Abstract
Safe access to drinking water and sanitation is a human right and a key goal of sustainable development, which must also be achieved in rural areas. This work proposes and simulates the application of a conceptual model for a basic sanitation safety plan tailored for rural areas, called the Rural Basic Sanitation Safety Plan (RBSSP). The methodology includes technical and scientific review approaches, followed by consultation with specialists through the Delphi method and simulation in a case study. The RBSSP framework includes six fundamental principles, six steps, and twenty actions to be performed. In the case study, the final conceptual model application was simulated for a rural settlement scenario, which led to significant changes in the actions, subdivisions and phases. Key findings highlight that community participation, involvement and empowerment are the most relevant factors for successful implementation. The necessary tools for RBSSP preparation, such as risk assessment methodologies and management plans, must be applied considering the scenario. Finally, after simulating the conceptual model, we conclude that it is necessary to adapt actions and apply methods and techniques developed and appropriate for rural areas to develop an effective RBSSP for each specific scenario.
1. Introduction
In addition to the objectives set for SDG 6, each country has its own targets. In Brazil, it is estimated that 5.5 million people live without water supply, and 58.4 million without safely managed sewage services [1]. It was established, as a national goal, that contracts for public for water and sewage services should include reaching 99% of the population with potable water and 90% with sewage collection and treatment by 2033 [2].
Evidence indicates the impact of sewage, solid waste management, and rainwater systems [3,4,5] on water quality for human consumption and population health. However, the literature often fails to address these systems as part of an integrated planning approach, particularly concerning safe management. In Brazil, potable water supply, sewage, solid waste and rainwater management constitute integral components of the overarching concept of basic sanitation, each requiring equal attention and adequate provision. Its inadequacy and insecurity, especially in rural areas, impacts population health status [6,7] since it is one of the main social determinants of health [8].
Safety plans are tools that aim to provide both management and operation of water supply (WSS) and sewage (SSS) systems in a safe way, based on risk management assessments, and have been applied around the world [3,9,10]. These tools have been separately applied in rural areas in order to achieve infrastructure and other low cost improvements [4,11,12], especially regarding safety measures [13,14,15], associating the reduction in health risks with water management systems’ improvement. The steps of Water Safety Plans (WSP) and Sanitation Safety Plans (SSP) include diagnostic stages, health risks assessment in populations exposed and management and improvement plans [14,16,17]. Both approaches divide into preparation, system assessment, operational monitoring, management, communication, and feedback steps. In addition to the previously mentioned steps, the scope of the WSP is limited to drinking water, covering the entire process from the catchment area (basin) to the tap. The WSP framework includes the public health context and health outcomes, health-based targets, the plan itself, and surveillance actions [13,14,15,16]. The SSP differs from the WSP in its scope, which encompasses the management of excreta. The SSP covers the entire process from the household where the sewage is produced to its final disposal [6,13,14,15,16]. Furthermore, both frameworks have been implemented since their development, and there is evidence suggesting that they provide advantages for the population and water suppliers [18,19].
However, rural areas require process simplification and the provision of comprehensive support to small communities, particularly from an educational standpoint [4,18]. In addition, rural areas may experience reduced risks by addressing all four components of basic sanitation together, rather than relying on a single WSP or SSP. These tools must be adapted to each local context when they are designed and implemented, and also legislation and established targets [14,16,19]. Recent advances show that safety plans can serve as effective tools for managing potential hazards and prioritizing investments, even in small systems [20,21,22].
In this context, significant research gaps exist regarding the adaptation of methodologies to the characteristics of any rural environment, as well as the need for an integrated approach to all components of basic sanitation in an integrated way: water supply, sewage, solid waste management and rainwater management. The literature usually focuses on adaptation for specific rural community typologies [4,5,7,11,18]. Additionally, case studies usually address either water supply or sanitation services independently, which do not consider all four components and their risks in the same community [3,4,5,10,11,18,20,21]. Thus, the objective of this work was to propose and simulate the implementation of a conceptual model for the Rural Basic Sanitation Safety Plan (RBSSP), tailored specially for rural areas.
2. Materials and Methods
This research posits the CMRBSSP, encompassing four basic sanitation components: potable water supply services, sanitary sewage, urban cleaning, and solid waste and drainage/rainwater management. Its development (Figure 1) progressed through three phases: (1) searching and reviewing technical and scientific documents to support WSP and/or SSP preparation and implementation; (2) proposing an initial conceptual model of the RBSSP (ICMRBSSP); and (3) consulting specialists via the Delphi method to refine the developed CMRBSSP, which was divided into two phases. Subsequently, the CMRBSSP was applied in a rural community.
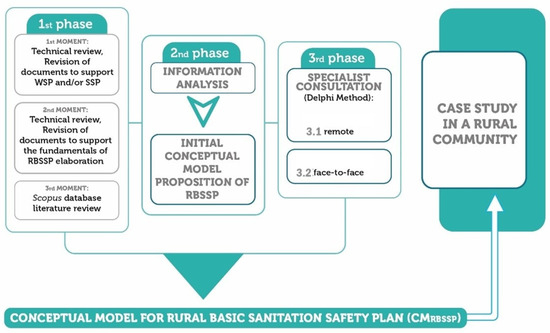
Figure 1.
Development phases flowchart for a Conceptual Model for Rural Basic Sanitation Safety Plan (CMRBSSP).
2.1. RBSSP Conceptual Model (CMRBSSP)
2.1.1. First phase
In phase 1.1, a survey of technical documents was applied according to the literature [23,24,25]. This survey was produced by the WHO to support WSP and/or SSP preparation. Then, descriptive analysis using data from the survey was executed to identify the main safety plans steps and elements, as well as the quantitative evaluation of their citations on the Google Scholar platform.
In phase 1.2, a search for technical documents, regulations and public policies with guidelines related to basic sanitation in rural areas and risk management was conducted. A listing of fundamental guiding services’ provision and contributions to the preparation of safety plans based on selected materials was also created. Finally, in phase 1.3, the scientific literature was reviewed, such being the method adopted for frameworks and conceptual model preparation in [24,26,27,28,29]. Scientific articles were obtained from the Scopus database, applying different descriptor combinations as follows: “safety plan” OR “security plan” AND “small communities” OR rural AND water OR sanitation in title, abstract and keywords and selection of filters “Articles” and “Language: English and Portuguese”.
After reading the title and abstract, some scientific papers were excluded for the following reasons: (i) did not deal with WSP or SSP preparation or support its preparation; (ii) did not explain the method or technique used to elaborate or support the preparation of WSP or SSP; (iii) only mentioned the words WSP or SSP without emphasis on them; or (iv) were not analyzed by peers.
The scientific papers included were those which explained the methodology for preparing the WSP and SSP or other methods that collaborated in this process, as well as their adaptations. Thus, the information obtained from these papers, as well as the number of citations, were extracted upon verification of the subject’s relevance.
Data registered in phase 1 supported the next phase, regarding the identification of fundamental principles and the necessary steps for ICMRBSSP.
2.1.2. Second Phase
The analysis of the information obtained in the previous phase was executed, including the WSP and SSP stages’ relevant fundaments extracted from the gray literature and methodologies adopted by the scientific literature, and an initial proposal for the CMRBSSP was built, consisting of the following items:
- Fundamental principles that will be the basis for plan preparation;
- RBSSP steps, which will demonstrate their logical sequence;
- Objective that will explain the purpose of the each stage;
- List of actions with activity sequence, and how they should be performed in order to achieve the objective;
- Instruments that will be used to perform the listed actions;
- Products that must be obtained at each stage end of RBSSP;
- Implementation of a summary figure, instrument used to facilitate the visualization of the steps, and the general structure of the RBSSP.
2.1.3. Third Phase
This phase, performed in two sections (remotely and in person), was the specialists’ consultation using the Delphi method, aimed at constructing frameworks and conceptual models [23,24,27].
In phase 3.1, an individual survey was elaborated with the CMRBSSP initial proposal (Supplementary Materials, Tables S1–S3) to be submitted for analysis and contributions. Then, 16 specialists trained and with enough experience regarding basic sanitation, rural areas, WSP and specificities of the Brazilian regions received, by e-mail, individual questionnaires. Thus, using these surveys, they were able to evaluate ICMRBSSP topics (fundamental principles, stages, actions, among others). In addition to objective responses, they could register any comments on each evaluated item.
Phase 3.2 was accomplished in person and, for this reason (which implied travel costs and time availability), only eight specialists, who participated in phase 3.1, were able to attend. The items that built the ICMRBSSP (listed in the second phase) were discussed among the specialists until consensus was reached, contemplating the following dynamics: (i) presentation, or initial round, of discussion topics, including results and contributions obtained in phase 3.1; (ii) compilation of contributions and the presentation of a new proposal; (iii) discussion round with new contributions added, followed by the compilation of information; (iv) continuous repetition of Item “iii” until a consensus of the results was reached; and (v) building a Conceptual Model for RBSSP (CMRBSSP).
