3.1. Epidemiology
Understanding the spread of viral transmission is critical to design and evaluate the impact of public health interventions. Typically, viral transmission is modeled using a compartmentalized approach that labels each person as part of one of the following groups: susceptible (
S), infected (
X), or recovered (
R), where the total population is
n =
S(
t)
+ X(
t)
+ R(
t) [
12]. Differential equations can be used to quantify the transitions from one state to the other for a given unit time. The
R0 or reproduction number is a term that indicates the contagiousness of an infectious disease within a population that has not previously been infected or vaccinated. A similar value, the effective reproduction number (
Re), reflects the variation in transmission intensity over time while the dispersion factor (
k) describes the extent to which an infection clusters and thus the impact of individual variation in infectiousness on disease emergence [
13].
Estimates for the
R0 can vary based on the mathematical method used to calculate it, geographic region considered, and period of time covered by available data. The time-dependent reproduction number can be estimated by the following equation:
Re =
R0S(
t). In calculating viral spread, a challenge is accounting for the delay between onset of disease and presentation of symptoms (or diagnosis). Additionally, uncertainty around the impact of viral load on viral transmission and longevity of antibody protection for those naturally infected means that those in the
R(
t) state may transition back into the
S(
t) state after recovery and
X(
t) state if they are re-infected. If SARS-CoV-2 continues to be a risk in the long-term, people may need to receive seasonal or yearly vaccines to boost anti-SARS-CoV-2 antibody levels and maintain population-wide immunity. As a result, sustained manufacturing operations will be required to meet cyclical demand. More work is needed to determine the length of protection conferred by approved vaccines to proactively plan manufacturing and supply operations, as well as vaccination campaigns. Another challenge can arise if a mutated version of the SARS-CoV-2 becomes prevalent and vaccines currently in development fail to provide protection. Analysis of SARS-CoV-2 genome mutations from 28 countries shows correlations between specific genetic variants (e.g., S protein D614G and ORF1ab P4715L) and fatality rates [
