
Spatially-Resolved Multiply-Excited Autofluorescence and Diffuse Reflectance Spectroscopy: SpectroLive Medical Device for Skin In Vivo Optical Biopsy


Abstract
1. Introduction
2. Materials and Methods
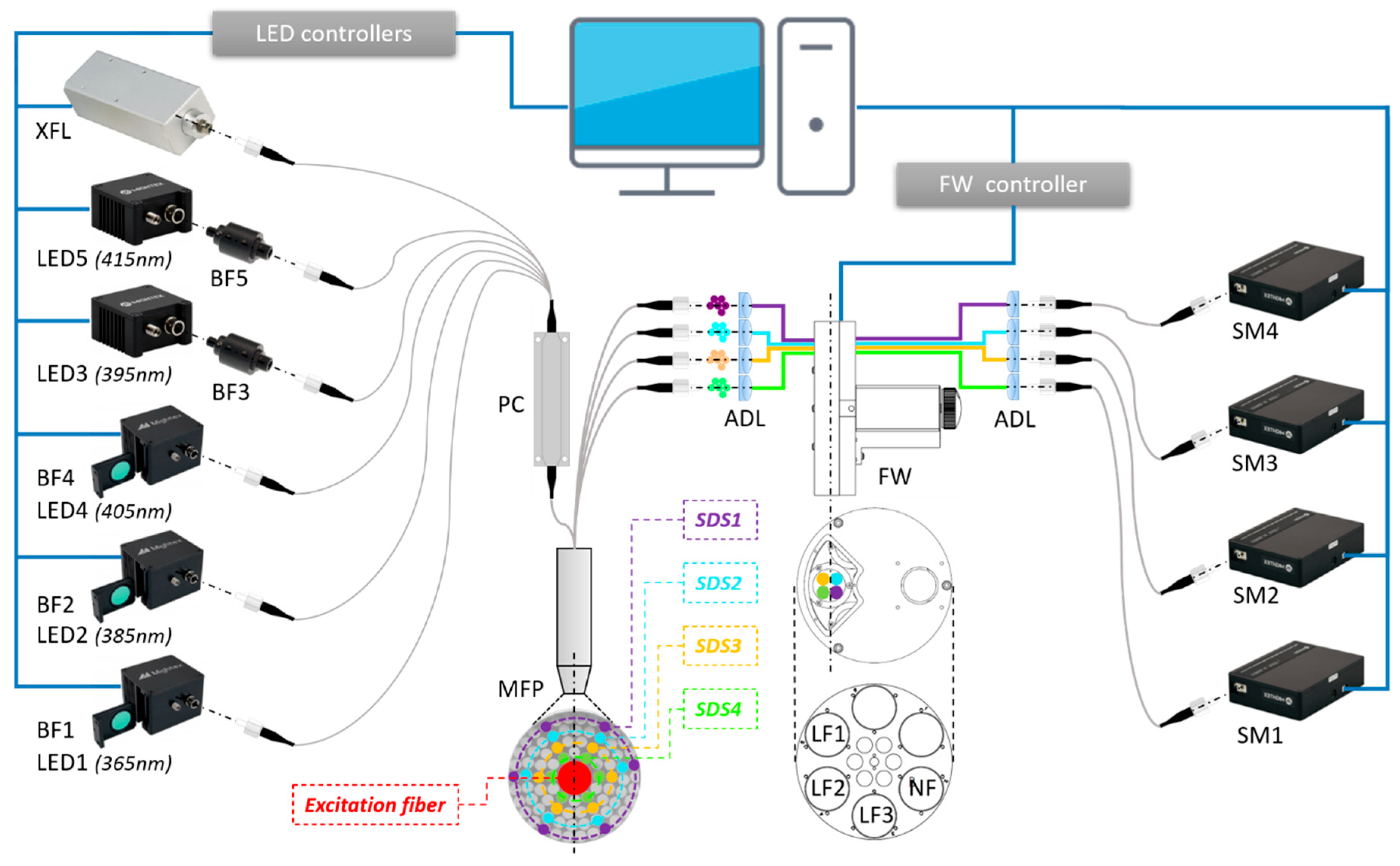
2.1. SpectroLive Spectroscopic Device
2.1.1. Light Sources
2.1.2. Optical Probe
2.1.3. Detection Channels
- LF1 (BLP01-364R-25, Semrock®) used to filter excitation from the 365 nm-LED;
- LF2 (BLP01-405R-25, Semrock®) used to filter excitation from the 385, 395 and 405 nm LEDs;
- LF3 (BLP01-442R-25, Semrock®) used to filter excitation from the 415 nm LED;
- A neutral density filter (NF) is used for the diffuse reflectance measurement (using the white light source). The two remaining filter holder locations are left empty on the wheel.
