Allergies to Titanium Dental Implants: What Do We Really Know about Them? A Scoping Review

 ,
,  , ,
, , 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
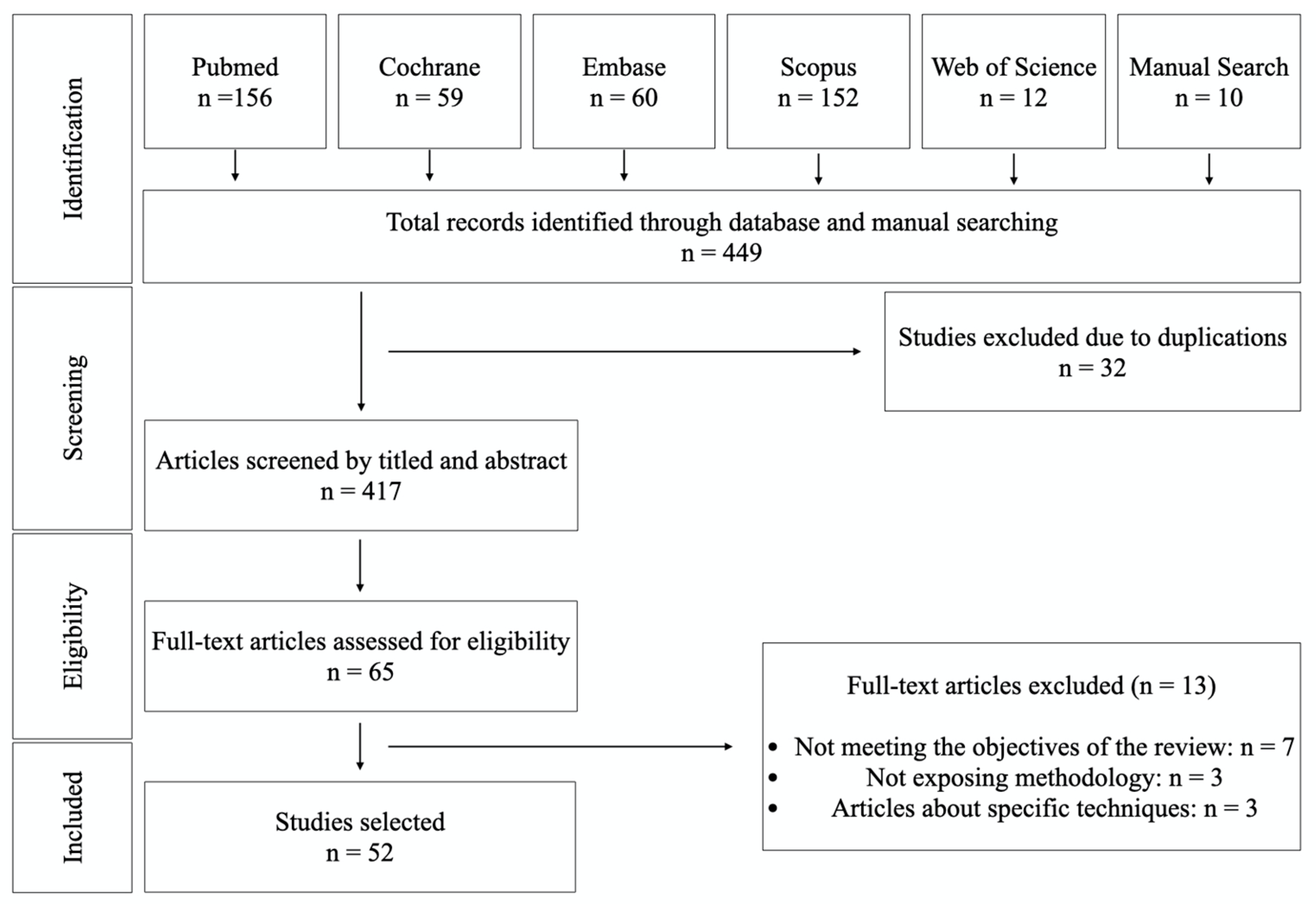
2.1. Search Strategy
2.2. Eligibilty Criteria
2.3. Data Extraction and Collection
3. Results
3.1. Mechanisms that Can Trigger Allergies to Titanium
3.1.1. In Vitro
3.1.2. In Vivo Experiments
- Non-dental implants
- Dental implants
3.2. Clinical Characteristics of Hypersensitivity to Titanium
3.3. Tests for Identifying Metal Allergies
3.4. Cases of Allergies to Titanium Dental Implants
3.5. Titanium Allergy Management
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Siddiqi, A.; Payne, A.G.T.; De Silva, R.K.; Duncan, W. Titanium allergy: Could it affect dental implant integration? Clin. Oral Implant. Res. 2011, 22, 673–680. [Google Scholar] [CrossRef] [PubMed]
- De Graaf, N.P.J.; Feilzer, A.J.; Kleverlaan, C.J.; Bontkes, H.; Gibbs, S.; Rustemeyer, T. A retrospective study on titanium sensitivity: Patch test materials and manifestations. Contact Dermat. 2018, 79, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Wood, M.M.; Warshaw, E.M. Hypersensitivity reactions to titanium: Diagnosis and management. Dermatitis 2015, 26, 7–25. [Google Scholar] [CrossRef] [PubMed]
- Brånemark, I.P.; Hansson, O.B.; Adell, R.; Breine, U.; Lindström, J.; Hallén, O.; Ohman, A. Osseointegrated implants in the treatment of the edentulous jaw. Experience from a 10-year period. Scand. J. Plast. Reconstr. Surg. Suppl. 1977, 16, 1–132. [Google Scholar] [PubMed]
- Cochran, D.L.; Jackson, J.M.; Jones, A.A.; Jones, J.D.; Kaiser, D.A.; Taylor, T.D.; Weber, H.P.; Higginbottom, F.L.; Richardson, J.R.; Oates, T. A 5-Year Prospective Multicenter Clinical Trial of Non-Submerged Dental Implants with a Titanium Plasma-Sprayed Surface in 200 Patients. J. Periodontol. 2011, 82, 990–999. [Google Scholar] [CrossRef]
- Lambrecht, J.; Filippi, A.; Künzel, A.; Schiel, H. Long-term evaluation of submerged and nonsubmerged ITI solid-screw titanium implants: A 10-year life table analysis of 468 implants. J. Prosthet. Dent. 2004, 91, 602. [Google Scholar] [CrossRef]
- Ravald, N.; Dahlgren, S.; Teiwik, A.; Gröndahl, K. Long-term evaluation of Astra Tech and Brånemark implants in patients treated with full-arch bridges. Results after 12–15 years. Clin. Oral Implant. Res. 2013, 24, 1144–1151. [Google Scholar] [CrossRef]
- Thomas, P.; Bandl, W.-D.; Maier, S.; Summer, B.; Przybilla, B. Hypersensitivity to titanium osteosynthesis with impaired fracture healing, eczema, and T-cell hyperresponsiveness in vitro: Case report and review of the literature. Contact Dermat. 2006, 55, 199–202. [Google Scholar] [CrossRef]
- Suito, H.; Iwawaki, Y.; Goto, T.; Tomotake, Y.; Ichikawa, T. Oral Factors Affecting Titanium Elution and Corrosion: An In Vitro Study Using Simulated Body Fluid. PLoS ONE 2013, 8, e66052. [Google Scholar] [CrossRef]
- Olmedo, D.G.; Paparella, M.L.; Spielberg, M.; Brandizzi, D.; Guglielmotti, M.B.; Cabrini, R.L. Oral Mucosa Tissue Response to Titanium Cover Screws. J. Periodontol. 2012, 83, 973–980. [Google Scholar] [CrossRef]
