Evaluation of Inflammation Caused by Cardiopulmonary Bypass in a Small Animal Model

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
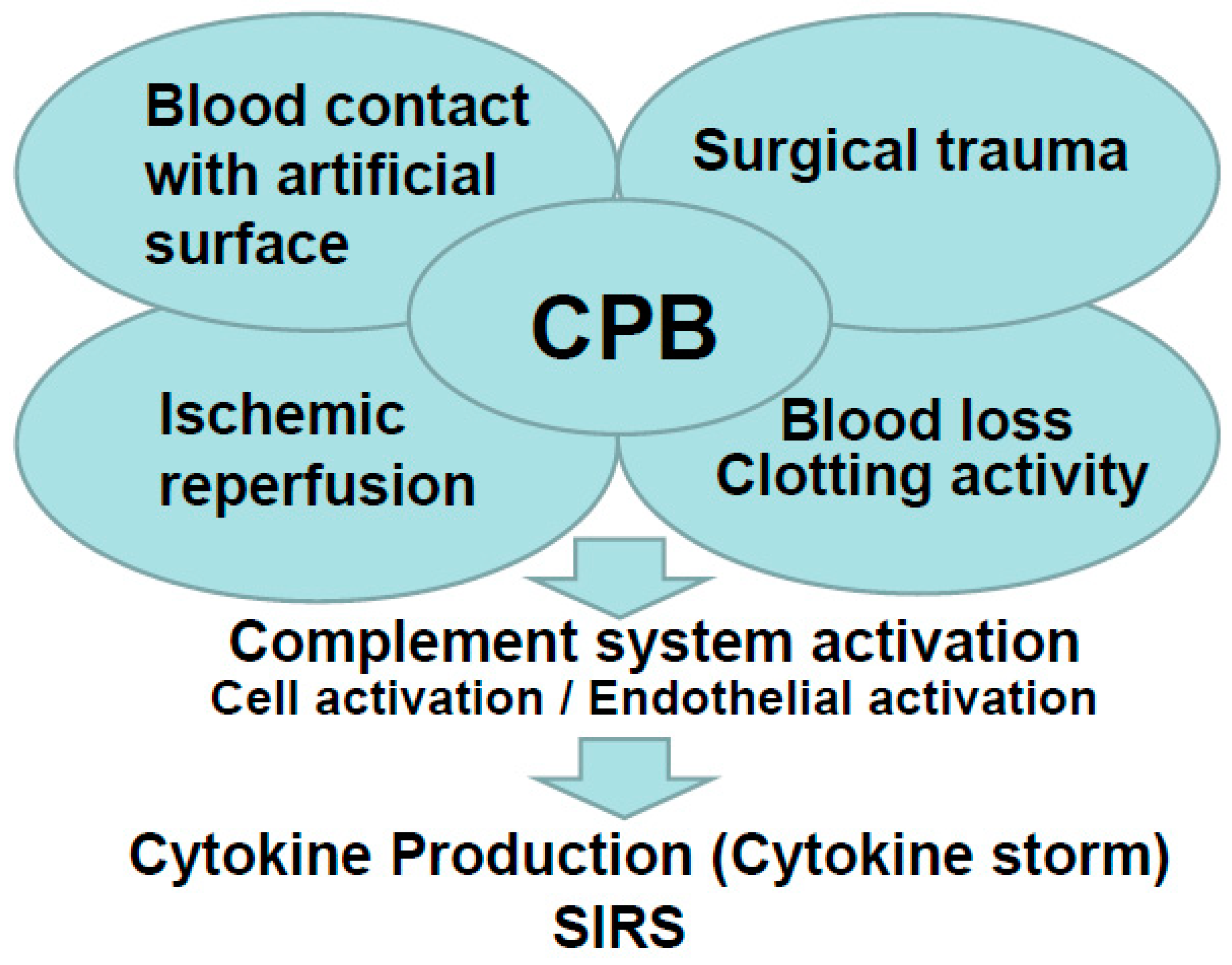
1. Introduction
2. Evaluation of Inflammation Caused by Cardiopulmonary Bypass in a Small Animal Model
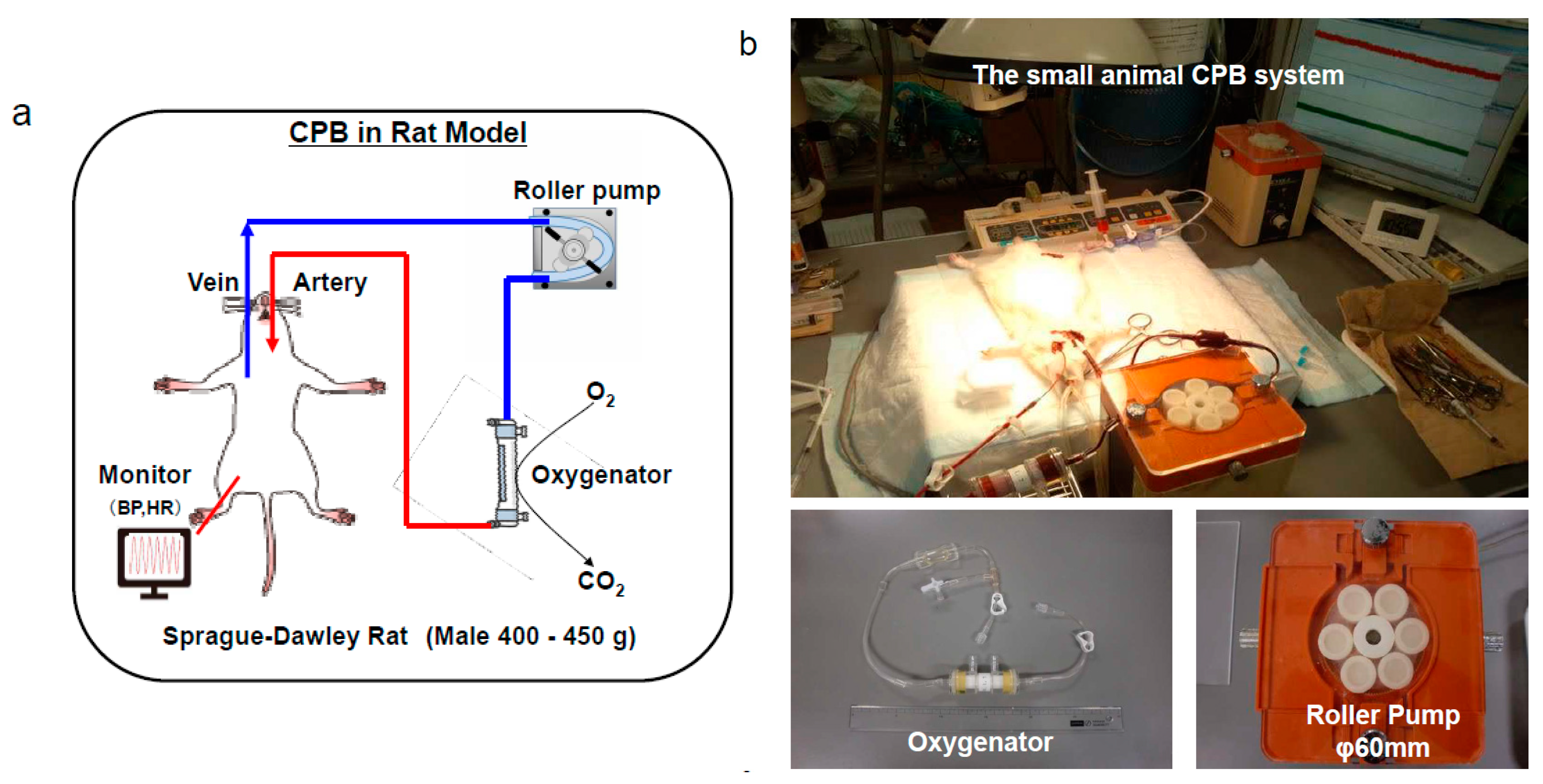
2.1. Our Rat Cardiopulmonary Bypass Model
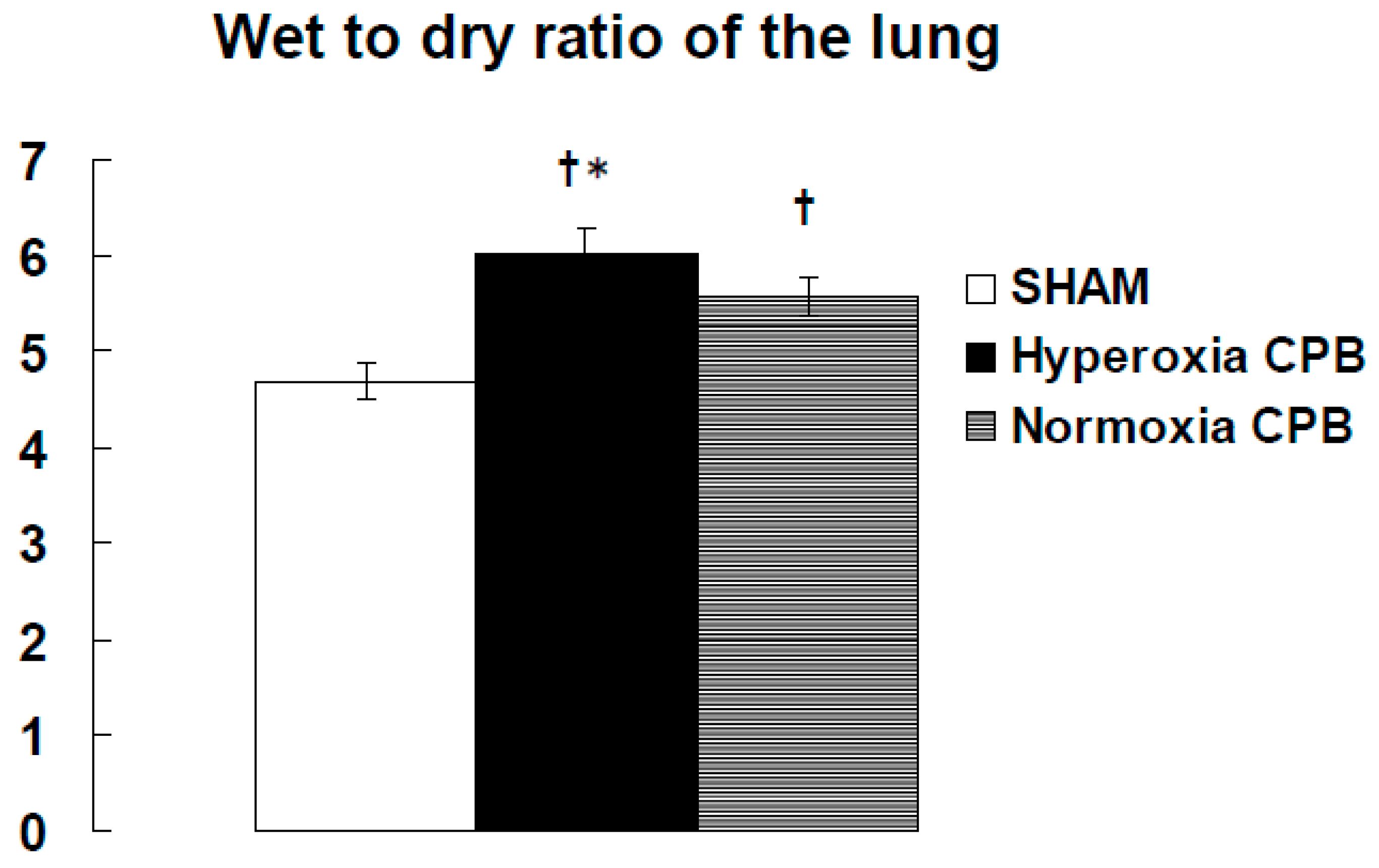
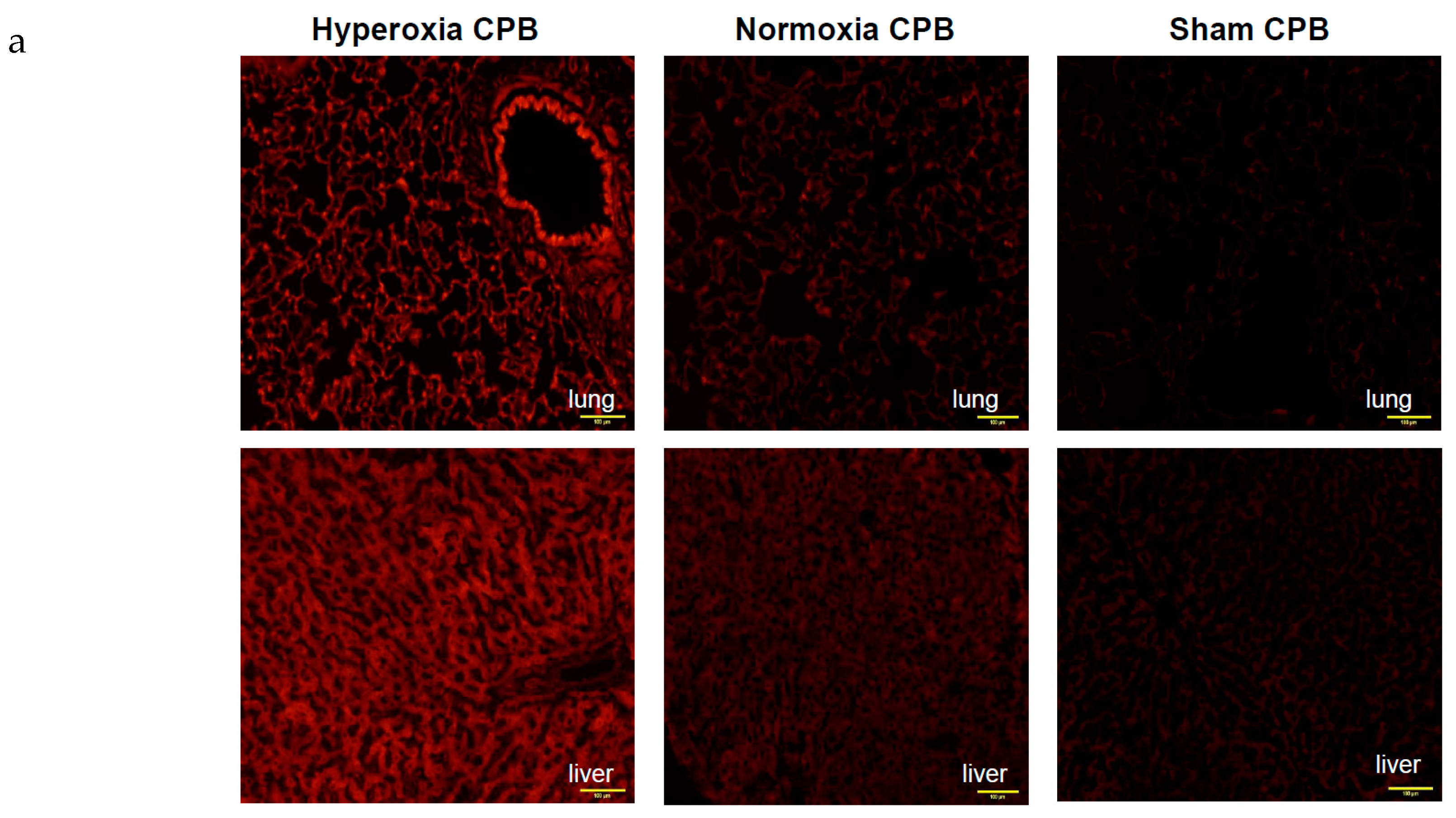
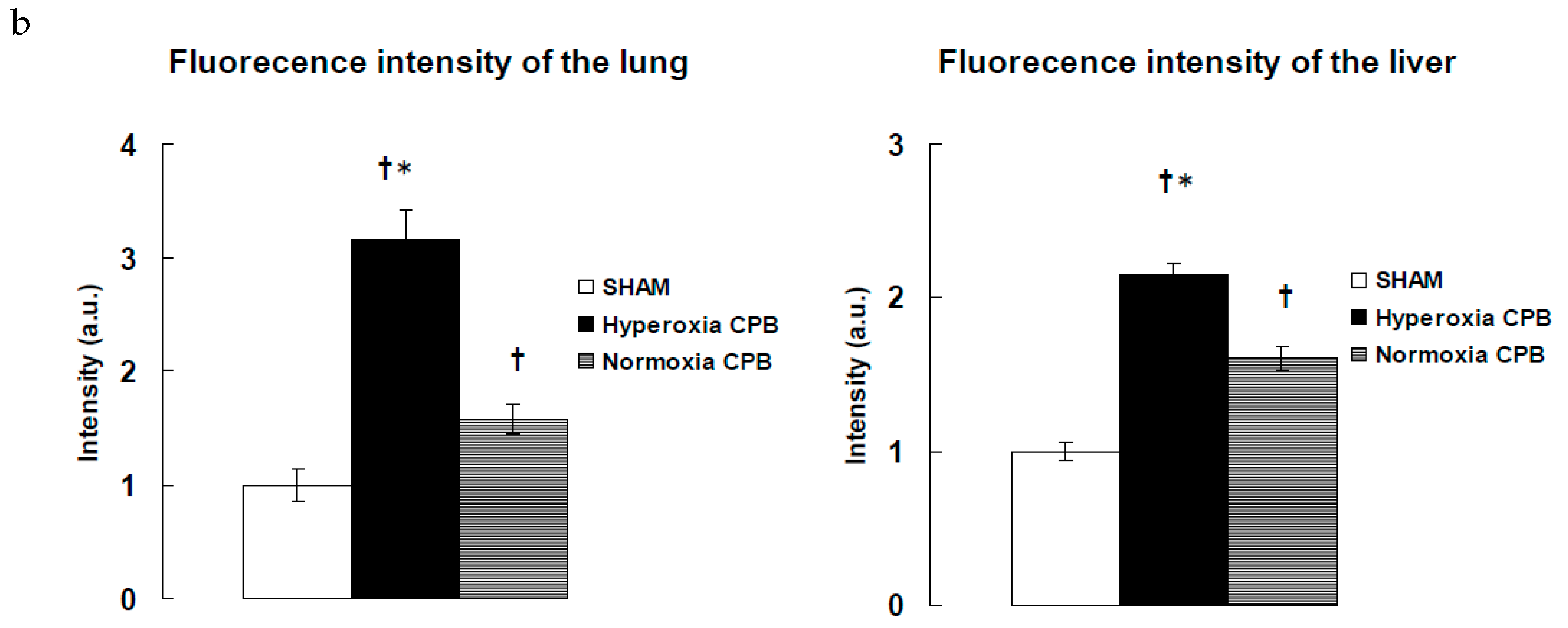
2.2. Hyperoxia Promotes the Inflammatory Response during Cardiopulmonary Bypass
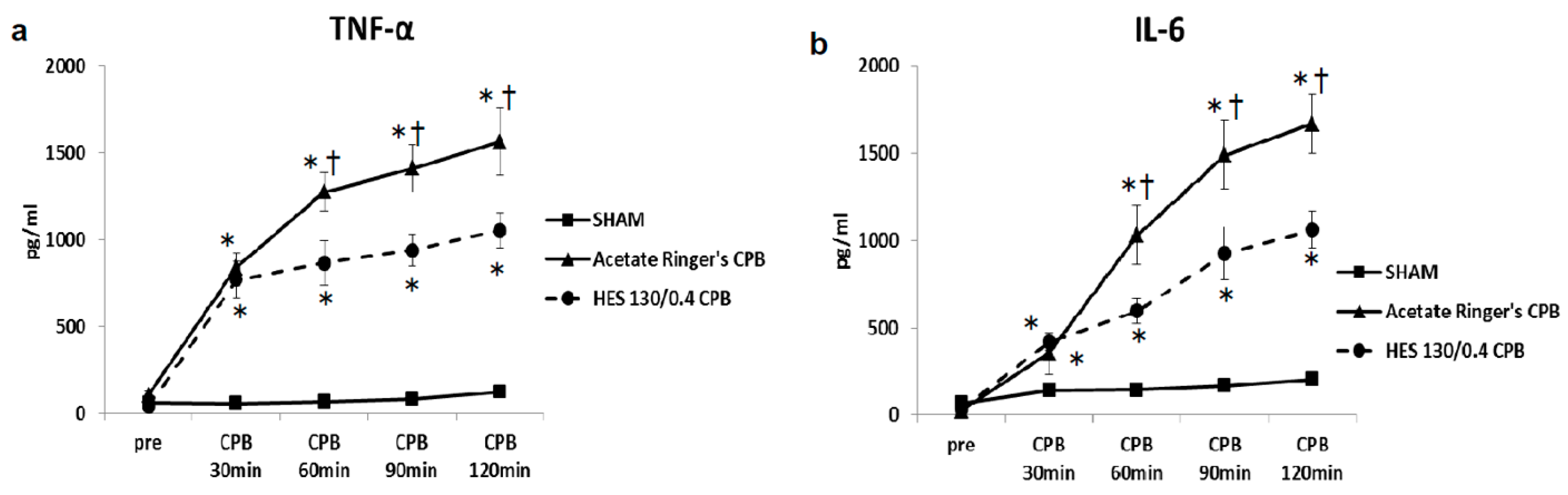
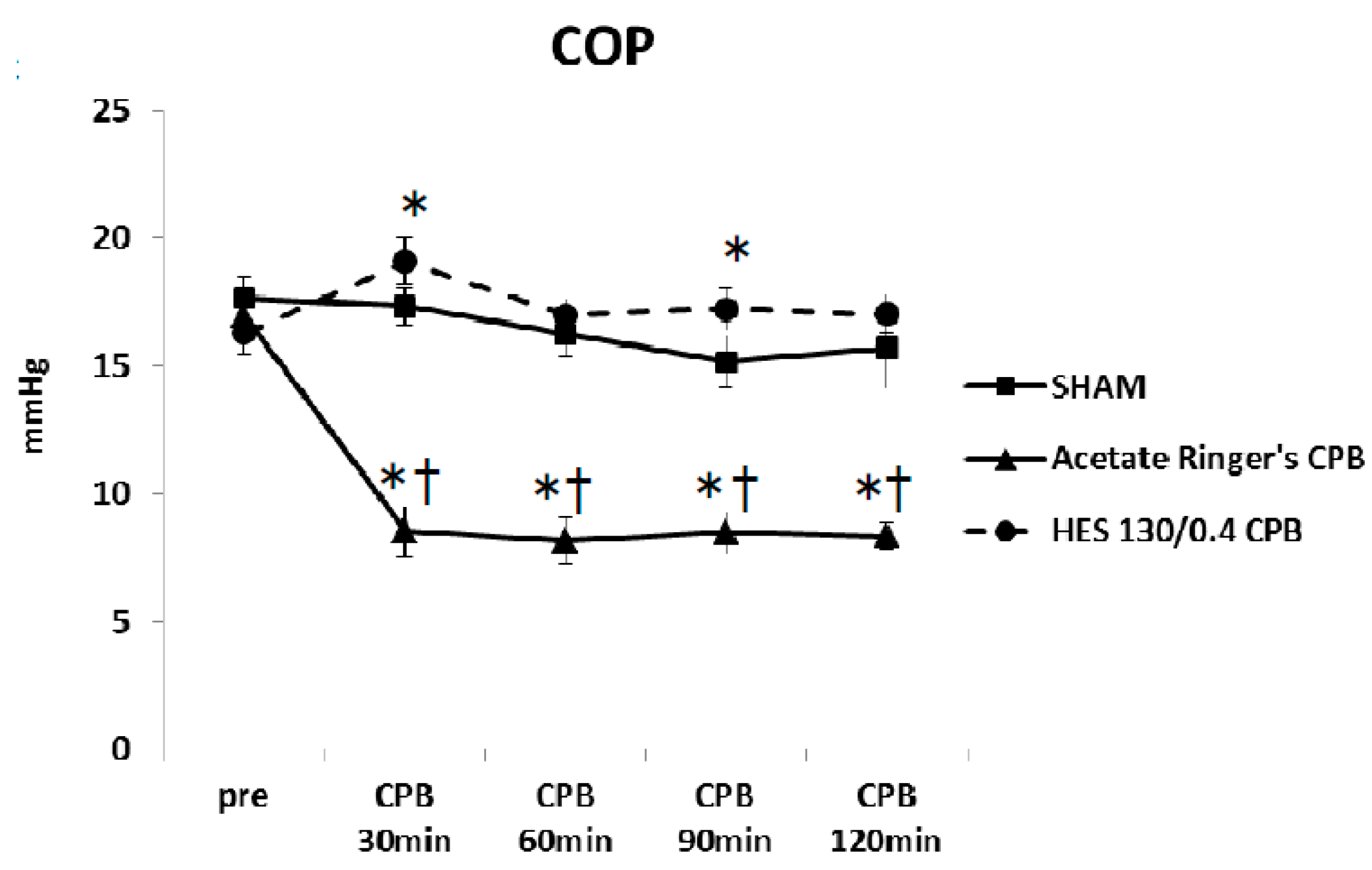
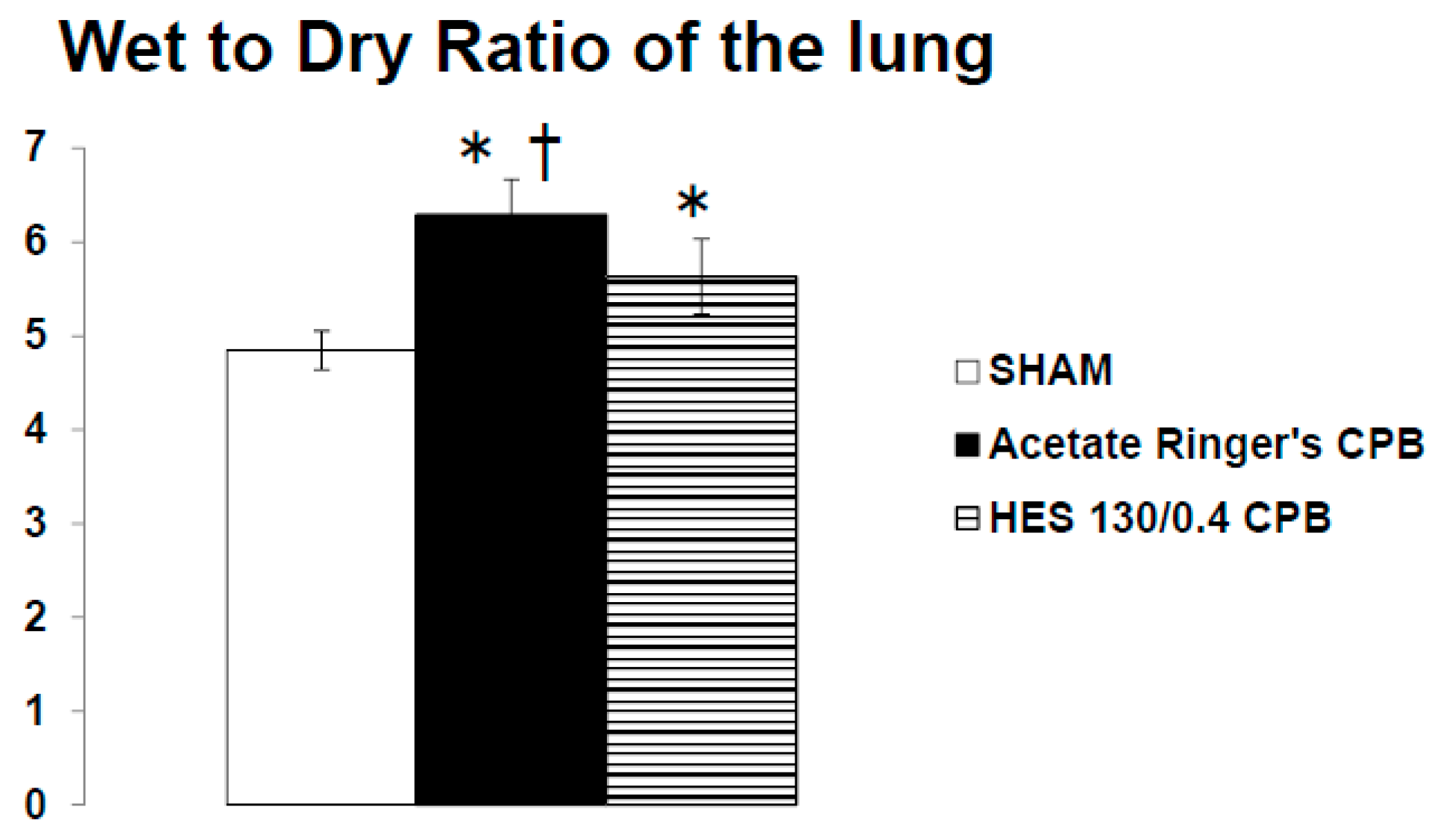
2.3. Effect of Blood Plasma Substitute Priming on the Systemic Inflammation and Lung Edema Following Cardiopulmonary Bypass
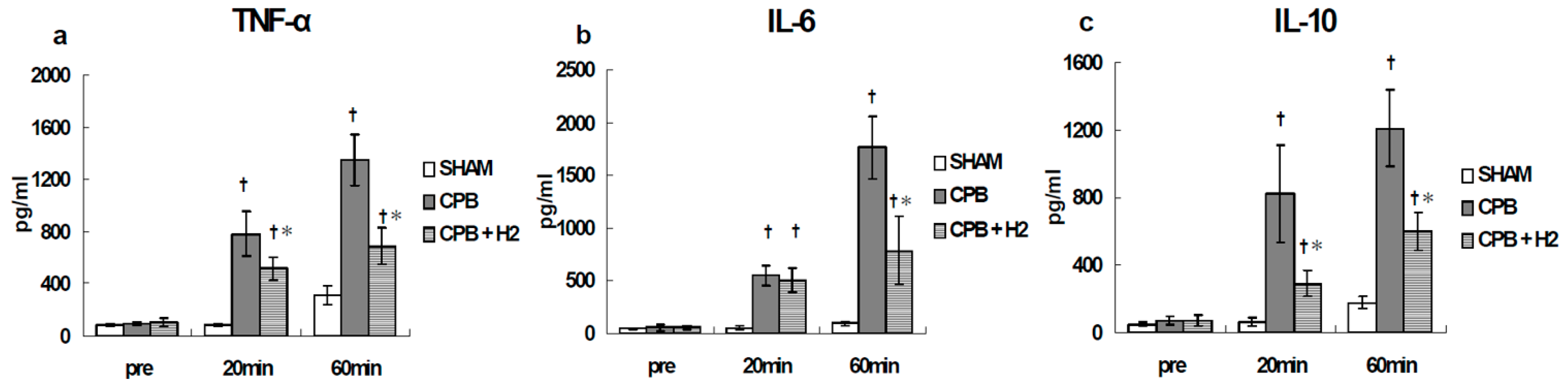
2.4. Method of Suppressing the Inflammatory Response during Extracorporeal Circulation
3. Summary
4. Ethics Approval and Consent to Participate
Availability of Data and Materials
Conflicts of Interest
Abbreviations
| ECC | Extra-corporeal circulation |
| CPB | Cardio-pulmonary bypass |
| W/D | Wet-to-dry |
| DHE | Dihydroethidium |
| ROS | Reactive oxygen species (ROS) |
| PaO2 | Arterial pressure of oxygen |
| PaCO2 | Arterial pressure of carbon dioxide |
| SE | Standard error |
| ANOVA | Analysis of variance |
| PLSD | Protected least significant difference |
| COP | Colloid osmotic pressure |
References
- Evora, P.R.; Bottura, C.; Arcêncio, L.; Albuquerque, A.A.; Évora, P.M.; Rodrigues, A.J. Key Points for Curbing Cardiopulmonary Bypass Inflammation. Acta Cir. Bras. 2016, 31, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Gibbon, J.H., Jr. The application of a mechanical heart and lung apparatus to cardiac surgery. Minn. Med. 1954, 37, 171–185. [Google Scholar] [PubMed]
- Bigelow, W.G. Application of hypothermia to cardiac surgery. Minn. Med. 1954, 37, 181–185. [Google Scholar] [PubMed]
- Kowalik, M.M.; Lango, R.; Siondalski, P.; Chmara, M.; Brzeziński, M.; Lewandowski, K.; Jagielak, D.; Klapkowski, A.; Rogowski, J. Clinical, biochemical and genetic risk factors for 30-day and 5-year mortality in 518 adult patients subjected to cardiopulmonary bypass during cardiac surgery—The INFLACOR study. Acta Biochim. Pol. 2018, 65, 241–250. [Google Scholar] [CrossRef]
