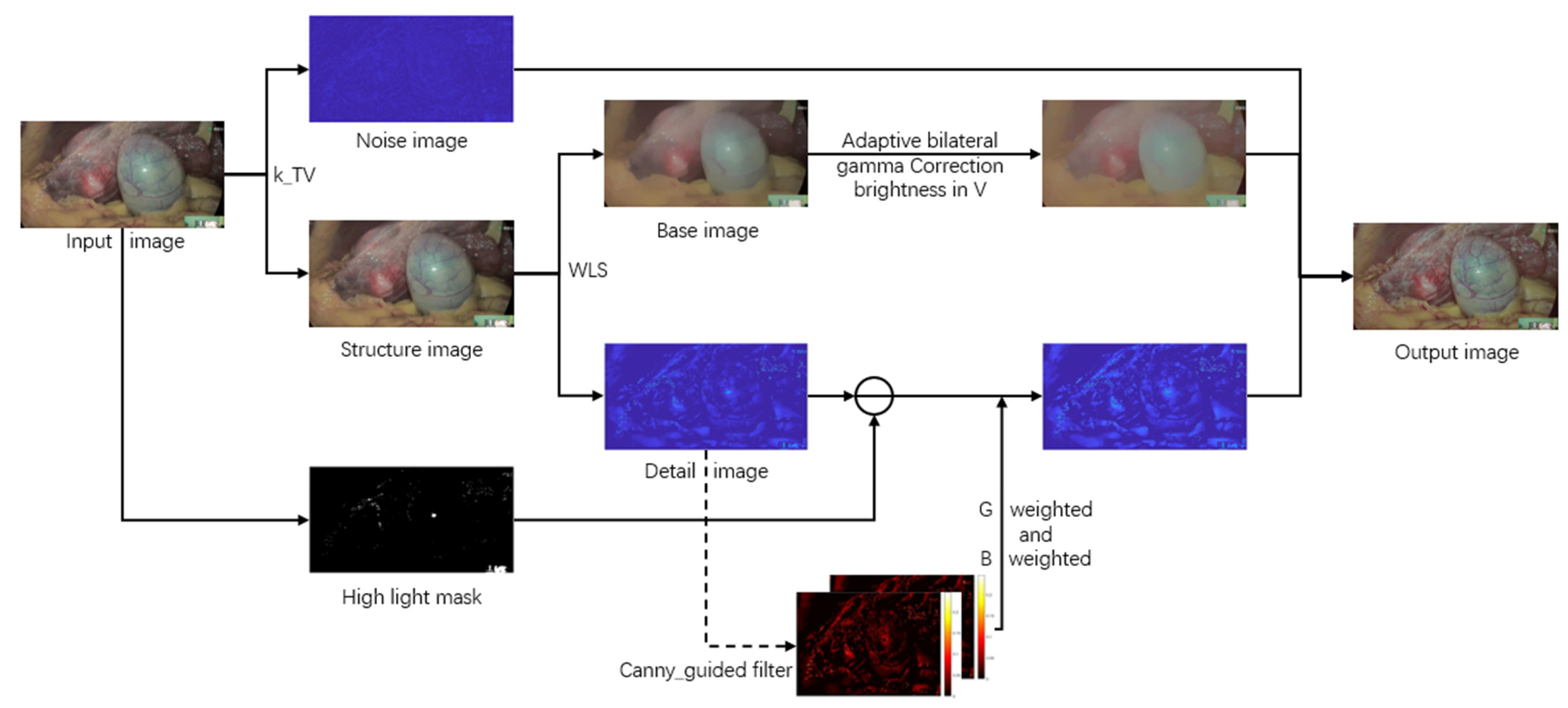
3. Proposed Algorithm
3.1. Modified Total-Variation to Extract the Noise Layer
3.2. Weighted Least Squares Decomposition of Images
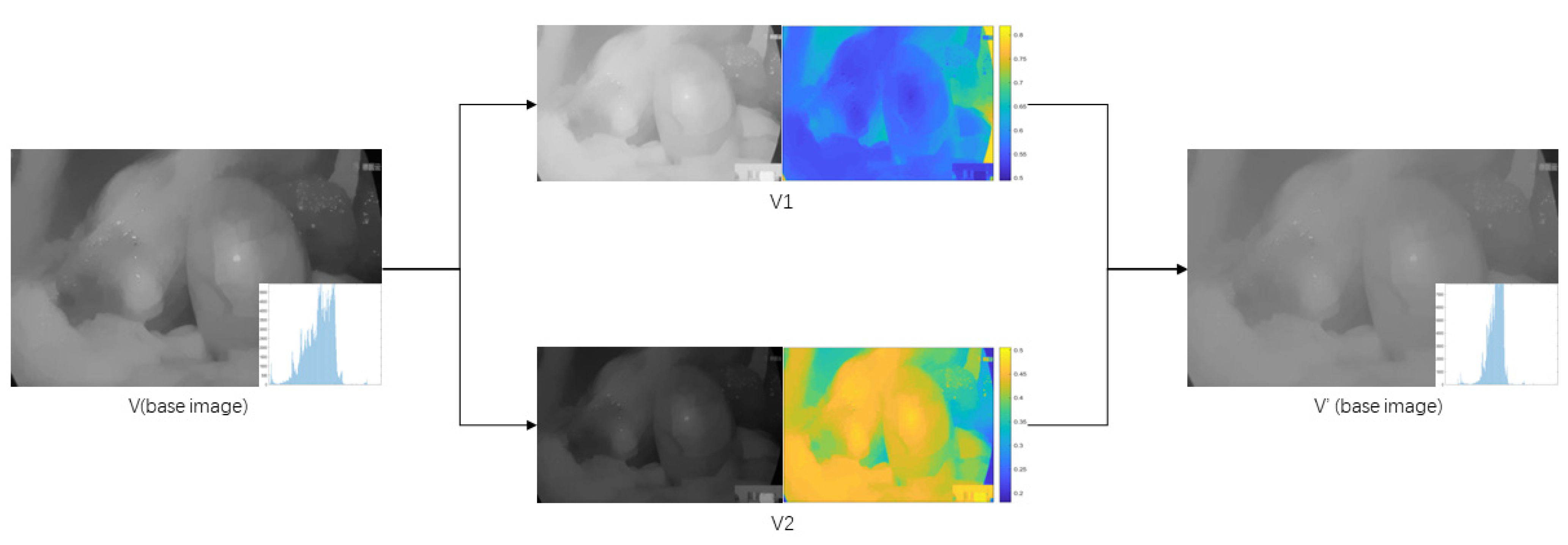
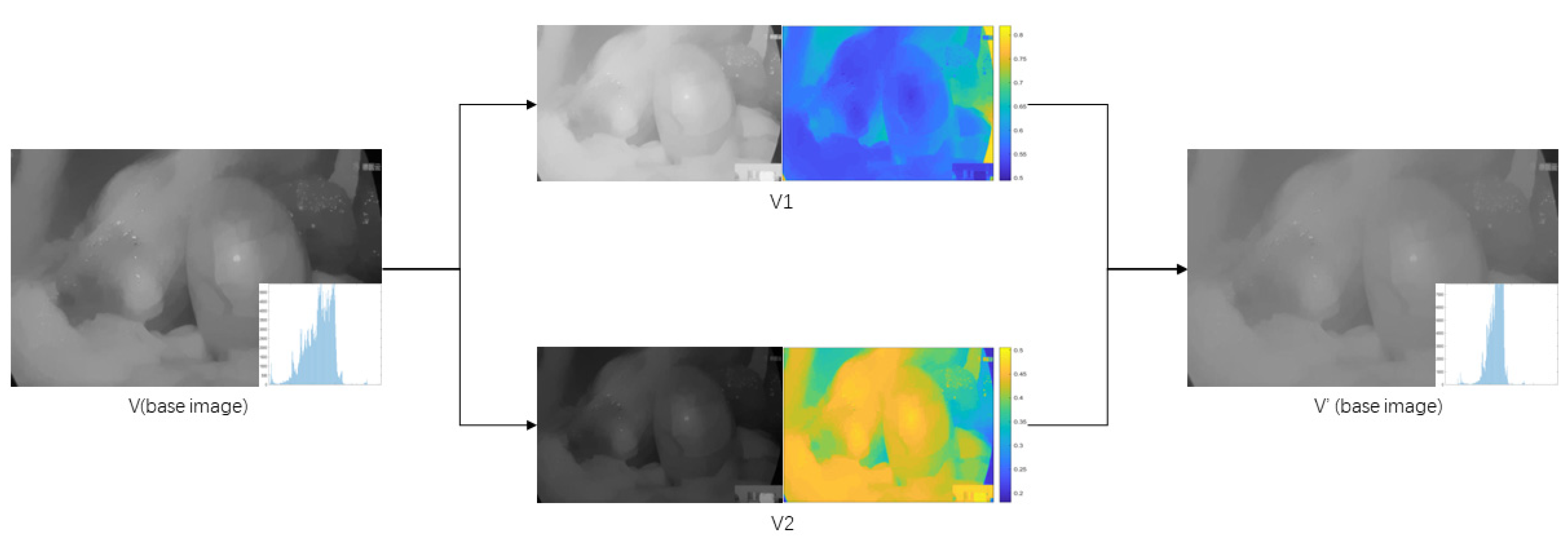
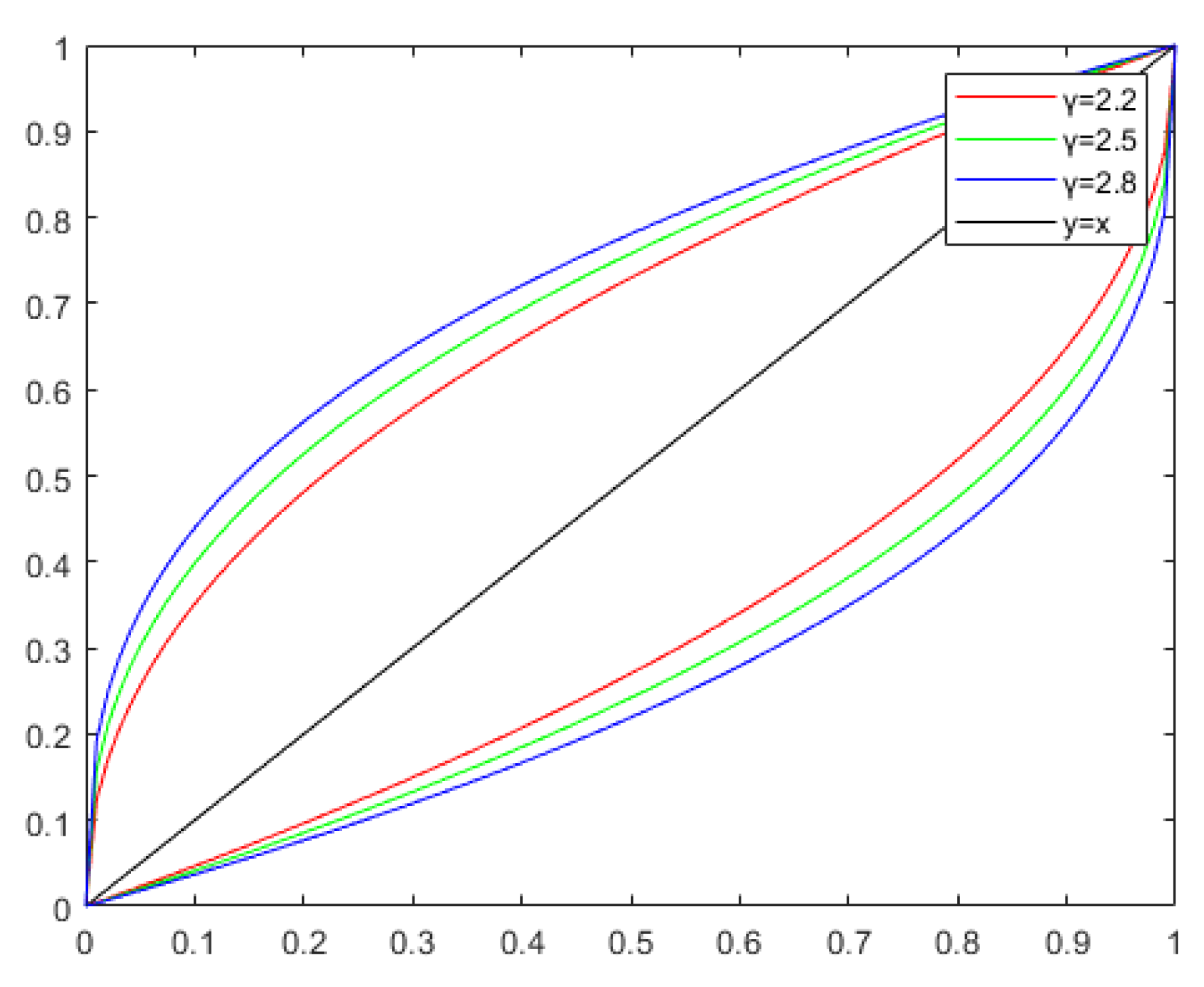
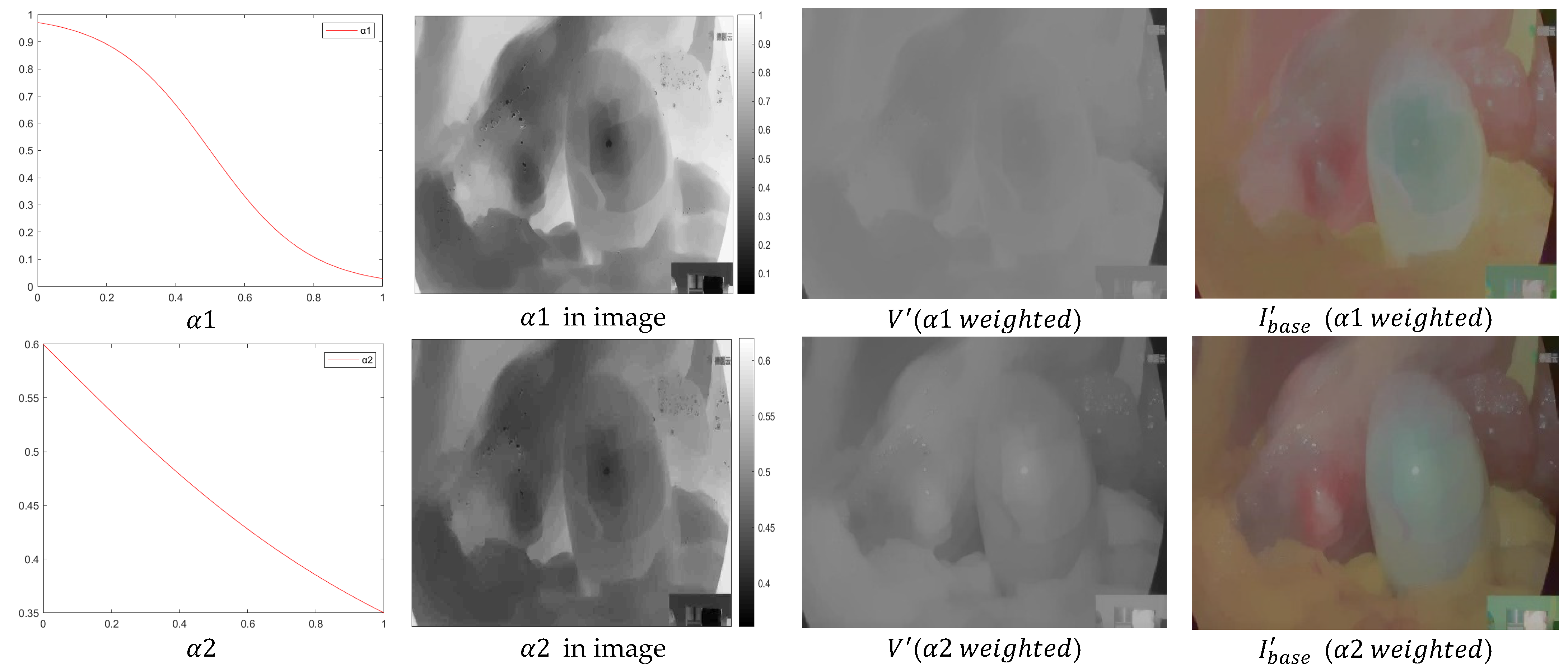
3.3. Adaptive Bilateral Gamma Correction Brightness
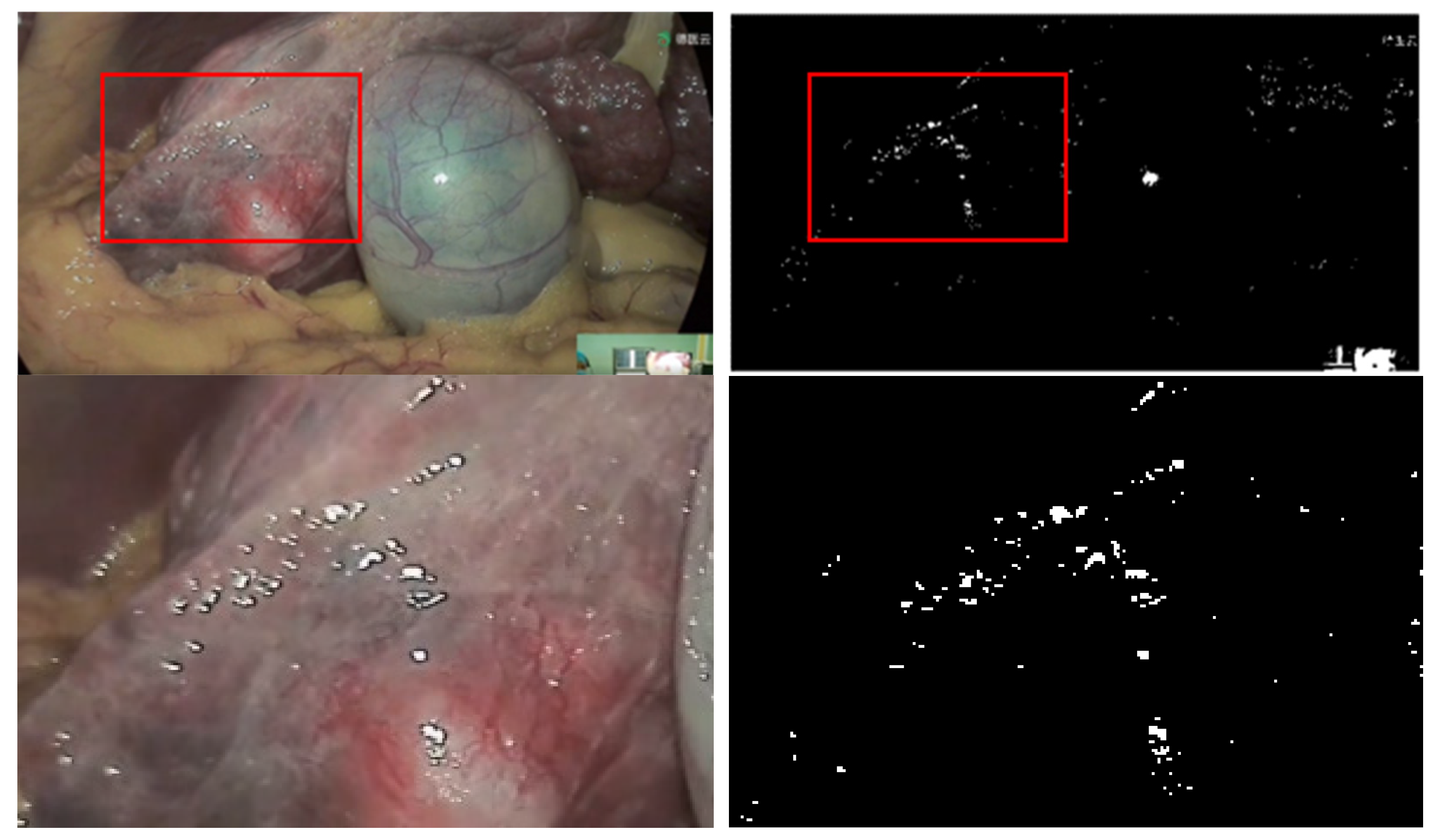
3.4. Highlight Detail Layer Information
4. Experimental Analysis
4.1. Experimental Environment
4.2. Parameter Setting
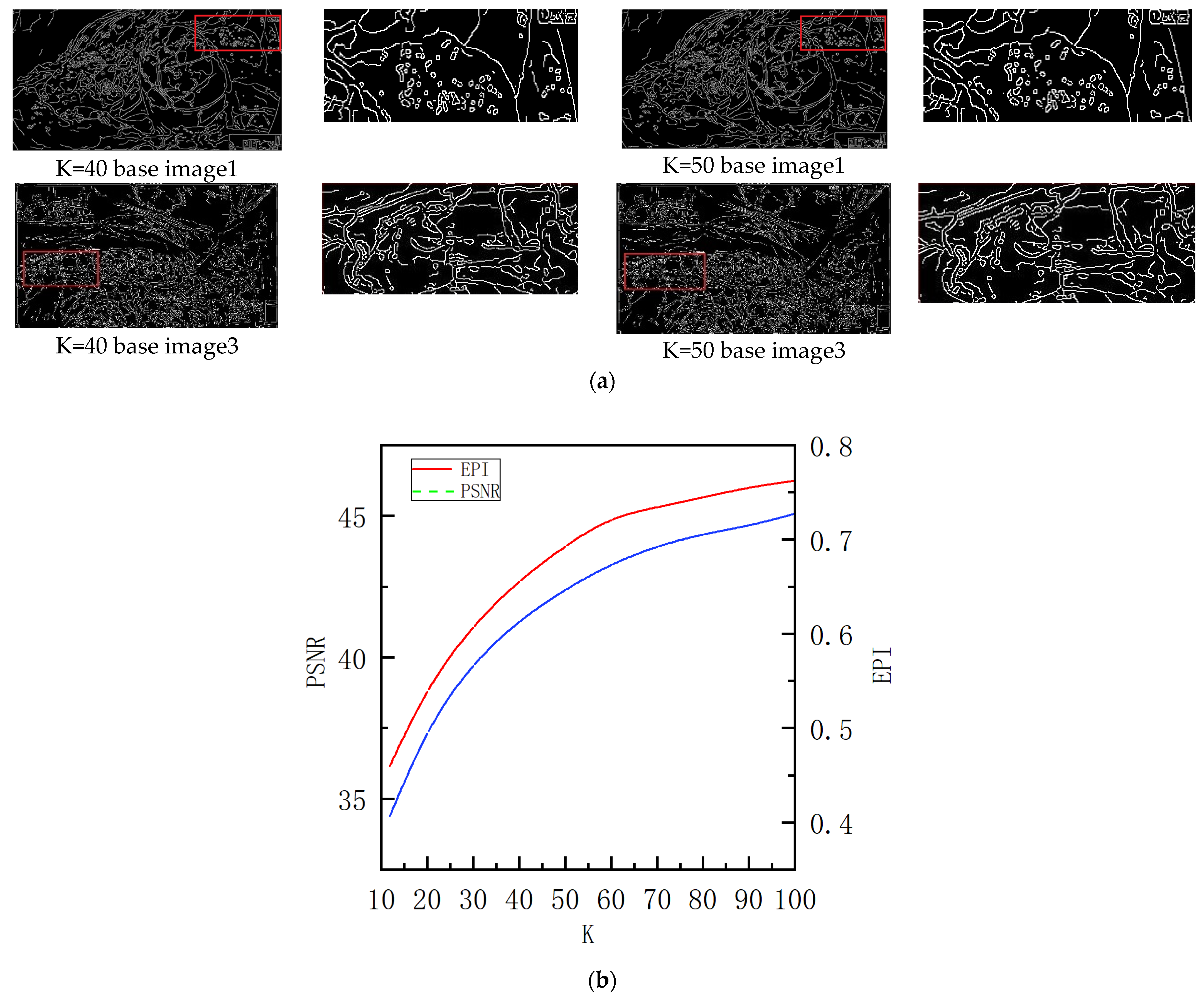
4.2.1. Noise Rejection Factor k
4.2.2. Setting of Parameter φ in Brightness Correction
4.3. Subjective and Objective Analysis
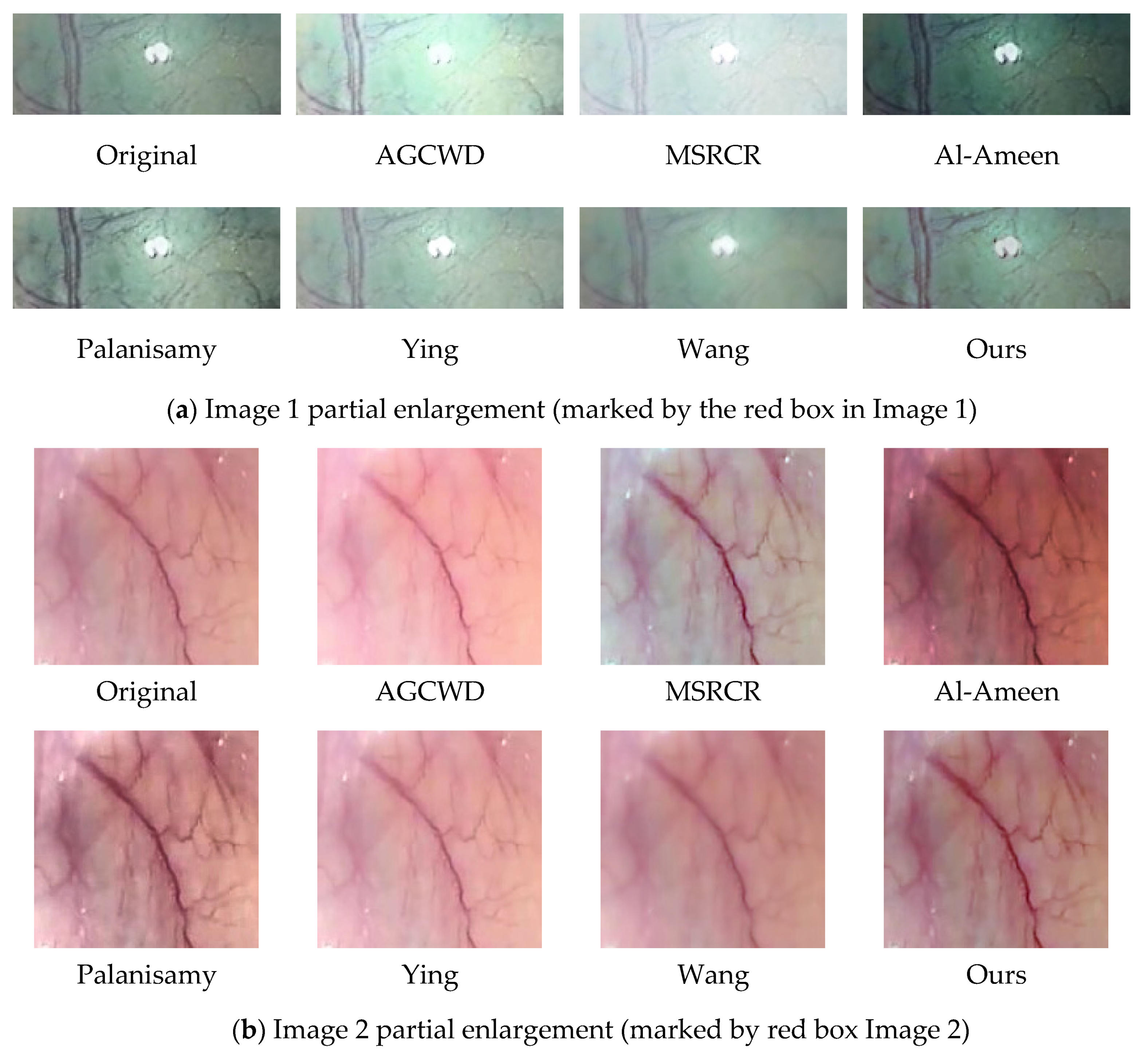
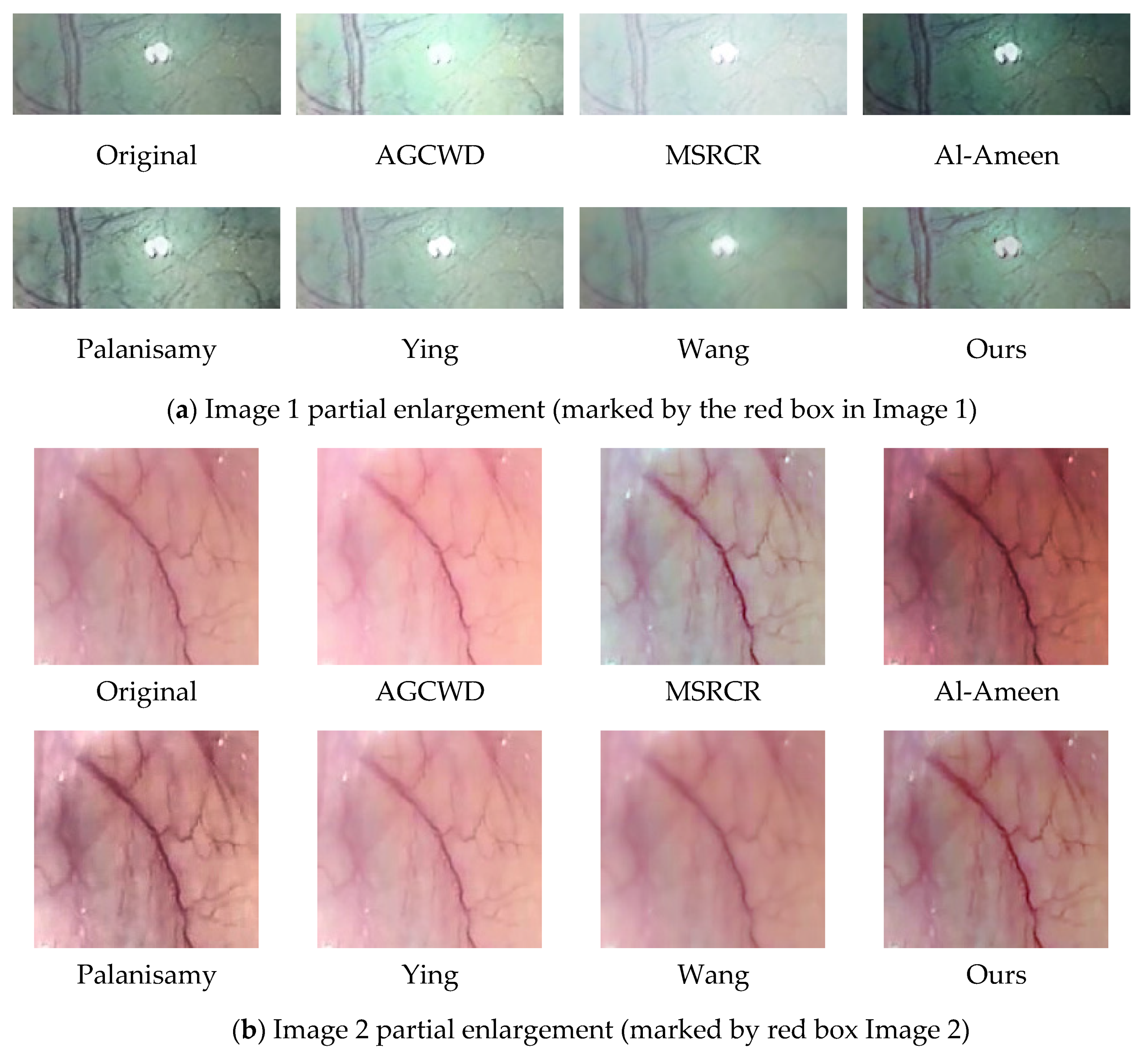
4.3.1. Subjective Analysis
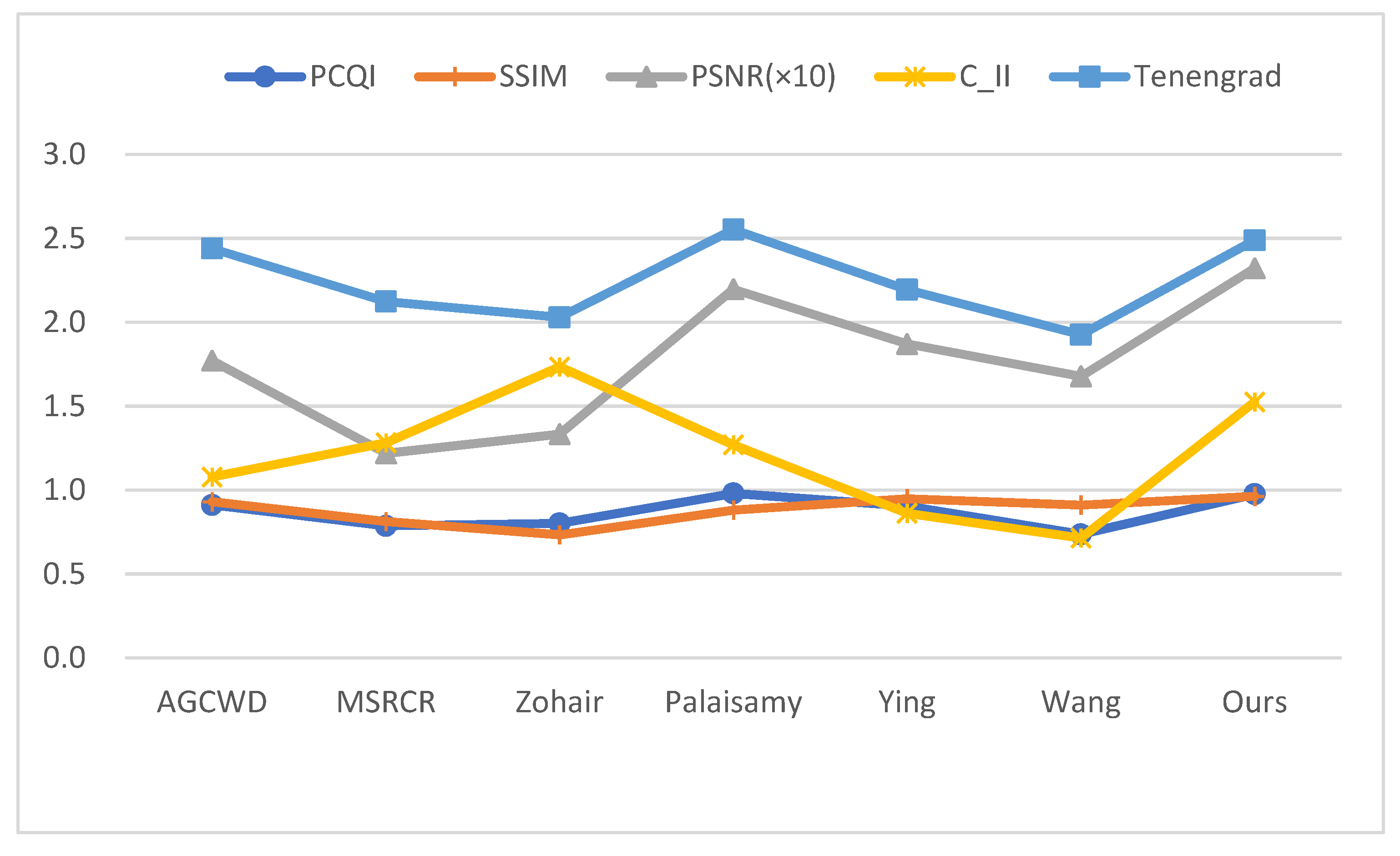
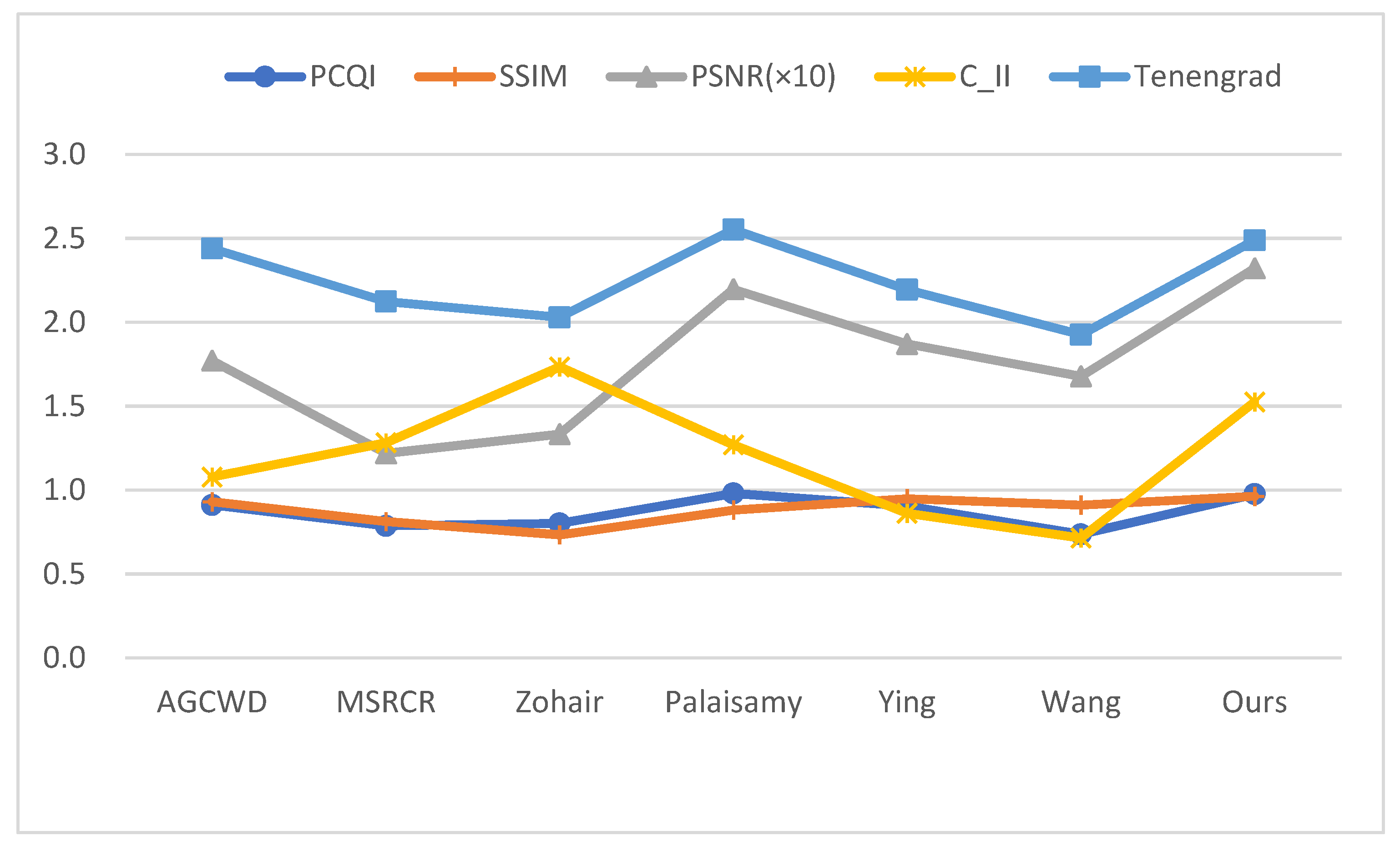
4.3.2. Objective Analysis
5. Discussion
5.1. Effectiveness
5.2. Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Nguyen, K.T.; Hoang, M.C.; Choi, E.; Kang, B.; Park, J.-O.; Kim, C.-S. Medical microrobot—A drug delivery capsule endoscope with active locomotion and drug release mechanism: Proof of concept. Int. J. Control Autom. Syst. 2020, 18, 65–75. [Google Scholar] [CrossRef]