- Sicilia, A.; Cuesta, S.; Coma, G.; Arregui, I.; Guisasola, C.; Ruiz, E.; Maestro, A. Titanium allergy in dental implant patients: A clinical study on 1500 consecutive patients. Clin. Oral Implant. Res. 2008, 19, 823–835. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.S.; Schroeter, A.L.; Van Hale, H.M.; Broadbent, J.C. Pacemaker contact sensitivity. Contact Dermat. 1984, 11, 214–218. [Google Scholar] [CrossRef] [PubMed]
- Lalor, P.A.; Revell, P.A.; Gray, A.B.; Wright, S.; Railton, G.T.; Freeman, M.A. Sensitivity to titanium. A cause of implant failure? J. Bone Joint. Surg. Br. 1991, 73, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Egusa, H.; Ko, N.; Shimazu, T.; Yatani, H. Suspected association of an allergic reaction with titanium dental implants: A clinical report. J. Prosthet. Dent. 2008, 100, 344–347. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Hosoki, M.; Nishigawa, K.; Miyamoto, Y.; Ohe, G.; Matsuka, Y. Allergic contact dermatitis caused by titanium screws and dental implants. J. Prosthodont. Res. 2016, 60, 213–219. [Google Scholar] [CrossRef]
- Preez, A.D.L.; Bütow, K.W.; Swart, T.J.P. Implant failure due to titanium hypersensitivity/allergy?—Report of a case. SADJ J. South Afr. Dent. Assoc. Tydskr. Die Suid-Afrik. Tandheelkd. Ver. 2007, 62, 24–25. [Google Scholar]
- Hosoki, M.; Nishigawa, K.; Tajima, T.; Ueda, M.; Matsuka, Y. Cross-sectional observational study exploring clinical risk of titanium allergy caused by dental implants. J. Prosthodont. Res. 2018, 62, 426–431. [Google Scholar] [CrossRef]
- Müller, K.; Valentine-Thon, E. Hypersensitivity to titanium: Clinical and laboratory evidence. Neuro Endocrinol. Lett. 2006, 27, 31–35. [Google Scholar]
- Mitchell, D.L.; Synnott, A.S.; VanDercreek, A.J. Tissue reaction involving an intraoral skin graft and CP titanium abutments: A clinical report. Int. J. Oral Maxillofac. Implant. 1990, 5, 79–84. [Google Scholar]
- Chaturvedi, T. Allergy related to dental implant and its clinical significance. Clin. Cosmet. Investig. Dent. 2013, 5, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Haug, R.H. Retention of asymptomatic bone plates used for orthognathic surgery and facial fractures. J. Oral Maxillofac. Surg. 1996, 54, 611–617. [Google Scholar] [CrossRef]
- Kasemo, B.; Lausmaa, J. Biomaterial and implant surfaces: A surface science approach. Int. J. Oral Maxillofac. Implant. 1988, 3, 45–68. [Google Scholar]
- Frangini, S.; Piconi, C. Repassivation rates of surgical implant alloys by rotating-disk scratching measurements. Mater. Corros. 2001, 52, 372–380. [Google Scholar] [CrossRef]
- Schutz, R.W. Utilizing titanium to successfully handle chloride process environments. CIM Bull. 2002, 95, 84–88. [Google Scholar]
- Lei, L.; Xiuli, H.; Mingduo, L.; Di, Z. Corrosion of titanium: Part 1: Aggressive environments and main forms of degradation. J. Appl. Biomater. Funct. Mater. 2017, 15, e291–e302. [Google Scholar] [CrossRef]