14]. Closely tracking the extent to which genetic drift of SARS-CoV-2 impacts the transmissibility of the virus and efficacy of vaccines for different strains will be important to plan future operations.
Various modeling tools provide historical estimates and future projections for the
Re based on the daily number of reported cases across geographies [
15]. This value can help estimate the proportion (
P) of the population that needs to be vaccinated to reach population-wide immunity using the equation:
P = 1
− (1/
R0). In a review of 14 published studies, the value for
R0 ranged from 1.4 to 6.49, with a mean of 3.28, a median of 2.79, and 95% CI (2.51, 4.05) [
16]. Using this estimate of
R0, we calculate the number of anti-SARS-CoV-2 vaccine doses (
D) required to meet the critical population coverage
P. Several factors need to be defined to estimate
D: total population, proportion of the population that is susceptible, vaccine efficacy, and number of doses that need to be administered to confer long-term immunity.
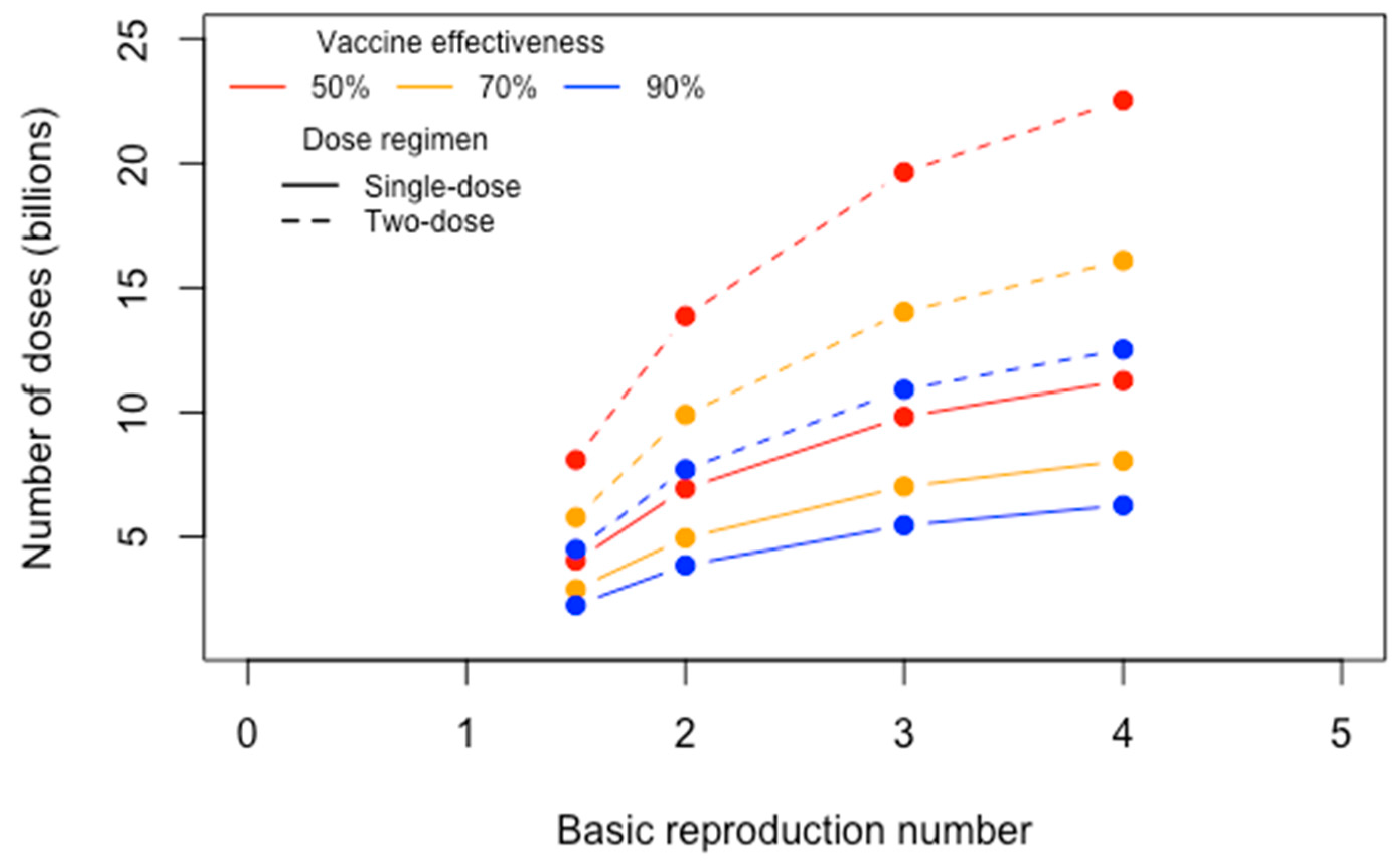
Figure 3 estimates the
D required to reach
P under varying vaccine efficacy levels (ranging from 50 to 90%),
R0 values (ranging from 1.5 to 4), and dose regimens (single- or two-dose), assuming an
S(
t) of 90%, and population of 7.8 billion. Taking the worst case scenario, with a vaccine efficacy of 50%,
R0 of 4, and each person needing a booster after initial administration, the estimated
D required to reach
P is over 22.5 billion. Under the best case scenario, with a vaccine efficacy level of 90% and
R0 of 1.5, the estimated
D required to reach
P is approximately 2.25 billion for a one-dose regimen and 4.5 billion for a two-dose regimen. These estimates provide a scale for the public health need to be met by vaccine manufacturers, regulators, and providers alike. It also provides insights into features of a vaccine that can be optimized during the design and development process to reduce the estimated
D.