- Long, D.M.; Jenkins, E.; Griffith, K. Perfusionist techniques of reducing acute kidney injury following cardiopulmonary bypass: An evidence-based review. Perfusion 2015, 30, 25–32. [Google Scholar] [CrossRef]
- Bronicki, R.A.; Hall, M. Cardiopulmonary Bypass-Induced Inflammatory Response: Pathophysiology and Treatment. Pediatr. Crit. Care Med. 2016, 17 (Suppl. S1), S272–S278. [Google Scholar] [CrossRef]
- Moor, D.; Aggarwal, G.; Quiney, N. Systemic response to surgery. Surgery (Oxf.) 2017, 35, 220–223. [Google Scholar] [CrossRef]
- Baehner, T.; Boehm, O.; Probst, C.; Poetzsch, B.; Hoeft, A.; Baumgarten, G.; Knuefermann, P. Cardiopulmonary bypass in cardiac surgery. Anaesthesist 2012, 61, 846–856. [Google Scholar] [CrossRef]
- Murphy, G.J.; Angelini, G.D. Side effects of cardiopulmonary bypass: What is the reality? J. Card. Surg. 2004, 19, 481–488. [Google Scholar] [CrossRef]
- Ben-Abraham, R.; Weinbroum, A.A.; Dekel, B.; Paret, G. Chemokines and the inflammatory response following cardiopulmonary bypass--a new target for therapeutic intervention? A review. Paediatr. Anaesth. 2003, 13, 655–661. [Google Scholar] [CrossRef]
- Liguori, G.R.; Kanas, A.F.; Moreira, L.F. Managing the inflammatory response after cardiopulmonary bypass: Review of the studies in animal models. Rev. Bras. Cir. Cardiovasc. 2014, 29, 93–102. [Google Scholar] [CrossRef]
- Hirai, S. Systemic inflammatory response syndrome after cardiac surgery under cardiopulmonary bypass. Ann. Thorac. Cardiovasc. Surg. 2003, 9, 365–370. [Google Scholar]
- Jaffer, U.; Wade, R.G.; Gourlay, T. Cytokines in the systemic inflammatory. response syndrome: A review. HSR Proc. Intensive Care Cardiovasc. Anesth. 2010, 2, 161–175. [Google Scholar]
- Chegeni, S.A.; Rahimzadeh, M.; Montazerghaem, H.; Khayatian, M.; Dasturian, F.; Naderi, N. Preliminary Report on the Association Between STAT3 Polymorphisms and Susceptibility to Acute Kidney Injury After Cardiopulmonary Bypass. Biochem. Genet. 2018, 56, 627–638. [Google Scholar] [CrossRef]