- Lee, S.; Lee, H.; Choi, H.; Jeon, S.; Hong, J.J. Effective calibration of an endoscope to an optical tracking system for medical augmented reality. Cogent Eng. 2017, 4, 1359955. [Google Scholar] [CrossRef]
- Monkam, P.; Wu, J.; Lu, W.; Shan, W.; Chen, H.; Zhai, Y.J. EasySpec: Automatic Specular Reflection Detection and Suppression from Endoscopic Images. IEEE Trans. Comput. Imaging 2021, 7, 1031–1043. [Google Scholar] [CrossRef]
- Wang, L.; Wu, B.; Wang, X.; Zhu, Q.; Xu, K.J.T. Endoscopic image luminance enhancement based on the inverse square law for illuminance and retinex. Int. J. Med. Robot. Comput. Assist. Surg. 2022, e2396. [Google Scholar] [CrossRef] [PubMed]
- Sato, T.J. TXI: Texture and color enhancement imaging for endoscopic image enhancement. J. Healthc. Eng. 2021, 2021, 5518948. [Google Scholar] [CrossRef]
- Yao, M.; Zhu, C. Study and comparison on histogram-based local image enhancement methods. In Proceedings of the 2017 2nd International Conference on Image, Vision and Computing (ICIVC), Chengdu, China, 2–4 June 2017; pp. 309–314. [Google Scholar]
- Meylan, L.; Susstrunk, S.J. High dynamic range image rendering with a retinex-based adaptive filter. IEEE Trans. Image Processing 2006, 15, 2820–2830. [Google Scholar] [CrossRef] [Green Version]