3.2. Production and Supply
Estimates for the
D required to reach
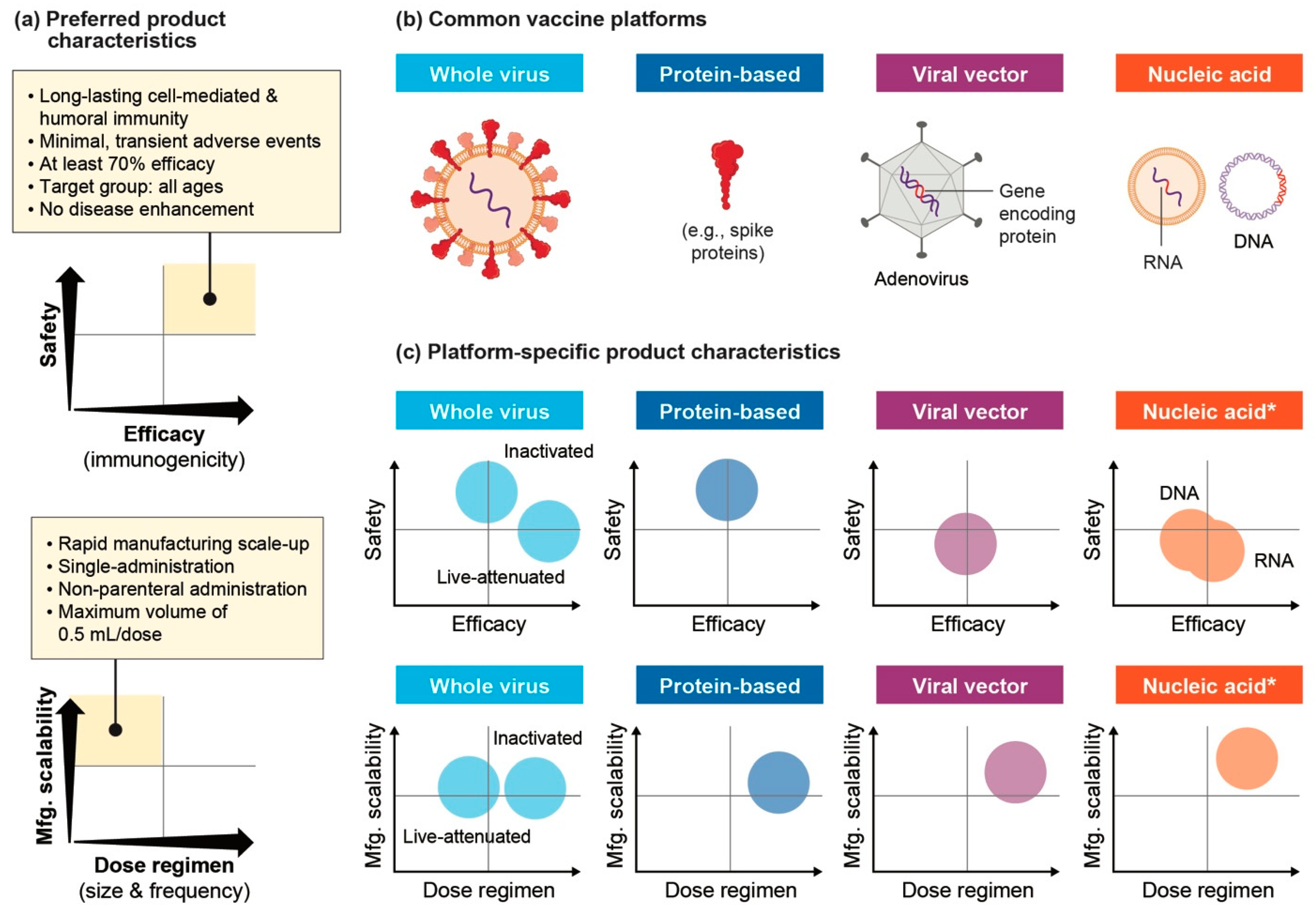
P highlight the unique challenge associated with scaling production and effectively supplying vaccines in a compressed timeline. There are numerous vaccine candidates being explored, both based on established platforms as well as novel technologies. Each brings unique opportunities and challenges to the goal of designing safe, effective vaccines for widespread use across geographies. Four primary platforms are: whole virus, recombinant protein-based/subunit, viral vector, and nucleic acid vaccines.