2.1.4. Spectra Acquisition Sequence
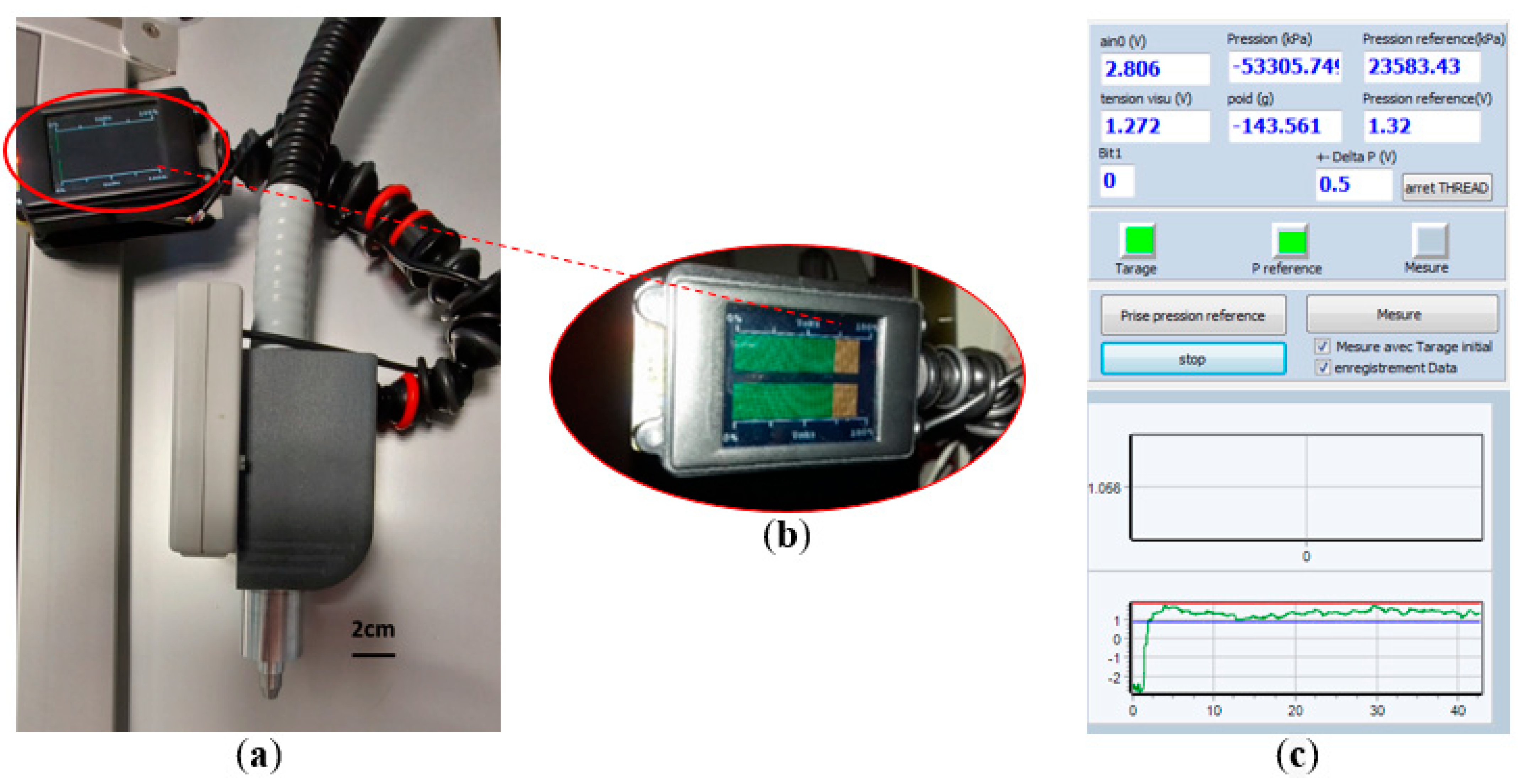
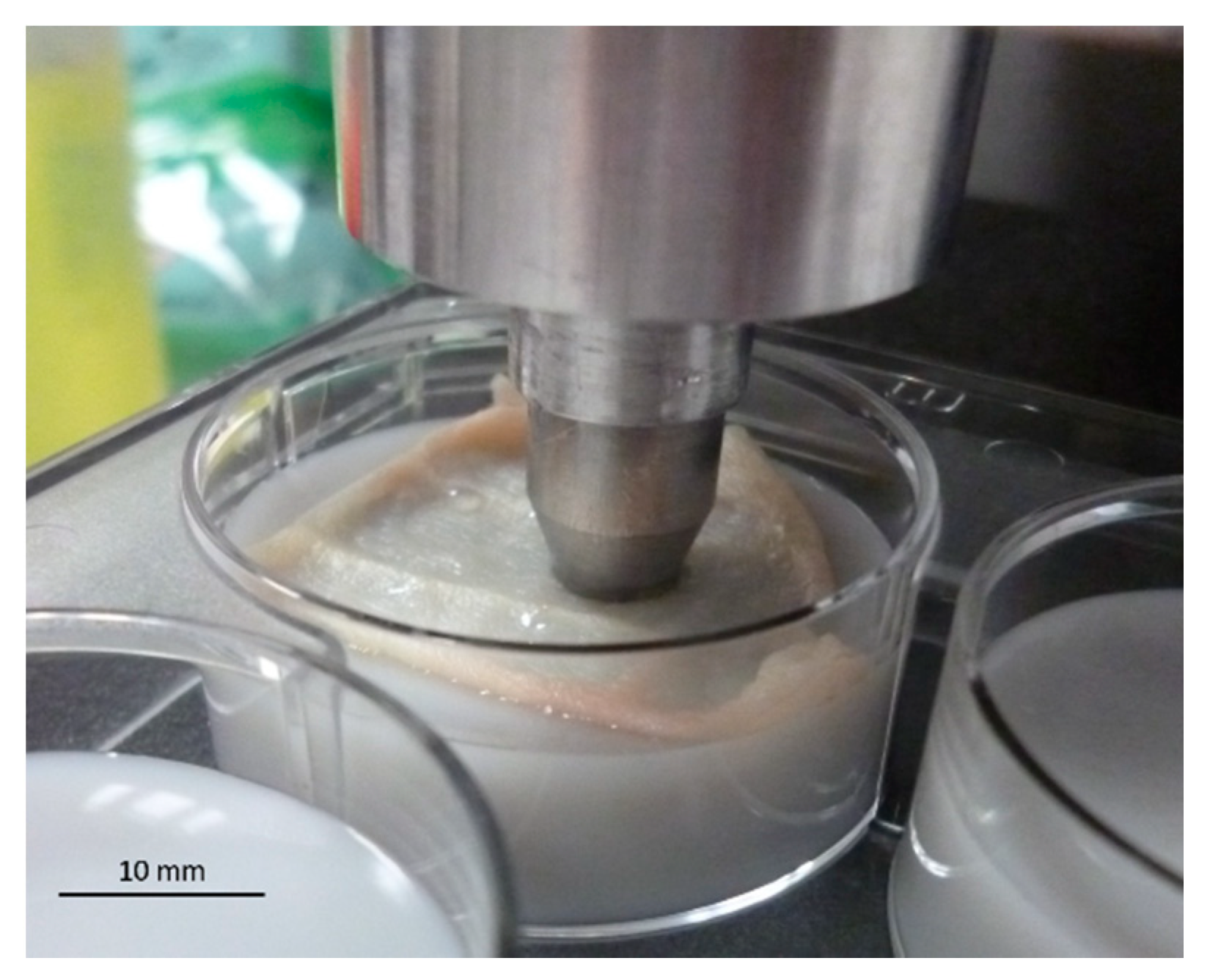
2.2. Probe Pressure Control Device
2.3. Intensity and Spectral Corrections and Calibrations
2.3.1. Correction of the Spectral Attenuations throughout Optical Acquisition Channels
2.3.2. Dark Noise and Background Noise Characterization and Correction
2.3.3. Light Sources Irradiance Characterization
2.4. Safety Tests
- -
- Electrical safety according to the EN60601-1:2007 standard entitled “Medical electrical equipment—Part 1: general requirements for basic safety and essential performance”,
- -
- Electromagnetic compatibility according to the EN60601-1-2:2007 standard entitled “Medical electrical equipment—Part 1-2: general requirements for basic safety and essential performance—Collateral standard: electromagnetic compatibility—Requirements and tests”.
- -
- Photobiological safety according to the EN 62471:2008 standard entitled “Photobiological safety of lamps and lamp systems”.
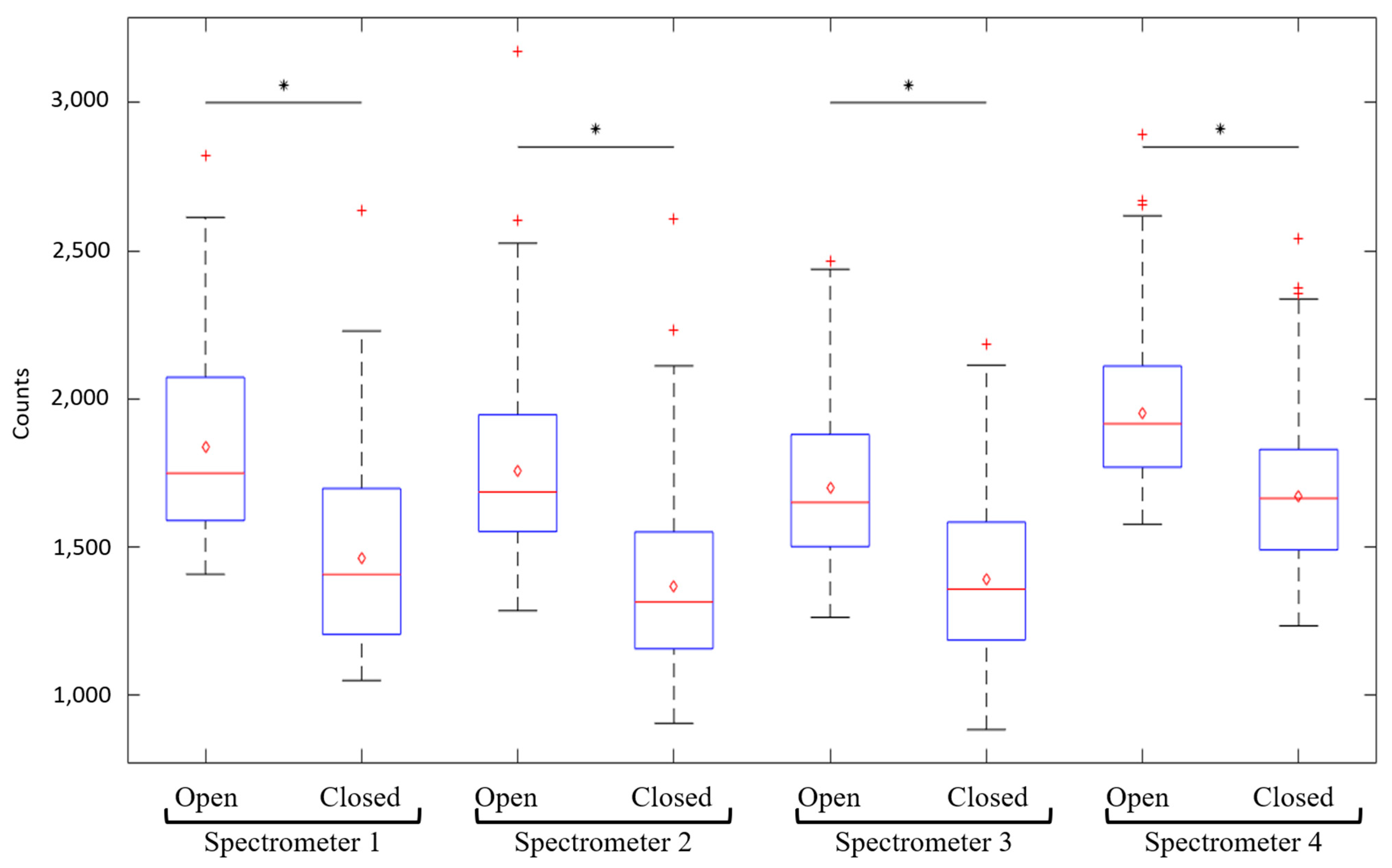
2.5. Depth Sensitivity Tests
3. Results
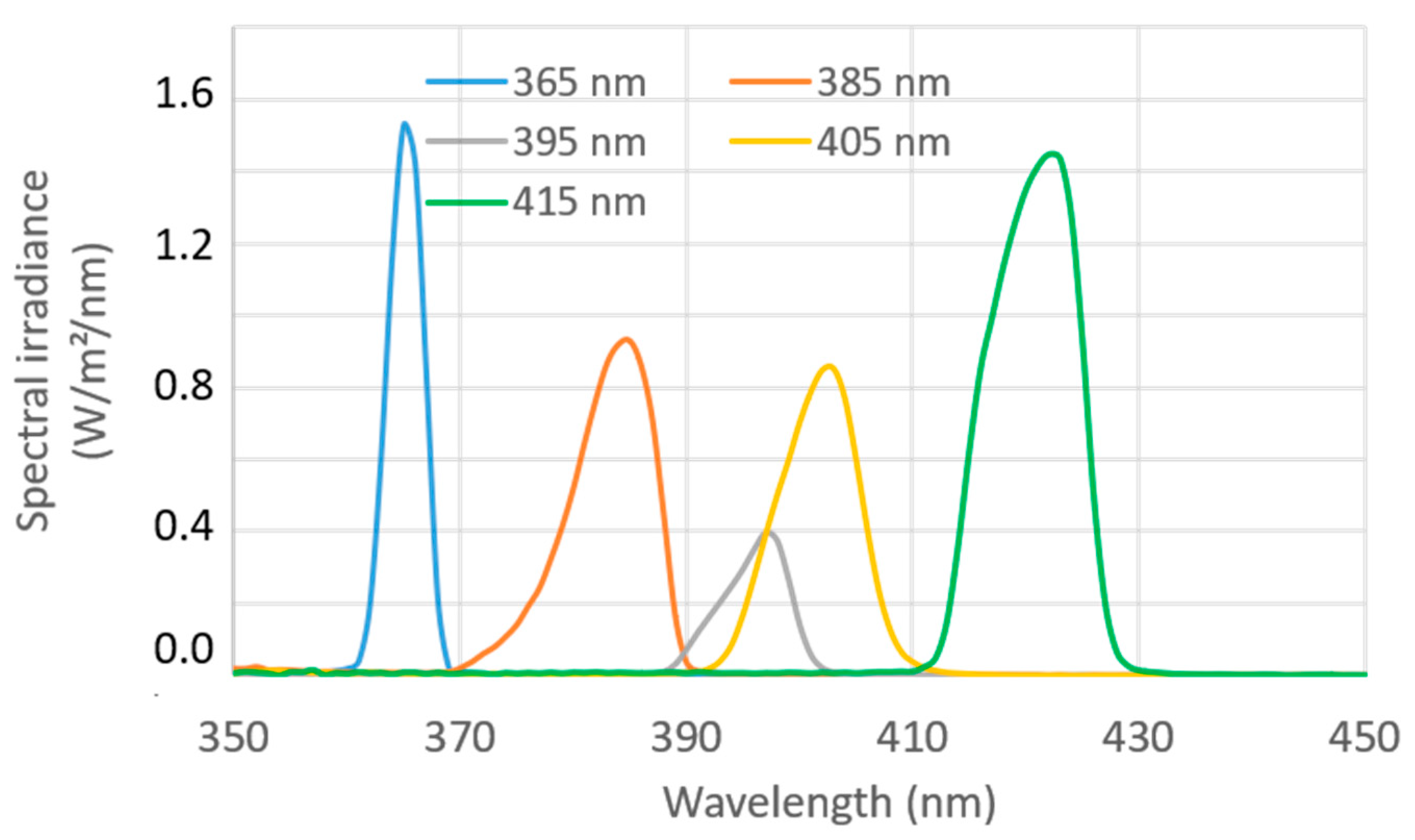
3.1. Excitation Spectral Irradiance of the SpectroLive Light Excitation Sources
3.2. Safety Tests
3.2.1. Electrical Safety
3.2.2. Electromagnetic Compatibility
3.2.3. Photobiological Safety
3.3. Spectral Correction and Intensity Relative Normalization
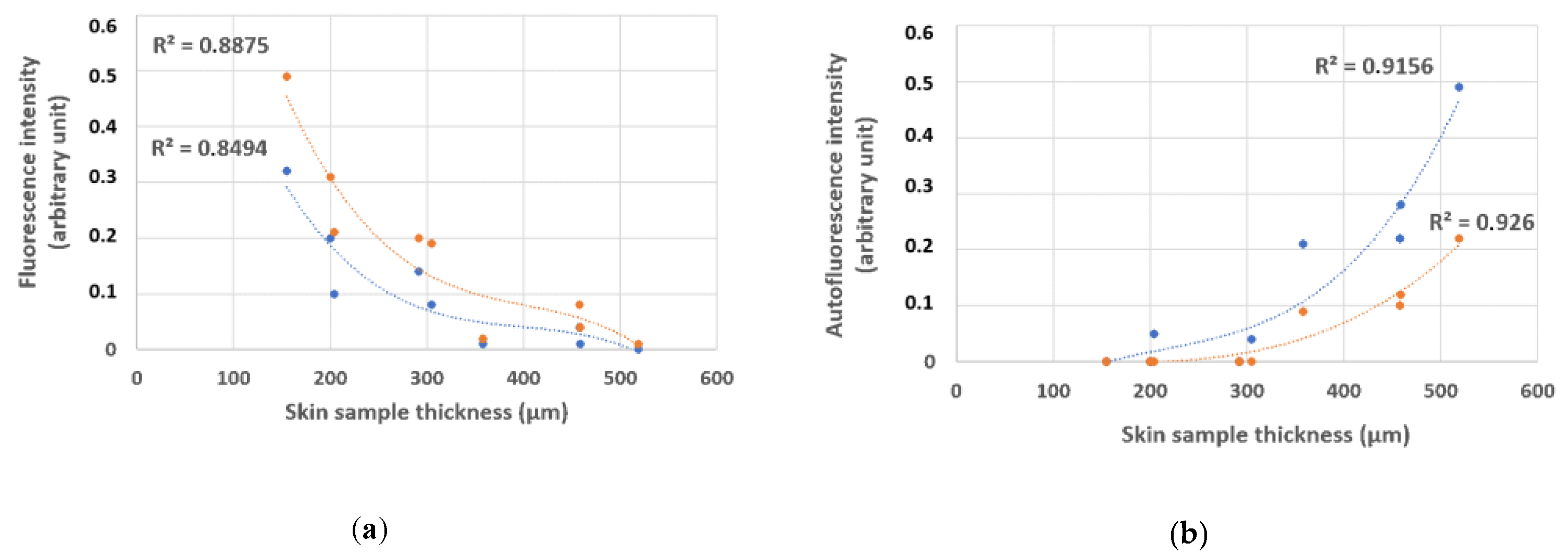
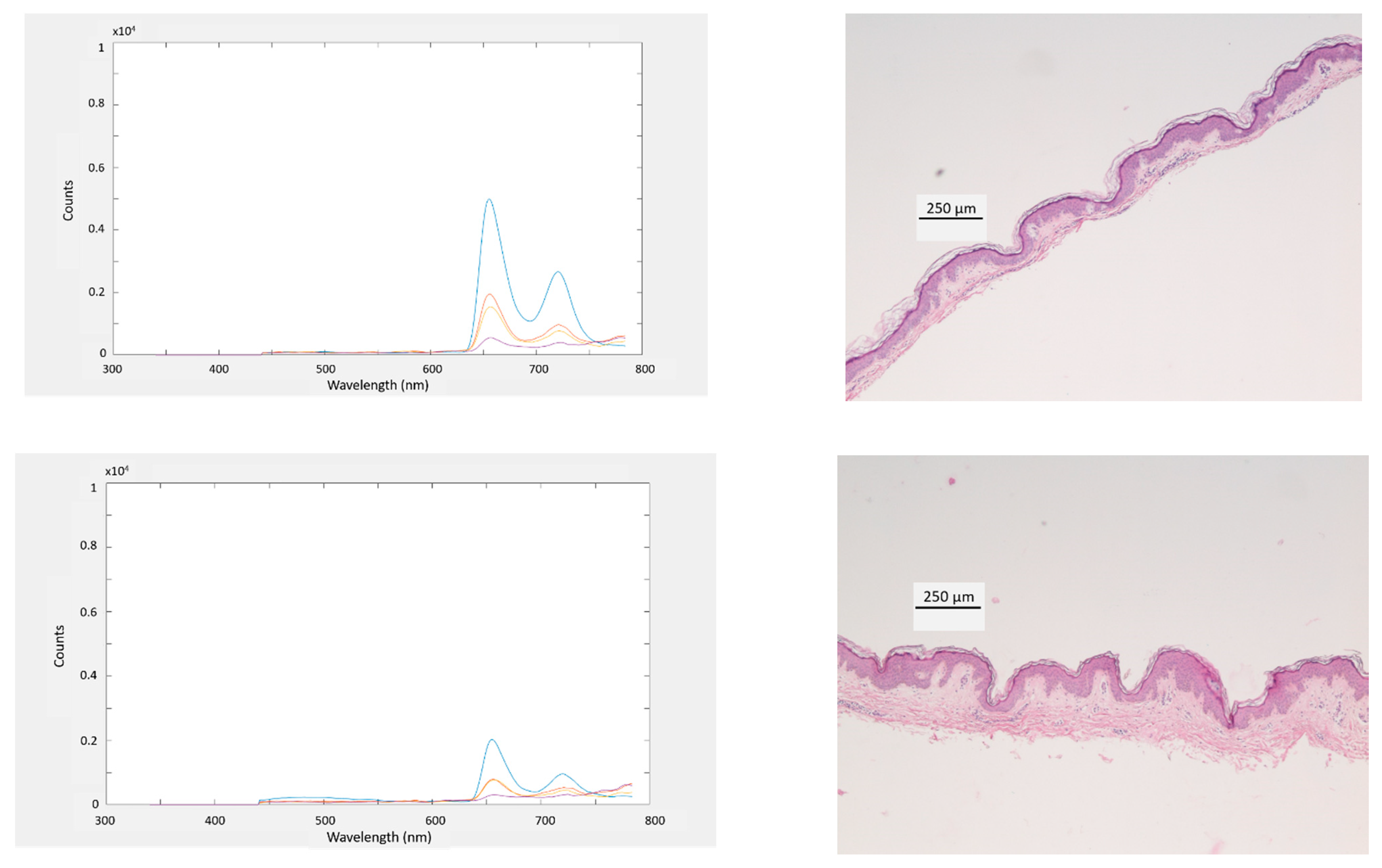
3.4. Depth Sensitivity of Fluorescence Measurement
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stratigos, A.; Garbe, C.; Lebbe, C.; Malvehy, J.; del Marmol, V.; Pehamberger, H.; Peris, K.; Becker, J.C.; Zalaudek, I.; Saiag, P.; et al. Diagnosis and Treatment of Invasive Squamous Cell Carcinoma of the Skin: European Consensus-Based Interdisciplinary Guideline. Eur. J. Cancer 2015, 51, 1989–2007. [Google Scholar] [CrossRef]
- Grillone, G.A.; Wang, Z.; Krisciunas, G.P.; Tsai, A.C.; Kannabiran, V.R.; Pistey, R.W.; Zhao, Q.; Rodriguez-Diaz, E.; A’Amar, O.M.; Bigio, I.J. The Color of Cancer: Margin Guidance for Oral Cancer Resection Using Elastic Scattering Spectroscopy. Laryngoscope 2017, 127 (Suppl. 4), S1–S9. [Google Scholar] [CrossRef]