2.2. Case Study
In order to verify the possible difficulties encountered during the application of CMRBSSP, a simulation was implemented in a rural community in the Brazilian state of Goiás. The community was chosen based on the existence of basic sanitation infrastructure, both collective and individual, water supply, sanitary sewage solutions, solid waste management and rainwater, regardless of its scope. This happened among the communities contemplated on the Sanitation and Environmental Health Project in Rural and Traditional Communities of Goiás (SanRural), in a partnership between the Federal University of Goiás (UFG) and the National Health Foundation (FUNASA). Thus, the João de Deus agrarian reform settlement was chosen (Figure 2), located in the Silvânia municipality, Goiás, Brazil, where its technical–participatory diagnosis was used [30], and where the necessary data for ICMRBSSP simulation application were found. João de Deus is a community with a population of 58 people. The water supply for 63.7% of the population comes from drilled wells (from both unconfined and confined aquifers). For the remaining 36.3%, the water supply is supplemented by springs and surface water as secondary sources. Most of the population (90.9%) collects water within their own dwellings. The water quality is classified as marginal, primarily due to the presence of Escherichia coli and heterotrophic bacteria exceeding potability standards. There is no water treatment system in place. Sewage management is limited since 90.9% of the population uses rudimentary tanks for sewage disposal. Furthermore, 81.8% of the waste is burned, and there is no infrastructure for rainwater drainage [30].
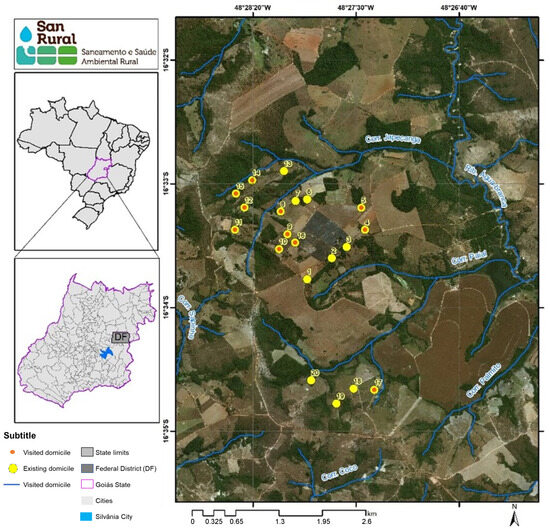
Figure 2.
João de Deus agrarian reform settlement location [30].
During the simulation, each step application and where their respective actions should occur was evaluated, with all results registered in a spreadsheet for comparison purposes with the CMRBSSP proposed, identifying aspects that could be adapted and/or improved. For CMRBSSP simulation stages, it was necessary to define which techniques and tools were to be used. Thus, the methodology proposed by Bezerra et al. [31] and, for individual ones, the rural sanitation safety index developed by Scalize et al. [32] were chosen.
As a simulation, this compound does not present the detailed results for CMRBSSP application, but instead shows the difficulties encountered and the adaptations/improvements necessary for a more proper application, and the local reality was taken into consideration.
3. Results
3.1. RBSSP Conceptual Model (CMRBSSP)
3.1.1. First Phase
Safety plans were recommended and proposed by the WHO, in first place, which produced manuals to support the implementation of said plans. Thus, these documents and those processed in phase 1.2, which impact or guide goals, actions and plans related to basic sanitation, were considered and analyzed. Table 1 lists the compilation of selected documents, their application area and the assumptions supporting the preparation of safety plans, including their application area and their quantity of Google Scholar citations, when applicable. Among the eleven documents, four refer to the WSP, two to the SSP and one document to each of the following topics: risk management; basic sanitation in rural areas; basic sanitation legislation; and health legislation and drinking water regulations. All were used to extract assumptions that could form the foundations of the RBSSP.

Table 1.
Relevant documents for security plans implementation at first and second moments of first phase, application area, citations and assumptions that guide the documents.
Based on the listed assumptions (Table 1), linking them to basic sanitation components and framework elements (Table 2), six guiding fundamental principles were formulated to compose the CMRBSSP, (1) risk management; (2) education and social participation; (3) reality-suited technologies; (4) multiple barriers; (5) expanded health concept; and (6) all federal basic sanitation policy principles in Brazil, enabling a comparison with the answers of specialists. For application in countries without basic sanitation policies, the sixth CMRBSSP principle must be adapted to local legislation.
Table 2.
Types of safety plans, their steps and elements of their respective frameworks.
Since the release of the WHO manuals in 2009 [16], some safety plans have been implemented and, until 2017, at least 93 countries had at least one experience implementing WSP in communities, towns, cities, and systems, among others [40]. The SSP, however, a shorter existence plan, where the pilot-test took place in Philippines, only started in 2016 [14].
Among all relevant documents that were reviewed (Table 1), four of them explained the framework stages and parts to guarantee water safety and sewage in WSP and SSP [14,16,35,40].
Phase 3.1 referred to the bibliographic research and resulted in 53 scientific papers. From them, 16 were excluded due to the application of filters, while the other 32 were removed by exclusion criteria. Finally, 21 articles met all inclusion criteria, which presented an average of 11.62 citations, with standard deviation of 13.99 and variation coefficient of 1.20 (Table 3). Of these, twelve (57.14%) used the full WHO methodology, six (28.57%) used adapted WHO methodology, and three (14.28%) used their own methodologies.
Table 3.
Methodologies for preparing WSS or SSS used in research found in literature review.
Among the works that adopted the WHO methodology in full for the preparation of the WSP or SSP, several techniques were used for data collection and risk analysis, including the risk matrix [11,42,47,50]. The tools for executing each step were not developed in this work and will be addressed in the discussion.
3.1.2. Second Phase
In the technical review (phases 1.1 and 1.2), the main stages and elements of a conceptual model for safety plans were identified, in addition to the guiding fundamental principles for their preparation. In the scientific review (phase 1.3), the main methodologies used and their adequacy to each local reality were verified, including additional methods applied in evaluated experiences.
From this, the ICMRBSSP was developed (Figure 3) in two parts, composed by six fundamental principles and six steps.
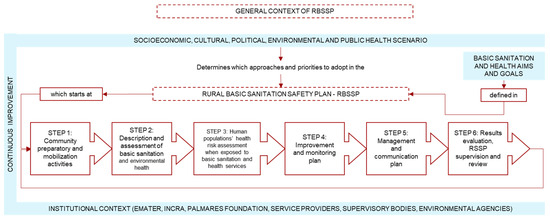
Figure 3.
Initial RBSSP diagram of the conceptual model—ICMRBSSP.
The first part of the ICMRBSSP involves the fundamental principles, including the local context and safety plans, specifically risk management; education and social participation; technologies suited to reality; multiple barriers; and expanded health concept and principles of Law n. 11,445/2007 [39]. The second part of the ICMRBSSP was constructed in two steps—each one with its respective objective and a set of actions—and covers how these should be implemented, what instruments are needed, and the products expected when finishing their execution.
3.1.3. Third Phase
The results of this phase will be presented as follows: products obtained at phases 3.1 and 3.2; initial and final versions of fundamental principles, steps and actions; and final structure of the CMRBSSP.
In phase 3.1, after the initial contact, the survey was sent by e-mail to 16 specialists that live in different regions of the country who research and know the characteristics of the proposed subject. After 20 days, with a dropout rate of 26.6%, 12 specialists sent their completed surveys, with 33.3% of the experts being members of FUNASA-DF, the main national public foundation for health promotion and prevention, especially in actions related to rural sanitation basics. The states of Bahia, Ceará, Minas Gerais and Paraíba contributed, each one, with 8.33% of the surveys; Goiás and Santa Catarina contributed with 16.66% of the surveys; the other 66.6% represented other Brazilian locations.
Phase 3.2 was applied in the city of Goiânia, Brazil, in November 13 and 14, in 2018, as a panel discussion. Eight specialists were present, representing 66.6% of those who participated in the phase 3.1, aiming to define the CMRBSSP and its parts.
The first group consensus reached was that the methodology should be composed by short, objective and flexible elements. Thus, the CMRBSSP should contemplate only RBSSP fundamental principles, its stages and actions. The items referred to how each action was performed, the necessary instruments and the expected products, which are included for the initial proposal, that must be excluded from the conceptual model, although they may be examples of its execution, in practice.
- (a)
- Fundamental principles
In the survey, 63.6% of the specialists partially agreed with the fundamental principles mentioned, and 36.4% fully agreed. Figure 4 lists the initial proposition, the written contributions and the final fundamental principles’ proposition.
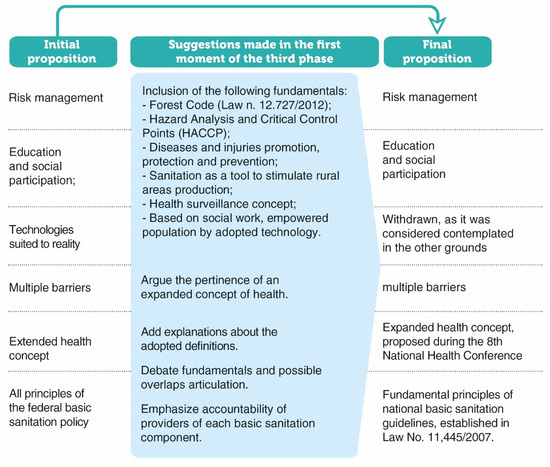
Figure 4.
Debate results of specialists regarding the fundamental principles: initial proposition, suggestions made at phase 3.1, and final proposition of the CMRBSSP.
All contributions were discussed in a panel of specialists, where they reached the consensus of fully adopting two contributions: the adoption of the denomination “health extended concept” and elimination of the item “technologies locally adapted”, as it was already contemplated in another fundamental (fundamental principles of national basic sanitation guidelines). There were discussions to avoid overlapping fundamental principles and to limit their scope to basic sanitation. Finally, the last consensus among specialists was the mobilization and social participation actions, which should transversally permeate all RBSSP stages and actions.
