
CogniViTra, a Digital Solution to Support Dual-Task Rehabilitation Training

 ,
, 
 ,
,  and
and
Abstract
1. Introduction
2. Related Work
3. Cognitive Health Ecosystem
- Screening—sustainable population-based cognitive screening strategies to allow the population at risk to be tracked, without requiring physical travel to specialized clinical centers or expensive radiology, nuclear, or molecular medicine exams;
- Diagnosis—solutions to optimize the global neuropsychological assessment process of patients and to improve the collection of data on cognitive functioning to reduce patient fatigue and the duration of assessments;
- Rehabilitation—strategies to allow individual or group cognitive training programs, using cognitive tasks and others that involve exercises and movement, ideally at home or in community-based institutions;
- Research—multicentric scientific studies facilitated by a translational network environment that promotes large sample sizes, while simultaneously shortening the time needed to recruit patients and complete the study. These studies carried out within the ecosystem aim to facilitate the rapid implementation of innovative processes and the mobility of the knowledge produced;
- Impact—articulation between the various domains described above to have a significant impact in terms of the cognitive health of the population served, measured by the levels of intellectual performance, social participation, and quality of life of the citizens.
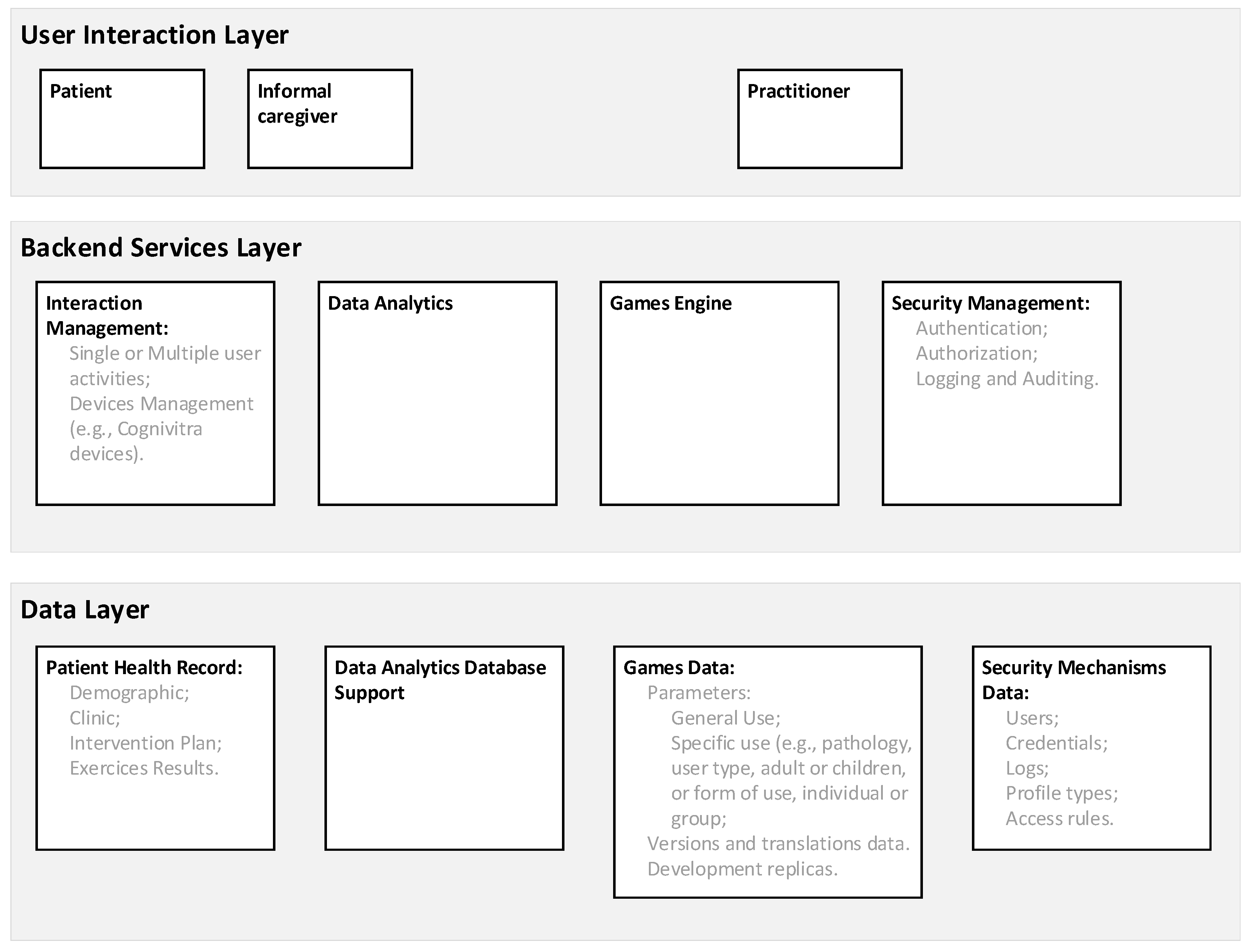
3.1. Platform of Services
3.2. User Application Layer
3.3. Backend Services Layer
- Authentication, to provide the identification of the users;
- Authorization, to regulate access to the information, including the establishment of access controls to limit personnel access, which is challenged by a diverse set of policies, complexity of workflows, and high risk of denying access to key information;
- Logging and Auditing, to trace which users look at which records so an auditor can use this information to detect abuses.
3.4. Data Layer
4. CogniViTra
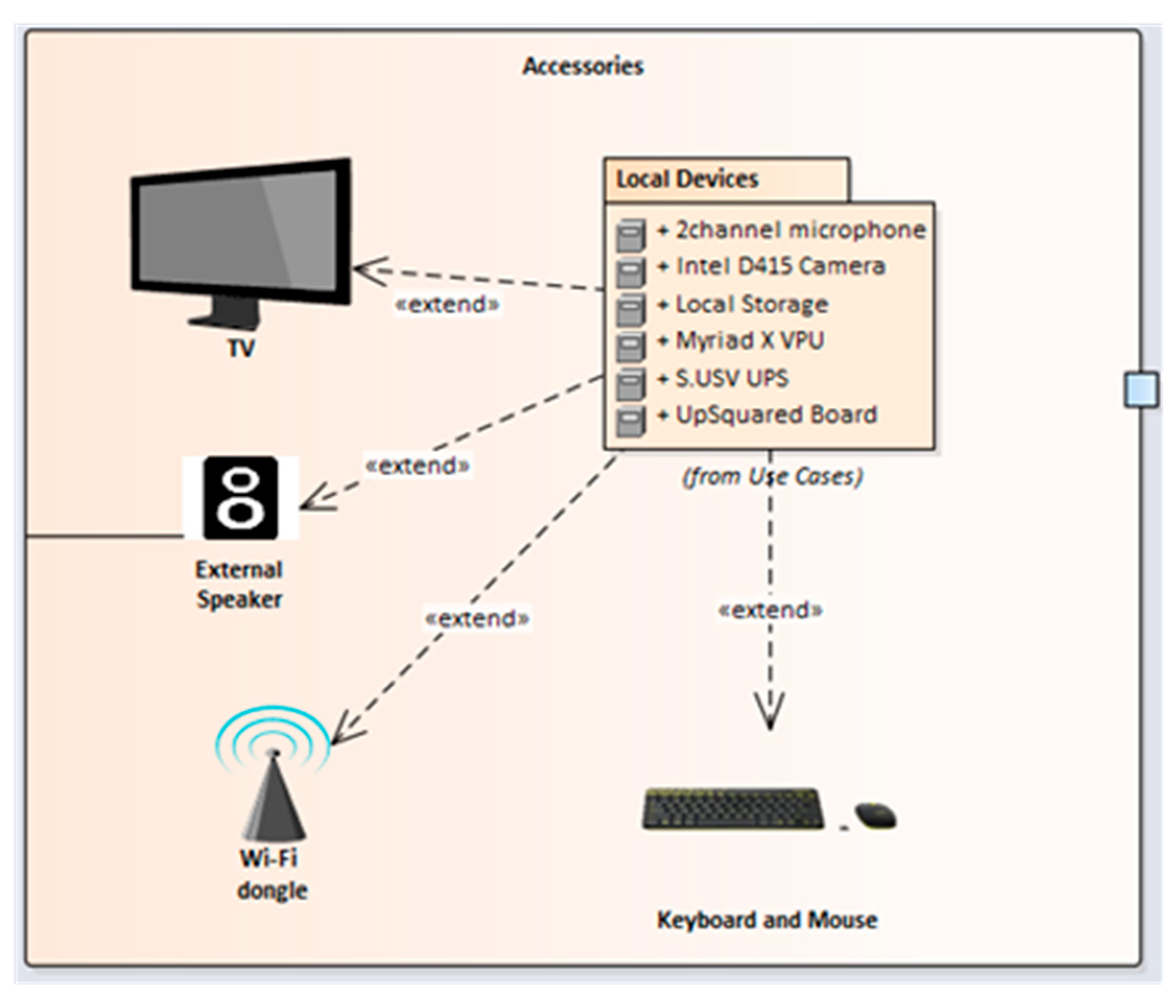
4.1. CogniViTra Box
- With the UPS requiring the latest version of the Ubuntu operating system (18.04 Long Term Support) and the VPU requiring at least version 16, the first step is to install and activate the Ubuntu operating system on the main board;
- Having the operating system and kernel installed, all peripheral ports will be available, and the remaining drivers can be installed in any order, namely the latest version of OpenVINO, OpenCV 3.4.4, Python 3.7, Virtualenv, and also Intel RealSense Software Development Kit 2.0.