- Greenberg, J.H.; Whitlock, R.; Zhang, W.R.; Thiessen-Philbrook, H.R.; Zappitelli, M.; Devarajan, P.; Eikelboom, J.; Kavsak, P.A.; Devereaux, P.J.; Shortt, C.; et al. TRIBE-AKI Consortium. Interleukin-6 and interleukin-10 as acute kidney injury biomarkers in pediatric cardiac surgery. Pediatr. Nephrol. 2015, 30, 1519–1527. [Google Scholar] [CrossRef]
- Träger, K.; Fritzler, D.; Fischer, G.; Schröder, J.; Skrabal, C.; Liebold, A.; Reinelt, H. Treatment of post-cardiopulmonary bypass SIRS by hemoadsorption: A case series. Int. J. Artif. Organs 2016, 39, 141–146. [Google Scholar] [CrossRef]
- Thakar, C.V.; Worley, S.; Arrigain, S.; Yared, J.P.; Paganini, E.P. Influence of renal dysfunction on mortality after cardiac surgery: Modifying effect of preoperative renal function. Kidney Int. 2005, 67, 1112–1119. [Google Scholar] [CrossRef] [PubMed]
- Dasta, J.F.; Kane-Gill, S.L.; Durtschi, A.J.; Pathak, D.S.; Kellum, J.A. Costs and outcomes of acute kidney injury (AKI) following cardiac surgery. Nephrol. Dial. Transplant. 2008, 23, 1970–1974. [Google Scholar] [CrossRef]
- Abdelhadi, R.H.; Gurm, H.S.; Van Wagoner, D.R.; Chung, M.K. Relation of an exaggerated rise in white blood cells after coronary bypass or cardiac valve surgery to development of atrial fibrillation postoperatively. Am. J. Cardiol. 2004, 93, 1176–1178. [Google Scholar] [CrossRef] [PubMed]
- Lamm, G.; Auer, J.; Weber, T.; Berent, R.; Ng, C.; Eber, B. Postoperative white blood cell count predicts atrial fibrillation after cardiac surgery. J. Cardiothorac. Vasc. Anesth. 2006, 20, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Fontes, M.L.; Amar, D.; Kulak, A.; Koval, K.; Zhang, H.; Shi, W.; Thaler, H. Increased preoperative white blood cell count predicts postoperative atrial fibrillation after coronary artery bypass surgery. J. Cardiothorac. Vasc. Anesth. 2009, 23, 484–487. [Google Scholar] [CrossRef]
- Sabol, F.; Jakubová, M.; Mitro, P.; Bomba, A.; Chmelárová, A.; Petrášová, D.; Stančák, B.; Nagy, V.; Török, P.; Sebová, A. Is there a relationship between inflammatory markers, oxidative stress and postoperative atrial fibrillation? Vnitr. Lek. 2012, 58, 730–734. [Google Scholar] [PubMed]