- Borisova, E.; Pavlova, P.; Pavlova, E.; Troyanova, P.; Avramov, L. Optical Biopsy of Human Skin - A Tool for Cutaneous Tumours’ Diagnosis. Int. J. Bioautomation 2012, 16, 53–72. [Google Scholar]
- Yaroslavsky, A.N.; Feng, X.; Yu, S.H.; Jermain, P.R.; Iorizzo, T.W.; Neel, V.A. Dual-Wavelength Optical Polarization Imaging for Detecting Skin Cancer Margins. J. Investig. Dermatol. 2020, 140, 1994–2000. [Google Scholar] [CrossRef]
- Cabrera, R.; Recule, F. Unusual Clinical Presentations of Malignant Melanoma: A Review of Clinical and Histologic Features with Special Emphasis on Dermatoscopic Findings. Am. J. Clin. Dermatol. 2018, 19, 15–23. [Google Scholar] [CrossRef]
- Dubois, A.; Levecq, O.; Azimani, H.; Siret, D.; Barut, A.; Suppa, M.; del Marmol, V.; Malvehy, J.; Cinotti, E.; Rubegni, P.; et al. Line-Field Confocal Optical Coherence Tomography for High-Resolution Noninvasive Imaging of Skin Tumors. J. Biomed. Opt. 2018, 23, 106007. [Google Scholar] [CrossRef]
- Fraga-Braghiroli, N.; Grant-Kels, J.M.; Oliviero, M.; Rabinovitz, H.; Ferenczi, K.; Scope, A. The Role of Reflectance Confocal Microscopy in Differentiating Melanoma in Situ from Dysplastic Nevi with Severe Atypia: A Cross-Sectional Study. J. Am. Acad. Dermatol. 2020, 83, 1035–1043. [Google Scholar] [CrossRef]
- Yélamos, O.; Manubens, E.; Jain, M.; Chavez-Bourgeois, M.; Pulijal, S.V.; Dusza, S.W.; Marchetti, M.A.; Barreiro, A.; Marino, M.L.; Malvehy, J.; et al. Improvement of Diagnostic Confidence and Management of Equivocal Skin Lesions by Integration of Reflectance Confocal Microscopy in Daily Practice: Prospective Study in 2 Referral Skin Cancer Centers. J. Am. Acad. Dermatol. 2020, 83, 1057–1063. [Google Scholar] [CrossRef]
- Bigio, I.J.; Mourant, J.R. Ultraviolet and Visible Spectroscopies for Tissue Diagnostics: Fluorescence Spectroscopy and Elastic-Scattering Spectroscopy. Phys. Med. Biol. 1997, 42, 803–814. [Google Scholar] [CrossRef]