4.2. Interaction Management
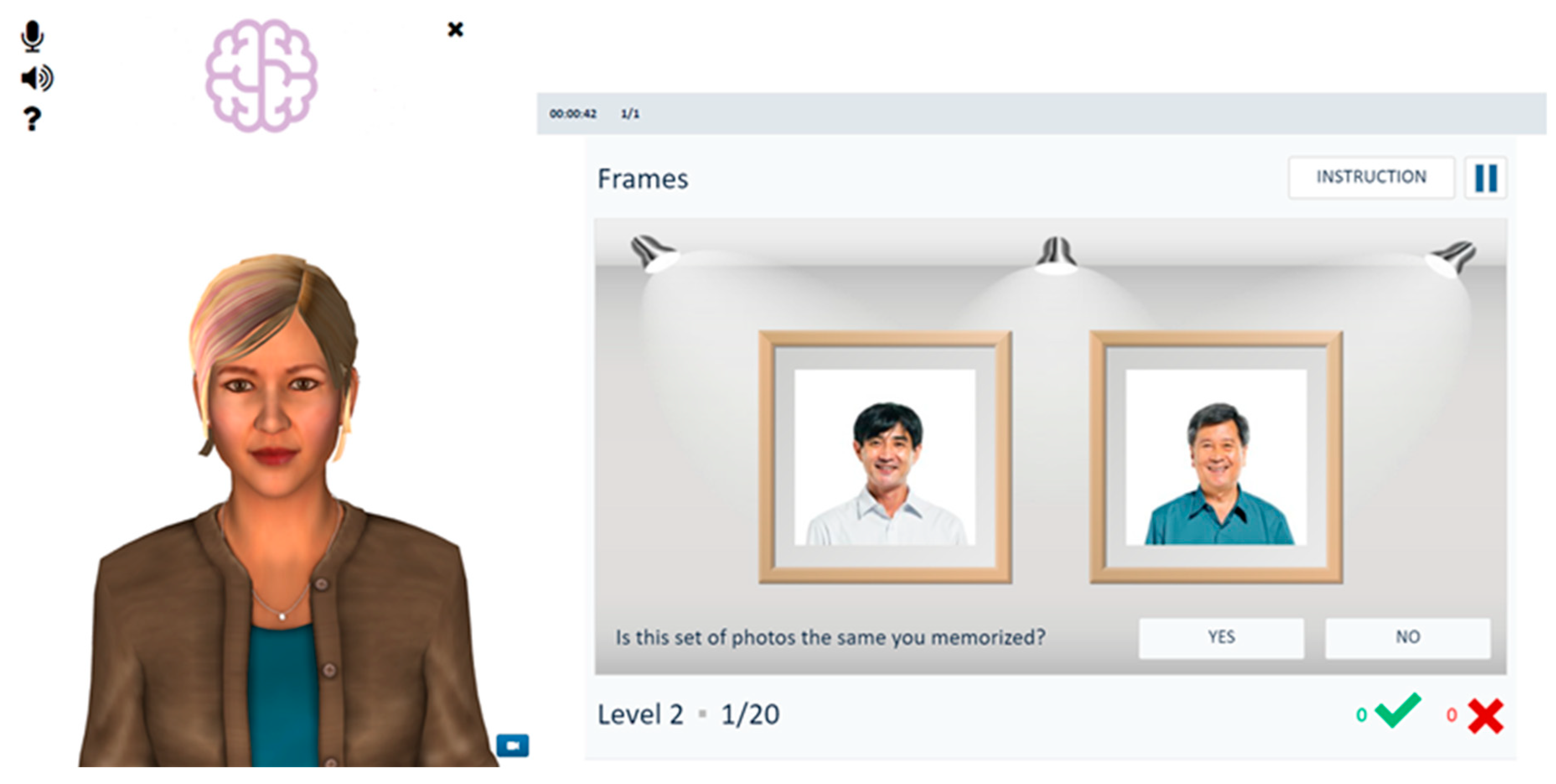
4.2.1. Digital Coach
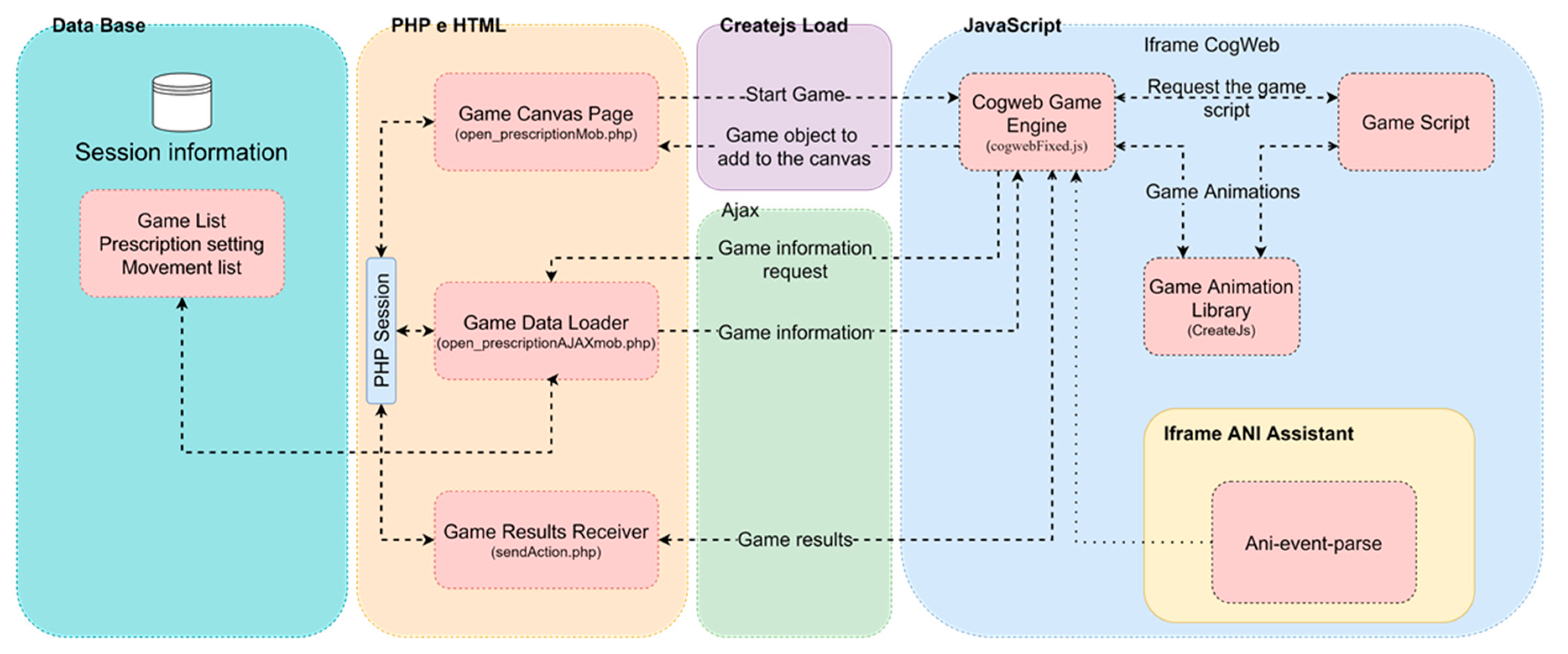
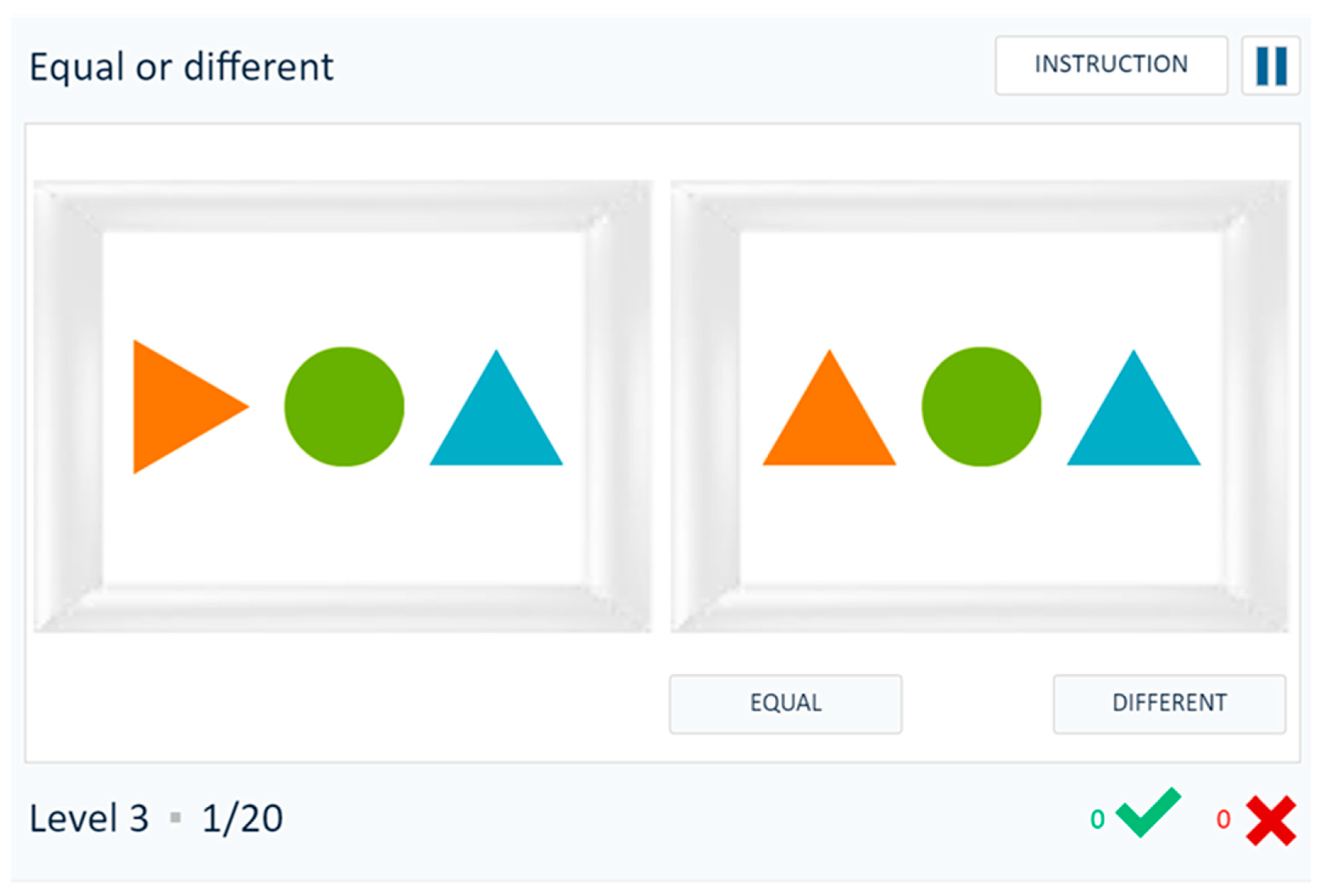
4.2.2. Games Presentation
- Game Canvas Page, where the game is presented on the client side;
- Game Data Loader, the point of access to information related to the game (e.g., game Id, name, or language);
- Game Results Receiver, the point of reception and storage of game results.
- These three elements are internments united by the PHP session system, which retains all information regarding client authentication and identification during the operation period.
- Looking at the Cognitive Game Engine from the Platform of Services side, the JavaScript elements are:
- Game Animation Library, which uses a set of modular libraries and tools that work together or independently to allow interactive web content called CreateJS;
- Cognitive Game Engine, the central point in our system, being responsible for managing several important exercise system elements, such as game loading and subsequent presentation on the canvas;
- Game Script, the file with specific logical instructions (e.g., operation or winning conditions) from the game, developed and generated in Adobe Animate.
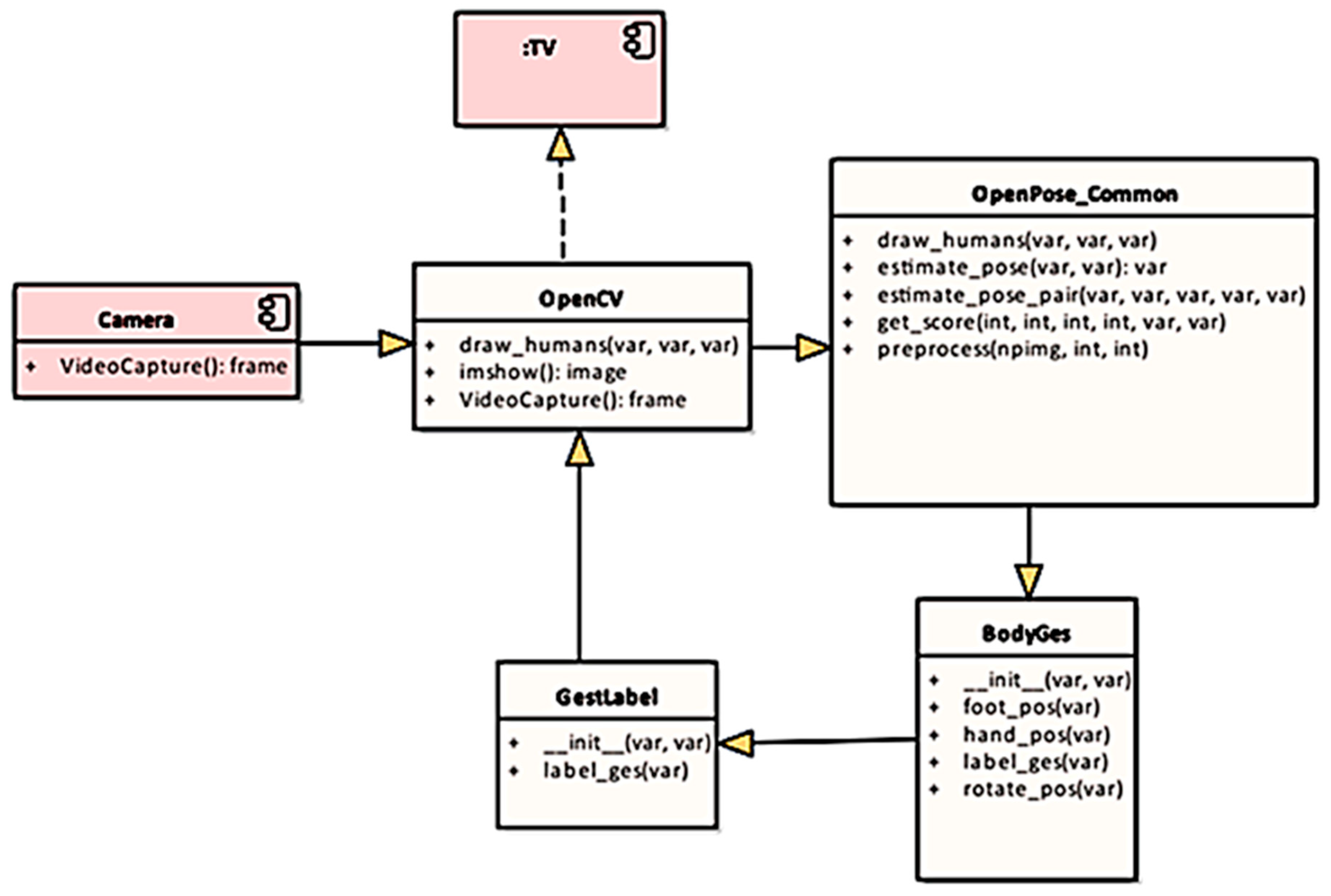
4.2.3. Pose and Gesture Recognition
- Body―full body poses, actions or motions;
- Hand and arm―arm pose and hand gestures;
- Head and face―nodding or shaking head, winkling lips.