- Fontes, M.L.; Mathew, J.P.; Rinder, H.M.; Zelterman, D.; Smith, B.R.; Rinder, C.S. Multicenter Study of Perioperative Ischemia (McSPI) Research Group. Atrial fibrillation after cardiac surgery/cardiopulmonary bypass is associated with monocyte activation. Anesth. Analg. 2005, 101, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Fujii, Y.; Shirai, M.; Inamori, S.; Shimouchi, A.; Sonobe, T.; Tsuchimochi, H.; Pearson, J.T.; Takewa, Y.; Tatsumi, E.; Taenaka, Y. Insufflation of Hydrogen Gas Restrains the Inflammatory Response of Cardiopulmonary Bypass in a Rat Model. Artif. Organs 2013, 37, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Fujii, Y.; Shirai, M.; Tsuchimochi, H.; Pearson, J.T.; Takewa, Y.; Tatsumi, E.; Taenaka, Y. Hyperoxic condition promotes an inflammatory response during cardiopulmonary bypass in a rat model. Artif. Organs 2013, 37, 1034–1040. [Google Scholar] [CrossRef] [PubMed]
- Fujii, Y.; Shirai, M.; Pearson, J.T.; Takewa, Y.; Tatsumi, E. Changes in inflammatory response during and after cardiopulmonary bypass using a rat extracorporeal circulation model. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2015, 2015, 957–960. [Google Scholar]
- Sukumaran, V.; Tsuchimochi, H.; Fujii, Y.; Hosoda, H.; Kangawa, K.; Akiyama, T.; Shirai, M.; Tatsumi, E.; Pearson, J.T. Ghrelin Pre-treatment Attenuates Local Oxidative Stress and End Organ Damage During Cardiopulmonary Bypass in Anesthetized Rats. Front. Physiol. 2018, 9, 196. [Google Scholar] [CrossRef]
- Fujii, Y.; Shirai, M.; Inamori, S.; Takewa, Y.; Tatsumi, E. A novel small animal extracorporeal circulation model for studying pathophysiology of cardiopulmonary bypass. J. Artif. Organs 2015, 18, 35–39. [Google Scholar] [CrossRef]
- Kilgannon, J.H.; Jones, A.E.; Shapiro, N.I.; Angelos, M.G.; Milcarek, B.; Hunter, K.; Parrillo, J.E.; Trzeciak, S. Investigators. Association between arterial hyperoxia following resuscitation from cardiac arrest and in-hospital mortality. JAMA 2010, 303, 2165–2171. [Google Scholar] [CrossRef]