- (b)
- Stages
Figure 5 presents the initially proposed steps and their final version after the specialists’ consensus. Among the six steps, only two (4 and 5) kept the name proposed initially. The remaining steps underwent changes as a result of discussions that aimed to generalize the actions to be performed, avoid repetitions and convey a clear and concise message.
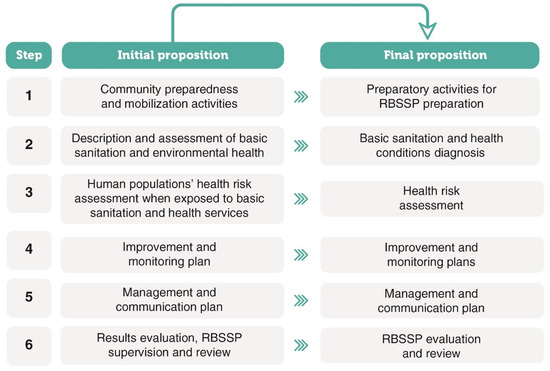
Figure 5.
Specialists’ consultation’s results regarding the stages: CMRSSP initial and final proposition.
- (c)
- Actions
Figure 6 and Figure 7 show the actions for initial proposition of ICMRBSSP: the result of the specialists’ assessment in phase 3.1 of consultation regarding full (Y) or partial agreement (P) or disagreement (N), and their final proposition after phase 3.2. On subsequent paragraphs, the evolution of each stage is detailed. CMRBSSP application in the third phase, meanwhile, requires local adaptation to each reality, local cultural, regulatory and socio-environmental characteristics that must be observed.
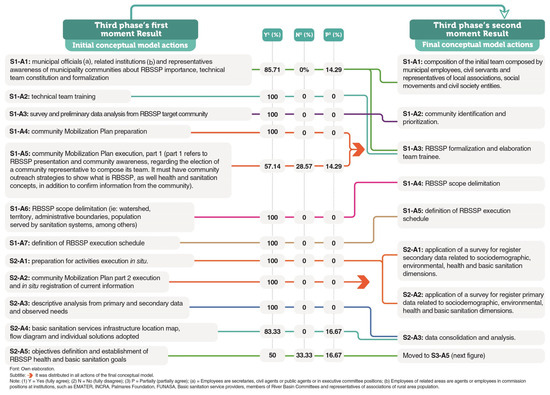
Figure 6.
Results of specialists’ consultation for S1 and S2 stages: evaluated actions, agreement percentage during remote assessment and final CMRBSSP actions proposal, after face-to-face phase.
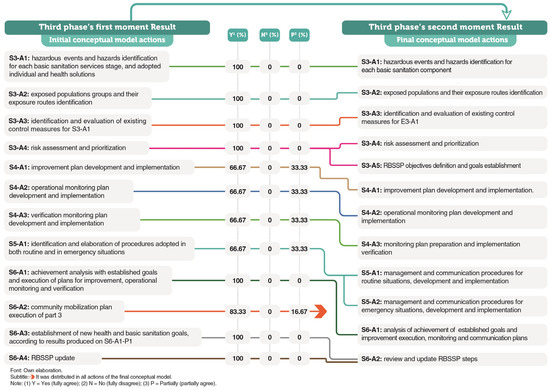
Figure 7.
Results of specialists’ consultation for S3 and S6 stages: evaluated actions, agreement percentage during remote assessment and final CMRBSSP actions proposal, after the face-to-face phase.
For Step 1, remote actions at the time were approved. Action S1-A5 had the highest disagreement and received three textual contributions. The first one was the need, in practice, to include a perception survey on the existing sanitation reality and what the community wanted from this service. In the second one, an inquiry questioned how many representatives existed per community, and whether if just one would be enough. Finally, it was suggested, in order to apply the action in practice, that health and sanitation concepts must be built with the participation of the community, as a more properly integrated way to make contributions. Despite this, after the specialist panel, it was decided to reorganize the actions and generalize the necessary representations in action S1-A1 including population groups, relevant for RBSSP preparation, and the elimination of actions S1-A6 and S1-A7.
For Step 2, although in the survey phase there was total agreement (100%) regarding the proposed name and actions were concluded in debate, specialists suggested changes as a way to simplify the textual writing. Two of the five actions were disagreed upon in the survey phase. As result, actions S2-A1, S2-A2 and S2-A3 were rewritten generalizing the activities meant to be developed, and S2-A4 and S2-A5 were eliminated. For the latter, textual contributions were the final products and they did not have actions to be performed, pointing out that S2-A5 was a consequence of the previous ones. There was the need to expand the collected data, encompassing those on sociodemographic and environmental aspects, in addition to those initially proposed (health and basic sanitation). This information is important to justify consecutive steps.
Step 3 obtained unanimity among specialists in phase 3.1, regarding both the title and the actions (Figure 7). Even though there was consensus concerning the actions discussed, textual contributions were made related to stage objective writing and to proposed actions. In the face-to-face discussion, the items’ writing and organization were reformulated, seeking to simplify terms without eliminating any action. The specialists agreed that, at this stage, the RBSSP goals’ purpose as a whole objective should be established. The choice to execute all activities listed in a single step aimed to ease the flow of information, necessary for the definition of goals, so that the developer could assess the risk and be able to directly apply the result assessment for sanitation and health problems resolution.
For Step 4, at the survey phase, it was possible to observe partial disagreement in all actions (Figure 7). The textual considerations pointed out the need of adjustment of the terms adopted and to add an item or action aiming to assess the commitment of the decision makers. However, after solid discussion in person, it was agreed that this was not the space to include this action which was initially suggested in the proposal.
In Step 5, the specialists did not approve the action suggested in the survey (Figure 7). The written considerations highlighted the possibility of confusion for the procedures adopted in routine and in emergency situations. It was, then, suggested that it should be divided into two separate actions, originating S5-A1 and S5-A2.
In Step 6, there was disagreement regarding the S6-A2 in phase 3.1, when further explanation was requested regarding the established health goals (Figure 7). In the face-to-face discussion, the number of actions was reduced to two (S6-A1 and S6-A2) in order to avoid actions overlapping and simplify writing.
Finishing the face-to-face discussion, the specialists emphasized that, for RBSSP implementation, education and social participation must remain, in a transversal way and for all its stages and actions. In this way, S1-A4, S1-A5, S2-A2 and S6-A2, which are constant in the ICMRBSSP (Figure 6 and Figure 7), remain throughout the CMRBSSP.
Likewise, it is essential to maintain consistency in the articulation and compatibility of concepts and denominations adopted in the plan with those endorsed on the National Program on Rural Basic Sanitation (PSBR), and the social movements related to the type of community that will receive it, when its application occurs in Brazil. The RBSSP must be prepared and implemented in alignment with public policies for each country, state, province or locality. Finally, there was also an emphasis on the importance of integrating and incorporating the community for RBSSP preparation, as a way of facilitating its successful implementation.
- (d)
- CMRBSSP final framework
In order to enhance CMRBSSP understanding and its application, the diagram shown in Figure 2 was adjusted according to research results, and transformed into the final RBSSP framework, as seen on diagram in Figure 8.
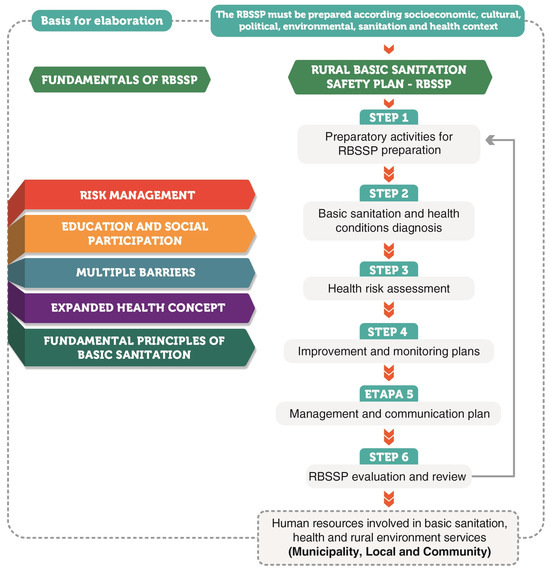
Figure 8.
Methodology structure for preparing RBSSP agreed by specialists.
3.2. Case Study
A simulation for CMRBSSP application to elaborate a RBSSP was executed at João de Deus agrarian reform settlement. This allowed the required identification of steps and actions, with adaptations for this specific municipality. The main steps and actions were related to the execution order, separation into sub-steps and inclusion of phases. In Supplementary Materials, Tables S1–S3, the actions obtained on CMRBSSP are shown, as well as the suggestions for adaptations. It can be noted that all actions were contemplated with phases, and some steps were divided into sub-steps.
4. Discussion
4.1. RBSSP Conceptual Model (CMRBSSP)
4.1.1. Phase 1.1
After analyzing the documents, it was possible to identify that the WSP emerged around year 2000, shortly after the proposed WHO review Drinking Water Quality Guide and the Australian experience in Victoria, with water management plans risk [59,60]. During the discussions of the present work, it was possible to observe the need to develop guidance guides and good practices for safe drinking water supplying covering quality and quantity issues [13,34,60]. This material evolved throughout discussions, and the approach which became a tool to guarantee safe drinking water was the WSP, whose official guide was launched in 2005 by the WHO and uses Hazard Analysis and Critical Control Points (HACCP) as a methodology key for the identification of hazardous events [16,61].