- Goth, W.; Lesicko, J.; Sacks, M.S.; Tunnell, J.W. Optical-Based Analysis of Soft Tissue Structures. Annu. Rev. Biomed. Eng. 2016, 18, 357–385. [Google Scholar] [CrossRef]
- Drakaki, E.; Borisova, E.; Makropoulou, M.; Avramov, L.; Serafetinides, A.A.; Angelov, I. Laser Induced Autofluorescence Studies of Animal Skin Used in Modeling of Human Cutaneous Tissue Spectroscopic Measurements. Skin Res. Technol. 2007, 13, 350–359. [Google Scholar] [CrossRef] [PubMed]
- Basen-Engquist, K.; Shinn, E.H.; Warneke, C.; de Moor, C.; Le, T.; Richards-Kortum, R.; Follen, M. Patient Distress and Satisfaction with Optical Spectroscopy in Cervical Dysplasia Detection. Am. J. Obstet. Gynecol. 2003, 189, 1136–1142. [Google Scholar] [CrossRef]
- Volynskaya, Z.; Haka, A.S.; Bechtel, K.L.; Fitzmaurice, M.; Shenk, R.; Wang, N.; Nazemi, J.; Dasari, R.R.; Feld, M.S. Diagnosing Breast Cancer Using Diffuse Reflectance Spectroscopy and Intrinsic Fluorescence Spectroscopy. J. Biomed. Opt. 2008, 13, 024012. [Google Scholar] [CrossRef] [PubMed]
- Mustafa, F.H.; Jaafar, M.S. Comparison of Wavelength-Dependent Penetration Depths of Lasers in Different Types of Skin in Photodynamic Therapy. Indian J. Phys. 2013, 87, 203–209. [Google Scholar] [CrossRef]
- Robertson, K.; Rees, J.L. Variation in Epidermal Morphology in Human Skin at Different Body Sites as Measured by Reflectance Confocal Microscopy. Acta Derm. Venereol. 2010, 90, 368–373. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, M.; Dousset, L.; Mahfouf, W.; Serrano-Sanchez, M.; Redonnet-Vernhet, I.; Mesli, S.; Kasraian, Z.; Obre, E.; Bonneu, M.; Claverol, S.; et al. Energy Metabolism Rewiring Precedes UVB-Induced Primary Skin Tumor Formation. Cell Rep. 2018, 23, 3621–3634. [Google Scholar] [CrossRef]
- Hennessy, R.; Goth, W.; Sharma, M.; Markey, M.K.; Tunnell, J.W. Effect of Probe Geometry and Optical Properties on the Sampling Depth for Diffuse Reflectance Spectroscopy. J. Biomed. Opt. 2014, 19. [Google Scholar] [CrossRef]
- Deonizio, J.; Werner, B.; Mulinari-Brenner, F.A. Histological Comparison of Two Cryopeeling Methods for Photodamaged Skin. ISRN Dermatol. 2014, 2014, 950754. [Google Scholar] [CrossRef]