- Lee, P.J.; Choi, A.M. Pathways of cell signaling in hyperoxia. Free Radic. Biol. Med. 2003, 35, 341–350. [Google Scholar] [CrossRef]
- Morita, K. Surgical reoxygenation injury of the myocardium in cyanotic patients: Clinical relevance and therapeutic strategies by normoxic management during cardiopulmonary bypass. Gen. Thorac. Cardiovasc. Surg. 2012, 60, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Jungheinrich, C.; Scharpf, R.; Wargenau, M.; Bepperling, F.; Baron, J.F. The pharmacokinetics and tolerability of an intravenous infusion of the new hydroxyethyl starch 130/0.4 (6%, 500 mL) in mild-to-severe renal impairment. Anesth. Analg. 2002, 95, 544–551. [Google Scholar] [PubMed]
- Felfernig, M.; Franz, A.; Bräunlich, P.; Fohringer, C.; Kozek-Langenecker, S.A. The effects of hydroxyethyl starch solutions on thromboelastography in preoperative male patients. Acta Anaesthesiol. Scand. 2003, 47, 70–73. [Google Scholar] [CrossRef] [PubMed]
- Lang, K.; Suttner, S.; Boldt, J.; Kumle, B.; Nagel, D. Volume replacement with HES 130/0.4 may reduce the inflammatory response in patients undergoing major abdominal surgery. Can. J. Anaesth. 2003, 50, 1009–1016. [Google Scholar] [CrossRef]
- Fujii, Y.; Tanabe, T.; Yamashiro, T.; Shirai, M.; Takewa, Y.; Tatsumi, E. Effect of Hydroxyethyl Starch Priming on the Systemic Inflammatory Response and Lung Edema after Cardiopulmonary Bypass in a Rat Model. ASAIO J. 2017, 63, 618–623. [Google Scholar] [CrossRef]
- Fujii, Y. The potential of the novel leukocyte removal filter in cardiopulmonary bypass. Expert Rev. Med. Devices 2016, 13, 5–14. [Google Scholar] [CrossRef]
- Salameh, A.; Dhein, S.; Dähnert, I.; Klein, N. Neuroprotective Strategies during Cardiac Surgery with Cardiopulmonary Bypass. Int. J. Mol. Sci. 2016, 17, 1945. [Google Scholar] [CrossRef]
- Fudulu, D.; Angelini, G. Oxidative Stress after Surgery on the Immature Heart. Oxid. Med. Cell. Longev. 2016, 2016, 1971452. [Google Scholar] [CrossRef]
- McDonald, C.I.; Fraser, J.F.; Coombes, J.S.; Fung, Y.L. Oxidative stress during extracorporeal circulation. Eur. J. Cardiothorac. Surg. 2014, 46, 937–943. [Google Scholar] [CrossRef]
