1. Introduction
The declining trend in birthrates and an aging society has risen to varying degrees globally [
1]. For example, China, which hosts 18% of the global population, currently has nearly 200 million elderly people, but this number has been predicted to increase to more than 365 million by 2050 [
2]. Additionally, among this aging population, 115 million are expected to be at least 80 years old, and 600,000 are expected to be centenarians. With increasing age, the functions of the human body gradually decrease, and the physical and mental health of the elderly has increasingly become an unignorable global issue [
3].
Most people prefer to age in place as it allows them to maintain independence and autonomy, reduce social isolation and loneliness [
4] and enable them to stay connected to their social supports, such as friends and family [
5]. The living environment around a neighborhood often affects the physical and mental health of the elderly [
6]. Currently, due to historical, political, and economic reasons, old neighborhoods left over from the last century are prevalent in China. Due to factors such as the structure of early housing, the one-child policy, and the transfer of the young workforce, the elderly people living in these old neighborhoods often make up a large proportion of their population [
7].
Previous research on aging has shown that elderly people have recently started taking on increasingly greater responsibilities, whether at the social level (i.e., some countries delaying retirement age) or at the family level (i.e., more accession to the next generation of education) [
8,
9]. For example, in many parts of East Asia, multi-generational cohabitation is considered an ideal living arrangement. This “cohabitation and common wealth” of the family implies the establishment of mutual assistance and trust between members without an agreement; for example, many young people in China prefer to take their children to their grandparents for regular care [
10]. Under the double influence of educational responsibility and a decline in physical function, the health state of elderly populations in the skipped-generation household (SGH) tends to be highly fragile [
11]. Therefore, research on the health and well-being of these populations is urgently needed. Early research in the U.S. reported the adverse health effects of grandchild care [
12,
13], such as a reduction in life satisfaction [
14] and in physical function in the elderly [
13]; however, recent research in mainland China, Hong Kong, and Taiwan has found health advantages for grandparents who provide occasional, extensive, or custodial care for grandchildren. For example, caregiving grandparents experienced less depressive symptoms than their non-caregiving counterparts [
15,
16,
17]. However, in many developing areas, especially areas in China, the rapid development of urbanization has hollowed out many urban and rural areas in non-central cities, where local elderly individuals need to take more time to care for their family.
The impact of the built environment of old neighborhoods on the health of the elderly has recently become a research topic of interest. With a decline in their physical function, walking is a preferred activity for the elderly, making the outdoor spaces in these neighborhoods the main activity place for the elderly [
18]. These outdoor spaces host many necessary functions for the elderly, including outdoor sports, natural contact, and social activities [
19]. Previous studies have shown a potential relationship between the neighborhood environment and the health status of the elderly [
20,
21], but parenting behavior can increase the complexity of this relationship, both mentally and physically.
In China, old neighborhoods are defined as those built before 2000. In old neighborhoods, there is a high concentration of environmental problems and safety hazards, which can prevent elderly needs from being satisfied, and the health effects of these issues on the elderly are yet to be verified. The demographic composition of these neighborhoods is often complex, with their low land prices attracting many low-income people and increasing the severity of security problems; therefore, it is imperative to improve the neighborhood environment. The urban planning strategy of China is changing with the development of an aging society, and it would rather transform old neighborhoods than demolish them and rebuild [
22]. The environmental problems of old neighborhoods are complex, and the causal mechanisms of these problems also need to be analyzed in combination with specific situations to avoid developing solutions that are solely based on the appearances of these problems. However, practical experience has shown that the previous old community renewal practice expects too much and tries to solve the environmental problems overnight. Many scholars have questioned the sustainability of such unsystematically evaluated renovation projects [
23,
24], which easily obtained average results and ignored the core issues affecting the health environment of old neighborhoods. It is often valuable to explore the root causes of old neighborhood problems and conduct targeted transformations and upgrades according to the interactive relationship between various influencing factors. The objective of this study was to establish a novel evaluation system to assess the health of elderly families in old neighborhoods and to understand the relationships between the indicators to avoid waste in response to the future transformation of old neighborhoods.
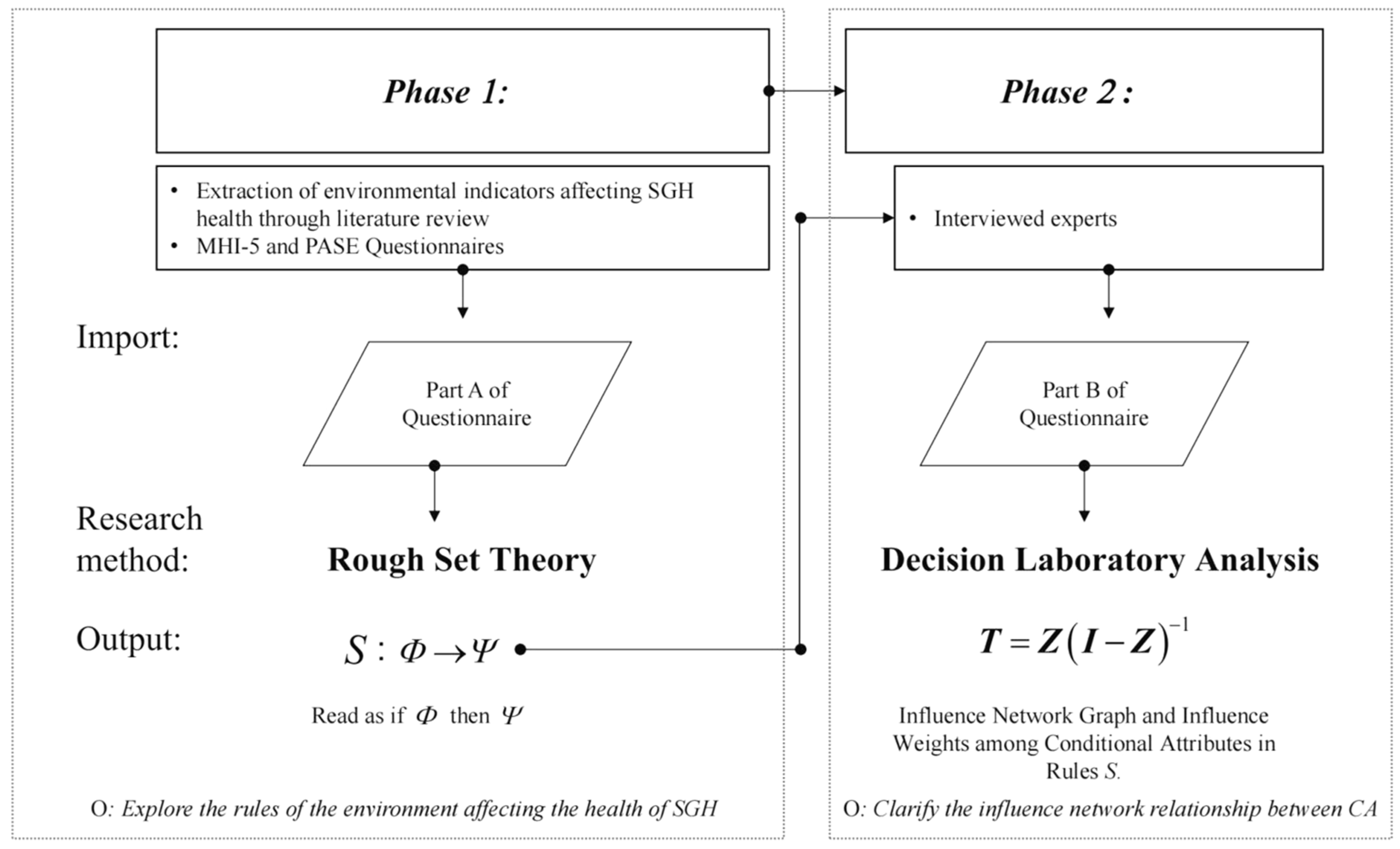
The study was designed in the following manner: First, an evaluation framework about the health level of the elderly living in SGHs and the neighborhood environment was built based on contemporary aging research. Second, the rough set theory (RST) technique was used to explore the core attributes of the environment that affect the health of local elderly people, and to clarify the hierarchical decision-making rules related to the health of elderly populations and environmental quality evaluation data (e.g., if–then). Third, decision-making trial and evaluation laboratory (DEMATEL) technology was applied to clarify the influence of network relationships between key environmental indicators based on contemporary knowledge in the field. Finally, hierarchical decision rules and the influential network relationship map (INRM) were integrated to develop renewal strategies for old neighborhoods.