- Huang, S.-C.; Cheng, F.-C.; Chiu, Y.-S.J. Efficient contrast enhancement using adaptive gamma correction with weighting distribution. IEEE Trans. Image Processing 2012, 22, 1032–1041. [Google Scholar] [CrossRef]
- Jobson, D.J.; Rahman, Z.-U.; Woodell, G.A.J. A multiscale retinex for bridging the gap between color images and the human observation of scenes. IEEE Trans. Image Processing 1997, 6, 965–976. [Google Scholar] [CrossRef] [Green Version]
- Xu, F.; Liu, J.; Song, Y.; Sun, H.; Wang, X.J. Multi-Exposure Image Fusion Techniques: A Comprehensive Review. Remote Sens. 2022, 14, 771. [Google Scholar] [CrossRef]
- Hayat, N.; Imran, M.J. Multi-exposure image fusion technique using multi-resolution blending. IET Image Process. 2019, 13, 2554–2561. [Google Scholar] [CrossRef]
- Ying, Z.; Li, G.; Ren, Y.; Wang, R.; Wang, W. A new image contrast enhancement algorithm using exposure fusion framework. In Proceedings of the International Conference on Computer Analysis of Images and Patterns, Ystad, Sweden, 22–24 August 2017; pp. 36–46. [Google Scholar]
- Kaur, M.; Kaur, J.; Kaur, J.J. Applications. Survey of contrast enhancement techniques based on histogram equalization. Int. J. Adv. Comput. Sci. Appl. 2011, 2, 137–141. [Google Scholar]
- Zuiderveld, K. Contrast limited adaptive histogram equalization. In Graphics Gems IV; Academic Press: Cambridge, MA, USA, 1994; pp. 474–485. [Google Scholar]
