1. Introduction
Actinic keratoses (AKs) are one of the more common premalignant cutaneous lesions, clinically present as erythematous, hyperkeratotic macules, papules or plaques typically occurring in chronically sun-exposed skin, such as the face, lower lip, scalp, ears, neck, forearms, hands and lower legs. AKs can occur as a single lesion or, more frequently, as multiple, appearing on a chronically photodamaged area, or field cancerization. The concept of field cancerization describes the presence of genetic abnormalities in a tissue chronically exposed to a carcinogen (e.g., ultraviolet radiations light exposure) [
1]. These abnormalities are responsible for the presence of multilocular clinical and sub-clinical (nonvisible, nonpalpable) cancerous lesions that explains the increased risks of multiple cancers in this area. AKs and squamous cell carcinomas (SCCs) exist in field cancerization on a continuum from subclinical keratinocyte dysplasia to invasive SCC, so AK have been histologically classified as cutaneous SCC
in situ [
2]. Optimal management of field cancerization focused on the treatment of large areas, without too much discomfort and with a good cosmetics outcome. Among them, topical photodynamic therapy (PDT) with methyl aminolevulinate (MAL) has proven to be effective, non-invasive and with better cosmetic results for AKs [
3].
The diagnosis of AKs and the clinical response to PDT are generally based on clinical examination; however, if clinical inspection is uncertain or invasive SCC is suspected, repeated biopsies for histological evaluations are needed. However, in this way, are lost the major clinical advantages of PDT: lack of invasiveness and optical cosmetic results.
In vivo reflectance confocal microscopy (RCM) is a non-invasive tool for real-time imaging of epidermis and superficial dermis
in vivo, generating horizontal skin sections at high resolution close to conventional histology. RCM has been previously reported to facilitate the
in vivo evaluation of several pigmented and non-pigmented skin lesions, including AKs [
4,
5,
6], as first described by Aghassi and co-workers [
7].
The aim of this study was to investigate the use of in vivo RCM in the assessment of the response of AKs treated with MAL-PDT.
2. Experimental Section
2.1. Patients
A total of 10 biopsy-proven non-hyperkeratotic AKs in 10 consecutive outpatients were enrolled in the present study.
The study was approved by the local ethics committee and all subjects gave written informed consent prior to entry.
2.2. Treatment Protocol
All AKs were first prepared with a gentle, bloodless debridement with a curette aiming only to remove crusts and scales [
8]. Then, a 1 mm thick layer of a cream containing 160 mg g
−1 MAL (Metvix cream
®, Galderma, France) was applied under an occlusive and opaque dressing. Three hours later the cream was removed and the red fluorescence of porphyrins was visualized with a Wood’s light before exposure to 37 J cm
−2 of red (635 ± 18 nm) light from a LED source (Aktilite CL128
®, PhotoCure ASA, Oslo, Norway) with an irradiance of 86 mW cm
−2 at skin level, as measured with a Macam SR 9910 spectroradiometer (MACAM Photometrics, Livingston, UK). All lesions received two treatment sessions 7 days apart.
At a follow-up visit after three months, treated skin were examined clinically and by confocal reflectance microscopy. A 3 mm punch biopsy was taken from all treated areas and it was orientated by clinical and confocal examinations.
2.3. In Vivo Reflectance Confocal Microscopy (RCM)
RCM investigation was performed with a Vivascope 1500® (MAVIG GmbH, Munich, Lucid-Tech Inc., Henrietta, NY, USA) microscopy.
Details of this technique and the device have been previously published [
9].
Each skin lesions were systematically evaluated by RCM: one X–Y horizontal mapping (4 × 4-mm, called “mosaic”) was performed at each epidermal layer beginning with the stratum corneum through the entire epidermis and until the papillary dermis (maximal depth of imaging: 200–250 µm).
Based on previously defined RCM criteria, each lesion was evaluated for the presence or absence of RCM features of AK [
6,
10]: disruption of the stratum corneum, individual corneocytes, hyperkeratosis and parakeratosis, overall architectural disarray, keratinocyte with nuclear atypia and cellular pleomorphism at the level of the basal, spinous and granular layer. Other features were spongiosis, exocytosis, solar elastosis, increased vascularity or blood vessel dilatationand superficial inflammatory infiltrate.