- Sensor data collection―the raw data of poses and gestures are captured by sensors;
- Pose and gesture identification—in each frame, a pose or a gesture is identified from raw data;
- Pose and gesture tracking―the located skeleton is tracked during body movement;
- Pose and gesture classification―tracked pose or gesture is classified according to predefined pose and gesture types.
5. Assessment
5.1. Methods
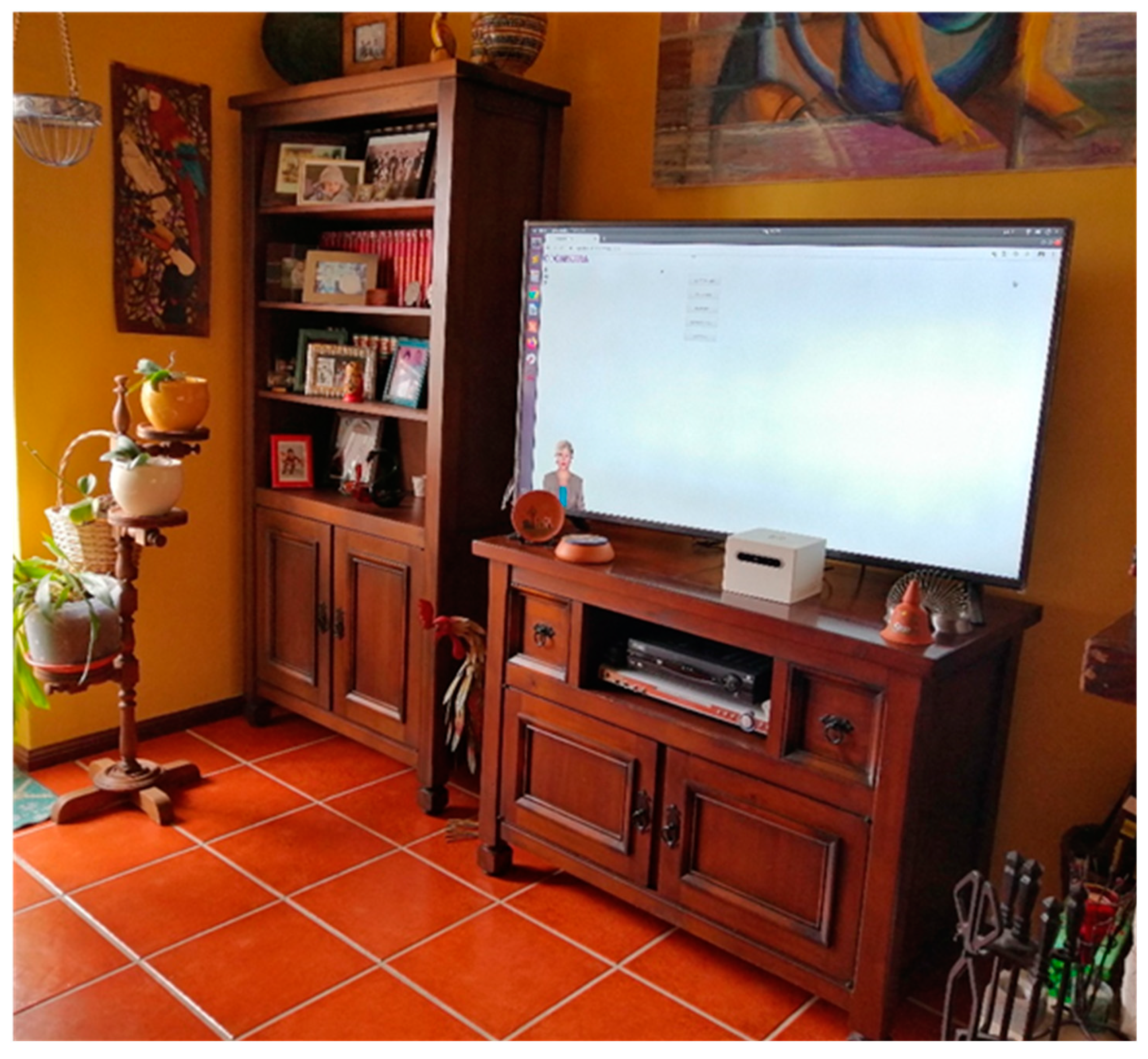
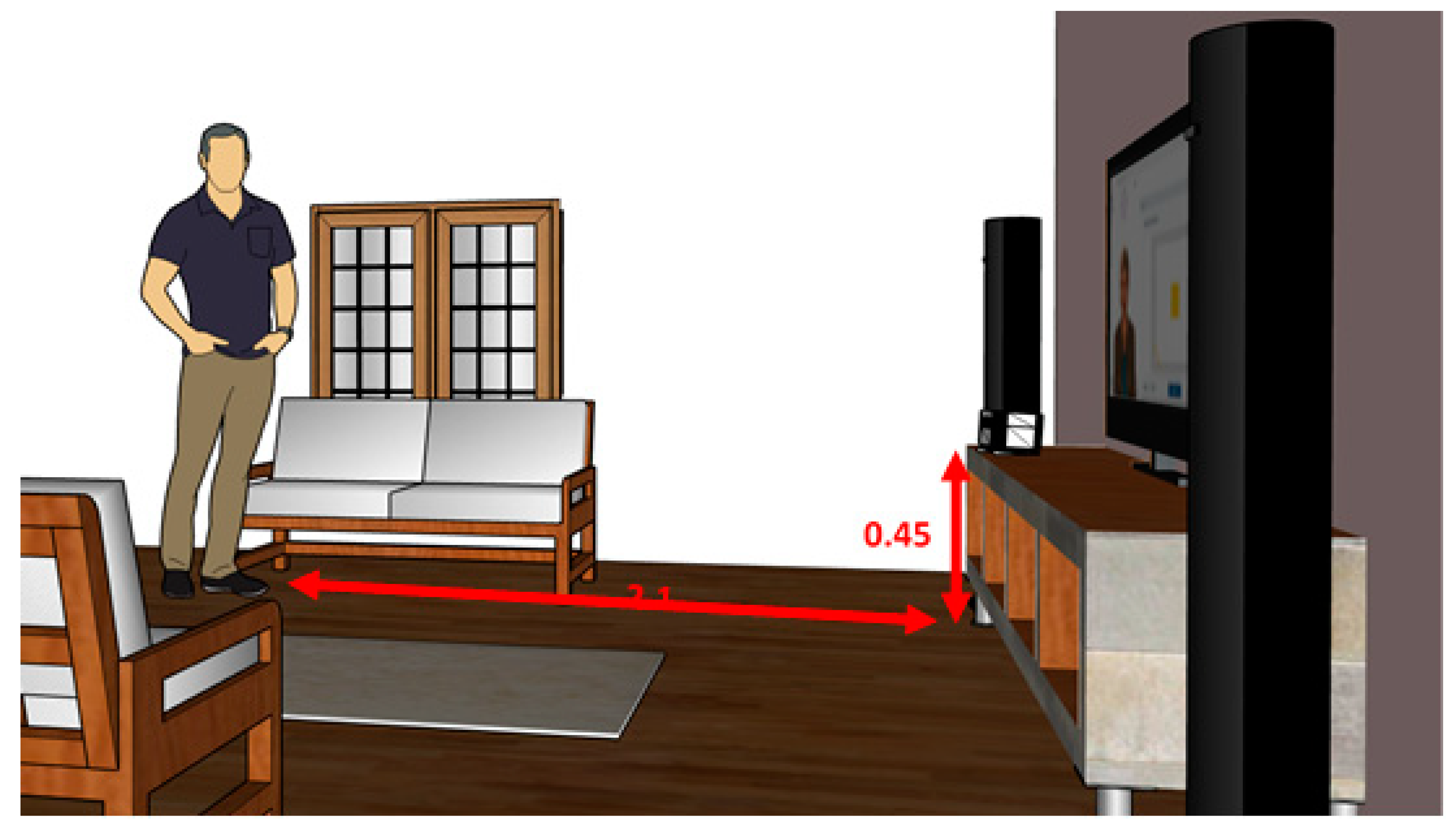
5.2. Prototype Setup
5.3. Results of the Conceptual Validation
6. Conclusions and Future Work
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ABAC | Attribute-based access control |
| AES | Advanced Encryption Standard |
| BML | Behavioral markup language |
| CogniViTra | Cognitive Vitality Training |
| HDMI | High-Definition Multimedia Interface |
| HTML | Hypertext Markup Language |
| GCM | Galois/Counter Mode |
| JSON | JavaScript Object Notation |
| JWT | JSON Web Token |
| PAF | Part affinity field |
| PHP | Hypertext Preprocessor |
| RBAC | Role-based access control |
| RGB | Red, green, and blue |
| SBC | Single board computer |
| SOA | Service oriented architecture |
| USB | Universal Serial Bus |
| UPS | Uninterruptible power supply |
| VPU | Vision processing unit |
| XACML | eXtensible Access Control Markup Language |
References
- Irazoki, E.; Contreras-Somoza, L.M.; Toribio-Guzmán, J.M.; Jenaro-Río, C.; van der Roest, H.; Franco-Martín, M.A. Technologies for Cognitive Training and Cognitive Rehabilitation for People with Mild Cognitive Impairment and Dementia. A Systematic Review. Front. Psychol. 2020, 11, 648. [Google Scholar] [CrossRef] [PubMed]
- Lezak, M.D.; Howieson, D.B.; Loring, D.W.; Fischer, J.S. Neuropsychological Assessment; Oxford University Press: Oxford, UK, 2004. [Google Scholar]
- Tacchino, A.; Veldkamp, R.; Coninx, K.; Brulmans, J.; Palmaers, S.; Hämäläinen, P.; D’hooge, M.; Vanzeir, E.; Kalron, A.; Brichetto, G.; et al. Design, Development, and Testing of an App for Dual-Task Assessment and Training Regarding Cognitive-Motor Interference (CMI-APP) in People with Multiple Sclerosis: Multicenter Pilot Study. JMIR mHealth uHealth 2020, 8, e15344. [Google Scholar] [CrossRef] [PubMed]
- McIsaac, T.L.; Lamberg, E.M.; Muratori, L.M. Building a framework for a dual task taxonomy. BioMed Res. Int. 2015, 591475. [Google Scholar] [CrossRef]
- Plummer, P.; Osborne, M.B. What Are We Attempting to Improve When We Train Dual-Task Performance? J. Neurol. Phys. Ther. 2015, 39, 154–155. [Google Scholar] [CrossRef]
- Ansai, J.H.; de Andrade, L.P.; de Souza Buto, M.S.; de Vassimon Barroso, V.; Farche, A.C.S.; Rossi, P.G.; de Medeiros Takahashi, A.C. Effects of the addition of a dual task to a supervised physical exercise program on older adults’ cognitive performance. J. Aging Phys. Act. 2017, 25, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Simon, S.S.; Yokomizo, J.E.; Bottino, C.M. Cognitive intervention in amnestic Mild Cognitive Impairment: A systematic review. Neurosci. Biobehav. Rev. 2012, 4, 1163–1178. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Shimada, H.; Makizako, H.; Doi, T.; Yoshida, D.; Tsutsumimoto, K.; Anan, Y.; Uemura, K.; Lee, L.; Park, H. Effects of multicomponent exercise on cognitive function in older adults with amnestic mild cognitive impairment: A randomized controlled trial. BMC Neurol. 2012, 1, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Shimada, H.; Makizako, H.; Doi, T.; Yoshida, D.; Ito, K.; Shimokata, H.; Washimi, Y.; Endo, H.; Kato, T. A randomized controlled trial of multicomponent exercise in older adults with mild cognitive impairment. PLoS ONE 2013, 4, e61483. [Google Scholar] [CrossRef] [PubMed]
- Langhorne, P.; Bernhardt, J.; Kwakkel, G. Stroke rehabilitation. Lancet 2011, 9778, 1693–1702. [Google Scholar] [CrossRef]
- Aminoff, M.J.; Boller, F.; Swaab, D.F. Foreward. In Handbook of Clinical Neurology; Michael, P.B., David, C.G., Eds.; Elsevier: Amsterdam, The Netherlads, 2013. [Google Scholar]
- Barnes, M.P.; Good, D.C. Preface. In Handbook of Clinical Neurology; Michael, P.B., David, C.G., Eds.; Elsevier: Amsterdam, The Netherlads, 2013. [Google Scholar]
- Barnes, D.E.; Santos-Modesitt, W.; Poelke, G.; Kramer, A.F.; Castro, C.; Middleton, L.E.; Yaffe, K. The Mental Activity and eXercise (MAX) trial: A randomized controlled trial to enhance cognitive function in older adults. JAMA Intern. Med. 2013, 9, 797–804. [Google Scholar] [CrossRef] [PubMed]
- Anderson-Hanley, C.; Barcelos, N.M.; Zimmerman, E.A.; Gillen, R.W.; Dunnam, M.; Cohen, B.D.; Yerokhin, V.; Miller, K.; Hyes, D.; Arciero, P.; et al. The aerobic and cognitive exercise study (ACES) for community-dwelling older adults with or at-risk for mild cognitive impairment (MCI): Neuropsychological, neurobiological and neuroimaging outcomes of a randomized clinical trial. Front. Aging Neurosci. 2018, 10, 76. [Google Scholar] [CrossRef] [PubMed]
- Damirchi, A.; Hosseini, F.; Babaei, P. Mental training enhances cognitive function and BDNF more than either physical or combined training in elderly women with MCI: A small-scale study. Am. J. Alzheimer’s Dis. Other Dement. 2018, 1, 20–29. [Google Scholar] [CrossRef]