- Chang, Y.T.; Wang, J.T.; Yang, W.H.; Chen, X.W. Contrast enhancement in palm bone image using quad-histogram equalization. In Proceedings of the 2014 International Symposium on Computer, Consumer and Control, Taichung, Taiwan, 10–12 June 2014; pp. 1091–1094. [Google Scholar]
- Al-Ameen, Z.; Sulong, G.J. A new algorithm for improving the low contrast of computed tomography images using tuned brightness controlled single-scale Retinex. Scanning 2015, 37, 116–125. [Google Scholar] [CrossRef] [PubMed]
- Palanisamy, G.; Ponnusamy, P.; Gopi, V.P. An improved luminosity and contrast enhancement framework for feature preservation in color fundus images. Signal Image Video Process. 2019, 13, 719–726. [Google Scholar] [CrossRef]
- Obukhova, N.; Motyko, A.; Pozdeev, A.; Timofeev, B. Review of Noise Reduction Methods and Estimation of their Effectiveness for Medical Endoscopic Images Processing. In Proceedings of the 2018 22nd Conference of Open Innovations Association (FRUCT), Jyväskylä, Finland, 15–18 May 2018; pp. 204–210. [Google Scholar]
- Tai, S.-C.; Yang, S.-M. A fast method for image noise estimation using laplacian operator and adaptive edge detection. In Proceedings of the 2008 3rd International Symposium on Communications, Control and Signal Processing, St Julian’s, Malta, 12–14 March 2008; pp. 1077–1081. [Google Scholar]