2. Literature Review
Previous research has shown that most elderly people prefer to live in a familiar environment rather than an aged care facility [
25,
26,
27], and an increasing number of people choose to age in place in their later years; in other words, they prefer to “live in a neighborhood, with dignity and independence” [
28]. Sociologists believe that “aging in place” is the most humane and cost-effective way for elderly people to age because it avoids the trauma and hassles associated with over-caring for elderly people [
29]. Elderly people who live in their own homes have higher satisfaction and lower levels of depression, and can better maintain their physical function than their assisted-living counterparts [
30].
Zhou et al. [
31] believe that aging in place is one of the essential reasons for the formation of an aging neighborhood. In some aging and increasingly populated neighborhoods, economic status, the living environment, employment, and other factors have motivated some young people to be very inclined to leave. Contrarily, most of the elderly population choose to stay because of the familiar living environment and their social networks. Gradually, the elderly people who remain in these neighborhoods become their main demographic, which explains the aging of many older neighborhoods. The deterioration of the quality of the environment and the facilities within a neighborhood is inevitable over time, and this change is often difficult for the elderly to detect; however, it cannot be ignored that these environmental factors have a significant impact on the physical and mental health of elderly people [
32].
Furthermore, there is a high abundance of SGHs in the demographic structure of these older neighborhoods, and child-rearing in SGHs is becoming an essential challenge for healthy aging in China. The declining socioeconomic status of the elderly, limited social and family support, and deteriorating physical functions make their health highly sensitive and vulnerable to skip-generation parenting [
33,
34]. Notably, the parenting situation of children in intergenerational families is a global phenomenon not limited to China. Moreover, grandparents are often important in the education of their grandchildren, with previous research suggesting that older adults are highly likely to experience parenting pressures in such situations. This might be a consequence of several factors, including behavioral problems of the grandchildren [
35,
36], a lack of family competence (e.g., inability to solve problems, express emotions, and facilitate individual autonomy), the poor health and emotional well-being of the primary caregivers [
37,
38,
39], and the transition of the grandparents into becoming primary caregivers for grandchildren [
40,
41]. Research from Australia suggests that the regular care of grandchildren, especially grandparents with infants and young children, can be a burden, both physically and emotionally [
42]. Additionally, some studies have found that caring for grandchildren sometimes disrupts finances or reduces the time that the grandparents commit to leisure and social activities, which can increase their feelings of loneliness and social isolation [
43,
44].
Many previous quantitative studies on the health of the elderly have used statistical methods [
45,
46,
47], with some scholars having used data mining methods in their research on elderly healthcare [
48]; however, there are often complex and non-negligible mutual influences among the environmental elements. Therefore, Zhu et al. [
49] use the DANP-V method in multi-criteria decision-making to explore the continuous improvement in the health and well-being of the elderly that is caused by environmental improvements.
The behavioral and social behaviors of the SGH elderly are not the same as those of their non-SGH counterparts, and the intergenerational parenting behavior of children has undoubtedly increased the complexity of the impact of the neighborhood environment on their health. The physical and mental health of SGH inhabitants affects their well-being later in their lives, and the education and growth of the next generation; therefore, contemporary research regarding elderly health and the neighborhood environment informs us that it is necessary to study the health of this population. Furthermore, previous research suggests that neighborhood environments may be positively associated with the longevity of elderly lifespans [
6]. Wiles et al. [
50] acknowledge that the environmental elements of the neighborhood and its social activities have important effects on the health of elderly people, and Buffel et al. [
51] strengthen the public understanding of the needs of elderly people in the communities by examining the physical environment (infrastructure, transportation, and housing) and social dimension (civic engagement, neighborhood care, and support). Additionally, Wahl and Weisman [
52] emphasize the importance of enhancing recreational opportunities, amenities, and transportation to promote physical activity and the social interactions among elderly people. Some scholars have also studied the relationship between specific neighborhood environmental factors and the health of the elderly, including traffic and street safety [
53], green and blue space design [
54,
55], friendly slow walking [
56,
57], multifunctional space design [
58], social relationships [
59], public transport connectivity, and accessibility [
60,
61]. Several studies have also highlighted the positive effects of a good neighborhood environment on the health of elderly people, such as improved physical activity levels [
62], reduced stress and depression [
63], increased social interaction networks [
64], and an enhanced sense of belonging in the neighborhood [
65]. To sum up, through the review of previous studies, this study summarized the neighborhood environmental factors that have a key influence on the health of the elderly (see
Table 1).