Imaging with in vivo RCM was performed before MAL-PDT to confirm the diagnosis of AK and after 3 months to evaluate the response to treatment.
2.4. Histopathologic Examination
Punch biopsies was taken from all lesions suspected for AK upon clinical and RCM evaluation before treatment and 3 months after PDT for histopathologic examination. After fixation with formalin, a correlation of hematoxylin-and eosin (H&E)-stained histologic vertical sections was made with the corresponding en face horizontal confocal images.
3. Results and Discussion
Ten Caucasian patients (2 females and 8 males, age ranging between 67 and 82 years) with 10 biopsy-proven AKs were enrolled. Patients presented AKs located on the face (2 AKs) or head (8 AKs).
All lesions showed clinical feature of non-hyperkeratotic AK and presented upon confocal examination the above-mentioned criteria for in vivo confocal diagnosis of AK.
At 3 months follow-up, a complete response (total disappearance of AK features) was observed by clinical examination in 9 out of 10 lesions and a partial clinical response (persistence of AK features) in 1 lesion.
In vivo RCM examination identified 3 months after PDT complete response in 7 lesions (
Figure 1) and partial response in 3 out of 10 lesions, detecting 2 residual AKs in subclinical form, missed by clinical examination (
Figure 2) presented as stratum corneum disruption with individual corneocytes and parakeratosis, architectural disarray with pleomorphism of keratinocytes and loss of cell-to-cell demarcation in stratum granulosum/spinosum and dilatated blood vessels containing blood cells in superficial dermal layer. Histologic analysis confirmed these results (
Figure 1 and
Figure 2). All results have been summarized in
Table 1.
Figure 1.
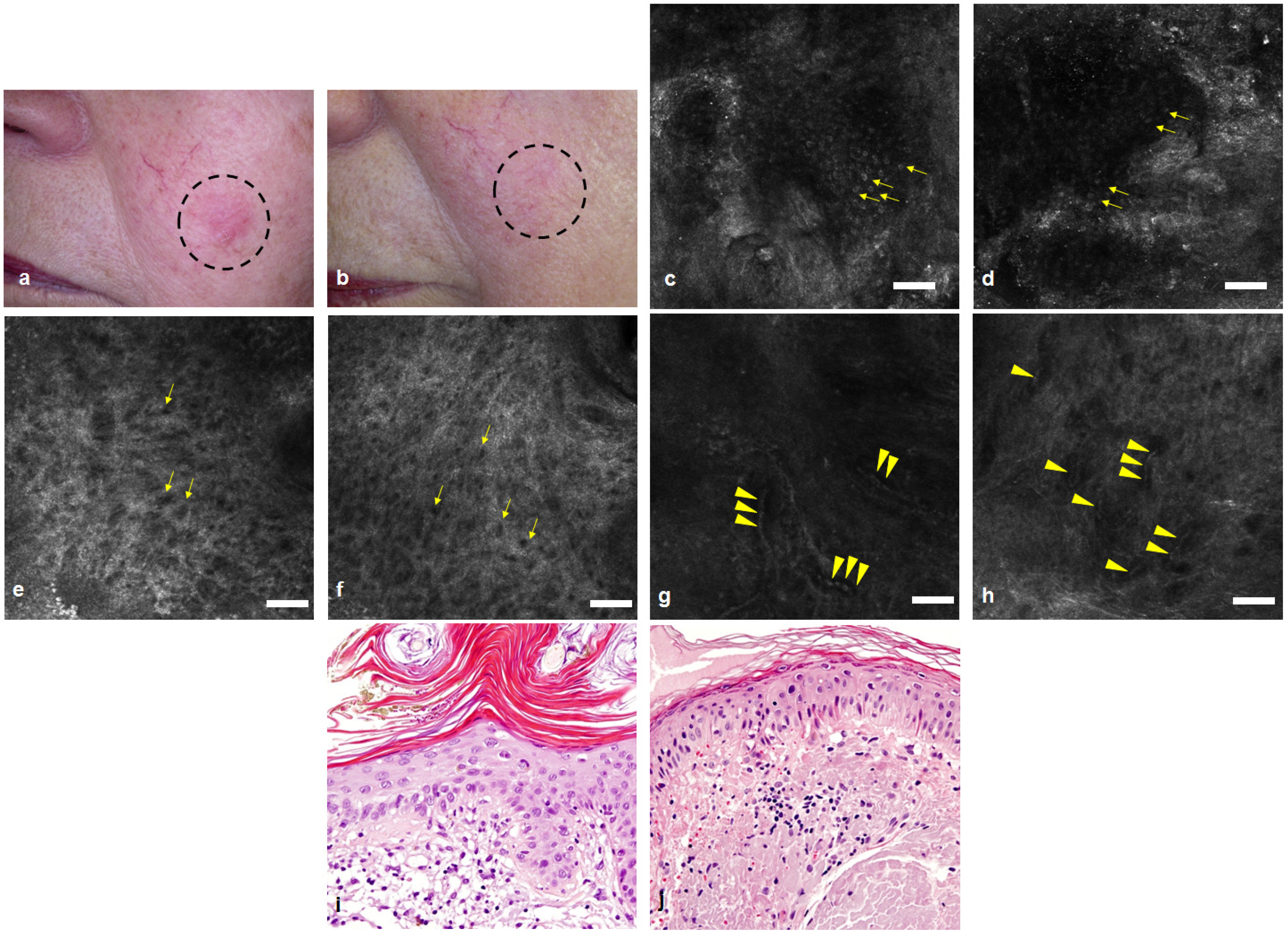
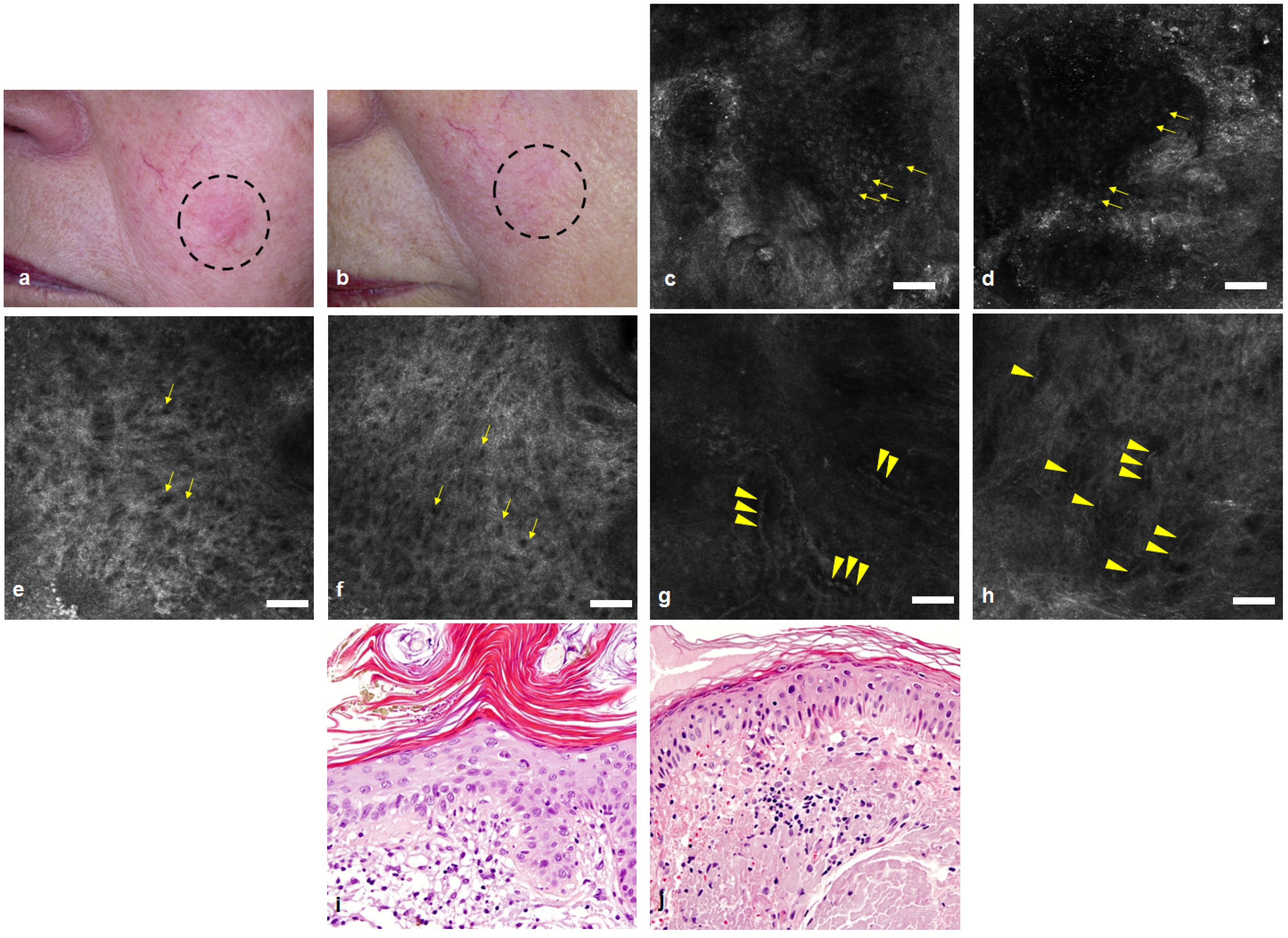
Actinic keratoses (AK) before (a) and three months after (MAL-PDT) (b): clinical examination shows complete response; In vivo reflectance confocal microscopy (RCM) images before MAL-PDT show stratum corneum disruption with detached corneocytes and parakeratosis (arrows) (c), architectural disarray with pleomorphism of keratinocytes (arrows) in stratum granulosum/spinosum (e) and thickened, moderately refractile fibres in the superficial dermal layer (g) representative of solar elastosis (arrows); After MAL-PDT we observe in RCM a recovery of stratum corneum with large anuclear polygonal cells (arrows) (d), restoration of normal honeycomb patter in the stratum granulosum/spinosum (f), but persistence of solar elastosis (arrows) in the upper dermis (h) (Scale bar: 50 µm). Corresponding histology confirms presence of parakeratosis, hyperkeratosis, pleomorphism of keratinocytes and solar elastosis pre-treatment (i) and normal epidermis with persistence of solar elastosis post-treatment (j) (Hematoxylin-eosin stain; original magnification: 200×).
Figure 1.
Actinic keratoses (AK) before (a) and three months after (MAL-PDT) (b): clinical examination shows complete response; In vivo reflectance confocal microscopy (RCM) images before MAL-PDT show stratum corneum disruption with detached corneocytes and parakeratosis (arrows) (c), architectural disarray with pleomorphism of keratinocytes (arrows) in stratum granulosum/spinosum (e) and thickened, moderately refractile fibres in the superficial dermal layer (g) representative of solar elastosis (arrows); After MAL-PDT we observe in RCM a recovery of stratum corneum with large anuclear polygonal cells (arrows) (d), restoration of normal honeycomb patter in the stratum granulosum/spinosum (f), but persistence of solar elastosis (arrows) in the upper dermis (h) (Scale bar: 50 µm). Corresponding histology confirms presence of parakeratosis, hyperkeratosis, pleomorphism of keratinocytes and solar elastosis pre-treatment (i) and normal epidermis with persistence of solar elastosis post-treatment (j) (Hematoxylin-eosin stain; original magnification: 200×).
![Cosmetics 01 00037 g001]()
Table 1.
Evaluation of response of AKs to MAL-PDT by clinical examination, in vivo RCM and histology at 3 months after the treatment.
Table 1.