- Vijayaraghavan, V.; Sabane, A.; Tejas, K. Hypersensitivity to Titanium: A Less Explored Area of Research. J. Indian Prosthodont. Soc. 2012, 12, 201–207. [Google Scholar] [CrossRef]
- Chaturvedi, T.P. An overview of the corrosion aspect of dental implants (titanium and its alloys). Indian J. Dent. Res. 2009, 20, 91–98. [Google Scholar] [CrossRef]
- Delgado-Ruiz, R.A.; Romanos, G.E. Potential Causes of Titanium Particle and Ion Release in Implant Dentistry: A Systematic Review. Int. J. Mol. Sci. 2018, 19, 3585. [Google Scholar] [CrossRef]
- Parr, G.R.; Gardner, L.; Toth, R.W. Titanium: The mystery metal of implant dentistry. Dental materials aspects. J. Prosthet. Dent. 1985, 54, 410–414. [Google Scholar] [CrossRef]
- Olmedo, D.G.; Tasat, D.R.; Guglielmotti, M.B.; Cabrini, R.L. Biodistribution of titanium dioxide from biologic compartments. J. Mater. Sci. Mater. Electron. 2008, 19, 3049–3056. [Google Scholar] [CrossRef] [PubMed]
- Olmedo, D.G.; Tasat, D.R.; Evelson, P.; Rebagliatti, R.; Guglielmotti, M.B.; Cabrini, R.L. In vivo comparative biokinetics and biocompatibility of titanium and zirconium microparticles. J. Biomed. Mater. Res. Part A 2011, 98, 604–613. [Google Scholar] [CrossRef] [PubMed]
- Frisken, K.W.; Dandie, G.W.; Lugowski, S.; Jordan, G.J. A study of titanium release into body organs following the insertion of single threaded screw implants into the mandibles of sheep. Aust. Dent. J. 2002, 47, 214–217. [Google Scholar] [CrossRef] [PubMed]
- Del Amo, F.S.-L.; Garaicoa-Pazmiño, C.; Fretwurst, T.; Castilho, R.M.; Squarize, C.H. Dental implants-associated release of titanium particles: A systematic review. Clin. Oral Implant. Res. 2018, 29, 1085–1100. [Google Scholar] [CrossRef] [PubMed]
- Mombelli, A.; Hashim, D.; Cionca, N. What is the impact of titanium particles and biocorrosion on implant survival and complications? A critical review. Clin. Oral Implant. Res. 2018, 29, 37–53. [Google Scholar] [CrossRef]
- Schliephake, H.; Sicilia, A.; Al-Nawas, B.; Donos, N.; Gruber, R.; Jepsen, S.; Milinkovic, I.; Mombelli, A.; Navarro, J.M.; Quirynen, M.; et al. Drugs and diseases: Summary and consensus statements of group 1. The 5th EAO Consensus Conference 2018. Clin. Oral Implant. Res. 2018, 29, 93–99. [Google Scholar] [CrossRef]
- Holgers, K.M.; Roupe, G.; Tjellstroöm, A.; Bjursten, L.M. Clinical, immunological and bacteriological evaluation of adverse reactions to skin-penetrating titanium implants in the head and neck region. Contact Dermat. 1992, 27, 1–7. [Google Scholar] [CrossRef]
- Mine, Y.; Makihira, S.; Nikawa, H.; Murata, H.; Hosokawa, R.; Hiyama, A.; Mimura, S. Impact of titanium ions on osteoblast-, osteoclast- and gingival epithelial-like cells. J. Prosthodont. Res. 2010, 54, 1–6. [Google Scholar] [CrossRef]
- Albrektsson, T.; Chrcanovic, B.; Mölne, J.; Wennerberg, A. Foreign body reactions, marginal bone loss and allergies in relation to titanium implants. Eur. J. Oral Implant. 2018, 11, S37–S46. [Google Scholar]