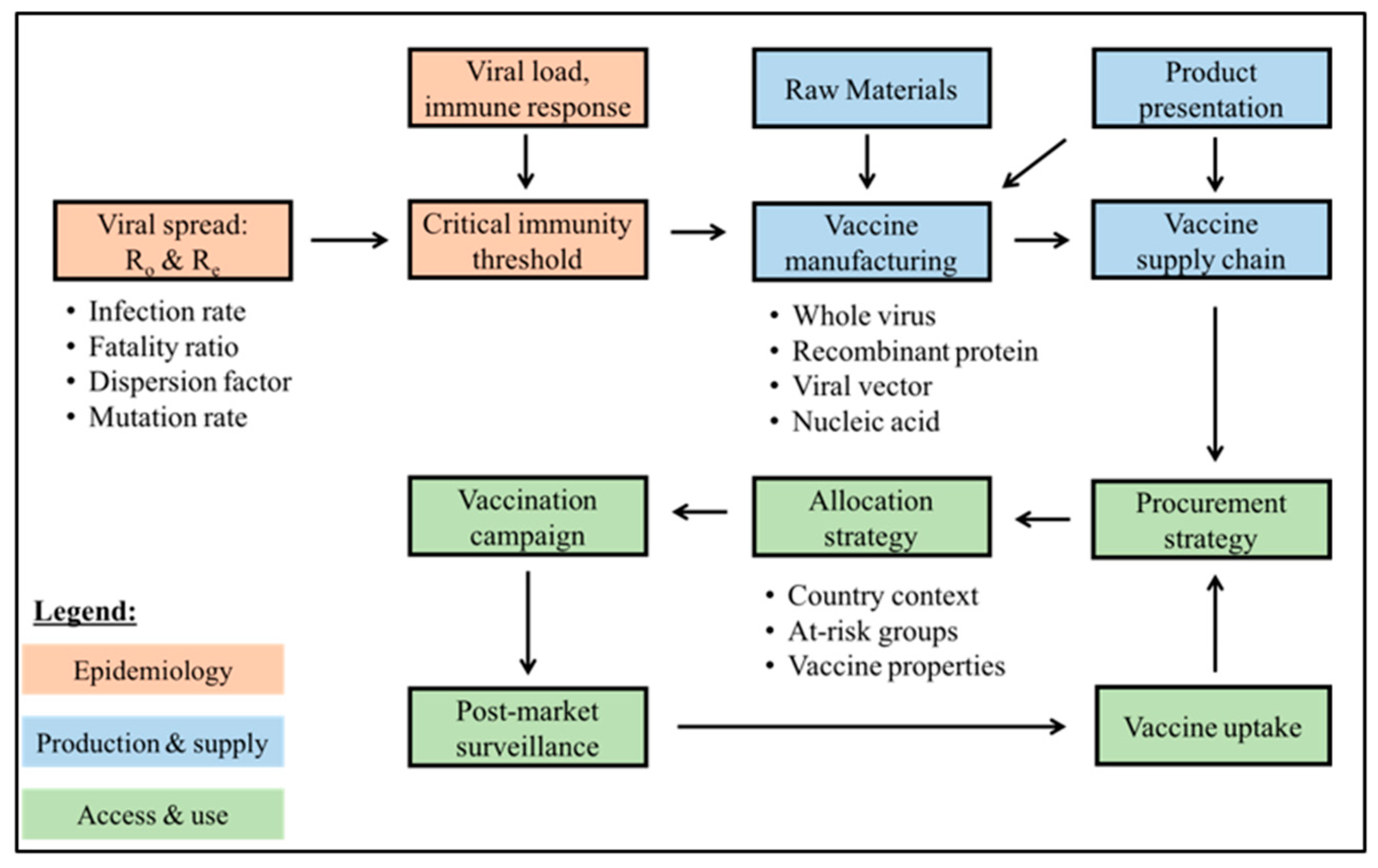
Figure 4 compares these vaccine platforms across key preferred product characteristics (PPCs), optimal product properties that can help meet strategic public health goals and subsequently inform more specific target product profiles. For example, low dose size, high production yield, temperature stability, and easy injection, among other factors, are ideal for global delivery. While PPCs are informative to compare vaccine platforms to the ideal product design, data from ongoing clinical trials will be crucial to better define the specific characteristics across different anti-SARS-CoV-2 vaccines. Whole virus and protein-based vaccines are considered safer as they have a long history as regulated and commercially marketed products. Live-attenuated vaccines most effectively induce a strong immune response, while other vaccine platforms rely on various adjuvants and product-specific properties to tune immunogenicity. All vaccine platforms, expect live-attenuated vaccines and some inactivated vaccines, have a high dose regimen as they usually require multiple doses for long-term immunity. The use of replication-defective viruses, both as antigens in vaccines and as vectors for transporting them, is ideal to reduce the risk of reverting to a virulent form after successive mutations that can occur when the virus replicates [
17]. Despite the relative novelty of viral vector and nucleic acid vaccine platforms, they may be faster to scale-up manufacturing compared to traditional platforms. Nucleic acid vaccines, for example, can made through catalytic chemical reactions rather than the typical, resource-intensive production in eggs or mammalian cells. Of the 200+ programs under development, whole virus vaccines are the least frequent while protein-based vaccines are most common [
18].