- Han, C.H.; Guan, Z.B.; Zhang, P.X.; Fang, H.L.; Li, L.; Zhang, H.M.; Zhou, F.J.; Mao, Y.F.; Liu, W.W. Oxidative stress induced necroptosis activation is involved in the pathogenesis of hyperoxic acute lung injury. Biochem. Biophys. Res. Commun. 2018, 495, 2178–2183. [Google Scholar] [CrossRef]
- Jones, C.I., 3rd; Han, Z.; Presley, T.; Varadharaj, S.; Zweier, J.L.; Ilangovan, G.; Alevriadou, B.R. Endothelial cell respiration is affected by the oxygen tension during shear exposure: Role of mitochondrial peroxynitrite. Am. J. Physiol. Cell Physiol. 2008, 295, 180–191. [Google Scholar] [CrossRef]
- Lang, K.; Boldt, J.; Suttner, S.; Haisch, G. Colloids versus crystalloids and tissue oxygen tension in patients undergoing major abdominal surgery. Anesth. Analg. 2001, 93, 405–409. [Google Scholar]
- Woodcock, T.E.; Woodcock, T.M. Revised Starling equation and the glycocalyx model of transvascular fluid exchange: An improved paradigm for prescribing intravenous fluid therapy. Br. J. Anaesth. 2012, 108, 384–394. [Google Scholar] [CrossRef]
- Aljure, O.D.; Fabbro, M., 2nd. Cardiopulmonary Bypass and Inflammation: The Hidden Enemy. J. Cardiothorac. Vasc. Anesth. 2019, 33, 346–347. [Google Scholar] [CrossRef]
- Lewis, S.R.; Pritchard, M.W.; Evans, D.J.; Butler, A.R.; Alderson, P.; Smith, A.F.; Roberts, I. Colloids versus crystalloids for fluid resuscitation in critically ill people. Cochrane Database Syst Rev. 2018, 8, CD000567. [Google Scholar] [CrossRef]
- Chang, C.; Raza, S.; Altarabsheh, S.E.; Delozier, S.; Sharma, U.M.; Zia, A.; Khan, M.S.; Neudecker, M.; Markowitz, A.H.; Sabik, J.F., 3rd; et al. Minimally Invasive Approaches to Surgical Aortic Valve Replacement: A Meta-Analysis. Ann. Thorac. Surg. 2018, 106, 1881–1889. [Google Scholar] [CrossRef]
- Winkler, B.; Heinisch, P.P.; Gahl, B.; Aghlmandi, S.; Jenni, H.J.; Carrel, T.P. Minimally Invasive Extracorporeal Circulation Circuit Is Not Inferior to Off-Pump Coronary Artery Bypass Grafting: Meta-Analysis Using the Bayesian Method. Ann. Thorac. Surg. 2017, 103, 342–350. [Google Scholar] [CrossRef]
- Jacob, K.A.; Nathoe, H.M.; Dieleman, J.M.; van Osch, D.; Kluin, J.; van Dijk, D. Inflammation in new-onset atrial fibrillation after cardiac surgery: A systematic review. Eur. J. Clin. Investig. 2014, 44, 402–428. [Google Scholar] [CrossRef]