In Portugal, this methodology has been implemented since 2003 with one leading, applied in Águas de Cávado, as a WHO pilot experiment [62,63,64]. In methodology terms, this WSP was implemented in three phases: (1) the fundamental principles, in which the system is described, and risks, critical limits and corrective actions are evaluated; (2) operational aspects, where the relevant aspects about risks within the system, the critical control points and the necessary contingency plan are registered; and finally the last phase, which is the (3) functioning, monitoring and continuous evaluation [62,63].
In Bangladesh, WSP application took place in small communities, as a very innovative experience in 2005, aiming to avoid contamination [65]. Considering this methodology, in addition to evaluate sanitation systems and the incidence of diarrhea, hygiene practices and community’s behavior was considered in the pilot systems. The community was trained on operational monitoring, preventive maintenance and water collection systems, using visual tools adapted to this reality [51,65]. The experience in Bangladesh showed that community engagement tools, focused on water safety, promote community empowerment and contribute to design and implement plans successfully. This is because people provide relevant information to identify hazardous events and can act as plan monitoring agents. After reviewing papers, Ref. [20] emphasized the importance of connecting the impacts and outcomes of WSPs, improving training, and building staff capacity. Additionally, they suggested that simplifying the WSP methodology could facilitate successful implementation. Pilot schemes demonstrating the benefits of WSPs could stimulate their broader adoption.
The framework to ensure safe water, according to the WHO, is composed of health targets, a WSP (including system evaluation steps, monitoring, management and communication) and a surveillance solution, placed for public health context [34].
In 2010, the same year that water and sanitation were recognized as human rights, the WHO recommended the development of a specific SSP manual, which was published in 2016 [14,66]. The framework for implementing SSP includes national government, local governance functions and community-level engagement functions, including individual and shared services, and infrastructure [35].
Considering the technical documents evaluated, general safety plans’ structure must include steps such as diagnosis, risk assessment and plans improvement. In addition, other factors can influence the different plans’ design and implementation. SSP pilot experiences took place in Banglare (India), Lima and San Juan de Lurigancho District (Peru), Baliwag and Quezon City (Philippines), Benavente (Portugal), Kampala (Uganda) and Hanoi (Vietnam) [14,60]. These authors identified that appropriate partnerships between civil society, the sense of plan ownership, financial and experienced external consultants support consisted of the set of successful factors for the preparation of plans [61].
The cases presented in the technical documents demonstrate the need to adapt this methodology to local peculiarities concerning the financial, ecological or social terms. In addition, support mechanisms for local reality and community participation have the potential to make the WSP and SSP more effective [14,16]. Thus, it is necessary that any and every safety plan proposal is able to contemplate the general structure previously identified, and other elements facilitating success in its implementation.
4.1.2. Phase 1.2
Hereafter, the fundamental principles listed in the results will be detailed in terms of their meaning. Risk management is the set of activities coordinated aiming to direct and control the risks of an organization [36]. When this approach is incorporated into regulations related to drinking water supply, its main advantage is a safe parameter pattern that will be tested, the encouragement of actions to prevent or mitigate contamination, and more efficient resource allocation, when major public health risks in the system were identified [34]. Based on risk assessment, which is part of its management, it is possible to make decisions concerning control measures and highlight differences between urban and rural systems [11,42].
Regarding education in rural areas’ basic sanitation, it can occur as formal, informal or non-formal ways, which are central modalities used to receive proficient training in the area. Training and educational programs contribute to the water supply systems’ continuity [67,68].
Social participation in this sphere includes aspects such as: understanding the relationship between water supply, sanitary sewage, solid waste and rainwater management, healthiness and health, and understanding technologies adopted, their services’ operation and management, a basic sanitation forum, sharing information, and participation in public audiences [37,69,70]. Social participation in basic sanitation is not a widespread practice; although its benefits are known, those do not arise from the simple existence of said processes [28,71,72].
However, it is necessary to point out that every population practice, interest and need should be aligned with each other, enabling existing technologies and projects in this subject, and supplying the necessary tools to achieve their objectives [71,73,74]. In addition, the social participation process offers, as a result, strength and legitimate interventions, causing an increase in the population’s concern with basic sanitation problems, strengthening both sustainability and quality services. On the other hand, when the population avoids participating, projects may offer a lower quality of monitoring mechanisms [28,68]. Therefore, the participation of all actors, combined with educational actions, is fundamental for public policies, especially those related to water supply, sanitary sewage, solid waste and rainwater management and health, such as the RBSSP.
The premise of multiple barriers is associated with the adoption of more than one control measure type (also called barrier) in systems, looking to minimize risks and ensure their safety [13,60]. The multiple barriers’ approach is widely adopted on WSP and SSP safe management, due to its advantage, which is the fact that when a barrier fails, others can compensate this deficiency; with this, system safety and continuity can be guaranteed [34,36,75]. In addition to the recommendation made by the WHO, the principle has been adopted in several countries and recommended by environmental agencies, as shown in a Canadian case [44,76,77].
According to the WHO, health is defined as the whole human state of physical, mental and social well-being, not merely the absence of disease and illness [78]. This concept does not consider local specificities, where the individual or population lives, besides referring to a fixed and ideal situation.
The relationship between health and sanitation, especially in rural areas, can be observed in the scientific literature [25,79,80,81,82]. To consider this, the specific context where human beings live must be included in health, as in the so-called “health extended concept”. The determinants and constraints that impact living conditions and, therefore, health are not simply the absence of disease, but basic sanitation, food, housing, work, education, and the environment, among others [6,8]. In a recent study, Ref. [22] evaluated the impacts of Water Safety Plan (WSP) implementation in Egypt, focusing on the performance of the country’s water sector. The study highlighted the need to strengthen the link between public health and WSPs in the county. It recommended building a core team with expertise in risk management and incorporating staff from diverse specializations and capacities, which requires training the staff in WSP and risk management [22].
Safety plans must be aligned with the current national legislation [16,83,84]. In Brazil, the Legal Framework for Basic Sanitation (Law No. 11,445/2007 [39] and its updates) is one of the world’s laws that defines and guides basic services’ provision, regarding the provider’s nature, which must be guided by 16 fundamental principles (Article 2). Among the aforementioned principles, 14 can be applied in rural areas, and 1 applies when the concession contract establishes it (Section IV) [39]. In the absence of national legislation, these principles can be adopted as guidelines for RBSSP preparation.
4.1.3. Phase 1.3
For the implementation of WSP and SSP, the WHO’s methodology must be applied considering some flexibilities, adapting and improving this methodology, especially in the risk assessment stage. In some cases, the addition of interested aspects to each reality might impact the WSP. In Vanuatu, Oceania, the variable water availability was included to assess possible climate change impacts [9]. In Senegal and Burkina Faso, after assessing the implementation sustainability of WSP, the application of a survey was proposed, prior to its preparation, with the purpose of identifying the facilitating aspects or challenges in its implementation. Therefore, this survey helps identify the local leaders’ participation in the water supply system’s complexity as key factors to be reinforced before preparing the WSP [52,85].
Other factors for safety plans’ implementation were pointed out as important, among which are previous community preparation, aiming towards its understanding and knowledge, which can result in better adherence to the methodology [50,86,87]. Hence, the service provider’s participation and the identification of individual solutions for each location reduces problems during the plan’s implementation [3].
The matrix, especially the semi-quantitative one, was the most identified risk assessment methodology [11,42,48,50,57]. However, other tools such as assessment software, scores, surveys and workshops have also proven to be useful for safety plan step [41,53,54,55]. However, specific risk assessment procedures for rural areas are being developed and can be part of specific plans, as in RBSSP case [31,32].
4.1.4. Second Phase
The conceptual model initially proposed included three aspects: the main elements found in WSP and SSP, recommendations from the literature and local legislation requirements, in this case, in the scope of Brazilian law. Such aspects were incorporated in the presented steps, which are similar to those found in the preparation of safety plans guideline documents [16,83]. The stage of community preparation and mobilization activities was included with the objective of providing relevant considerations offered by the scientific literature, which emphasized the importance of adapting the methodology to the local reality and preparing the community to participate and receive the respective training for RBSSP preparation [52,85,86]. The foundations adopted include, therefore, the local legislation requirements and the literature recommendations, such as risk management and social participation.
4.1.5. Third Phase
As for RBSSP stages, in the first stage, it is possible to point out that interventions in rural areas’ basic sanitation, where the consultation of interested parties who consider the local context and the community preferences tends to result in better performance than with those that do not [28,72,73]. Including community members in the preparation is the key success factor for WSP [56,87]. Thus, the first stage was proposed with a specific function, deemed as an important moment to prepare the responsible team and community, as well as enabling the effective inclusion and preparation of the population.
Also, in this stage, the RBSSP limits were defined. In the WSP, the scope goes from water catchment until its consumption, while in the SSP, the boundaries must be defined based on the plan’s objective [14,16]. In the RBSSP case, as it incorporates all basic sanitation components, its delimitation must consider such services and rural areas’ characterization, where the plan will be applied. Some techniques help to establish these borders, such as the characterization of the area, based on census sectors [88], and the direct application of the concept of rurality from PSBR [37], among other relevant methods and adapted to the local reality.