Regardless of the platform utilized, the vaccine development timeline from clinical trials through patient access is traditionally five years or longer. Given the current situation, the shared aim among manufacturers, governments, and other stakeholders is to work towards delivering vaccines within an expedited timeline of 12–18 months from when COVID-19 was declared a pandemic. This translates to an ambitious launch of prospective vaccines between Q4 of 2020 and Q2 of 2021. A significant challenge is the need for product and process development, clinical testing, and large-scale manufacturing to move forward in parallel rather than in sequence. This non-traditional approach to vaccine development introduces significant tradeoffs as decisions that would have been delayed until data becomes available are now being made at-risk.
The potential for significantly reducing the timeline for vaccine delivery can be attributed to a few factors [
20]: (i) pre-existing work to understand coronaviruses such as SARS and MERS, whose genomic and structural similarity to SARS-CoV-2 can help shorten discovery of vaccines and animal studies; (ii) re-prioritization of efforts and investments to support vaccine development (especially from governments, foundations, and the biotechnology industry); (iii) risk-taking by expediting the start of clinical phases despite limited knowledge about SARS-CoV-2 and simultaneously investing in large scale production capacity before safety and efficacy results are available; (iv) innovative trial designs; (v) using emergency provisions to expedite regulatory review; (vi) diversifying the portfolio of vaccine candidates, including novel platforms that have no regulatory precedence but may be faster to produce than traditional vaccines; (vii) increased levels of collaboration across stakeholders (e.g., government, industry, academia, foundations, etc.) to better understand the virus, develop the necessary production capacity, and make vaccines. To adequately demonstrate the effects of a vaccine, an adequate number of clinical trial volunteers are needed and clinical trial sites with sufficient transmission rates need to be selected. Innovative clinical trial designs have been suggested, such as the NIH-launched COVID-19 Prevention Trials Network, which allows comparison of protection across multiple vaccine trials in 100+ sites across the globe [
21].
The production of vaccines from raw materials, to drug substance, and eventual drug product is a time- and resource-intensive process, with each vaccine platform adopting unique manufacturing processes. Raw materials need to be qualified and in adequate supply to avoid bottlenecks in manufacturing. The risk of supply interruptions increases when raw materials are sourced from one country that may prioritize national use over exportation or when manufacturing equipment needs to be customized to specific manufacturing processes. Building in redundancy by having multiple qualified vendors from whom materials can be purchased can abate some of this risk to avoid delays in the production and eventual distribution of vaccines. Scale-up of raw materials supply chains for COVID-19 vaccines, especially critical components such as glass for vials and single-dose syringes, rubber stoppers, plastic bags for single-use systems, nucleotides, lipids, resins, filters, media, and freezer systems, among others, are a prerequisite to continuous, large scale manufacturing [
22]. There have been a growing number of bilateral agreements made between governments and vendors to secure raw materials in anticipation of a successful vaccine candidate. In all cases, demonstrating quality is essential to avoid variability in raw material properties that may eventually lead to deviations from a vaccine’s target product profile.