Evaluation of response of AKs to MAL-PDT by clinical examination, in vivo RCM and histology at 3 months after the treatment.
| Response of AKs to MAL-PDT | Clinical examination | In vivo RCM | Histology |
|---|
| Complete response | 9 | 7 | 7 |
| Partial response/Treatment failure | 1 | 3 | 3 |
Figure 2.
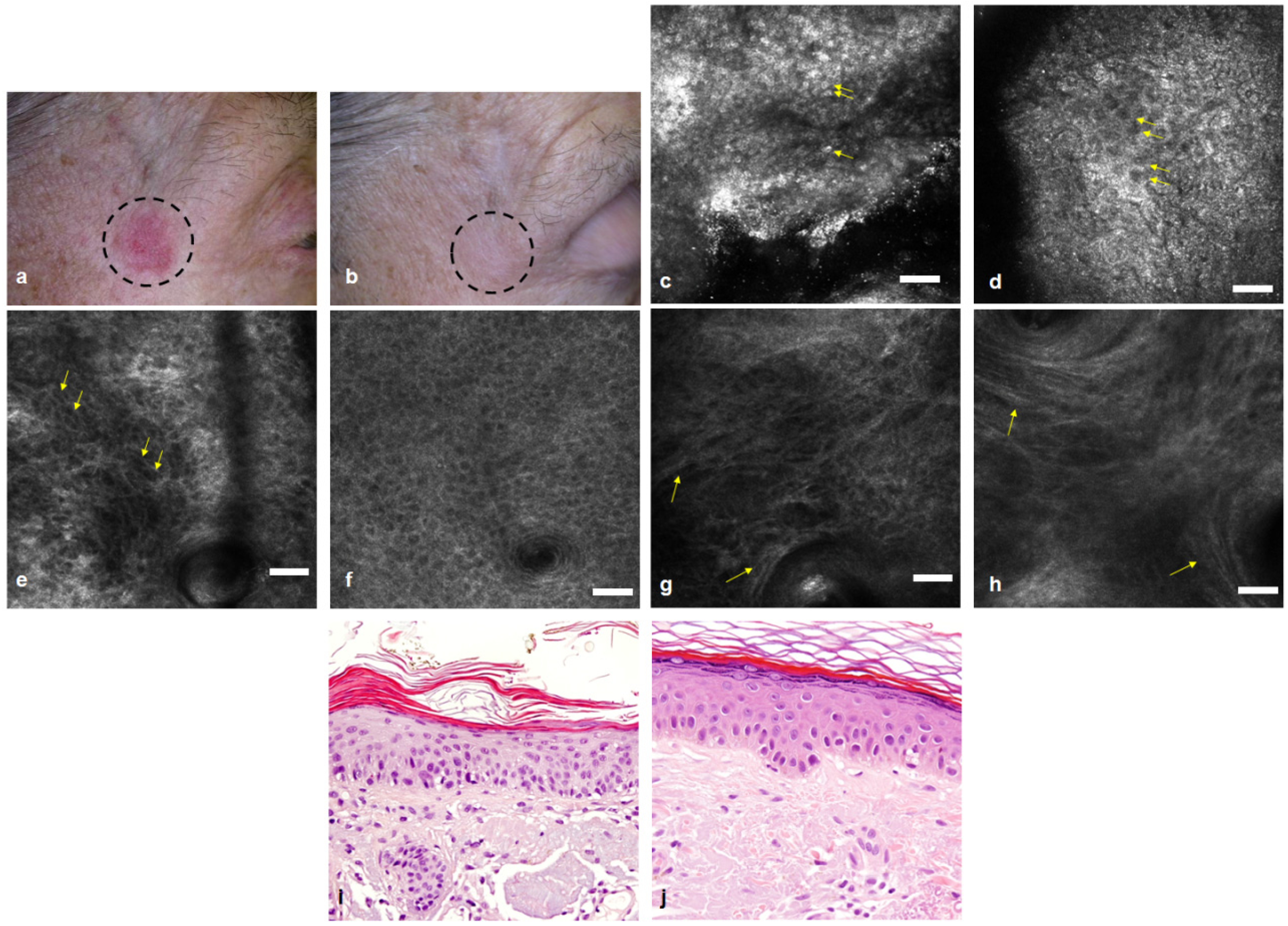
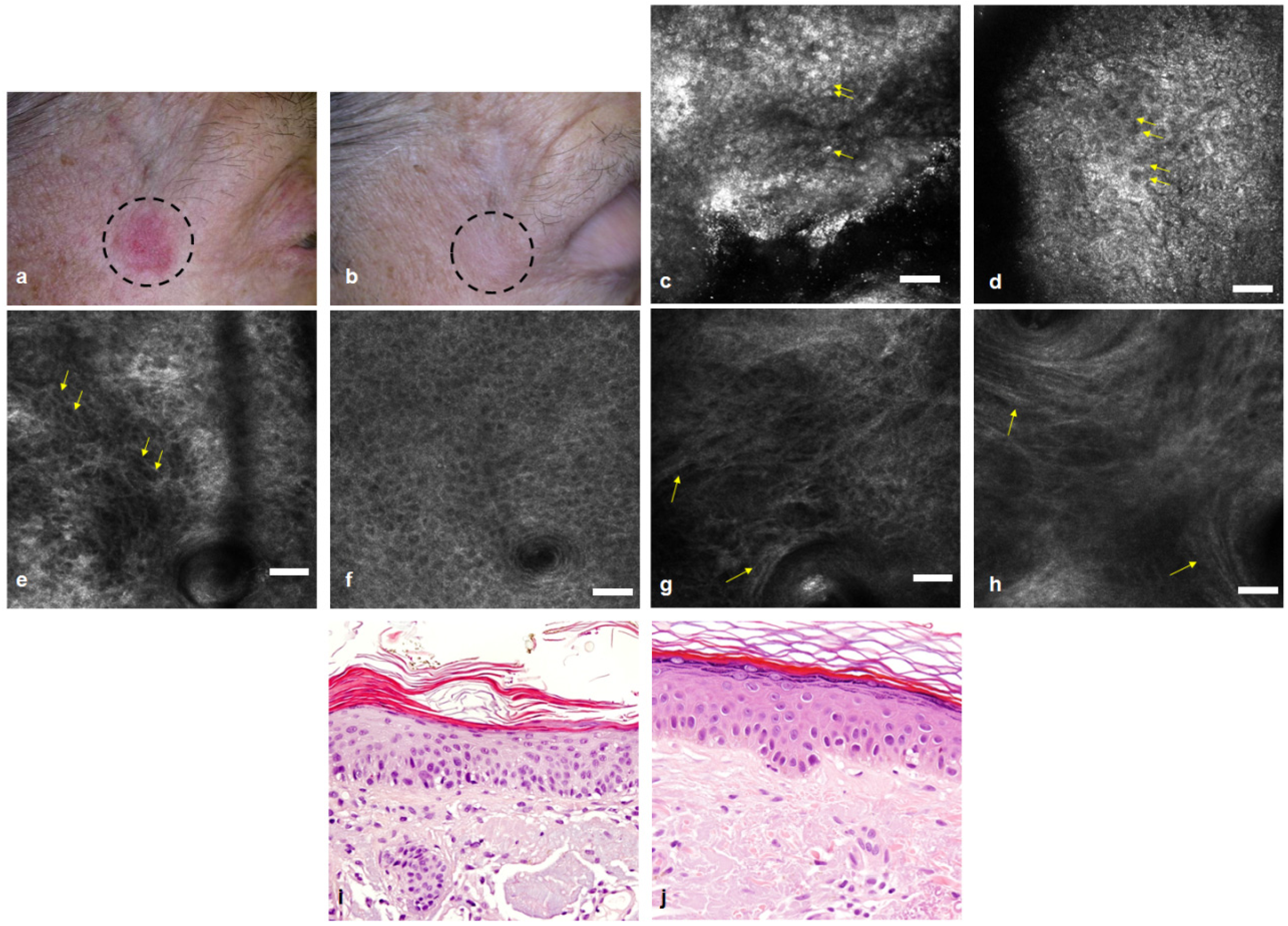
AK before (a) and three months after MAL-PDT (b): clinical examination shows complete response; In vivo RCM images before MAL-PDT show stratum corneum disruption with individual corneocytes and parakeratosis (arrows) (c), architectural disarray with pleomorphism of keratinocytes and loss of cell-to-cell demarcation (arrows) in stratum granulosum/spinosum (e) and dilatated blood vessels (arrowheads) containing refractile blood cells in superficial dermal layer (g); After MAL-PDT we observed in RCM persistence of all criteria for AK diagnosis in all layers (d,f,h) (arrows and arrowheads) (Scale bar: 50 µm). Corresponding histology confirms persistence of all criteria for AK diagnosis before (i) and after (j) MAL-PDT (Hematoxylin-eosin stain; original magnification: 200×).