Step 2, which deals with diagnosis, has actions that describe, locally, basic sanitation reality and health. Perceiving the local context comprehensively is one of the factors which facilitates WSP implementation in rural areas and must consider aspects such as housing, socio-political structure, and local authorities, and the presence of committees related to water, control measures, existing management practices, among others [9,52]. Therefore, this part of the RBSSP preparation supports the next steps and, when carried out in an inclusive way, can facilitate its implementation. In addition, gathering information, which is not only about basic sanitation, but also about habitability and health, can support the preparation of improvement plans, as they impact possible solutions.
Risk assessment (Step 3) can be one of the most difficult phases since similar difficulties are observed in those related to the preparation of WSP. The adaptation of both the risk assessment and other methodologies adopted might be the enabling factor for the implementation of WSP in rural areas [11,18,55]. In some cases, it is recommended to develop this step in a simplified way, based on discussion and decision-making from a defined technical team [14,16]. Risk assessment techniques and studies, adapted to local reality, especially focusing on the rural area, should be prioritized and have been developed and presented in the literature [5,31,32,42,89]. The authors of [21] adapted the risk assessment methodology for small rural systems. The authors highlighted the importance of having data on infrastructure, control measures, and historical information about the systems. They recommended using their results to build a national database on water supply risks [21].
The implementation of control measures is an essential activity to reduce health risks in an exposed population [14,34]. As well as operational monitoring and verification, improvement plans are essential for the execution of WSS since it is necessary to support those involved in the process and evaluate its impacts or results [9,18,22,90]. Regarding monitoring and verification, a unified group of operational indicators may help to measure the impact of safety plans [22].
Dealing with routine situations is important, as the preparation for emergency situations is as well [14,16,91]. Even when water safety is not completely assured, warning systems can, for example, introduce additional treatments, if necessary [55]. In this sense, a stage (stage S5—Figure 6) committed to this activity, which is also provided to WSP and SSP, can help in the ability to respond in these situations [11,42].
The evaluation of safety plans, its review and adaptation to local context include aspects learned and improving it is a continuous and necessary process to obtain best results [11,18]. The characteristic of continuous improvement, which is inherent to safety plans, implies a step like S6 (Figure 6), dedicated to this activity. The use of indicators can reveal advances and challenges for the implementation of safety plans [3,22,45], being recommended by the WHO for WSP and SSP monitoring [14,16].
4.2. Case Study
The proposed CMRBSSP allows for changes and adjustments according to the scenario. The actions of the conceptual model were enhanced through a comparison with empirical data and information obtained from the João de Deus settlement. In the simulation performed at the present research, this feature was tested so that researchers and other interested parties could apply this CMRBSSP, adapting it to every reality, according to local needs and demands. This recommendation is also indicated by the WHO for WSP and SSP [14,16].
Still during the present case study, the need to collect the concerns of the population, given the diagnosis obtained, has proven that community participation and promotion is fundamental for RBSSP and, at the same time, an informal education process, meeting the literature requirements [28,67,68].
CMRBSSP Step S3 simulation was implemented, and collective and individual systems were evaluated separately. Thus, as in the community used for assessment, others can also access basic sanitation services in both ways. In collective solutions, a semi-quantitative risk matrix was used [31]. For individual systems, a safety index was adopted, showing the situation of households, which can be used in safety plans [32]. Other tools and techniques can be also used, adapting them to the local reality, available in the technical–scientific literature [5,42,89].
During the CMRBSSP Step S4 simulation, referring to improvement and the preparation of monitoring plans, the need for the participation of the community was identified. Action S4-A1 (survey for registering concerns of the population that uses basic sanitation services) was included, where the possibility of collecting the concerns regarding basic sanitation, health and habitability was included on the definition of RBSSP objectives and targets, guiding the construction of the improvement. The Step S4 simulation reinforced the importance of social participation as fundamental, as well as the recommendations issued by specialists, and as seen in the literature [28,72].
To promote an assertive review process, during the application of the CMRBSSP simulation, indicators were used to promote continuous monitoring of RBSSP. Each indicator was established in order to verify whether established goals, based on the community’s aspirations, were achieved, as well as to proceed on towards possible evolutions. There is a variety of methods for the selection of indicators for monitoring water, sewage and hygiene [92,93,94].
Therefore, the RBSSP differs from the models proposed by the WHO in three key aspects:
- -
- Detailed steps and actions: The RBSSP consists of 6 steps and 20 actions which differ from the WHO proposal, as outlined in Table 2. This level of detail facilitates understanding and implementation by smaller service providers and communities that lack sufficient staffing.
- -
- Expanded fundamental principles: The fundamental principles of the RBSSP are broader than those of the WHO. While the WHO primarily focuses on the principle of multiple barriers and risk analysis, the RBSSP extends further to incorporate social participation, an expanded concept of health, and the four components of basic sanitation (water supply, sewage, waste, and drainage).
- -
- Comprehensive context: the RBSSP context includes socio-economic, cultural, and political issues, which are not addressed in the general WHO framework for WSP and SSP.
The strengths of this paper lie in its comprehensive safety plan, which is closer to the integrated nature of rural environments where all components are interconnected. Moreover, the modern six fundamental principles align with the concept of health extended and that is not rooted, ensuring applicability beyond places with basic sanitation standards established. Additionally, the detailed and self-explanatory actions facilitate implementation, particularly beneficial for small providers with limited staff. About the limitations, this paper does not develop the tools to address risk assessment to rural areas. In addition, more case studies can be performed in order to obtain specific examples and possibilities for each rural settlement, which may help small providers and small communities.
5. Conclusions
This work allows us to draw the following conclusions:
- The WSP and SSP frameworks consist of multiple steps and must include phases for diagnosis, risk assessment, management plans and continuous improvement phases, which are relevant for any safety plan methodology.
- A methodology for the preparation of safety plans for rural areas, related to basic sanitation, can be used as it is or adapted, depending on the local reality, such as cultural, economic, regulatory and community involvement aspects. However, there is a gap in the adaptation process. The methodology adaptation to rural settlements and to include the four components of basic sanitation remains a gap in the literature, which evidences the importance of RBSSP.
- It is possible to develop a comprehensive safety plan that integrates water supply, sewage, solid waste management and rainwater management in rural settlements. This plan should be based on the principles of basic sanitation, ensuring that all steps are applied to these four services.
- The methodology for the preparation of RBSSP must address specific and/or greater impact issues, such as the community representation team for its preparation, and the expanded concept of health application connected to each one of the basic sanitation services (water supply, sewage, solid waste management and rainwater management), which differentiates it from urban areas.
- Community participation, involvement and empowerment must be considered in RBSSP methodology, as these are factors of greater relevance in its implementation, specially to ensure the connection between the four components of basic sanitation and because most of these services are provided by the population.
- It is important that RBSSP fundamental principles are explicit and are used during its preparation, implementation and for decision-making. This can strengthen the implementation of RBSSP, ensuring that it focuses on the most important issues in rural basic sanitation.
- The necessary tools for the preparation of RBSSP, such as risk assessment methodologies and management plans, must be applied considering RBSSP fundamental principles.
- The application simulation of the conceptual model showed that it is necessary to adapt the actions, to apply appropriate methods and techniques developed for the rural area, as a way to properly prepare RBSSP, according to the scenario. After conducting the case study, the final RBSSP framework consists of six fundamental principles, six steps, and twenty actions to be implemented in any type of rural settlement.
Thus, the CMRBSSP for the preparation of RBSSP proposed here contemplates basic sanitation components (water supply, sanitary sewage, solid waste management and rainwater) in a comprehensive safety plan, community participation and health expanded concept as key guiding factors. It can also be applied to rural communities, in full or modified form, with the potential to improve their quality of life. There is a gap related to the need for improvement or development of the tools used in the preparation of RSSP, which must be aligned and integrated with the proposed methodology and existing public policies.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/resources13070090/s1, Table S1: Case study application: Steps 1 and 2; Table S2: Case study application: Steps 3 and 4; Table S3: Case study application: Steps 5 and 6.
Author Contributions
Conceptualization, R.O.B., N.R.B. and P.S.S.; methodology, R.O.B., N.R.B. and P.S.S.; software, R.O.B., N.R.B. and P.S.S.; validation, R.O.B., N.R.B. and P.S.S.; formal analysis, R.O.B., N.R.B. and P.S.S.; investigation, R.O.B., N.R.B. and P.S.S.; resources, R.O.B., N.R.B. and P.S.S.; data curation, R.O.B.; writing—original draft preparation, R.O.B.; writing—review and editing, R.O.B., N.R.B. and P.S.S.; visualization, R.O.B., N.R.B. and P.S.S.; supervision, P.S.S.; project administration, P.S.S.; funding acquisition, P.S.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Fundação Nacional de Saúde (FUNASA), TED 05/2017, and the APC was funded by Fundação Nacional de Saúde (FUNASA). This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES)—Finance Code 001.
Data Availability Statement
Data are contained within the article.
Acknowledgments
The authors would like to thank everyone involved in the Projeto Saneamento e Saúde Ambiental em Comunidades Rurais e Tradicionais de Goiás—SanRural, for promoting scientific research in the state of Goiás.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Agência Nacional De Águas e Saneamento Básico (Brasil). ODS 6 no Brasil: Visão da ANA Sobre os Indicadores, 2nd ed.; (SDG 6 in Brazil: ANA´s Vision about Indicatros); ANA: Brasília, Brazil, 2022; 212p. Available online: https://metadados.snirh.gov.br/geonetwork/srv/api/records/c93c5670-f4a7-4de6-85cf-c295c3a15204/attachments/ODS6_Brasil_ANA_2ed_digital_simples.pdf (accessed on 25 January 2023).