- Zherebtsova, A.I.; Dremin, V.V.; Makovik, I.N.; Zherebtsov, E.A.; Dunaev, A.V.; Goltsov, A.; Sokolovski, S.G.; Rafailov, E.U. Multimodal Optical Diagnostics of the Microhaemodynamics in Upper and Lower Limbs. Front. Physiol. 2019, 10. [Google Scholar] [CrossRef]
- Papayan, G.V.; Petrishchev, N.N.; Zhurba, V.M.; Kishalov, A.A.; Galagudza, M.M. Fiber Fluorescence–Reflection Spectrometer with Multiwave Excitation. J. Opt. Technol. 2014, 81, 29–32. [Google Scholar] [CrossRef]
- Dremin, V.; Potapova, E.; Zherebtsov, E.; Kandurova, K.; Shupletsov, V.; Alekseyev, A.; Mamoshin, A.; Dunaev, A. Optical Percutaneous Needle Biopsy of the Liver: A Pilot Animal and Clinical Study. Sci. Rep. 2020, 10, 14200. [Google Scholar] [CrossRef] [PubMed]
- Ehlen, L.; Zabarylo, U.J.; Speichinger, F.; Bogomolov, A.; Belikova, V.; Bibikova, O.; Artyushenko, V.; Minet, O.; Beyer, K.; Kreis, M.E.; et al. Synergy of Fluorescence and Near-Infrared Spectroscopy in Detection of Colorectal Cancer. J. Surg. Res. 2019, 242, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Amouroux, M.; Diaz-Ayil, G.; Blondel, W.C.P.M.; Bourg-Heckly, G.; Leroux, A.; Guillemin, F. Classification of Ultraviolet Irradiated Mouse Skin Histological Stages by Bimodal Spectroscopy: Multiple Excitation Autofluorescence and Diffuse Reflectance. J. Biomed. Opt. 2009, 14, 014011. [Google Scholar] [CrossRef] [PubMed]
- Lim, L.; Nichols, B.; Migden, M.R.; Rajaram, N.; Reichenberg, J.S.; Markey, M.K.; Ross, M.I.; Tunnell, J.W. Clinical Study of Noninvasive in vivo Melanoma and Nonmelanoma Skin Cancers Using Multimodal Spectral Diagnosis. J. Biomed. Opt. 2014, 19, 117003. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.K.; Mirabal, Y.N.; Atkinson, E.N.; Cox, D.; Malpica, A.; Follen, M.; Richards-Kortum, R. Combined Reflectance and Fluorescence Spectroscopy for in vivo Detection of Cervical Pre-Cancer. J. Biomed. Opt. 2005, 10, 024031. [Google Scholar] [CrossRef] [PubMed]