- Harloff, T.; Hönle, W.; Holzwarth, U.; Schuh, A.; Bader, R.; Thomas, P. Titanium allergy or not? “Impurity” of titanium implant materials. Health 2010, 2, 306–310. [Google Scholar] [CrossRef]
- Forte, G.; Petrucci, F.; Bocca, B. Metal allergens of growing significance: Epidemiology, immunotoxicology, strategies for testing and prevention. Inflamm. Allergy Drug Targets 2008, 7, 145–162. [Google Scholar] [CrossRef] [PubMed]
- Schuh, M.A.; Thomas, P.; Kachler, W.; Göske, J.; Wagner, L.; Holzwarth, U.; Forst, R. Das Allergiepotenzial von Implantatwerkstoffen auf Titanbasis. Orthopäde 2005, 34, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Fage, S.W.; Muris, J.; Jakobsen, S.S.; Thyssen, J.P. Titanium: A review on exposure, release, penetration, allergy, epidemiology, and clinical reactivity. Contact Dermat. 2016, 74, 323–345. [Google Scholar] [CrossRef] [PubMed]
- Strupp, C. Beryllium Metal II. A Review of the Available Toxicity Data. Ann. Occup. Hyg. 2010, 55, 43–56. [Google Scholar] [CrossRef] [PubMed]
- Javed, F.; Al-Hezaimi, K.; Almas, K.; Romanos, G.E. Is Titanium Sensitivity Associated with Allergic Reactions in Patients with Dental Implants? A Systematic Review. Clin. Implant. Dent. Relat. Res. 2011, 15, 47–52. [Google Scholar] [CrossRef]
- Olmedo, D.G.; Paparella, M.; Brandizzi, D.; Cabrini, R. Reactive lesions of peri-implant mucosa associated with titanium dental implants: A report of 2 cases. Int. J. Oral Maxillofac. Surg. 2010, 39, 503–507. [Google Scholar] [CrossRef]
- Kim, K.T.; Eo, M.Y.; Nguyen, T.T.H.; Kim, S.M. General review of titanium toxicity. Int. J. Implant. Dent. 2019, 5, 1–12. [Google Scholar] [CrossRef]
- Kitagawa, M.; Murakami, S.; Akashi, Y.; Oka, H.; Shintani, T.; Ogawa, I.; Inoue, T.; Kurihara, H. Current status of dental metal allergy in Japan. J. Prosthodont. Res. 2019, 63, 309–312. [Google Scholar] [CrossRef]
- Fregert, S. Manual of Contact Dermatitis. On behalf of the International Contact Dermatitis Research Group and the North American Contact Dermatitis Group, 2nd ed.; Munksgaard Publishers: Copenhagen, Denmark, 1981. [Google Scholar]
- Ownby, D.R. Skin Tests in Comparison to Other Diagnostic Methods. Immunol. Allergy Clin. N. Am. 2001, 21, 355–367. [Google Scholar] [CrossRef]
- Valentine-Thon, E.; Müller, K.; Guzzi, G.; Kreisel, S.; Ohnsorge, P.; Sandkamp, M. LTT-MELISA is clinically relevant for detecting and monitoring metal sensitivity. Neuro Endocrinol. Lett. 2006, 27, 17–24. [Google Scholar]
- Koene, R.A.P. The ’memory lymphocyte immunostimulation assay’ (MELISA) is useless for the detection of metal allergy. Ned. Tijdschr Geneeskd 2005, 149, 2090–2092. [Google Scholar] [PubMed]
- Cederbrant, K.; Hultman, P.; Marcusson, J.A.; Tibbling, L. In vitro Lymphocyte Proliferation as Compared to Patch Test Using Gold, Palladium and Nickel. Int. Arch. Allergy Immunol. 1997, 112, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Cederbrant, K.; Gunnarsson, L.-G.; Hultman, P.; Norda, R.; Tibbling-Grahn, L. In vitro lymphoproliferative assays with HgCl2 cannot identify patients with systemic symptoms attributed to dental amalgam. J. Dent. Res. 1999, 78, 1450–1458. [Google Scholar] [CrossRef] [PubMed]