The production volume required to manufacture D can be estimated based on the expected dose size of the vaccine. Ongoing clinical trials play an important role in validating the ideal dose size that elicits the desired immunogenic response. Another important consideration is the ability to rapidly scale up manufacturing to produce billions of doses in the shortest timeframe. Bioprocess modeling can be used to determine the product volume per batch and per unit time based on a range of factors (e.g., cell line productivity, run duration, time between runs, batch success rate, production yield, titer, bioreactor number, volumetric capacity). Under normal conditions, there is a long lead time required to design, build, and validate new facilities that have unique production processes in place. In pandemic response, however, vaccine developers are exploring a combination of alternative options to rapidly secure the adequate manufacturing capacity to meet D: (i) retrofitting existing, unused facilities, (ii) optimizing scheduling in existing facilities, (iii) outsourcing less time-critical products to contract manufacturing organizations, (iv) scaling-out by initiating production in multiple sites in parallel, and (v) collaborating with foundations and governments to rapidly develop new capacity. Each of these has tradeoffs around cost, time to market, and risk that need to be considered before investments are made.
Formulation of the finished product should also be designed in such a way that enables easy distribution, as well as efficient delivery at the point-of-care. An important choice is the drug presentation, specifically whether the finished product is a liquid or lyophilized freeze-dried powder. For liquid formulation, single-dose or multi-dose containers can be filled with the drug product and sealed with sterile stoppers. Alternatively, single-dose glass syringes can be pre-filled ahead of distribution. In most cases, liquid formulation requires a cold chain that keeps products at a low temperature in order to maintain potency during transportation and storage. Lyophilization provides thermal stability and can help extend shelf-life, however, there is an elevated risk of deviations in product quality and efficacy when transitioning between liquid and solid states. For pandemic response, to reduce supply chain footprint and as a result of anticipated shortages in filling capacity, multi-dose vials are the preferred option although they may require an effective bacteriostatic agent to reduce risks of contamination that could lead to wastage [
23]. Ultimately, the choice of formulation will have substantial impact on the downstream product supply chain and performance of immunization programs. More evidence is needed on the impact of formulation choice, for example dose per vaccine, on factors such as operational and product costs, timely coverage, and safety [
24].
Another important consideration is maintaining integrity of the supply chain by preventing counterfeit (falsified) medicines, including both finished products (e.g., 2012 case of bevacizumab) or individual raw materials and active ingredients (e.g., 2008 case of heparin). The complex, multi-stage, and often opaque pharmaceutical supply chain provides ample opportunities for illicit activities and makes it difficult to effectively track-and-trace the source of problems. In response to the growing threat of falsified medicines, the WHO launched the Global Surveillance and Monitoring System in 2013 to encourage governments to more systematically report incidents in a common, structured manner. Additionally, various methods have been developed to detect falsified medicines: analytical chemistry and spectroscopy technologies (e.g., detecting chemical signatures of ingredients), as well as digital anti-counterfeit technologies (e.g., package-level barcodes and radio frequency identification). Reports of cyberattacks against the COVID-19 vaccine distribution chain, especially cold-chain companies, as well as online fraud linked to the marketing of fake products are emerging as vaccines start to receive regulatory authorization [
25].
The large manufacturing volume required to meet public health needs continues to be a rate-limiting step, meaning that typical operations may need to be displaced for some time. Looking forward, an important consideration is how manufacturing decisions impact the production timelines of other products, as well as strategically anticipating how investments made as part of a pandemic response can promote agility, business continuity, and proactive manufacturing systems in the future to better respond to unmet needs and new threats. Manufacturing and logistic models play an important role in promoting effective operations, especially considering the production scale, complex temperature requirements of most vaccines, and the impact product presentation can have on downstream transportation, storage, and delivery. Accounting for risks across the product value-chain is crucial to anticipate the time to reach the product volume D under different scenarios.
3.3. Access and Use
Closing the mismatch between supply and demand requires dynamic, responsive systems that integrate information around production, storage, transportation, and procurement. To make vaccines globally and equitably accessible, especially in initial periods of scarcity, clear allocation frameworks are also needed. A key performance indicator of vaccine supply chains is the continuous and uninterrupted availability of affordable products at the point of administration, especially when a large proportion of the population needs to be vaccinated. However, shortages or stockouts continue to jeopardize the delivery of many vaccines. In most cases, stockouts can be attributed to country-specific factors such as delays in government funding that restrict procurement, poor forecasting, and inefficient stock management. Understanding the root-cause of these stockouts can help anticipate potential barriers in the timely delivery of sufficient vaccine doses against SARS-CoV-2 when they become available. The primary objective of modeling efforts around the procurement and allocation of vaccines is determining the optimal strategy that will help reach P in the shortest time to meet public health goals.