Figure 2.
AK before (a) and three months after MAL-PDT (b): clinical examination shows complete response; In vivo RCM images before MAL-PDT show stratum corneum disruption with individual corneocytes and parakeratosis (arrows) (c), architectural disarray with pleomorphism of keratinocytes and loss of cell-to-cell demarcation (arrows) in stratum granulosum/spinosum (e) and dilatated blood vessels (arrowheads) containing refractile blood cells in superficial dermal layer (g); After MAL-PDT we observed in RCM persistence of all criteria for AK diagnosis in all layers (d,f,h) (arrows and arrowheads) (Scale bar: 50 µm). Corresponding histology confirms persistence of all criteria for AK diagnosis before (i) and after (j) MAL-PDT (Hematoxylin-eosin stain; original magnification: 200×).
The three recurrent AKs were treated with another MAL-PDT treatment cycle.
All patients were followed up for at least 12 months and further recurrences were not registered.
The diagnosis of AKs is generally based on clinical inspection, however if recurrences or progression in SCC are suspected, biopsy with histopathologic examination are needed.
Among the non-invasive imaging technologies available, in order to increase diagnostic accuracy for AKs, recent studies reported high sensitivity and specificity rated for diagnosis of AKs by
in vivo RCM [
5,
11].
The applicability of RCM to evaluate the response of AKs to non-invasive, topical treatment modalities has been previously reported in a small group of patients with subclinical features of AK treated by imiquimod [
10]. Another study compared the effect of imiquimod and 5-ALA PDT in AK in organ transplantation patients who have a high prevalence of AKs and the authors demonstrated that RCM was an excellent tool to monitor the response in both cases [
12]. In agreement with these results the present study suggests that RCM was able to identify AKs, even in a very early sub-clinical stage, and to assess the response of AKs treated with MAL-PDT.
RCM detected residual AKs in two patients after PDT avoiding false negative findings of clinical examination.
There was a complete concordance of RCM findings with histological results, but, unlike histology, RCM has some advantages: it is not invasive (avoiding pain and scar formation from repeated biopsies) and can provide results in real time.
However because of limitations in optical resolution and penetration of this imaging technology, RCM wouldn’t be used for evaluation of hyperkeratotic AKs and SCC with hyperkeratosis or with invasion into the dermis more that 250 µm. Furthermore RCM is user-dependent and it needs to long time for image acquisition in wide anatomic areas.
4. Conclusions
In conclusion, in vivo RCM may be a promising, alternative tool for the non-invasive diagnosis of AKs and evaluation of AKs response to non-invasive treatments, as MAL-PDT. This approach has two main advantages: early treatment of relapses at the subclinical state and preservation of good cosmetic outcomes obtained with MAL-PDT, without the disadvantages of repeated invasive skin biopsies and conventional histology.
In addition, RCM might increase our insights into the mechanism of action of PDT, visualizing in vivo and in real-time the cellular modifications at the base of photodynamic process.
Finally, further investigations are needed to clarify if RCM may be useful also in the follow-up of field cancerization, decreasing recurrence rates of AKs and reducing the risk of eventually progression into invasive SCC.


{kind=link}
{kind=link}