- Zinelis, S.; Thomas, A.G.; Syres, K.; Silikas, N.; Eliades, G. Surface characterization of zirconia dental implants. Dent. Mater. 2010, 26, 295–305. [Google Scholar] [CrossRef] [PubMed]
- Aita, H.; Hori, N.; Takeuchi, M.; Suzuki, T.; Yamada, M.; Anpo, M.; Ogawa, T. The effect of ultraviolet functionalization of titanium on integration with bone. Biomaterials 2009, 30, 1015–1025. [Google Scholar] [CrossRef]
- Massaro, C.; Rotolo, P.; De Riccardis, F.; Milella, E.; Napoli, A.; Wieland, M.; Textor, M.; Spencer, N.D.; Brunette, D.M. Comparative investigation of the surface properties of commercial titanium dental implants. Part I: Chemical composition. J. Mater. Sci. Mater. Med. 2002, 13, 535–548. [Google Scholar] [CrossRef]
- Messer, W. Dental materials: Biocompatibility; Buschow, K.H.J., Ed.; Encyclopedia of Materials: Science and Technology; Elsevier: Amsterdam, The Netherlands, 2002; pp. 1–10. [Google Scholar]
- Syed, M. Allergic Reactions to Dental Materials—A Systematic Review. J. Clin. Diagn. Res. 2015, 9, ZE04–ZE09. [Google Scholar] [CrossRef]
- Pieralli, S.; Kohal, R.; Jung, R.; Vach, K.; Spies, B. Clinical Outcomes of Zirconia Dental Implants: A Systematic Review. J. Dent. Res. 2016, 96, 38–46. [Google Scholar] [CrossRef]
- Oliva, X.; Oliva, J.D. Full-mouth oral rehabilitation in a titanium allergy patient using zirconium oxide dental implants and zirconium oxide restorations. A case report from an ongoing clinical study. Eur. J. Esthet. Dent. Off. J. Eur. Acad. Esthet. Dent. 2010, 5, 190–203. [Google Scholar]
- Lohmann, C.H.; Hameister, R.; Singh, G. Allergies in orthopaedic and trauma surgery. Orthop. Traumatol. Surg. Res. 2017, 103, S75–S81. [Google Scholar] [CrossRef]
- Cionca, N.; Hashim, D.; Mombelli, A. Zirconia dental implants: Where are we now, and where are we heading? Periodontology 2000 2017, 73, 241–258. [Google Scholar] [CrossRef] [PubMed]
- Sivaraman, K.; Chopra, A.; Narayan, A.I.; Balakrishnan, D. Is zirconia a viable alternative to titanium for oral implant? A critical review. J. Prosthodont. Res. 2018, 62, 121–133. [Google Scholar] [CrossRef] [PubMed]
- Catauro, M.; Barrino, F.; Dal Poggetto, G.; Milazzo, M.; Blanco, I.; Vecchio, C.S. Structure, drug absorption, bioactive and antibacterial properties of sol-gel SiO2/ZrO2 materials. Ceram. Int. 2020, 46, 29459–29465. [Google Scholar] [CrossRef]
- He, X.; Reichl, F.-X.; Milz, S.; Michalke, B.; Wu, X.; Sprecher, C.M.; Yang, Y.; Gahlert, M.; Röhling, S.; Kniha, H.; et al. Titanium and zirconium release from titanium- and zirconia implants in mini pig maxillae and their toxicity in vitro. Dent. Mater. 2020, 36, 402–412. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors and Year | Study | Number of Patients (Mean Age/Range in Years) | Gender | Number of Implants | Subjects with Ti Allergy Compared with the Overall Sample | Time Lag between Placement of Implants and Subsequent Explantation | Clinical Signs of Associated Allergy | Conclusions |