- Hariri Tabrizi, S.; Aghamiri, S.M.R.; Farzaneh, F.; Sterenborg, H.J.C.M. The Use of Optical Spectroscopy for in vivo Detection of Cervical Pre-Cancer. Lasers Med. Sci. 2014, 29, 831–845. [Google Scholar] [CrossRef] [PubMed]
- Georgakoudi, I.; Jacobson, B.C.; Dam, J.V.; Backman, V.; Wallace, M.B.; Müller, M.G.; Zhang, Q.; Badizadegan, K.; Sun, D.; Thomas, G.A.; et al. Fluorescence, Reflectance, and Light-Scattering Spectroscopy for Evaluating Dysplasia in Patients with Barrett’s Esophagus. Gastroenterology 2001, 120, 1620–1629. [Google Scholar] [CrossRef]
- Bard, M.P.L.; Amelink, A.; Skurichina, M.; Noordhoek Hegt, V.; Duin, R.P.W.; Sterenborg, H.J.C.M.; Hoogsteden, H.C.; Aerts, J.G.J.V. Optical Spectroscopy for the Classification of Malignant Lesions of the Bronchial Tree. Chest 2006, 129, 995–1001. [Google Scholar] [CrossRef]
- Borisova, E.; Genova, T.; Bratashov, D.; Lomova, M.; Terziev, I.; Vladimirov, B.; Avramov, L.; Semyachkina-Glushkovskaya, O. Macroscopic and Microscopic Fluorescence Spectroscopy of Colorectal Benign and Malignant Lesions—Diagnostically Important Features. Biomed. Opt. Express 2019, 10, 3009–3017. [Google Scholar] [CrossRef]
- Wagnieres, G.A.; Star, W.M.; Wilson, B.C. In Vivo Fluorescence Spectroscopy and Imaging for Oncological Applications. Photochem. Photobiol. 1998, 68, 603–632. [Google Scholar] [CrossRef]
- Rajaram, N.; Aramil, T.J.; Lee, K.; Reichenberg, J.S.; Nguyen, T.H.; Tunnell, J.W. Design and Validation of a Clinical Instrument for Spectral Diagnosis of Cutaneous Malignancy. Appl. Opt. 2010, 49, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Motz, J.T.; Gandhi, S.J.; Scepanovic, O.R.; Haka, A.S.; Kramer, J.R.; Dasari, R.R.; Feld, M.S. Real-Time Raman System for in vivo Disease Diagnosis. J. Biomed. Opt. 2005, 10, 031113. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Ayil, G.; Amouroux, M.; Blondel, W.C.P.M.; Bourg-Heckly, G.; Leroux, A.; Guillemin, F.; Granjon, Y. Bimodal Spectroscopic Evaluation of Ultra Violet-Irradiated Mouse Skin Inflammatory and Precancerous Stages: Instrumentation, Spectral Feature Extraction/Selection and Classification (k-NN, LDA and SVM). Eur. Phys. J. Appl. Phys. 2009, 47, 12707. [Google Scholar] [CrossRef]