- Gallou-Guyot, M.; Mandigout, S.; Combourieu-Donnezan, L.; Bherer, L.; Perrochon, A. Cognitive and physical impact of cognitive-motor dual-task training in cognitively impaired older adults: An overview. Neurophysiol. Clinique. 2020, 6, 441–453. [Google Scholar] [CrossRef] [PubMed]
- Tay, L.; Lim, W.S.; Chan, M.; Ali, N.; Chong, M.S. A combined cognitive stimulation and physical exercise programme (MINDVital) in early dementia: Differential effects on single-and dual-task gait performance. Gerontology 2016, 6, 604–610. [Google Scholar] [CrossRef]
- Liao, Y.Y.; Chen, I.; Lin, Y.J.; Chen, Y.; Hsu, W.C. Effects of virtual reality-based physical and cognitive training on executive function and dual-task gait performance in older adults with mild cognitive impairment: A randomized control trial. Front. Aging Neurosci. 2019, 11, 162. [Google Scholar] [CrossRef]
- McCaskey, M.A.; Schättin, A.; Martin-Niedecken, A.L.; de Bruin, E.D. Making more of IT: Enabling intensive motor cognitive rehabilitation exercises in geriatrics using information technology solutions. BioMed Res. Int. 2018, 2018, 1–17. [Google Scholar] [CrossRef]
- Martins, A.I.; Quintas, J.; Neves, L.; Sousa, S.; Cruz, V.T.; Pais, J.; Benhsain, D.; Callén, A.; Rocha, N.P. Cognivitra: An Information Technology-Based Solution to Support Cognitive and Physical Training at Home. In Proceedings of the 9th International Conference on Software Development and Technologies for Enhancing Accessibility and Fighting Info-exclusion, Vila Real, Portugal, 2–4 December 2020. [Google Scholar]
- Cruz, V.T.; Pais, J.; Ruano, L.; Mateus, C.; Colunas, M.; Alves, I.; Barreto, R.; Conde, E.; Sousa, A.; Araújo, I.; et al. Implementation and Outcomes of a Collaborative Multi-Center Network Aimed at Web-Based Cognitive Training–COGWEB Network. JMIR Ment. Health 2014, 1, e2. [Google Scholar] [CrossRef] [PubMed]
- Ruano, L.; Sousa, A.; Severo, M.; Alves, I.; Colunas, M.; Barreto, R.; Mateus, C.; Moreira, S.; Conde, E.; Bento, V.; et al. Development of a self-administered web-based test for longitudinal cognitive assessment. Sci. Rep. 2016, 1, 1–10. [Google Scholar] [CrossRef]
- Cicerone, K.D.; Langenbahn, D.M.; Braden, C.; Malec, J.F.; Kalmar, K.; Fraas, M.; Felicetti, T.; Laatsch, L.; Harley, J.P.; Bergquist, T.; et al. Evidence-based cognitive rehabilitation: Updated review of the literature from 2003 through 2008. Arch. Phys. Med. Rehabil. 2011, 4, 519–530. [Google Scholar] [CrossRef]
- Seshadri, S.; Wolf, P.A. Lifetime risk of stroke and dementia: Current concepts, and estimates from the Framingham Study. Lancet Neurol. 2007, 12, 1106–1114. [Google Scholar] [CrossRef]
- Vincent, C.; Desrosiers, J.; Landreville, P.; Demers, L. Burden of caregivers of people with stroke: Evolution and predictors. Cerebrovasc. Dis. 2009, 27, 456–464. [Google Scholar] [CrossRef] [PubMed]
- Rebok, G.W.; Langbaum, J.B.; Jones, R.N.; Gross, A.L.; Parisi, J.M.; Spira, A.P.; Kueider, A.M.; Petras, H.; Brandt, J. Memory training in the active study: How much is needed and who benefits? J. Aging Health 2012, 21S–42S. [Google Scholar] [CrossRef]
- World Health Organization. Atlas: Global Resources for Persons with Intellectual Disabilities; WHO Press: Geneva, Switzerland, 2007. [Google Scholar]
- Eaton, J.; McCay, L.; Semrau, M.; Chatterjee, S.; Baingana, F.; Araya, R.; Ntulo, C.; Thornicroft, G.; Saxena, S. Scale up of services for mental health in low-income and middle-income countries. Lancet 2011, 378, 1592–1603. [Google Scholar] [CrossRef]
- Kakuma, R.; Minas, H.; van Ginneken, N.; Dal Poz, M.R.; Desiraju, K.; Morris, J.E.; Saxena, S.; Scheffler, R.M. Human resources for mental health care: Current situation and strategies for action. Lancet 2011, 378, 1654–1663. [Google Scholar] [CrossRef]
- Putman, K.; de Wit, L. European comparison of stroke rehabilitation. Top Stroke Rehabil. 2009, 16, 20–26. [Google Scholar] [CrossRef] [PubMed]
- De Wit, L.; Putman, K.; Schuback, B.; Komárek, A.; Angst, F.; Baert, I.; Berman, P.; Bogaerts, K.; Brinkmann, N.; Connell, L.; et al. Motor and functional recovery after stroke: A comparison of 4 european rehabilitation centers. Stroke 2007, 38, 2101–2107. [Google Scholar] [CrossRef]
- Zeiler, S.R.; Krakauer, J.W. The interaction between training and plasticity in the poststroke brain. Curr. Opin. Neurol. 2013, 26, 609–616. [Google Scholar] [CrossRef]
- Dobkin, B.H.; Dorsch, A. The promise of mhealth: Daily activity monitoring and outcome assessments by wearable sensors. Neurorehabil. Neural Repair 2011, 25, 788–798. [Google Scholar] [CrossRef] [PubMed]
- Hobart, J.C.; Cano, S.J.; Zajicek, J.P.; Thompson, A.J. Rating scales as outcome measures for clinical trials in neurology: Problems, solutions, and recommendations. Lancet Neurol. 2007, 6, 1094–1105. [Google Scholar] [CrossRef]
- Rosser, N.; Floel, A. Pharmacological enhancement of motor recovery in subacute and chronic stroke. Neurorehabilitation 2008, 23, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Iosa, M.; Morone, G.; Fusco, A.; Bragoni, M.; Coiro, P.; Multari, M.; Venturiero, V.; de Angelis, D.; Pratesi, L.; Paolucci, S. Seven capital devices for the future of stroke rehabilitation. Stroke Res. Treat. 2012, 187965. [Google Scholar] [CrossRef]