3. Methodology
In old neighborhoods, there are multiple physical environmental indicators related to the health and well-being of older adults, which have been introduced into different dimensions in previous studies. To improve the physical environment of these old neighborhoods, it is crucial to clarify the core design attributes that can significantly affect the physical and mental health of the elderly. Similarly, it is necessary to understand the perception and behavioral habits of the elderly as they relate to the material environment indicators of the neighborhood, and also relate to the knowledge of the relationship between behavioral rules and the enhancement of their health. Previous research has focused on analyzing and discussing the resulting data. The construction of the environmental factor system and the analysis of its influence relationship in the decision-making process are predominantly based on expert experience (i.e., expert domain knowledge) [
19,
70,
71]; however, few studies have considered the natural behavioral patterns (i.e., behavioral laws) that govern real-world survey data results. This study is based on the assumption that these two key points have different characteristics and needs. If the two fields can be effectively integrated, the vision of policymakers working on the renewal of old neighborhoods will be widened, which may formulate highly suitable and less resource-intensive optimization strategies and programs.
Based on a review of the relevant literature and an investigation of empirical cases, this research aimed to reduce the initial summarized environmental indicators and retrieve their core attributes. We also aimed to clarify the perception and behavioral habits of the elderly regarding the elements of the material environment in the neighborhood and their knowledge of behavioral laws that affect their physical and mental health. In previous studies, RST has been widely used across multiple fields to address the imprecise knowledge relationship between conditional and decisional attributes in classification functions [
72,
73]. This theory does not require prior information about the probability distribution of the data and can evaluate both the quantitative and qualitative properties. There are important complex influences on network relationships among these reduced environmental indicators (i.e., conditional attributes). This study aimed to elucidate the factor that most influences the critical issues in relation to the formulation of strategies for improving the physical environment of old urban neighborhoods [
74,
75]. The most significant feature of the DEMATEL method is that it can clarify the influence of network relationships in an index/element system based on expert domain knowledge, which has allowed it to be employed successfully in many situations; this includes marketing strategies, public health management, tourism destination creation, and capacity development for group decision making [
76,
77]. The design and process of this study are illustrated in
Figure 1.
3.1. RST
RST, proposed by Pawlak in the 1980s [
78], is a mathematical tool capable of identifying hidden patterns in data, recognizing partial or total dependencies in databases, and removing redundant data [
79]. This theory uses two exact sets, that is, the lower and upper approximation sets, to approximate the bounds of a classification function based on an equivalence relation, which is adopted from the relationship between attributes. Therefore, when the number of objects in these two groups is equal, the current data with conditional attributes can express the bounds of the classification function; otherwise, the bounds are ambiguous. The gap between these two approximate sets is called the rough set, and the theory uses set theory to describe the relationship between attributes; this allows it to be transferred from basic behavioral rules in real datasets to knowledge rules (e.g., if–then), used to study fuzzy, uncertain, and flawed data and to develop a preliminary management framework. RST technology has been widely used in data exploration, machine learning, big data, gene expression data analysis, and other fields.
3.1.1. Sampling Strategies/Data Sources
This research used data collected via a questionnaire, and the data information source was selected from the Che Bei neighborhood, Guangzhou, China. The Che Bei neighborhood, established in the early 1980s, is located in Tianhe District, covers an area of 5.6 km
2, and is a typical neighborhood located at the urban–rural junction. There are many inexpensive rental houses, which has led to a complex population composition in this area. A recent census showed that the residential and local populations were 102,787 and 30,759, respectively, with 3996 people over the age of 65, that is, 13% of the total population (China Census Data 2021
https://www.hongheiku.com/lpxzsj/38135.html (accessed on 28 February 2020).).
The questionnaire was divided into two parts, with the first part including environmental and health-related factor indicators as the conditional attributes (CA), which were compiled from previous work. Five semantic scales were used to describe the relationship between each index and elderly activity. In the second part, Mental Health Inventory-5 (MHI-5) and Physical Activity Scale for the Elderly (PASE) questionnaires were used to test mental state, physical function, and exercise intensity as the decision attributes. The MHI-5 questionnaire is commonly used to test the general mental health and well-being of elderly people [
80]; the PASE questionnaire combines information on leisure, family, and occupational activities, and connects the questionnaire scores with physiological characteristics and physical health status [
81,
82]. The health benefits of engaging in moderate-to-vigorous physical activity are widely recognized for the elderly, with regular exercise positively influencing cognitive ability, limiting cognitive aging, and reducing the risk of Alzheimer’s disease and related dementias [
83,
84].
The questionnaire was completed in November 2021, and its results are presented in
Table 2. Overall, 655 questionnaires were distributed, including 384 that were distributed to elderly people who completed skipped-generation childcare tasks. After excluding missing, incorrect, and incomplete questionnaires, 242 valid questionnaires were obtained.
3.1.2. Computational Process
RST is presented as an information system on which our analyses were based. The information system can be symbolically represented as
, where U is the universal set consisting of every finite set of objects, and A is a collection of attributes. Each attribute equation,
, defines a message function with
. Among these attribute equations,
VA is a set composed of attribute “a” values, which becomes the value range for attribute “a”. Furthermore, when analyzing a dataset, objects and the relationships between them become indistinguishable because they contain the same information in some attributes; this can also be called an indiscernible relationship,, and they belong to the intersection of the same classification. The associated equivalence relation is defined in Equation (1) for any condition attribute subset where
.
Two rough sets, that is, the upper and lower approximate boundaries, represent the uncertainty of the data. For as long as possible and partially included, the individual is classified into the upper approximate boundary set; however, for the lower approximate boundary set, the individual can be included entirely within it.
Assuming that the set
X is a partial set of the universe set
U, and
A is a certain attribute set, the upper approximate boundary
and the lower approximate boundary
are defined by Equations (2) and (3), respectively:
The set of indispensable attributes found in the data material is called the core attribute. RST uses simplification to represent the attribute-reduced set, removes unnecessary attributes, and finds a relatively smaller set with a similar or the same classification ability as the original set. After the attribute simplification process, redundant attributes were deleted without reducing the classification ability.