- Immerkaer, J. Fast noise variance estimation. Comput. Vis. Image Underst. 1996, 64, 300–302. [Google Scholar] [CrossRef]
- Aujol, J.-F.; Gilboa, G.; Chan, T.; Osher, S.J. Structure-texture image decomposition—Modeling, algorithms, and parameter selection. Int. J. Comput. Vis. 2006, 67, 111–136. [Google Scholar] [CrossRef]
- Farbman, Z.; Fattal, R.; Lischinski, D.; Szeliski, R.J.A. Edge-preserving decompositions for multi-scale tone and detail manipulation. ACM Trans. Graph. 2008, 27, 1–10. [Google Scholar] [CrossRef]
- Rezazadeh, S.; Coulombe, S. A novel discrete wavelet transform framework for full reference image quality assessment. Signal Image Video Process. 2013, 7, 559–573. [Google Scholar] [CrossRef]
- Wang, Z.; Bovik, A.C.; Sheikh, H.R.; Simoncelli, E.P.J.I. Image quality assessment: From error visibility to structural similarity. IEEE Trans. Image Process. 2004, 13, 600–612. [Google Scholar] [CrossRef] [Green Version]
- El Meslouhi, O.; Kardouchi, M.; Allali, H.; Gadi, T.; Benkaddour, Y.A.J. Automatic detection and inpainting of specular reflections for colposcopic images. Cent. Eur. J. Comput. Sci. 2011, 1, 341–354. [Google Scholar] [CrossRef]