- Selzer, M.E. Textbook of Neural Repair and Rehabilitation; Cambridge University Press: New York, NY, USA, 2006. [Google Scholar]
- Sharma, N.; Classen, J.; Cohen, L.G. Neural plasticity and its contribution to functional recovery. Handb. Clin. Neurol. 2013, 110, 3–12. [Google Scholar]
- Behrman, A.L.; Bowden, M.G.; Rose, D.K. Chapter 5—Clinical trials in neurorehabilitation. In Handbook of Clinical Neurology; Michael, P.B., David, C.G., Eds.; Elsevier: Amsterdam, The Netherlads, 2013. [Google Scholar]
- Mahncke, H.W.; Connor, B.B.; Appelman, J.; Ahsanuddin, O.N.; Hardy, J.L.; Wood, R.A.; Joyce, N.M.; Boniske, T.; Atkins, S.M.; Merzenich, M.M. Memory enhancement in healthy older adults using a brain plasticity-based training program: A randomized, controlled study. Proc. Natl. Acad. Sci. USA 2006, 103, 12523–12528. [Google Scholar] [CrossRef] [PubMed]
- La Rue, A. Healthy brain aging: Role of cognitive reserve, cognitive stimulation, and cognitive exercises. Clin. Geriatr. Med. 2010, 26, 99–111. [Google Scholar] [CrossRef]
- Nudo, R.J. Recovery after brain injury: Mechanisms and principles. Front. Hum. Neurosci. 2013, 7, 887. [Google Scholar] [CrossRef]
- Gardner, W.J.; Karnosh, L.J.; McClure, C.C., Jr.; Gardner, A.K. Residual function following hemispherectomy for tumour and for infantile hemiplegia. Brain 1955, 78, 487–502. [Google Scholar] [CrossRef]
- Chen, R.; Cohen, L.G.; Hallett, M. Nervous system reorganization following injury. Neuroscience 2002, 111, 761–773. [Google Scholar] [CrossRef]
- Staudt, M. Reorganization after pre- and perinatal brain lesions. J. Anat. 2010, 217, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Cohen, L.G.; Weeks, R.A.; Sadato, N.; Celnik, P.; Ishii, K.; Hallett, M. Period of susceptibility for cross-modal plasticity in the blind. Ann. Neurol. Off. J. Am. Neurol. Assoc. Child Neurol. Soc. 1999, 4, 451–460. [Google Scholar] [CrossRef]
- Eyre, J.A. Corticospinal tract development and its plasticity after perinatal injury. Neurosci. Biobehav. Rev. 2007, 31, 1136–1149. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, R.; Harvey, A.S.; Anderson, V. Executive function following focal frontal lobe lesions: Impact of timing of lesion on outcome. Cortex 2007, 43, 792–805. [Google Scholar] [CrossRef]
- He, Y.; Yang, L.; Zhou, J.; Yao, L.; Pang, M.Y. Dual-task training effects on motor and cognitive functional abilities in individuals with stroke: A systematic review. Clin. Rehabil. 2018, 7, 865–877. [Google Scholar] [CrossRef]
- Wang, X.; Pi, Y.; Chen, P.; Liu, Y.; Wang, R.; Chan, C. Cognitive motor interference for preventing falls in older adults: A systematic review and meta-analysis of randomised controlled trials. Age Ageing 2014, 44, 205–212. [Google Scholar] [CrossRef]
- Bacha, J.M.R.; Gomes, G.C.V.; de Freitas, T.B.; Viveiro, L.A.P.; da Silva, K.G.; Bueno, G.C.; Pompeu, J.E. Effects of Kinect adventures games versus conventional physical therapy on postural control in elderly people: A randomized controlled trial. Games Health J. 2018, 7, 24–36. [Google Scholar] [CrossRef]
- Lotfi, A.; Langensiepen, C.; Yahaya, S.W. Socially assistive robotics: Robot exercise trainer for older adults. Technologies 2018, 6, 32. [Google Scholar] [CrossRef]
- Kannan, L.; Vora, J.; Bhatt, T.; Hughes, S.L. Cognitive-motor exergaming for reducing fall risk in people with chronic stroke: A randomized controlled trial. Neurorehabilitation 2019, 44, 493–510. [Google Scholar] [CrossRef] [PubMed]
- Sturnieks, D.L.; Menant, J.; Valenzuela, M.; Delbaere, K.; Sherrington, C.; Herbert, R.D.; Lord, S.R. Effect of cognitive-only and cognitive-motor training on preventing falls in community-dwelling older people: Protocol for the smart±step randomised controlled trial. BMJ Open 2019, 9, e029409. [Google Scholar] [CrossRef]
- Arlati, S.; Colombo, V.; Spoladore, D.; Greci, L.; Pedroli, E.; Serino, S.; Sacco, M. A social virtual reality-based application for the physical and cognitive training of the elderly at home. Sensors 2019, 19, 261. [Google Scholar] [CrossRef]
- Andriella, A.; Torras, C.; Alenya, G. Cognitive system framework for brain-training exercise based on human-robot interaction. Cogn. Comput. 2020, 12, 793–810. [Google Scholar] [CrossRef]
- Yun, S.J.; Kang, M.G.; Yang, D.; Choi, Y.; Kim, H.; Oh, B.M.; Seo, H.G. Cognitive Training Using Fully Immersive, Enriched Environment Virtual Reality for Patients with Mild Cognitive Impairment and Mild Dementia: Feasibility and Usability Study. JMIR Serious Games 2020, 8, e18127. [Google Scholar] [CrossRef] [PubMed]
- Phirom, K.; Kamnardsiri, T.; Sungkarat, S. Beneficial Effects of Interactive Physical-Cognitive Game-Based Training on Fall Risk and Cognitive Performance of Older Adults. Int. J. Environ. Res. Public Health 2020, 17, 6079. [Google Scholar] [CrossRef] [PubMed]
- Peng, H.T.; Tien, C.W.; Lin, P.S.; Peng, H.Y.; Song, C.Y. Novel mat exergaming to improve the physical performance, cognitive function, and dual-task walking and decrease the fall risk of community-dwelling older adults. Front. Psychol. 2020, 11, 1620. [Google Scholar] [CrossRef]