- Scrascia, G.; Rotunno, C.; Guida, P.; Amorese, L.; Polieri, D.; Codazzi, D.; Paparella, D. Perioperative steroids administration in pediatric cardiac surgery: A meta-analysis of randomized controlled trials*. Pediatr. Crit. Care Med. 2014, 15, 435–442. [Google Scholar] [CrossRef]
- Royse, C.F.; Saager, L.; Whitlock, R.; Ou-Young, J.; Royse, A.; Vincent, J.; Devereaux, P.J.; Kurz, A.; Awais, A.; Panjasawatwong, K.; et al. Impact of Methylprednisolone on Postoperative Quality of Recovery and Delirium in the Steroids in Cardiac Surgery Trial: A Randomized, Double-blind, Placebo-controlled Substudy. Anesthesiology 2017, 126, 223–233. [Google Scholar] [CrossRef]
- Pasquali, S.K.; Hall, M.; Li, J.S.; Peterson, E.D.; Jaggers, J.; Lodge, A.J.; Marino, B.S.; Goodman, D.M.; Shah, S.S. Corticosteroids and outcome in children undergoing congenital heart surgery: Analysis of the pediatric health information systems database. Circulation 2010, 122, 2123–2130. [Google Scholar] [CrossRef] [PubMed]
- Whitlock, R.P.; Devereaux, P.J.; Teoh, K.H.; Lamy, A.; Vincent, J.; Pogue, J.; Paparella, D.; Sessler, D.I.; Karthikeyan, G.; Villar, J.C.; et al. SIRS Investigators. Methylprednisolone in patients undergoing cardiopulmonary bypass (SIRS): A randomised, double-blind, placebo-controlled trial. Lancet 2015, 386, 1243–1253. [Google Scholar] [CrossRef]
- Scrascia, G.; Guida, P.; Rotunno, C.; de Luca Tupputi Schinosa, L.; Paparella, D. Anti-inflammatory strategies to reduce acute kidney injury in cardiac surgery patients: A meta-analysis of randomized controlled trials. Artif. Organs 2014, 38, 101–112. [Google Scholar] [CrossRef] [PubMed]
- Onorati, F.; Santini, F.; Mariscalco, G.; Bertolini, P.; Sala, A.; Faggian, G.; Mazzucco, A. Leukocyte filtration ameliorates the inflammatory response in patients with mild to moderate lung dysfunction. Ann. Thorac. Surg. 2011, 92, 111–121. [Google Scholar] [CrossRef]