Simultaneously, we can use the concept of upper and lower approximation bounds to establish data classification rules and to measure the certainty of data classifications with the accuracy of the approximate set. If a set has a bounded set in the equivalence relationship of A, it still has objects that cannot be classified as belonging to the set or not belonging to the set under the information of A. Therefore, the greater the number of elements in the bounding set, the lower the accuracy of the approximation set. The accuracy of the approximate set
X is defined as follows:
Decision rules are a methodical way to describe a new decision table formed after attribute reduction, and the rules of the decision table are defined as follows:
In Equation (5), Φ and Ψ represent the condition and decision attributes, respectively. After the decision rules are derived, they can be reduced to make the analysis highly efficient. This can be achieved through the minimum decision rules. The so-called minimum decision rules use minor conditional attributes to represent the rules.
3.2. DEMATEL
The DEMATEL method was developed by the Banelle Memorial Institute of Geneva between 1972 and 1976 for the Science and Human Affairs Program [
85]. This method is used to solve complex and tangled decision-making problems, and can improve the understanding of particular problems and clarify the source of their influence [
86]. The direct influence matrix was constructed through the relationship between the indicators in the system, and then the centrality and causality of each indicator were calculated. The critical indicators of the entire system can be identified by identifying the status, function, and system function of the influencing factors. This method is effective for evaluating and identifying the relationships between factors and is suitable for studying the interactions between factors in a complex system. As such, it has been widely used in many research fields, such as planning scheme selection, competitiveness analysis, and comprehensive system evaluation.
3.2.1. Sampling Strategies/Data Sources
The DEMATEL questionnaire consists of two parts: one is about the relationship between the environmental indicators that affect the mental health of SGH elderly, while the other concerns the physical health of SGH elderly. We then looked for experts with a background in aging and community environmental studies, who were randomly selected and invited to complete the questionnaire via email or phone. The reliability of the questionnaire was tested, and data collection was continued until the test results exceeded 95%.
The questionnaire about the relationship between the environmental indicators that affect the mental health of these SGH elderly in old neighborhoods consisted of four indicators from RST analyses. The reliability test result from the 11 questionnaires was 99.79%, which is above the threshold value of 95%. Moreover, the questionnaire about the relationship between the environmental indicators that affect the physical health of the elderly living in old neighborhood SGHs consisted of 10 indicators from RST analyses. The reliability test result from the 11 questionnaires was 97.2%, which is above the threshold value of 95%.
3.2.2. Computational Process
Experts converted the experience of real society into values representing the degree of interaction influence within the model structure using a Likert scale (1, no influence; 2, very low influence; 3, low influence; 4, high influence; and 5, very high influence). We then built an
non-negative value direct influential relation matrix
Y, where
represents the degree of influence from rule
i to rule
j, and
e is the order number of experts, as follows:
Integrating the direct relationship matrix
Y of expert
e, the initial direct influential relation matrix
A representing the experience of
e experts can be obtained (as shown in Equations (7) and (8).
We then built the boundary of the influence matrix through the initially direct influential relation matrix
using Equations (9) and (10). The influence values of the influence relationship matrix were all between 0 and 1. The normalized direct-relation matrix
was obtained, with minimum and maximum total values of 0 and 1, respectively.
The normalized direct-relation matrix
obtains the total impact value of the attribute, which are the influence and indirect impact values of the attribute by Equation (11).
Finally, the sum of the attribute columns is the sum of the attribute influence degree , and the sum of the attribute rows is the sum of how much the attribute is affected in the total influence relationship matrix T. represents prominence, that is, the degree of attribute association, and is relation, indicating the significance degree of the attribute influence. Additionally, this method of quantifying the system structure relationship can effectively simplify the correlation between the complexity of indicators and make it easier to understand the structure of the system.
4. Results and Discussion
4.1. Mental Health of the Elderly Living in SGHs in Old Neighborhoods
Based on the collected questionnaires, the mental health questionnaires of the elderly were scored on five scales. The mental health questionnaire scores were distributed in the range of 1 to 100. The MHI-5 questionnaire has only five questions; thus, it is easy to obtain the same score. Therefore, the mental health questionnaire used scores as the basis of this segmentation. That is, 0–19 was 1 point (worst), 20–39 was 2 points (poor), 40–59 was 3 points (ordinary), 60–79 was 4 points (better), and 80–100 was 5 points (excellent). The final scores are presented in
Table 3.
The quality of our classification of mental health status as a decision attribute was 0.9669. The core attributes were X
7 (walking) and X
8 (when you take your children into the neighborhood). The number of rules if
Φ then
Ψ was 103, and by selecting the rules that included core attributes and interpretation rates greater than 5%, we found the results shown in
Table 4.
The daily outdoor activities of the SGH elderly were primarily walking, with little and no equipment (anaerobic and aerobic exercise, respectively). They were required to be accompanied by others for their walking activities. When the environment and safety conditions of their walking routes were inferior, they could be put into a poor state of mental health. The SGH elderly whose daily primary travel mode is walking and who partake in childcare activities outdoors have very poor psychological health. This result was consistent with that of a previous study. The SGH elderly whose daily outdoor activities involve some sports equipment (anaerobic exercise), who live in neighborhoods with basic public cleaning facilities and green facilities with good shading, and who often visit riverside spaces for childcare activities have good mental health.
The interrelated environmental indicators of the mental health of the SGH elderly living in old neighborhoods are as follows: traffic and street safety, green and blue space designs, friendly slow walking, social relationships, physical activity ability, clean and sanitary facilities, and public transport connectivity and accessibility.
Friendly slow walking, traffic, and street safety are critical indicators of old neighborhoods that have a high proportion of SGH elderly. The worst psychological health status of the elderly can be avoided if these two indicators perform relatively well. As a result, the economic and energetic investments of policymakers and designers in these two indicators can receive relatively high returns when transforming old neighborhoods. Simultaneously, green space design and social networks also positively impact the mental health of the SGH elderly, which cannot be ignored when renewing old neighborhoods. Additionally, physical activity and clean and sanitary facilities can improve the mental health of the SGH elderly. If only the mental health level is considered, relevant resources can be invested in other influential indicators.