- Adcock, M.; Fankhauser, M.; Post, J.; Lutz, K.; Zizlsperger, L.; Luft, A.R.; de Bruin, E.D. Effects of an in-home multicomponent exergame training on physical functions, cognition, and brain volume of older adults: A randomized controlled trial. Front. Med. 2020, 6, 321. [Google Scholar] [CrossRef]
- Manuli, A.; Maggio, M.G.; Latella, D.; Cannavò, A.; Balletta, T.; de Luca, R.; Calabrò, R.S. Can robotic gait rehabilitation plus Virtual Reality affect cognitive and behavioural outcomes in patients with chronic stroke? A randomized controlled trial involving three different protocols. J. Stroke Cerebrovasc. Dis. 2020, 29, 104994. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Shen, Z.; Liu, S.; Yuan, D.; Miao, C. Ping Pong: An Exergame for Cognitive Inhibition Training. Int. J. Hum. Comput. Interact. 2021, 1–12. [Google Scholar] [CrossRef]
- Swinnen, N.; Vandenbulcke, M.; de Bruin, E.D.; Akkerman, R.; Stubbs, B.; Firth, J.; Vancampfort, D. The efficacy of exergaming in people with major neurocognitive disorder residing in long-term care facilities: A pilot randomized controlled trial. Alzheimers Res. Ther. 2021, 13, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Jardim, N.Y.V.; Bento-Torres, N.V.O.; Costa, V.O.; Carvalho, J.P.R.; Pontes, H.T.S.; Tomás, A.M.; Diniz, C.W.P. Dual-Task Exercise to Improve Cognition and Functional Capacity of Healthy Older Adults. Front. Aging Neurosci. 2021, 13, 33. [Google Scholar] [CrossRef] [PubMed]
- Molhemi, F.; Monjezi, S.; Mehravar, M.; Shaterzadeh-Yazdi, M.J.; Salehi, R.; Hesam, S.; Mohammadianinejad, E. Effects of virtual reality vs conventional balance training on balance and falls in people with multiple sclerosis: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2021, 102, 290–299. [Google Scholar] [CrossRef]
- Laskey, K.B.; Laskey, K. Service oriented architecture. Wiley Interdiscip. Rev. Comput. Stat. 2009, 1, 101–105. [Google Scholar] [CrossRef]
- Wechsler, D. WAIS-III Administration and Scoring Manual; Psychological Corporation: San Antonio, TX, USA, 1997. [Google Scholar]
- Rosa, M.; Barraca, J.P.; Zuquete, A.; Rocha, N.P. A Parser to Support the Definition of Access Control Policies and Rules Using Natural Languages. J. Med. Syst. 2020, 44, 1–12. [Google Scholar] [CrossRef] [PubMed]
- OASIS, XACML (2013). Available online: http://docs.oasis-open.org/xacml/3.0/xacml-3.0-core-spec-os-en.html (accessed on 26 May 2021).
- Rosa, M.; Barraca, J.P.; Rocha, N.P. Blockchain structures to guarantee logging integrity of a digital platform to support community-dwelling older adults. Clust. Comput. 2020, 23, 1887–1898. [Google Scholar] [CrossRef]
- SmartBody. Available online: https://smartbody.ict.usc.edu/ (accessed on 7 April 2021).
- Mitra, S.; Acharya, T. Gesture recognition: A survey. IEEE Trans. Syst. Man Cybern. Part C 2007, 3, 311–324. [Google Scholar] [CrossRef]
- Liu, H.; Wang, L. Gesture recognition for human-robot collaboration: A review. Int. J. Ind. Ergon. 2018, 68, 355–367. [Google Scholar] [CrossRef]
- Starner, T.; Weaver, J.; Pentland, A. Real-time american sign language recognition using desk and wearable computer based video. IEEE Trans. Pattern Anal. Mach. Intell. 1998, 12, 1371–1375. [Google Scholar] [CrossRef]
- Wachs, J.P.; Kölsch, M.; Stern, H.; Edan, Y. Vision-based hand-gesture applications. Commun. ACM 2011, 2, 60–71. [Google Scholar] [CrossRef]
- Gokturk, S.B.; Yalcin, H.; Bamji, C. A time-of-flight depth sensor-system description, issues and solutions. In Proceedings of the 2004 Conference on Computer Vision and Pattern Recognition Workshop, Washington, DC, USA, 27 June–2 July 2004; pp. 33–35. [Google Scholar]
- Kapuściński, T.; Oszust, M.; Wysocki, M. Hand gesture recognition using time-of-flight camera and viewpoint feature histogram. In Intelligent Systems in Technical and Medical Diagnostics; Springer: Berlin/Heidelberg, Germany, 2014. [Google Scholar]
- Wang, C.; Liu, Z.; Chan, S.C. Superpixel-based hand gesture recognition with kinect depth camera. IEEE Trans. Multimed. 2014, 1, 29–39. [Google Scholar] [CrossRef]
- Erol, A.; Bebis, G.; Nicolescu, M.; Boyle, R.D. Vision-based hand pose estimation: A review. Comput. Vis. Image Underst. 2007, 1, 52–73. [Google Scholar] [CrossRef]
- Boyali, A.; Hashimoto, N.; Matsumoto, O. Hand posture and gesture recognition using MYO armband and spectral collaborative representation based classification. In Proceedings of the 2015 IEEE 4th Global Conference on Consumer Electronics (GCCE), Osaka, Japan, 27–30 October 2015; pp. 200–201. [Google Scholar]
- Zhang, Y.; Harrison, C. Wearable, low-cost electrical impedance tomography for hand gesture recognition. In Proceedings of the 28th Annual ACM Symposium on User Interface Software & Technology, Charlotte, NC, USA, 8–11 November 2015; pp. 167–173. [Google Scholar]
- Haroon, N.; Malik, A.N. Multiple hand gesture recognition using surface EMG signals. J. Biomed. Eng. Med. Imaging 2016, 1, 1. [Google Scholar] [CrossRef]
- Roy, S.; Ghosh, S.; Barat, A. Real-time implementation of electromyography for hand gesture detection using micro accelerometer. In Proceedings of the Artificial Intelligence and Evolutionary Computations in Engineering Systems 2016, Chennai, Tamilnadu, India, 19–21 May 2016; pp. 357–364. [Google Scholar]
- Google, Project Soli. 2015. Available online: atap.google.com/soli (accessed on 26 May 2021).