- Hongpeng, J.; Kejian, Z.; Bo, Y.; Liqiang, W.J. A vascular enhancement algorithm for endoscope image. Opto-Electron. Eng. 2019, 46, 180167-1–180167-9. [Google Scholar]
- Duch, W. Filter methods. In Feature Extraction; Springer: Berlin/Heidelberg, Germany, 2006; pp. 89–117. [Google Scholar]
- Canny, J. A computational approach to edge detection. IEEE Trans. Pattern Anal. Mach. Intell. 1986, 6, 679–698. [Google Scholar] [CrossRef]
- Joseph, J.; Jayaraman, S.; Periyasamy, R.; V. Renuka, S. An edge preservation index for evaluating nonlinear spatial restoration in MR images. Curr. Med. Imaging 2017, 13, 58–65. [Google Scholar] [CrossRef]
- Wang, S.; Ma, K.; Yeganeh, H.; Wang, Z.; Lin, W.J. A patch-structure representation method for quality assessment of contrast changed images. IEEE Signal Process. Lett. 2015, 22, 2387–2390. [Google Scholar] [CrossRef]
- Shin, J.; Park, R.-H.J. Histogram-based locality-preserving contrast enhancement. IEEE Signal Process. Lett. 2015, 22, 1293–1296. [Google Scholar] [CrossRef]
- Huang, W.; Jing, Z.J. Evaluation of focus measures in multi-focus image fusion. Pattern Recognit. Lett. 2007, 28, 493–500. [Google Scholar] [CrossRef]
- Xiong, L.; Li, H.; Xu, L.J. An enhancement method for color retinal images based on image formation model. Comput. Methods Programs Biomed. 2017, 143, 137–150. [Google Scholar] [CrossRef]