4.2. Physical Health of the Elderly Living in SGHs in Old Neighborhoods
The distribution of the physical function questionnaire scores ranged from 0 to 348. Because this study explored the relationship between neighborhood environment indicators and the physical health of the SGH elderly, the performance significance of a score of 0 represented no activity; therefore, questionnaires with a score of 0 were regarded as invalid. The score on the physical function questionnaire was divided by the slope of the data distribution, where similar slope data had the same score; this avoided an excess of the same score and reduced the impact of extreme values on score segmentation. The final score segmented as 0–17 was 1 point (worst), 18–46 was 2 points (poor), 47–102 was 3 points (ordinary), 103–136 was 4 points (better), and 137–348 was 5 points (excellent). The results are shown in
Table 5.
The quality of the classification when physical health status was a decision attribute (D) was 0.9339, and the core attribute was X
1 (What do you usually do when you use the square space?), X
6 (What is most likely to be affected by green space in the neighborhood?), and X
7 (What is your state of walking?). The number of rules if Φ then Φ was 97, and by selecting the rules that included core attributes and interpretation rates greater than 5%, we found the results listed in
Table 6.
The SGH elderly usually walk alone and engage in rest and social activities on the riverside. When public resting facilities are poor, their physical health status is also poor. The SGH elderly whose primary conduct in square space is childcare and who usually take the riverside space as the main traffic path are in poor physical health. The SGH elderly who take their children for daily walks and value family ties and cultural identity in relation to a sense of belonging in a neighborhood have poor physical health. The SGH elderly who are involved in planting habits and are engaged in child-rearing behaviors in riverside spaces are also in poor health. The SGH elderly who like physical exercise, tend to travel by bus, and live in a neighborhood with green spaces that provide a good breathing environment and basic public resting facilities are in excellent physical health. The SGH elderly with a good walking environment and a neighborhood with green facilities that provide excellent shading, a relatively private environment with equipment for exercise, and clean sanitation facilities, are also in excellent physical health. The SGH elderly who consider walking as their leading outdoor activity, partake in less exercise with equipment (anaerobic exercise) while caring for their children, and live in a neighborhood with clean and sanitary facilities have good physical health.
The interrelated environmental indicators of the physical health of the SGH elderly living in old neighborhoods are as follows: traffic and street safety, green and blue space designs, friendly slow walking, multifunctional space design, social relationships, physical activity ability, neighborhood sense of belonging, clean and sanitary facilities, public transport connectivity and accessibility, and public resting facilities.