- Rubino, A.S.; Serraino, G.F.; Mariscalco, G.; Marsico, R.; Sala, A.; Renzulli, A. Leukocyte depletion during extracorporeal circulation allows better organ protection but does not change hospital outcomes. Ann. Thorac. Surg. 2011, 91, 534–540. [Google Scholar] [CrossRef]
- Wagner, R.; Piler, P.; Uchytil, B.; Halouzka, R.; Kovaru, H.; Bobkova, M.; Nemec, P. Systemic inflammatory response syndrome is reduced by preoperative plasma-thrombo-leukocyte aphaeresis in a pig model of cardiopulmonary bypass. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc. Czech Repub. 2016, 160, 399–406. [Google Scholar] [CrossRef]
- Pinto, A.; Jahn, A.; Immohr, M.B.; Jenke, A.; Döhrn, L.; Kornfeld, M.; Lichtenberg, A.; Akhyari, P.; Boeken, U. Modulation of Immunologic Response by Preventive Everolimus Application in a Rat CPB Model. Inflammation 2016, 39, 1771–1782. [Google Scholar] [CrossRef]
- Engels, M.; Bilgic, E.; Pinto, A.; Vasquez, E.; Wollschläger, L.; Steinbrenner, H.; Kellermann, K.; Akhyari, P.; Lichtenberg, A.; Boeken, U. A cardiopulmonary bypass with deep hypothermic circulatory arrest rat model for the investigation of the systemic inflammation response and induced organ damage. J. Inflamm. (Lond.) 2014, 11, 26. [Google Scholar] [CrossRef]
- Wang, Z.; Zhang, A.; Meng, W.; Wang, T.; Li, D.; Liu, Z.; Liu, H. Ozone protects the rat lung from ischemia-reperfusion injury by attenuating NLRP3-mediated inflammation, enhancing Nrf2 antioxidant activity and inhibiting apoptosis. Eur. J. Pharmacol. 2018, 835, 82–93. [Google Scholar] [CrossRef]










© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fujii, Y. Evaluation of Inflammation Caused by Cardiopulmonary Bypass in a Small Animal Model. Biology 2020, 9, 81. https://doi.org/10.3390/biology9040081
Fujii Y. Evaluation of Inflammation Caused by Cardiopulmonary Bypass in a Small Animal Model. Biology. 2020; 9(4):81. https://doi.org/10.3390/biology9040081
Chicago/Turabian StyleFujii, Yutaka. 2020. "Evaluation of Inflammation Caused by Cardiopulmonary Bypass in a Small Animal Model" Biology 9, no. 4: 81. https://doi.org/10.3390/biology9040081
APA StyleFujii, Y. (2020). Evaluation of Inflammation Caused by Cardiopulmonary Bypass in a Small Animal Model. Biology, 9(4), 81. https://doi.org/10.3390/biology9040081