- Tang, C.-P.; Hsieh, C.-H.; Lin, T.-L.J. Computer-Aided Image Enhanced Endoscopy Automated System to Boost Polyp and Adenoma Detection Accuracy. Diagnostics 2022, 12, 968. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Methods | Image | PCQI | SSIM | PSNR | C_II | Tenengrad |
|---|---|---|---|---|---|---|
| AGCWD | Im1 | 0.98 | 0.87 | 14.06 | 1.18 | 3.37 |
| Im2 | 0.88 | 0.96 | 18.94 | 1.03 | 1.06 | |
| Im3 | 0.94 | 0.94 | 18.49 | 1.07 | 2.89 | |
| Ave | 0.91 | 0.93 | 17.72 | 1.08 | 2.44 | |
| MSRCR | Im1 | 0.63 | 0.72 | 7.83 | 0.71 | 2.37 |
| Im2 | 1.01 | 0.88 | 17.14 | 2.16 | 1.70 | |
| Im3 | 0.68 | 0.83 | 11.06 | 0.91 | 2.29 | |
| Ave | 0.79 | 0.81 | 12.20 | 1.28 | 2.12 | |
| Al-Ameen | Im1 | 0.75 | 0.71 | 14.01 | 1.82 | 2.43 |
| Im2 | 0.81 | 0.75 | 12.73 | 2.06 | 1.20 | |
| Im3 | 0.78 | 0.75 | 12.97 | 1.58 | 2.45 | |
| Ave | 0.80 | 0.73 | 13.34 | 1.74 | 2.03 | |
| Palanisamy | Im1 | 1.10 | 0.89 | 23.10 | 1.26 | 4.15 |
| Im2 | 1.10 | 0.90 | 20.93 | 1.56 | 1.70 | |
| Im3 | 0.61 | 0.78 | 12.48 | 0.75 | 2.70 | |
| Ave | 0.99 | 0.88 | 21.97 | 1.27 | 2.55 | |
| Ying | Im1 | 0.90 | 0.93 | 17.23 | 0.83 | 2.87 |
| Im2 | 0.89 | 0.95 | 18.42 | 0.83 | 1.06 | |
| Im3 | 0.94 | 0.97 | 22.03 | 0.90 | 2.65 | |
| Ave | 0.91 | 0.95 | 18.71 | 0.86 | 2.19 | |
| Wang | Im1 | 0.75 | 0.89 | 14.81 | 0.69 | 2.60 |