The indicators of green space design (A2), blue space design (A3), friendly slow walking (A4), multifunctional space (A5), social relationship (A6), public transport connectivity and accessibility (A7), and neighborhood sense of belonging (A11) are the potential factors that affect the poor physical health status of the elderly. Among them, blue space design (A3), friendly slow walking (A4), and social relationships (A6) had a higher frequency; therefore, ensuring that these three indicators are at a relatively high level can effectively avoid the poor physical health of the SGH elderly. Furthermore, physical activity ability (A8) had a high positive correlation with the physical health degree of the SGH elderly, and the improvement of green space design (A2) and the quality of clean and sanitary facilities (A12) also contributed significantly to the health degree of the elderly. Additionally, friendly slow walking (A4), public transport connectivity and accessibility (A7), and public resting facilities (A13) have a potentially positive effect.
4.3. INRM about the Mental Health of Elderly Living in SGHs
According to the DMATEL calculation, the relationship matrix
T of the environmental indicators related to the mental health of the elderly in the SGH is shown in
Table 7.
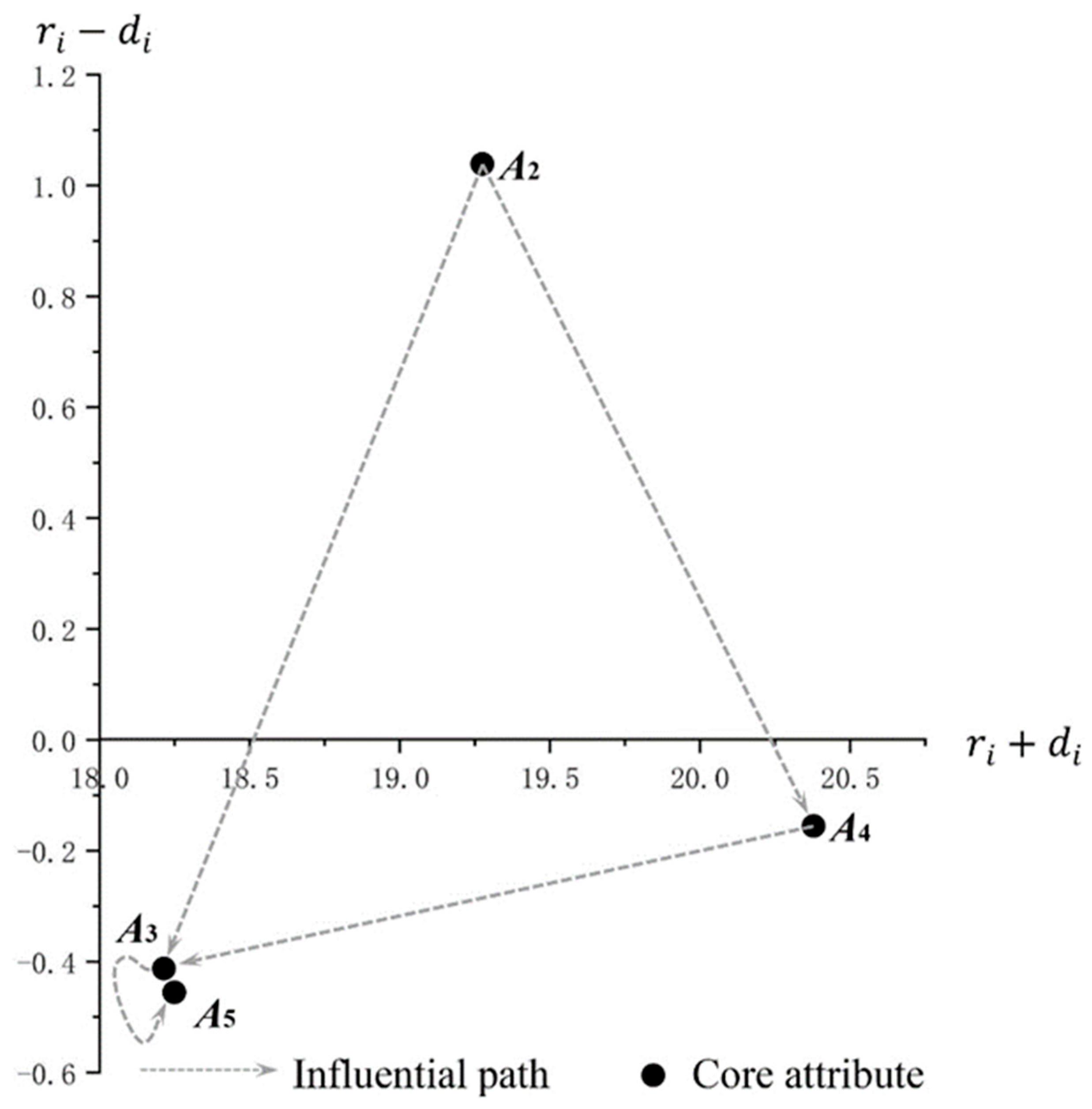
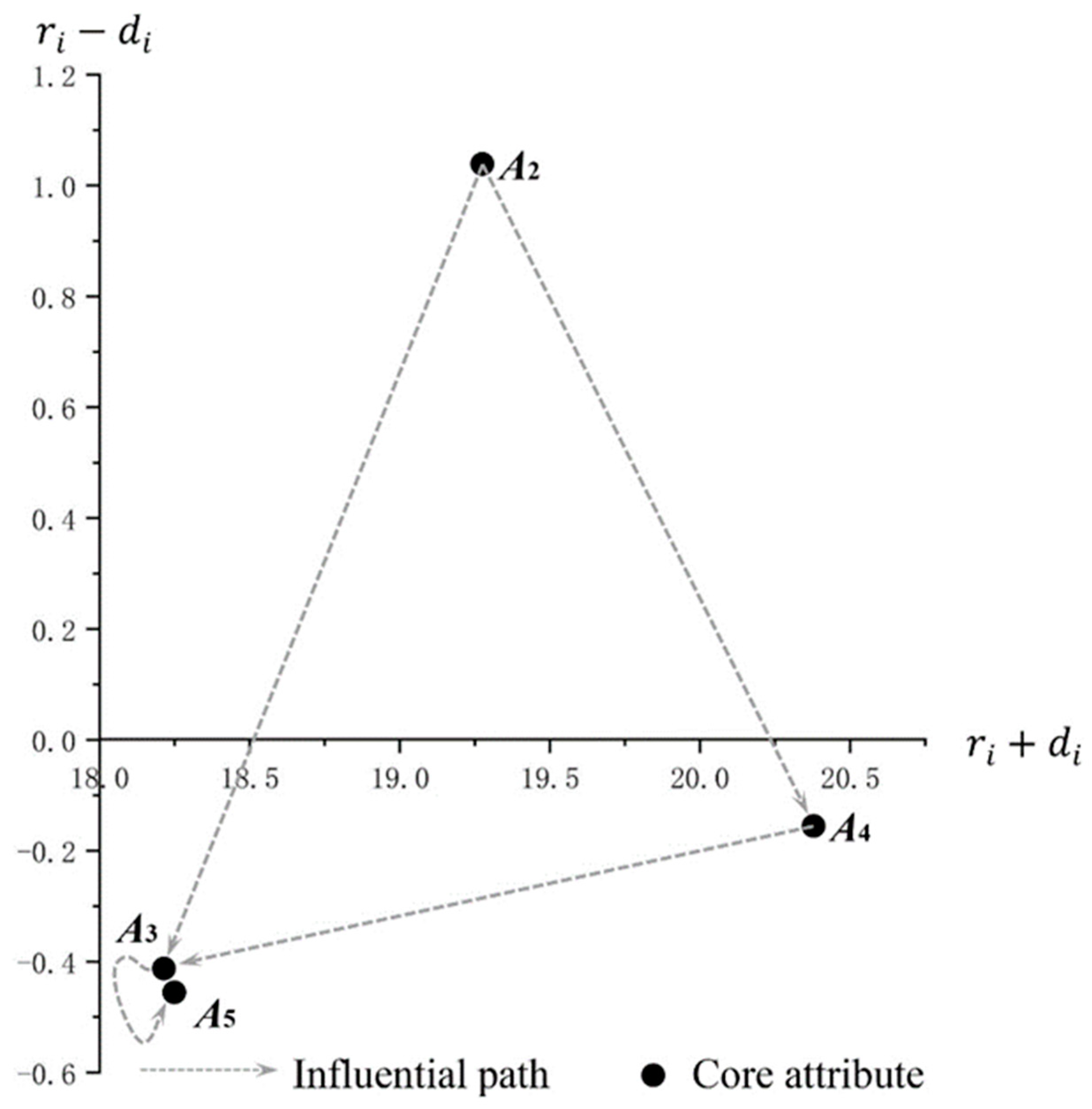
As shown by the INRM (As shown in
Figure 2), the most prominent factor was friendly slow walking (A
4), followed by green space design (A
2), and the lowest was blue space design (A
3) and multifunctional space (A
5). In terms of the indicator relationships, green space design (A
2) had a positive impact on the other indicators; friendly slow walking (A
4), blue space design (A
3), and multifunctional space design (A
5) were passive influences in the system. Moreover, blue space design (A
3) and multifunctional space design (A
5) were lower than friendly slow walking (A
4). Therefore, green space design (A
2) had a dominant positive influence on other indicators, and the influence of green space design (A
2) on friendly slow walking (A
4) was much more significant than the interaction relationship among other indicators.
Therefore, green space design (A
2) was a critical environmental factor that affected the mental health of the SGH elderly. When it changed, it inevitably affected other indicators. Coldwell et al. [
87] observed that greenery in the surrounding environment protects against adverse mental health effects. Green spaces can reduce depression and anxiety by improving the personal quality of life and reducing personal stress. In old and poor communities, green space is conducive to reducing the psychological pressure on community residents and has a specific correlation with residential mental health [
88,
89]. The blue space design (A
3) is also a core indicator; however, some studies believe that compared with green space design, blue space design is more suitable for the mental health of the elderly, especially for its anti-depression characteristics [
55]. However, this indicator is a passive influence in INRM and may be related to the parenting behavior patterns of the elderly in SGHs and the characteristics of the study area. These older adults must consider factors such as the activities and safety of the children, and the caregiving behavior of community activities. Notably, the blue space design (A
3) and multifunctional space design (A
5) were in relative proximity in terms of both prominence and relation; this is because of the RST results of only four local environmental indicators related to the mental health of the SGH elderly. Although blue space design (A
3) and multifunctional space design (A
5) were highly correlated, there was a close mutual influence relationship. Based on the above results, the quality of green space design is dominant for the mental health of the intergenerational elderly, and policy and resource investment into this indicator can effectively improve the other three indicators to achieve overall systematic improvement.