- Brasil. Lei nº. 14.026, de 15 de julho de 2020 (Law n. 14,026). In Atualiza o Marco Legal do Saneamento Básico; Diário Oficial da União: Brasília, Brazil, 2020. Available online: https://www.in.gov.br/en/web/dou/-/lei-n-14.026-de-15-de-julho-de-2020-267035421 (accessed on 2 October 2022).
- Rodriguez-Alvarez, M.S.; Gutiérrez-López, A.; Iribarnegaray, M.A.; Weir, M.H.; Seghezzo, L. Long-Term Assessment of a Water Safety Plan (WSP) in Salta, Argentina. Water 2022, 14, 2948. [Google Scholar] [CrossRef]
- Murei, A.; Mogane, B.; Mothiba, D.P.; Mochware, O.T.W.; Sekgobela, J.M.; Mudau, M.; Musumuvhi, N.; Khabo-Mmekoa, C.M.; Moropeng, R.C.; Momba, M.N.B. Barriers to Water and Sanitation Safety Plans in Rural Areas of South Africa—A Case Study in the Vhembe District, Limpopo Province. Water 2022, 14, 1244. [Google Scholar] [CrossRef]
- Vinti, G.; Bauza, V.; Clasen, T.; Tudor, T.; Zurbrugg, C.; Vaccari, M. Health risks of solid waste management practices in rural Ghana: A semi-quantitative approach toward a solid waste safety plan. Environ. Res. 2023, 216, 114728. [Google Scholar] [CrossRef] [PubMed]
- Pan American Health Organization—PAHO. Environmental Gradients and Health Inequalities in the Americas: Access to Water and Sanitation as Determinants of Health; PAHO: Washington, DC, USA, 2016; Available online: https://iris.paho.org/bitstream/handle/10665.2/31404/9789275119136-eng.pdf (accessed on 3 February 2023).
- Prüss-Ustün, A.; Wolf, J.; Bartram, J.; Clasen, T.; Cumming, O.; Freeman, M.C.; Gordon, B.; Hunter, P.R.; Medlicott, K.; Johnston, R. Burden of disease from inadequate water, sanitation and hygiene for selected adverse health outcomes: An updated analysis with a focus on low- and middle-income countries. Int. J. Hyg. Environ. Health 2019, 222, 765–777. [Google Scholar] [CrossRef] [PubMed]
- Brasil. Lei n. 8.080, de 19 de Setembro de 1990 (Law n. 8,080); Diário Oficial da União: Brasília, Brazil, 1990; p. 18055, Seção 1. Available online: https://www.planalto.gov.br/ccivil_03/leis/l8080.htm (accessed on 1 October 2022).
- Rand, E.C.; Foster, T.; Sami, E.; Sammy, E. Review of water safety planning processes and options for improved climate resilient infrastructure in Vanuatu. Water Pract. Technol. 2022, 17, 675. [Google Scholar] [CrossRef]
- Lane, K.; Megan, F.; Toni, S.; Stoddart, A. Exploring the use of a sanitation safety plan framework to identify key hazards in first nations wastewater systems. Water 2021, 13, 1454. [Google Scholar] [CrossRef]
- Pundir, S.; Singh, R.; Singh, P.; Kandari, V. Risk assessment and water safety planning for rural water supply in Uttarakhand, India. Environ. Monit. Assess. 2021, 193, 795–812. [Google Scholar] [CrossRef]
- Souter, R.T.; Ruuska, D.; Pene, S.; Benjamin, C.; Funubo, S.; Beal, C.D.; Sanderson, R.; Batikawai, S.; Ravai, A.; Antoinette-Wickham, T.; et al. Strengthening rural community water safety planning in Pacific Island countries: Evidence and lessons from Solomon Islands, Vanuatu, and Fiji. J. Water Health 2024, 22, 467–486. [Google Scholar] [CrossRef]
- World Health Organization—WHO. Water Safety Plans: Training Package; World Health Organization: Geneva, Switzerland, 2012; Available online: https://www.who.int/publications/m/item/water-safety-plans-training-package (accessed on 29 December 2022).
- World Health Organization—WHO. Sanitation Safety Planning: Manual for Safe Use and Disposal of Wastewater, Greywater and Excreta; WHO Library: Geneva, Switzerland, 2016; Available online: https://apps.who.int/iris/bitstream/handle/10665/171753/9789241549240_eng.pdf?sequence=1&isAllowed=y (accessed on 29 December 2022).
- World Health Organization—WHO. A Field Guide to Improving Small Drinking-Water Supplies: Water Safety Planning for Rural Communities; WHO Regional Office for Europe: Copenhagen, Denmark, 2022; Available online: https://wsportal.org/resource/a-field-guide-to-improving-small-drinking-water-supplies-water-safety-planning-for-rural-communities/ (accessed on 25 January 2023).
- Bartram, J.; Corrales, L.; Davison, A.; Dreere, D.; Drury, D.; Gordon, B.; Howard, G.; Rinehold, A.; Stevens, M. Water Safety Plan Manual: Step-By-Step Risk Management for Drinking-Water Suppliers; World Health Organization: Geneva, Switzerland, 2009; Available online: https://www.who.int/publications/i/item/9789241562638 (accessed on 1 October 2020).
- Brasil. Elaboração de Projeto de Melhoria Habitacional Para o Controle da Doença de Chagas; Governo Federal: Brasília, Brazil, 2013; 54p. Available online: https://bvsms.saude.gov.br/bvs/publicacoes/melhoria_habitacional_chagas.pdf (accessed on 1 February 2021).
- String, G.; Lantagne, D. A systematic review of outcomes and lessons learned from general, rural, and country-specific Water Safety Plan implementations. Water Sci. Technol.-Water Supply 2016, 16, 1580–1594. [Google Scholar] [CrossRef]
- Sutherland, D.; Payden. Observations and lessons learnt from more than a decade of water safety planning in SouthEast Asia. WHO South-East Asia J. Public Health 2017, 6, 27–33. [Google Scholar] [CrossRef]
- Alazaiza, M.Y.D.; Albahnasawi, A.; Al Maskari, T.; Nassani, D.E. Benefits, challenges and success factors of water safety plan implementation: A review. Global NEST J. 2022, 24, 414–425. [Google Scholar] [CrossRef]
- Fagundes, I.C.; Marques, G.F. Identification of potential hazards in rural alternative collective water supply solutions for the preparation of Water Safety Plans: An adaptation proposal. Eng. Sanit. Ambient. 2024, 29, e20220197. [Google Scholar] [CrossRef]
- Yehia, A.G.; Mehany, M.A.S.; Fareed, A.M.; El-sayed, W.H.; Taman, M.S. The role of water safety plan (WSP) to enhance the compatibility in water sector, Egypt. World Water Policy 2024, 10, 524–552. [Google Scholar] [CrossRef]
- Mcmeekin, N.; Wu, O.; Germeni, E.; Briggs, A. How methodological frameworks are being developed: Evidence from a scoping review. BMC Med. Res. Methodol. 2020, 20, 173. [Google Scholar] [CrossRef]
- Zare, F.; Elsawah, S.; Bagheri, A.; Nabavi, E.; Jakeman, A.J. Improved integrated water resource modelling by combining DPSIR and system dynamics conceptual modelling techniques. J. Environ. Manag. 2019, 246, 27–41. [Google Scholar] [CrossRef]
- Zavala, E.; King, S.E.; Sawadogo-Lewis, T.; Roberson, T. Leveraging water, sanitation and hygiene for nutrition in low- and middle-income countries: A conceptual framework. Matern. Child Nutr. 2021, 17, e13202. [Google Scholar] [CrossRef]
- Balaei, B.; Wilkinson, S.; Potangaroa, R.; Hassami, N.; Alavi-Shoshtari, M. Developing a Framework for Measuring Water Supply Resilience. Nat. Hazards Rev. 2018, 19, 04018013. [Google Scholar] [CrossRef]
- Howard, G.; Nijhawan, A.; Flint, A.; Baidya, M.; Pregnolato, M.; Ghimire, A.; Poudel, M.; Lo, E.; Sharma, S.; Mengustu, B.; et al. The how tough is WASH framework for assessing the climate resilience of water and sanitation. npj Clean Water 2021, 4, 39. [Google Scholar] [CrossRef]
- Jiménez, A.; Saikia, P.; Giné, R.; Avello, P.; Leten, J.; Lymer, B.L.; Schneider, K.; Ward, R. Unpacking water governance: A framework for practitioners. Water 2020, 12, 827. [Google Scholar] [CrossRef]
- Zhou, W.; Kalonji, G.; Chen, C.; Zheng, I.M.H. A three-staged framework for measuring water supply resilience in rural China based on PLS-SEM. Sci. Rep. 2022, 12, 4323. [Google Scholar] [CrossRef]
- Scalize, P.S. Diagnóstico Técnico-Participativo da Comunidade João de Deus–Silvânia–2018 (Technical-Participatory Diagnosis of the João de Deus Community–Silvânia City-2018); Cegraf UFG: Goiânia, Brazil, 2020; Available online: https://sanrural.ufg.br/wp-content/uploads/2022/02/DTP_JOAO_DE_DEUS.pdf (accessed on 25 January 2023).