| Im2 | 0.75 | 0.94 | 18.10 | 0.72 | 0.95 | |
| Im3 | 0.71 | 0.90 | 16.14 | 0.74 | 2.15 | |
| Ave | 0.74 | 0.91 | 16.78 | 0.72 | 1.93 | |
| Ours | Im1 | 1.01 | 0.96 | 27.65 | 1.43 | 3.02 |
| Im2 | 0.94 | 0.96 | 20.90 | 1.58 | 1.24 | |
| Im3 | 1.01 | 0.96 | 22.84 | 1.46 | 3.11 | |
| Ave | 0.98 | 0.96 | 23.23 | 1.53 | 2.49 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tan, W.; Xu, C.; Lei, F.; Fang, Q.; An, Z.; Wang, D.; Han, J.; Qian, K.; Feng, B. An Endoscope Image Enhancement Algorithm Based on Image Decomposition. Electronics 2022, 11, 1909. https://doi.org/10.3390/electronics11121909
Tan W, Xu C, Lei F, Fang Q, An Z, Wang D, Han J, Qian K, Feng B. An Endoscope Image Enhancement Algorithm Based on Image Decomposition. Electronics. 2022; 11(12):1909. https://doi.org/10.3390/electronics11121909
Chicago/Turabian StyleTan, Wei, Chao Xu, Fang Lei, Qianqian Fang, Ziheng An, Dou Wang, Jubao Han, Kai Qian, and Bo Feng. 2022. "An Endoscope Image Enhancement Algorithm Based on Image Decomposition" Electronics 11, no. 12: 1909. https://doi.org/10.3390/electronics11121909
APA StyleTan, W., Xu, C., Lei, F., Fang, Q., An, Z., Wang, D., Han, J., Qian, K., & Feng, B. (2022). An Endoscope Image Enhancement Algorithm Based on Image Decomposition. Electronics, 11(12), 1909. https://doi.org/10.3390/electronics11121909