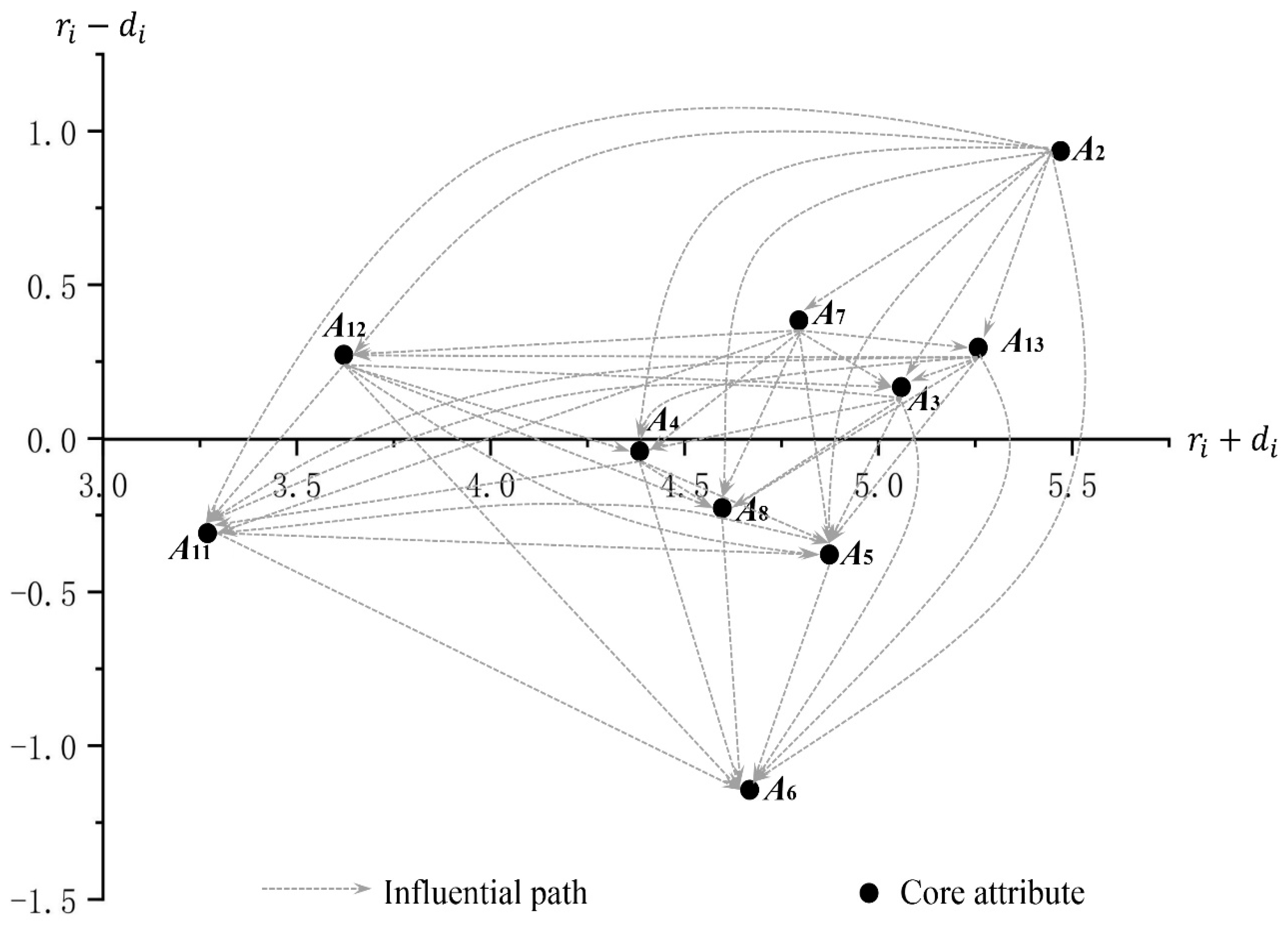
4.4. INRM about the Physical Health of Elderly Living in SGHs
According to DEMATEL calculation, the relationship matrix
T of the environmental indicators related to the physical health of the elderly in SGHs is shown in
Table 8.
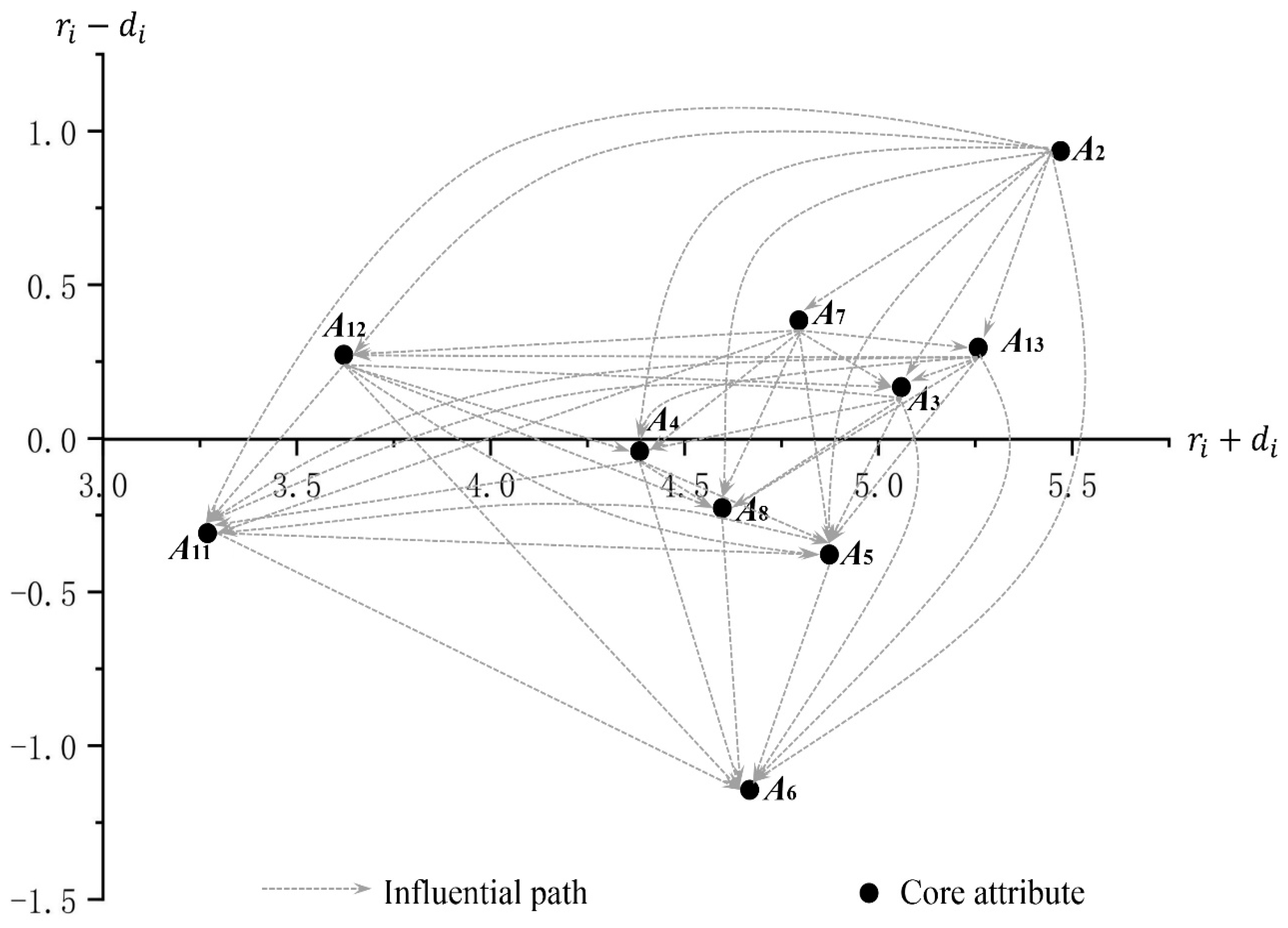
The results are shown in
Figure 3, with green space design (A
2), public resting facilities (A
13), and blue space design (A
3) having the highest prominence (5–6); clean and sanitary facilities (A
12) and a neighborhood sense of belonging (A
11) are the lowest (3–4); and the other indicators are located in the middle segment (4–5). Overall, green space design (A
2) was the highest relation indicator, which was consistent with that of mental health. Social relationship (A
6) was the lowest indicator compared to its influence, and the other indicators had the most significant influences.
Green space design (A
2) was the highest indicator of prominence and relevance. It is the core indicator in the evaluation system, and the results are the same as those of the mental health questionnaire for the SGH elderly. INRM shows that it has a higher impact on other indicators in the system, which is consistent with previous research results, such as green space improving personal physical activity levels [
90]. Wan et al. [
91] posited that green space design can enhance social activities and a sense of community belonging by improving the environmental quality, personal environmental perception, and the interaction mode. Fan et al. [
92] highlighted the relationship between green space design (A
2), blue space design (A
3), and public transportation accessibility (A
7) [
93]. Policymakers should consider this, as changes in this indicator will primarily affect the other indicators in the system. Neighborhood belonging (A
11) was the least significant indicator as it is a relatively vague concept that depends on the cognitive abilities of an individual [
94]. Through analysis, we showed that this indicator is at the edge of the system, and its value is less than 0, making it a passive influence; therefore, considering the investment effect, this indicator had the lowest priority. Based on the INRM, social relationships (A
6) were the lowest indicator. As other indicators had the most significant impact, the change in this indicator occurred in a state positively correlated with the final physical fitness of the elderly, which is consistent with the results of previous studies [
95]. Additionally, the indicators of public resting facilities (A
13), blue space design (A
3), public transport connectivity and accessibility (A
7), and clean and sanitary facilities (A
12) had a value greater than 0, making them indicators that positively affect the system; thus, the improvement of these would help improve the evaluation system. In contrast, for multifunctional space design (A
5), physical activity ability (A
8), and friendly slow walking (A
4), the values of these indicators were less than 0, making them indicators that negatively affect the system; the improvement of these would have a limited impact on the overall system evaluation.
5. Conclusions