- Abdat, F.; Amouroux, M.; Guermeur, Y.; Blondel, W. Hybrid Feature Selection and SVM-Based Classification for Mouse Skin Precancerous Stages Diagnosis from Bimodal Spectroscopy. Opt. Express 2012, 20, 228–244. [Google Scholar] [CrossRef] [PubMed]
- Amouroux, M.; Blondel, W.; Delconte, A. Medical Device for Fibred Bimodal Optical Spectroscopy. U.S. Patent 10895503 (B2), 19 January 2021. [Google Scholar]
- Nath, A.; Rivoire, K.; Chang, S.; Cox, D.; Atkinson, E.N.; Follen, M.; Richards-Kortum, R. Effect of Probe Pressure on Cervical Fluorescence Spectroscopy Measurements. J. Biomed. Opt. 2004, 9, 523–533. [Google Scholar] [CrossRef] [PubMed]
- Cerussi, A.; Siavoshi, S.; Durkin, A.; Chen, C.; Tanamai, W.; Hsiang, D.; Tromberg, B.J. Effect of Contact Force on Breast Tissue Optical Property Measurements Using a Broadband Diffuse Optical Spectroscopy Handheld Probe. Appl. Opt. 2009, 48, 4270–4277. [Google Scholar] [CrossRef]
- Atencio, J.A.D.; Guillén, E.E.O.; y Montiel, S.V.; Rodríguez, M.C.; Ramos, J.C.; Gutiérrez, J.L.; Martínez, F. Influence of Probe Pressure on Human Skin Diffuse Reflectance Spectroscopy Measurements. Opt. Mem. Neural Netw. 2009, 18, 6–14. [Google Scholar] [CrossRef]
- Lim, L.; Nichols, B.; Rajaram, N.; Tunnell, J.W. Probe Pressure Effects on Human Skin Diffuse Reflectance and Fluorescence Spectroscopy Measurements. J. Biomed. Opt. 2011, 16. [Google Scholar] [CrossRef]
- Wang, L.; Jacques, S.L.; Zheng, L. MCML—Monte Carlo Modeling of Light Transport in Multi-Layered Tissues. Comput. Methods Programs Biomed. 1995, 47, 131–146. [Google Scholar] [CrossRef]
- Alerstam, E.; Lo, W.C.Y.; Han, T.D.; Rose, J.; Andersson-Engels, S.; Lilge, L. Next-Generation Acceleration and Code Optimization for Light Transport in Turbid Media Using GPUs. Biomed. Opt. Express 2010, 1, 658–675. [Google Scholar] [CrossRef]
- Asllanaj, F.; Contassot-Vivier, S.; Hohmann, A.; Kienle, A. Light Propagation in Biological Tissue. J. Quant. Spectrosc. Radiat. Transf. 2019, 224, 78–90. [Google Scholar] [CrossRef]