|---|---|---|---|---|---|---|---|---|
| Sicilia et al. 2008 [11] | Clinical/Retrospective | 35 (50.2/21–68) | 10 M 25 F | NA | 9/1500 | NA | Rash, urticaria, pruritus, redness, dermatitis and facial eczema | Titanium allergy can be detected in dental implant patients |
| Egusa et al. 2008 [14] | Case-Report | 1 (50-year-old) | F | 2 | 2 years | Facial eczema | Allergic reactions can be detected in patients with Ti dental implants. | |
| Hosoki et al. 2016 [16] | Case-Report | 1 (69-year-old) | F | 2 | 6 years | Nummular eczema | Pre-implant patients should be asked about a history of hypersensitivity reactions to metals and patch testing should be recommended. | |
| du Preez et al. 2007 [17] | Case-Report | 1 (49-year-old) | F | 6 | 1 week | Pain, hyperaemia of soft tissues, swelling in submental and labial sulcus | A chronic inflammatory response with fibrosis was observed around all Ti implants, which could indicate a real allergy to titanium dental implants | |
| Hosoki et al. 2018 [18] | Clinical Retrospective | 270 (53, 9/7–85) 16 with titanium dental implants | 7 M, 9 F | NA | 4/16 | NA | Soreness, rash, itching, urticaria, discomfort, stomatitis, lichen planus, pustulosis palmaris et plantaris, crazing of a nail | Titanium allergy in patients caused by dental implants exists |
| Müller et al. 2006 [19] | Clinical and Experimental | 56 (53.8/14.3–84.1) | 17 M 39 F | NA | 21/56 | 6 months | Dermatitis and acne-like facial inflammation | Ti can induce clinically relevant hypersensitivity and other immune dysfunctions in certain patients chronically exposed to this reactive metal. |
| Mitchell et al. 1990 [20] | Case-report | 1 (49-year-old) | F | 4 | 1 | 2 weeks | Gingival hyperplasia | Hyperplasia in the gingival tissues may occur in patients with Ti dental implants. |
| 1 (44-year-old) | M | 4 | 1 | 3,5 months | Gingival hyperplasia |
| Article | Animal and Number | Administration | Conclusions |
|---|---|---|---|
| Olmedo et al. 2008 [31] | Rats (n = 20) | Titanium dioxide (TiO2) preparation injection | Internal exposure will lead to a concentration of titanium ions in the surrounding tissues, lymph nodes, and even in lung or liver tissue |
| Olmedo et al. 2011 [32] | Rats (n = 62) | Titanium dioxide (TiO2) preparation injection | Biokinetics will be influenced by the biomechanical properties of titanium particles |
| Frisken KW et al. 2002 [33] | Sheep (n = 12) | Titanium Dental Implants | The presence of titanium found in the lungs in cases of failed implants was 2.2–3.8 times higher than when implants were successful, while in local lymph nodes, it was 7.0–9.4 times higher. Ambiguous results were found in the liver and spleen. |
| Localization | Symptoms |
|---|---|
| Local Manifestations | Hives, edema, eczema, reddening, and itching of the skin or mucosa, erythema, contact dermatosis, atopic eczema, bullous eruptions, proliferative hyperplasia tissue/edematous tissue /non-keratinized tissue, peripheral giant cell pyogenic granuloma |