- Bezerra, N.R.; Baracho, R.O.; Oliveira, T.L.d.; Scalize, P.S. Technique proposal and application for risk assessment in collective basic sanitation system in rural areas. Environ. Forum Alta Paul. 2022, 18, 1–21. [Google Scholar] [CrossRef]
- Scalize, P.S.; Bezerra, N.R.; Baracho, R.O. Safety index of individual basic sanitation systems in rural area. Environ. Forum Alta Paul. 2022, 18, 56–75. [Google Scholar] [CrossRef]
- Davison, A.; Howard, G.; Stevens, M.; Callan, P.; Fewtrell, L.; Deere, D.; Bartram, J. Water Safety Plans: Managing Drinking-Water Quality from Catchment to Consumer; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- World Health Organization—WHO. Guidelines for Drinking-Water Quality: Fourth Edition Incorporating the First Addendum; World Health Organization: Geneva, Switzerland, 2017; Available online: https://www.who.int/publications/i/item/9789241549950 (accessed on 29 December 2022).
- World Health Organization—WHO. Guidelines on Sanitation and Health; World Health Organization: Geneva, Switzerland, 2018; Available online: https://www.who.int/publications/i/item/9789241514705 (accessed on 29 December 2022).
- Associação Brasileira De Normas Técnicas-ABNT. ABNT/NBR/ISO/IEC 31.000: Gestão de Riscos–Diretrizes (Risk Management-Guidelines). Rio de Janeiro. 2018. Available online: https://www.normas.com.br/visualizar/abnt-nbr-nm/28977/abnt-nbriso31000-gestao-de-riscos-diretrizes (accessed on 14 December 2022).
- Brasil. Ministério da Saúde. Programa Nacional de Saneamento Rural (National Rural Sanitation Program); Funasa: Brasília, Brazil, 2019; 260p, ISBN 978-85-7346-065-0. Available online: www.funasa.gov.br/documents/20182/38564/MNL_PNSR_2019.pdf (accessed on 2 October 2022).
- Brasil. Portaria Ministério da Saúde/Gabinete do Ministro GM/MS n. 888, de 04 de maio de 2021 (Ministry of Health Ordinance); Diário Oficial da União: Brasília, Brazil, 2021; p. 127, seção 1. Available online: https://www.in.gov.br/en/web/dou/-/portaria-gm/ms-n-888-de-4-de-maio-de-2021-318461562 (accessed on 14 December 2022).
- Brasil. Lei nº. 11.445, de 05 de Janeiro de 2007 (Law n. 11.445); Diário Oficial da União: Brasília, Brazil, 8 January 2007. Available online: https://www.planalto.gov.br/ccivil_03/_ato2007-2010/2007/lei/l11445.htm (accessed on 1 October 2022).
- World Health Organization—WHO; International Water Association—IWA. Global Status Report on Water Safety Plans: A Review of Proactive Risk Assessment and Risk Management Practices to Ensure the Safety of Drinking-Water; World Health Organization: Geneva, Switzerland, 2017; Available online: https://apps.who.int/iris/handle/10665/255649 (accessed on 29 December 2022).
- Corrêa, R.F.M.; Ventura, K.S. Plano de Segurança da Água: Modelo conceitual para monitoramento de riscos à contaminação de água em comunidades rurais (Water Safety Plan: Conceptual model for monitoring risks to water contamination in rural communities). Eng. Sanit. Ambient. 2021, 26, 369–379. [Google Scholar] [CrossRef]
- Li, H.; Smith, C.D.; Cohen, A.; Wang, L.; Li, Z.; Zhang, X.; Zhong, G.; Zhang, R. Implementation of water safety plans in China: 2004–2018. Int. J. Hyg. Environ. Health 2020, 223, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Ye, B.; Chen, Y.; Li, Y.; Li, H.; Yang, L.; Wang, W. Risk assessment and water safety plan: Case study in Beijing, China. J. Water Health 2015, 13, 510–521. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Perrier, E.; Kot, M.; Castleden, H.; Gagnon, G.A. Drinking water safety plans: Barriers and bridges for small systems in Alberta, Canada. Water Policy 2014, 16, 1140–1154. [Google Scholar] [CrossRef]
- Kumpel, E.; Delaire, C.; Peletz, R.; Kisiangani, J.; Rinehold, A.; De France, J.; Sutherland, D.; Khush, R. Measuring the Impacts of Water Safety Plans in the Asia-Pacific Region. Int. J. Environ. Res. Public Health 2018, 15, 1223. [Google Scholar] [CrossRef] [PubMed]
- Rondi, L.; Sorlini, S.; Collivignarelli, M.C. Water safety plan: An approach to reduce drinking water contamination in a rural area of Senegal. Procedia Environ. Sci. Eng. Manag. 2014, 1, 53–57. Available online: https://www.procedia-esem.eu/pdf/issues/2014/no1/10_Luca_14.pdf (accessed on 3 February 2023).
- Souza, P.F.d.; Burgess, J.E.; Swart, M.; Naidoo, V.; Blanckenberg, A. Web enablement of a Water Safety Plan via the municipal-based electronic Water Quality Management System (eWQMS). Water Sci. Technol. Water Supply 2011, 11, 568–577. [Google Scholar] [CrossRef]
- Hasan, T.J.; Hicking, A.; David, J. Empowering rural communities: Simple Water Safety Plans. Water Sci. Technol. Water Supply 2011, 11, 309–317. [Google Scholar] [CrossRef]
- Khatri, N.R.; Heijnen, H. Keeping drinking water safe: Adopting water safety plans in rural Nepal. Waterlines 2011, 30, 212–222. [Google Scholar] [CrossRef]
- McMillan, A. A pilot community water safety plan in Nepal for point sources with household water treatment. Waterlines 2011, 30, 189–202. Available online: https://www.jstor.org/stable/24686572 (accessed on 2 January 2023). [CrossRef]
- Mahmud, S.G.; Shamsuddin, S.A.J.; Ahmed, M.F.; Davison, A.; Deere, D.; Howard, G. Development and implementation of water safety plans for small water supplies in Bangladesh: Benefits and lessons learned. J. Water Health 2007, 5, 585–597. [Google Scholar] [CrossRef] [PubMed]
- Rondi, L.; Sorlini, S.; Collivignarelli, M.C. Sustainability of Water Safety Plans Developed in Sub-Saharan Africa. Sustainability 2015, 7, 11139–11159. [Google Scholar] [CrossRef]
- Barrington, D.; Fuller, K.; McMillan, A. Water safety planning: Adapting the existing approach to community-managed systems in rural Nepal. J. Water Sanit. Hyg. Dev. 2013, 3, 392–401. [Google Scholar] [CrossRef]
- Bazgir, A.B.; Mohammadi, H.; Pirsaraei, S.R.A. Risk assessment of drinking water supply and distribution system of Zanjan City from Tahm dam using water safety plan. Desalination Water Treat. 2020, 207, 213–220. [Google Scholar] [CrossRef]
- String, G.M.; Singleton, R.I.; Mirindi, P.N.; Lantagne, D.S. Operational research on rural, community-managed Water Safety Plans: Case study results from implementations in India, DRC, Fiji, and Vanuatu. Water Res. 2020, 170, 115288. [Google Scholar] [CrossRef] [PubMed]
- White, P.; Badu, I.R.; Shrestha, P. Achieving sustainable water supply through better institutions, design innovations and Water Safety Plans-an experience from Nepal. J. Water Sanit. Hyg. Dev. 2015, 5, 625–631. [Google Scholar] [CrossRef]
- Lane, K.; Stoddart, A.K.; Gagnon, G.A. Water safety plans as a tool for drinking water regulatory frameworks in Arctic communities. Environ. Sci. Pollut. Res. 2018, 25, 32988–33000. [Google Scholar] [CrossRef]
- Greaves, F. Piloting a community process for water safety plans. Waterlines 2011, 30, 223–231. [Google Scholar] [CrossRef]
- Australia-South Australia Government. Safe Drinking Water Act 2011–Part 3: Risk Management Plans. Available online: https://www.legislation.sa.gov.au/LZ/C/A/SAFE%20DRINKING%20WATER%20ACT%202011/CURRENT/2011.16.UN.PDF (accessed on 2 February 2023).
- World Health Organization—WHO. Assessing Microbial Safety of Drinking-Water: Improving Approaches and Methods; WHO Press: Geneva, Switzerland, 2003; Available online: https://www.who.int/publications/i/item/9241546301 (accessed on 3 February 2023).
- Winkler, M.S.; Jackson, D.; Sutherland, D.; Payden; Lim, J.M.U.; Srikantaiah, V.; Fuhrimann, S.; Medlicott, K. Sanitation safety planning as a tool for achieving safely managed sanitation systems and safe use of wastewater. WHO South-East Asia J. Public Health 2017, 6, 34–40. Available online: https://apps.who.int/iris/handle/10665/329620 (accessed on 2 February 2023). [CrossRef] [PubMed]
- Vieira, J.M.P.; Morais, C. Planos de Segurança da Água para Consumo Humano em Sistemas Públicos de Abastecimento (Water Safety Plans for Human Consumption in Public Supply Systems); Instituto Regulador de Águas e Resíduos/Universidade do Minho: Braga, Portugal, 2005; Available online: http://repositorium.sdum.uminho.pt/handle/1822/4609 (accessed on 25 January 2023).
- Vieira, J.M.P. Water Safety Plan Implementation in Portugal. J. Water Health 2011, 9, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Roeger, A.; Tavares, A.F. Water safety plans by utilities: A review of research on implementation. Util. Policy 2018, 53, 15–24. [Google Scholar] [CrossRef]
- World Health Organization—WHO. Bangladesh; WHO Press: Geneva, Switzerland, 2011; Available online: http://www.searo.who.int/entity/water_sanitation/bangladesh_wsp.pdf?ua=1 (accessed on 30 April 2018).