This research explored the relationship between neighborhood environmental indicators and SGH elderly living in old neighborhoods. Recommendations were provided for future neighborhood renewal plans to avoid wasting resources. Based on the RST analysis, two results on the mental and physical health of the SGH elderly were obtained from the 655 questionnaires. By clarifying the interactive relationships between various environmental elements, we created an INRM based on DEMATEL. In the research model, the higher the prominence value, the higher the core degree of the indicator, and the higher the relation value, the stronger the active influence of the indicator on the other indicators. Therefore, when the values of both indicators are high, the change in the indicator has a very significant impact on the model. Our research results showed that green space design (A2) is at the top of the two values in the physical and mental health model of the SGH; therefore, this indicator is the core attribute that affects the physical and mental health of elderly people living in SGHs. Blue space design (A3) and multifunctional space (A5) have small prominence values in the mental health model and are at the edge. Moreover, in the physical health model, their prominence values rank third and fourth, respectively, and the relation value of the blue space design (A3) was higher than that of the multifunctional space (A5). Although friendly slow walking (A4) had the highest prominence value in the mental health model, the relation value was negative and highly affected by green space design (A2). In the physical health model, the prominence and relation values of this indicator were relatively small, and its impact on the model was limited. Additionally, public resting facilities (A13) and public transport connectivity and accessibility (A7) had high prominence values and positive relation values in the physical health model; therefore, these two indicators also had a practical impact on the physical health of elderly people living in SGHs. Notably, these results were based on studies within the landscape ecology category. The impact of environmental indicators on the health of the SGH elderly is limited. An aging society is a complex issue, and future research should consider factors such as policy, economic status, medical conditions, and neighborhood management in order to effectively improve the health level of the SGH elderly.
This study has some limitations, including in the MHI-5 and PASE questionnaires, in investigating the physical and mental health status of the SGH elderly; however, the two questionnaires were operable and could reflect the actual mental and physical status of the tested population. The exact values of the physical indicators of the elderly, such as height, weight, and blood pressure, cannot be measured. There is insufficient data for a more accurate assessment of the health of the SGH elderly. This was a cross-sectional study conducted on the sample population extracted over time, and the collected data had a certain timeliness. This study addresses the aging society of the Chebei neighborhood in Guangzhou; however, the research model can be applied to similar studies, and the dynamic system model can be widely used in future research on an aging society.





{kind=link}
{kind=link}
{kind=link}