| Manifestations at a distance from the implant place | Hives, disseminated facial eczema, edema, reddening, and itching of the skin or mucosa, atopic dermatitis |
| Systemic reactions | Pain, necrosis, weakening of orthopedic implants, disturbed fracture healing, nervous disorders, chronic fatigue syndrome, neurological problems, depression, multiple chemical sensitivity |
| Test | In vivo/In vitro | Application Site | Evaluation Time | Positive Signs | Comments |
|---|---|---|---|---|---|
| Epicutaneous Patch Test [2,3,11,16,18,19,21,27,48,49,50,51,53,54] | In vivo | Titanium dioxide (TiO2) preparation patch on back or forearm | 3–7-day period | -Negative reaction -Doubtful reaction (erythema only, no infiltration) -Weak positive reaction (erythema, infiltration, possibly discrete papules) -Strong positive reaction (erythema, infiltration, vesicles, papules) -Extreme positive reaction (erythema, infiltration, confluent vesicles) -Irritant reaction | -One of the most common and important tests for metal allergy (Gold Standard). -The test is not very sensitive, may give a false positive or negative, only detects 75% of Type IV metal allergies. -Lack of standardization may limit their use |
| Cutaneous Injection Test [11,21,27,49] | In vivo | Titanium dioxide (TiO2) preparation injection in forearm | 15–30 min | Red, papular, and/or vesicular reaction of the skin is considered as positive | -Only recommended for Type I allergies and not for oral allergies |
| Lymphocyte Transformation Test (LTT) [3,14,21,27,53,54] | In vitro | In vitro, heparinized venous blood | 5 days | Stimulation index ≥2.0 | -Analyzes local and systemic effects |
| Memory Lymphocyte Immuno-Stimulation Assay (MELISA) [3,19,21,27,51,52,53,54] | In vitro | In vitro, defibrinated blood | 5 days | Stimulation index ≥3.0 together with the presence of lymphoblasts | -Analyzes local and systemic effects |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Comino-Garayoa, R.; Cortés-Bretón Brinkmann, J.; Peláez, J.; López-Suárez, C.; Martínez-González, J.M.; Suárez, M.J. Allergies to Titanium Dental Implants: What Do We Really Know about Them? A Scoping Review. Biology 2020, 9, 404. https://doi.org/10.3390/biology9110404
Comino-Garayoa R, Cortés-Bretón Brinkmann J, Peláez J, López-Suárez C, Martínez-González JM, Suárez MJ. Allergies to Titanium Dental Implants: What Do We Really Know about Them? A Scoping Review. Biology. 2020; 9(11):404. https://doi.org/10.3390/biology9110404
Chicago/Turabian StyleComino-Garayoa, Rubén, Jorge Cortés-Bretón Brinkmann, Jesús Peláez, Carlos López-Suárez, Jose María Martínez-González, and María Jesús Suárez. 2020. "Allergies to Titanium Dental Implants: What Do We Really Know about Them? A Scoping Review" Biology 9, no. 11: 404. https://doi.org/10.3390/biology9110404
APA StyleComino-Garayoa, R., Cortés-Bretón Brinkmann, J., Peláez, J., López-Suárez, C., Martínez-González, J. M., & Suárez, M. J. (2020). Allergies to Titanium Dental Implants: What Do We Really Know about Them? A Scoping Review. Biology, 9(11), 404. https://doi.org/10.3390/biology9110404