- United Nations—UN. Resolution adopted by the General Assembly on 28 July 2010: 64/292. In The Human Right to Water and Sanitation; UN: New York, NY, USA, 2010; Available online: https://www.un.org/waterforlifedecade/human_right_to_water.shtml (accessed on 30 April 2018).
- Aleixo, B.; Pena, J.L.; Heller, L.; Rezende, S. Infrastructure is a necessary but insufficient condition to eliminate inequalities in access to water: Research of a rural community intervention in Northeast Brazil. Sci. Total Environ. 2019, 652, 1445–1455. [Google Scholar] [CrossRef] [PubMed]
- Riswan, M. Community Participation and Rural Water Supply System: Policy and Practice in Developing Countries. KALAM–Int. J. Fac. Arts Cult. South East. Univ. Sri Lanka 2021, 14, 675–683. [Google Scholar]
- Brasil. Caderno Metodológico Para ações de Educação Ambiental e Mobilização Social em Saneamento (Methodological Book for Environmental Education Actions and Social Mobilization in Sanitation); Ministério das Cidades: Brasília, Brazil, 2009. Available online: https://www.conder.ba.gov.br/sites/default/files/2018-08/Caderno%20metodol%C3%B3gico%20para%20a%C3%A7%C3%B5es%20de%20educa%C3%A7%C3%A3o%20ambiental%20e%20mobiliza%C3%A7%C3%A3o%20social%20em%20saneamento.PDF (accessed on 1 October 2022).
- Brasil. Orientações metodológicas para programa de educação ambiental em saneamento para pequenos municípios. In Caderno de Orientações-Caderno I; UEFS, Funasa: Brasília, Brazil, 2014. Available online: http://www.funasa.gov.br/site/wp-content/files_mf/orient_ed_sa_caderno1.pdf. (accessed on 1 October 2022).
- Kwangware, J.; Mayo, A.; Hoko, Z. Sustainability of donor-funded rural water supply and sanitation projects in Mbire District, Zimbabwe. Phys. Chem. Earth 2014, 76, 134–139. [Google Scholar] [CrossRef]
- Wijayanti, G.M.; Yanfika, H.; Asmara, M.; Perdana, R.; Rahmat, A. Strategy for the provision of drinking water and environmental sanitation based on the community in Sidodadi Village, Pesawaran Regency. In IOP Conference Series: Earth and Environmental Science; IOP Publishing: Bristol, UK, 2021; Volume 739. [Google Scholar] [CrossRef]
- Rubinger, S.D.; Rezende, S.C.; Heller, L. Discursos dissonantes: A comunicação entre técnicos e a população como fator para a participação social. In Participação e Controle Social em Saneamento Básico: Conceitos, Potencialidades e Limites (Participation and Social Control in Basic Sanitation: Concepts, Potentialities and Limits); Heller, L., Aguiar, M.M.d., Rezende, S.C., Eds.; Editora UFMG: Belo Horizonte, Brazil, 2016; 319p. [Google Scholar]
- Al Djono, T.P.; Daniel, D. The effect of community contribution on the functionality of rural water supply programs in Indonesia. Groundw. Sustain. Dev. 2022, 19, 100822. [Google Scholar] [CrossRef]
- Kayser, G.; Loret, J.F.; Setty, K.; Blaudin De Thé, C.; Martin, J.; Puigdomenech, C.; Bartram, J. Water safety plans for water supply utilities in China, Cuba, France, Morocco and Spain: Costs, benefits, and enabling environment elements. Urban Water J. 2019, 16, 277–288. [Google Scholar] [CrossRef] [PubMed]
- Bereskie, T.; Haider, H.; Rodriguez, M.J.; Sadiq, R. Framework for continuous performance improvement in small drinking water systems. Sci. Total Environ. 2017, 1, 1405–1414. [Google Scholar] [CrossRef]
- Barnes, C. Safe Drinking Water for All: A Status Update on Walkerton´s Legacy, 20 Years after Release of Inquiry Reports; Canadian Environmental Law Association: Toronto, ON, Canada, 2020; Available online: https://cela.ca/wp-content/uploads/2022/09/1490-Safe-Drinking-Water-for-All-Walkerton-Inquiry-Status-Report-Aug2022.pdf (accessed on 25 February 2023).
- World Health Organization—WHO. Basic Documents: Forty-Ninth Edition (Including Amendments Adopted up to 31 May 2019); World Health Organization: Geneva, Switzerland, 2020; Available online: https://apps.who.int/gb/bd/pdf_files/BD_49th-en.pdf (accessed on 29 December 2022).
- Bizuneh, H.; Getnet, F.; Meressa, B.; Tegene, Y.; Worku, G. Factors associated with diarrheal morbidity among under-five children in Jigjiga town, Somali Regional State, eastern Ethiopia: A cross-sectional study. BMC Pediatr. 2017, 17, 182. [Google Scholar] [CrossRef]
- Dey, N.C.; Parvez, M.; Islam, M.R.; Mistry, S.K.; Levine, D.I. Effectiveness of a community-based water, sanitation, and hygiene (WASH) intervention in reduction of diarrhoea among under-five children: Evidence from a repeated cross-sectional study (2007–2015) in rural Bangladesh. Int. J. Hyg. Environ. Health 2019, 222, 1098–1108. [Google Scholar] [CrossRef] [PubMed]
- Soboksa, N.E.; Gari, S.; Hailu, A.; Alemu, B. Association between microbial water quality, sanitation and hygiene practices and childhood diarrhea in Kersa and Omo Nada districts of Jimma Zone, Ethiopia. PLoS ONE 2020, 15, e0229303. [Google Scholar] [CrossRef]
- Torlesse, H.; Cronin, A.A.; Sebayang, S.K.; Nandy, R. Determinants of stunting in Indonesian children: Evidence from a cross-sectional survey indicate a prominent role for the water, sanitation and hygiene sector in stunting reduction. BMC Public Health 2016, 16, 669. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. A Practical Guide to Auditing Water Safety Plans; WHO: New York, NY, USA, 2015; 85p, Available online: https://www.who.int/publications/i/item/9789241509527 (accessed on 25 January 2022).
- Baum, R.; Bartram, J. A systematic literature review of the enabling environment elements to improve implementation of water safety plans in high-income countries. J. Water Health 2018, 16, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Tsitsifli, S.; Tsoukalas, D.S. Water Safety Plans and HACCP implementation in water utilities around the world: Benefits, drawbacks and critical success factors. Environ. Sci. Pollut. Res. 2021, 28, 18837–18849. [Google Scholar] [CrossRef] [PubMed]
- Kot, M.; Castleden, H.; Gagnon, G.A. The human dimension of water safety plans: A critical review of literature and information gaps. Environ. Rev. 2015, 23, 24–39. [Google Scholar] [CrossRef]
- Wahaab, R.A.; Elsayed, W.H.; Ibrahiem, M.S.; Hasballah, A.F. Application of Water Safety Plans to Improve Desalination Water Supply at Matrouh Governorate, Egypt. Egypt. J. Chem. 2021, 64, 6749–6759. [Google Scholar] [CrossRef]
- Pinheiro, R.V.N.; Chagas, I.M.; Basso, R.E.; Nóbrega, J.N.; Bezerra, N.R.; Scalize, P.S. Proposition and application of a method for the characterization of rural areas in the census sectors from the sanitation point of view. Environ. Forum Alta Paul. 2022, 18, 67–85. [Google Scholar] [CrossRef]
- Bezerra, N.R. Application of the Delphi technique to validate the methods to be used in the system on a web platform for the implementation of a water safety plan. Rev. Eletrôn. Gestão Tecnol. Ambient. 2018, 6, 29–40. [Google Scholar] [CrossRef]
- Nijhawan, A.; Jain, P.; Sargaonkar, A.; Labhasetwar, P.K. Implementation of water safety plan for a large-piped water supply system. Environ. Monit. Assess. 2014, 186, 5547–5560. [Google Scholar] [CrossRef]
- Brasil. Plano de Segurança da Água: Garantindo a Qualidade e Promovendo a Saúde: Um Olhar do SUS (Water Safety Plan: Ensuring Quality and Promoting Health: A View from SUS); Ministério da Saúde: Brasília, Brazil, 2012. Available online: https://bvsms.saude.gov.br/bvs/publicacoes/plano_seguranca_agua_qualidade_sus.pdf (accessed on 3 February 2023).
- Schwelein, S.; Cronk, R.; Bartram, J. Indicators for Monitoring Water, Sanitation, and Hygiene: A Systematic Review of Indicator Selection Methods. Int. J. Environ. Res. Public Health 2016, 13, 333. [Google Scholar] [CrossRef] [PubMed]
- Cassivi, A.; Tilley, E.; Waygood, E.O.D.; Dorea, C. Evaluating self-reported measures and alternatives to monitor access to drinking water: A case study in malawi. Sci. Total Environ. 2021, 750, 141516. [Google Scholar] [CrossRef] [PubMed]
- Turman-Bryant, N.; Clasen, T.F.; Frankhauser, K.; Thomas, E.A. Measuring progress towards sanitation and hygiene targets: A critical review of monitoring methodologies and technologies. Waterlines 2022, 41, 5–23. [Google Scholar] [CrossRef]








Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).