In June, the WHO released a preliminary vaccine allocation framework to inform distribution within and between countries based on epidemiological and other country-specific factors [
26]. Such a framework aims to identify priority populations and inform the optimal use of scarce resources with the goal of reducing mortality and protecting health systems. Data can be used to further highlight geographies where the virus is most prevalent and health systems are most vulnerable. The initial allocation of products can then be fine-tuned based on the unique product characteristics of vaccines that become available over time, as they may only be suitable for certain sub-populations and geographies. Continuous learning based on available data is crucial to proactively and effectively plan vaccine operations across the value-chain.
An ideal global access program would allow all countries to engage in a shared mechanism for the procurement of products in a way that pools risks for both the manufacturers and governments. Such a system has been established in the form of an advanced market commitment (AMC) for vaccines, where investments from governments incentivize manufacturers to establish the necessary manufacturing capacity and produce substantial volumes of vaccines [
27]. This AMC, named ‘COVAX’, is co-led by Gavi (The Vaccine Alliance), the Coalition for Epidemic Preparedness Innovations (CEPI) and WHO, as part of a broader effort called Access to COVID-19 Tools (ACT) Accelerator. The financing framework provides volume guarantees to specific manufacturers for vaccine candidates before they are licensed. Since governments are likely able to substantially invest in only one or a few vaccine programs, each of which has an average success rate of 7% while in the pre-clinical phase (compared to 17% in Phase I, 21% in Phase II, and 67% in Phase III trials), the ability to invest in a portfolio of vaccine candidates provides insurance against the risk of failures [
28]. Although there has been extensive support for the AMC, there are a growing number of bilateral purchasing agreements between a single government (e.g., Operation Warp Speed in the US) or regional group (e.g., European Union) and manufacturers, leading to a risk of vaccine monopolies or a hoarding of vaccine supply in ways that delay access for low- and middle-income countries [
29]. As of December 2020, high-income countries held 3.9 billion doses and middle-income countries held 2.7 billion doses from confirmed bilateral agreements, while low-income countries continue to be entirely reliant on doses provided by COVAX [
30].
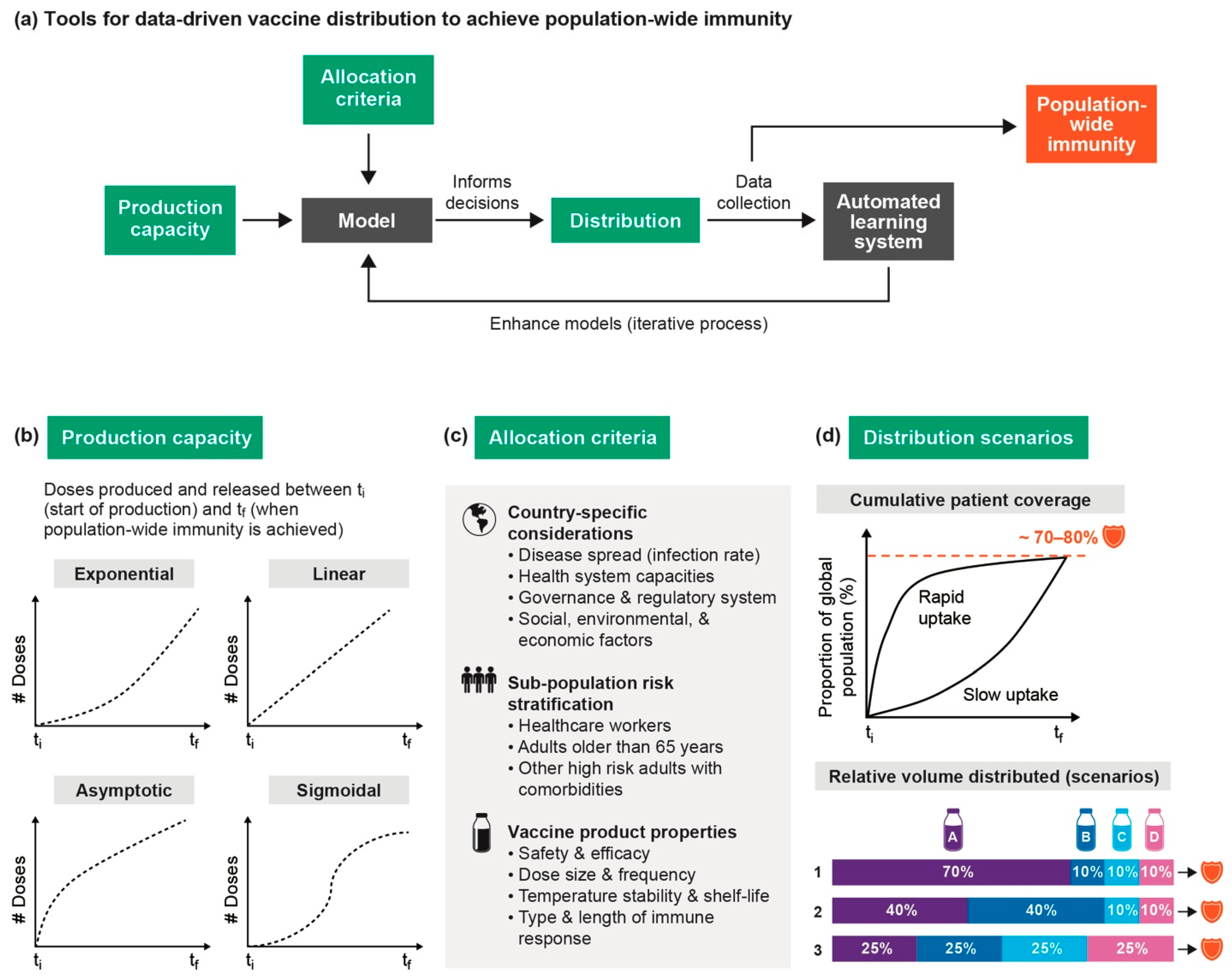