- Vargas, G.; Chan, K.F.; Thomsen, S.L.; Welch, A.J. Use of Osmotically Active Agents to Alter Optical Properties of Tissue: Effects on the Detected Fluorescence Signal Measured through Skin. Lasers Surg. Med. 2001, 29, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Que, S.K.T.; Zwald, F.O.; Schmults, C.D. Cutaneous Squamous Cell Carcinoma: Incidence, Risk Factors, Diagnosis, and Staging. J. Am. Acad. Dermatol. 2018, 78, 237–247. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Light Source | Narrow Band Excitation Peaks (nm) | Broad Band Excitation (DR) | ||||
|---|---|---|---|---|---|---|
| 365 | 385 | 395 | 405 | 415 | Xenon Flash Lamp | |
| Irradiance (W/m²) | 6 | 9 | 3 | 9 | 11 | 2 |
| FWHM (nm) | 4 | 9 | 7 | 9 | 10 | NA * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blondel, W.; Delconte, A.; Khairallah, G.; Marchal, F.; Gavoille, A.; Amouroux, M. Spatially-Resolved Multiply-Excited Autofluorescence and Diffuse Reflectance Spectroscopy: SpectroLive Medical Device for Skin In Vivo Optical Biopsy. Electronics 2021, 10, 243. https://doi.org/10.3390/electronics10030243
Blondel W, Delconte A, Khairallah G, Marchal F, Gavoille A, Amouroux M. Spatially-Resolved Multiply-Excited Autofluorescence and Diffuse Reflectance Spectroscopy: SpectroLive Medical Device for Skin In Vivo Optical Biopsy. Electronics. 2021; 10(3):243. https://doi.org/10.3390/electronics10030243
Chicago/Turabian StyleBlondel, Walter, Alain Delconte, Grégoire Khairallah, Frédéric Marchal, Amélie Gavoille, and Marine Amouroux. 2021. "Spatially-Resolved Multiply-Excited Autofluorescence and Diffuse Reflectance Spectroscopy: SpectroLive Medical Device for Skin In Vivo Optical Biopsy" Electronics 10, no. 3: 243. https://doi.org/10.3390/electronics10030243
APA StyleBlondel, W., Delconte, A., Khairallah, G., Marchal, F., Gavoille, A., & Amouroux, M. (2021). Spatially-Resolved Multiply-Excited Autofluorescence and Diffuse Reflectance Spectroscopy: SpectroLive Medical Device for Skin In Vivo Optical Biopsy. Electronics, 10(3), 243. https://doi.org/10.3390/electronics10030243