- Smith, J.; White, T.; Dodge, C.; Paradiso, J.; Gershenfeld, N.; Allport, D. Electric field sensing for graphical interfaces. IEEE Comput. Graph. Appl. 1998, 18, 54–60. [Google Scholar] [CrossRef]
- Adib, F.; Katabi, D. See through walls with WiFi! In Proceedings of the ACM SIGCOMM 2013 Conference, Hong Kong, China, 12–16 August 2013; pp. 75–86. [Google Scholar]
- Adib, F.; Kabelac, Z.; Katabi, D.; Miller, R.C. 3d tracking via body radio reflections. In Proceedings of the 11th USENIX Symposium on Networked Systems Design and Implementation (NSDI 14), Seattle, WA, USA, 2–4 April 2014. [Google Scholar]
- Adib, F.; Hsu, C.Y.; Mao, H.; Katabi, D.; Durand, F. Capturing the human figure through a wall. ACM Trans. Graph. 2015, 6, 1–3. [Google Scholar] [CrossRef]
- Ye, M.; Wang, X.; Yang, R.; Ren, L.; Pollefeys, M. Accurate 3d pose estimation from a single depth image. In Proceedings of the 2011 International Conference on Computer Vision, Barcelona, Spain, 6–13 November 2011; pp. 731–738. [Google Scholar]
- Peterson, L.E. K-nearest neighbor. Scholarpedia 2009, 2, 1883. [Google Scholar] [CrossRef]
- Muja, M.; Lowe, D.G. Fast approximate nearest neighbors with automatic algorithm configuration. VISAPP 2009, 2, 331–340. [Google Scholar]
- Wilson, A.D.; Bobick, A.F. Parametric hidden markov models for gesture recognition. IEEE Trans. Pattern Anal. Mach. Intell. 1999, 9, 884–900. [Google Scholar] [CrossRef]
- Wilson, A.D.; Bobick, A.F. Hidden Markov models for modeling and recognizing gesture under variation. Int. J. Pattern Recognit. Artif. Intell. 2001, 1, 123–160. [Google Scholar] [CrossRef]
- Hearst, M.A.; Dumais, S.T.; Osuna, E.; Platt, J.; Scholkopf, B. Support vector machines. IEEE Intell. Syst. Their Appl. 1998, 4, 18–28. [Google Scholar] [CrossRef]
- Patsadu, O.; Nukoolkit, C.; Watanapa, B. Human gesture recognition using Kinect camera. In Proceedings of the 2012 International Conference on Computer Science and Software Engineering (JCSSE), Bangkok, Thailand, 30 May–1 June 2012; pp. 28–32. [Google Scholar]
- Feng, K.P.; Yuan, F. Static hand gesture recognition based on HOG characters and support vector machines. In Proceedings of the 2nd International Symposium on Instrumentation and Measurement, Sensor Network and Automation (IMSNA), Toronto, ON, Canada, 23–24 December 2013; pp. 936–938. [Google Scholar]
- Ghimire, D.; Lee, J. Geometric feature-based facial expression recognition in image sequences using multi-class adaboost and support vector machines. Sensors 2013, 6, 7714–7734. [Google Scholar] [CrossRef] [PubMed]
- Haykin, S. Neural Networks and Learning Machines; Prentice Hall: New York, NY, USA, 2009. [Google Scholar]
- Maung, T.H. Real-time hand tracking and gesture recognition system using neural networks. World Acad. Sci. Eng. Technol. 2009, 50, 466–470. [Google Scholar]
- D’Orazio, T.; Attolico, G.; Cicirelli, G.; Guaragnella, C. A Neural Network Approach for Human Gesture Recognition with a Kinect Sensor. In Proceedings of the ICPRAM, Anger, France, 6–8 March 2014. [Google Scholar]
- Hinton, G.; LeCun, Y.; Bengio, Y. Deep learning. Nature 2015, 7553, 436–444. [Google Scholar]
- Cao, Z.; Hidalgo, G.; Simon, T.; Wei, S.E.; Sheikh, Y. OpenPose: Realtime multi-person 2D pose estimation using Part Affinity Fields. IEEE Trans. Pattern Anal. Mach. Intell. 2019, 43, 172–186. [Google Scholar] [CrossRef]
- Sowards, S.W. What is Peer Review, and Does it Have a Future? Bibl. Forsch. Prax. 2015, 39, 200–205. [Google Scholar] [CrossRef]
- AAL Forum—Ageing Well in the Digital World. Available online: http://www.aal-europe.eu/aal-forum/ (accessed on 7 April 2021).
- Hayden, E.C. How to beat HIV. Nat. News 2015, 7559, 146. [Google Scholar] [CrossRef] [PubMed]




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| # | Title | Year | Cognitive Function as Primary Clinical Outcome | Interaction | Automatic Quantification of Cognitive Performance | Support Tools and Clinical Information Integration | Environment |
|---|---|---|---|---|---|---|---|
| [51] | Effects of Kinect adventures games versus conventional physical therapy on postural control in elderly people: a randomized controlled trial. | 2018 | No | Body movement | No | No | Clinical setting |
| [52] | Socially assistive robotics: Robot exercise trainer for older adults. | 2018 | No | Body movement | No | No | At home |
| [53] | Cognitive-motor exergaming for reducing fall risk in people with chronic stroke: A randomized controlled trial. | 2019 | No | Body movement | No | No | Clinical setting |
| [54] | Effect of cognitive-only and cognitive-motor training on preventing falls. in community-dwelling older people: protocol for the smart±step randomized controlled trial. | 2019 | No | Feet movement | No | No | Clinical setting and at home |
| [55] | A social virtual reality-based application for the physical and cognitive training of the elderly at home. | 2019 | No | Leg movement | No | No | Clinical setting and at home |
| [56] | Cognitive system framework for brain-training exercise based on human-robot interaction. | 2019 | Yes | No | No | No | Clinical setting |
| [3] | Design, development, and testing of an app for dual-task assessment and Training regarding cognitive-motor interference (CMI-APP) in people with multiple sclerosis: multicenter pilot study. | 2020 | Yes | No | No | No | Clinical setting |
| [57] | Cognitive training using fully immersive, enriched environment virtual reality for patients with mild cognitive impairment and mild dementia: Feasibility and usability study. | 2020 | Yes | Body movement | No | No | Clinical setting |
| [58] | Beneficial effects of interactive physical-cognitive game-based training on fall risk and cognitive performance of older adults. | 2020 | No | Body movement | No | No | Clinical setting and at home |
| [59] | Novel mat exergaming to improve the physical performance, cognitive function, and dual-task walking and decrease the fall risk of community-dwelling older adults. | 2020 | No | Body movement | No | No | At home |
| [60] | Effects of an in-home multicomponent exergame training on physical functions, cognition, and brain volume of older adults: A randomized controlled trial. | 2020 | No | Body movement | No | No | At home |
| [61] | Can robotic gait rehabilitation plus virtual reality affect cognitive and behavioral outcomes in patients with chronic stroke? A randomized controlled trial involving three different protocols. | 2020 | Yes | No | No | No | Clinical setting |
| [62] | An exergame for cognitive inhibition training. | 2021 | Yes | Body movement | No | No | At home |
| [63] | The efficacy of exergaming in people with major neurocognitive disorder residing in long-term care facilities: a pilot randomized controlled trial. | 2021 | No | Feet movement | No | No | Clinical setting |
| [64] | Dual-task exercise to improve cognition and functional capacity of healthy older adults. | 2021 | Yes | No | No | No | Clinical setting |
| [65] | Effects of virtual reality vs conventional balance training on balance and falls in people with multiple sclerosis: a randomized controlled trial. | 2021 | No | Body movement | No | No | At home |
| CogniViTra | Yes | Body movement | Yes | Yes | Clinical setting and at home |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quintas, J.; Pais, J.; Martins, A.I.; Santos, H.; Neves, L.; Sousa, S.; Benhsain, D.; Dierick, F.; Callén, A.; Cunha, A.; et al. CogniViTra, a Digital Solution to Support Dual-Task Rehabilitation Training. Electronics 2021, 10, 1304. https://doi.org/10.3390/electronics10111304
Quintas J, Pais J, Martins AI, Santos H, Neves L, Sousa S, Benhsain D, Dierick F, Callén A, Cunha A, et al. CogniViTra, a Digital Solution to Support Dual-Task Rehabilitation Training. Electronics. 2021; 10(11):1304. https://doi.org/10.3390/electronics10111304
Chicago/Turabian StyleQuintas, João, Joana Pais, Ana Isabel Martins, Hugo Santos, Lúcia Neves, Sérgio Sousa, David Benhsain, Frédéric Dierick, Antonio Callén, António Cunha, and et al. 2021. "CogniViTra, a Digital Solution to Support Dual-Task Rehabilitation Training" Electronics 10, no. 11: 1304. https://doi.org/10.3390/electronics10111304
APA StyleQuintas, J., Pais, J., Martins, A. I., Santos, H., Neves, L., Sousa, S., Benhsain, D., Dierick, F., Callén, A., Cunha, A., Rocha, N. P., & Cruz, V. T. (2021). CogniViTra, a Digital Solution to Support Dual-Task Rehabilitation Training. Electronics, 10(11), 1304. https://doi.org/10.3390/electronics10111304