Figure 5a shows how various data-driven modeling tools can help evaluate the impact of different vaccine strategies based on production, procurement, allocation, and distribution behaviors of vaccines. For example, tools can be developed to stratify a population into risk groups based on various features (e.g., age, comorbidities, etc.). An assignment algorithm could then be built to allocate the most optimal vaccines based on country characteristics and product properties to the appropriate population sub-group.
Integrating real-world data into an automated learning system is particularly important to continually enhance models and inform decisions using evidence generated over time. While safety and efficacy will need to be demonstrated prior to regulatory approval, regardless of the vaccine, there is always some risk of an acceptable level of adverse events. Therefore, safety and efficacy across diverse populations needs to be demonstrated as large-scale vaccination campaigns begin. Adverse events following immunization can be categorized based on the severity (mild, moderate, and serious), the type of reaction they elicit (product-related reaction, quality defect-related reaction, immunization error-related reaction, immunization anxiety-related reaction, coincidental event), and frequency [
31]. To better understand the risks posed by a vaccine, differentiating coincidental events from those caused by a reaction to a vaccine can be done by comparing the background rate (determined prior to vaccination or simultaneously in non-vaccinated people) with the observed rate of an event.
Vaccination at the point-of-care also requires special attention. Depending on the vaccine presentation, the product may need to be stored at a specific temperature to maintain high quality throughout its shelf-life. The route of administration, the path by which a vaccine is brought into contact with the body, is particularly important since it may affect the flow of patients and skills needed by healthcare professionals to effectively deliver the vaccine. Parenteral dosage forms, the most traditional among vaccines, are administered as a needle-based injection in one of three following ways: intramuscular (especially common for vaccines containing adjuvants to avoid adverse effects), subcutaneous (between the muscle and skin), and intradermal. Most vaccines against SARS-CoV-2 have been designed for intramuscular injection. Non-parenteral vaccines can be administered orally, via intranasal spray, or through the skin using pressure by gas or electrophoresis, thus eliminating the need for needles and incentivizing great patient compliance due to self-administration [
32]. These delivery routes are appealing as mucosal surfaces can induce both mucosal antibodies (IgA) and cell-mediated immune responses, while still producing a systemic antibody response (IgG), though they are less efficacious and thus seldom used [
33].





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}





