Acute Physiological Responses to High-Intensity Resistance Circuit Training vs. Traditional Strength Training in Soccer Players


 , ,
, ,  ,
,  and
and 
Simple Summary
Abstract
1. Introduction
2. Method
2.1. Participants
2.2. Experimental Design
2.3. Procedures
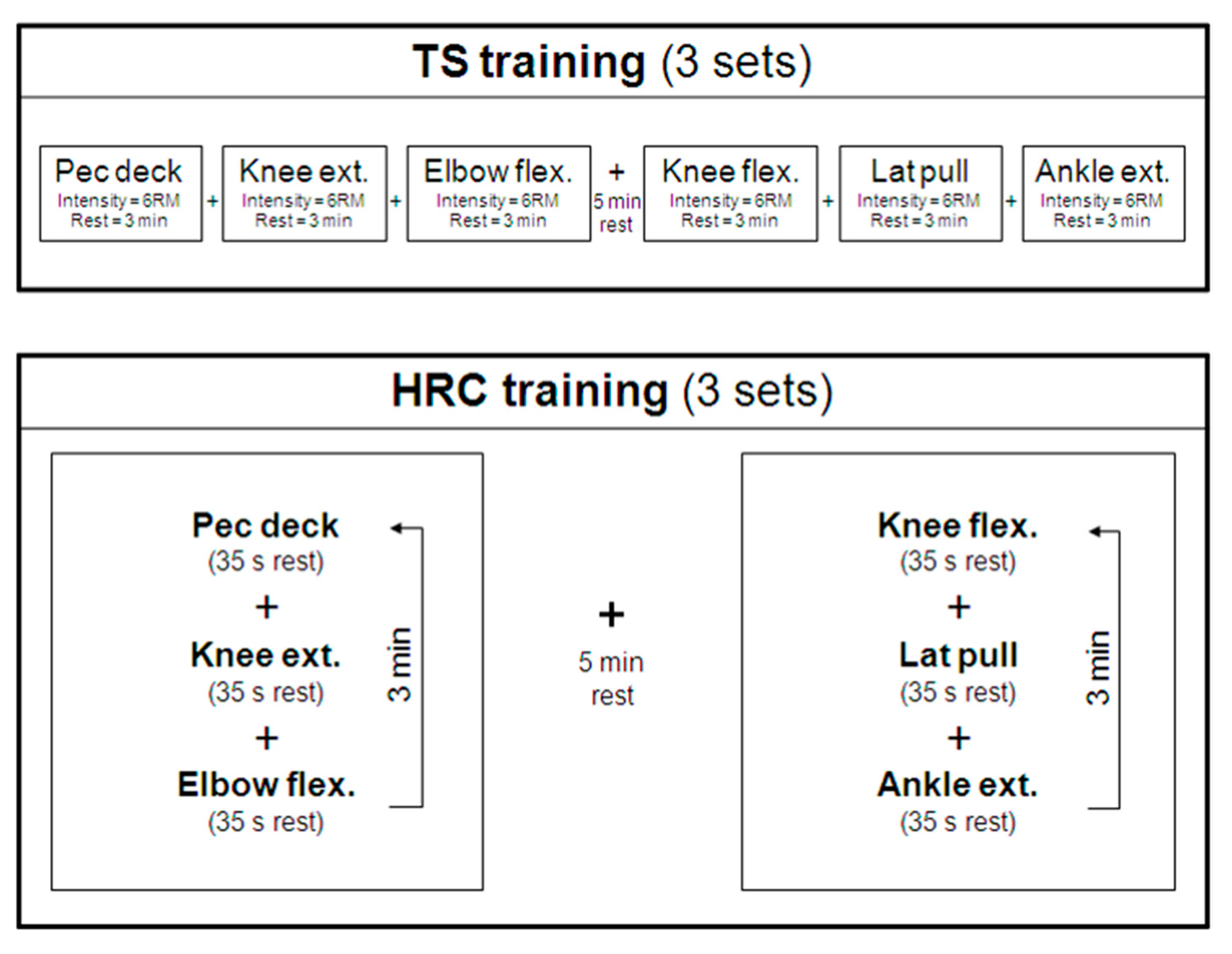
2.4. Resistance Training Sessions
2.5. Statistical Analysis
3. Results
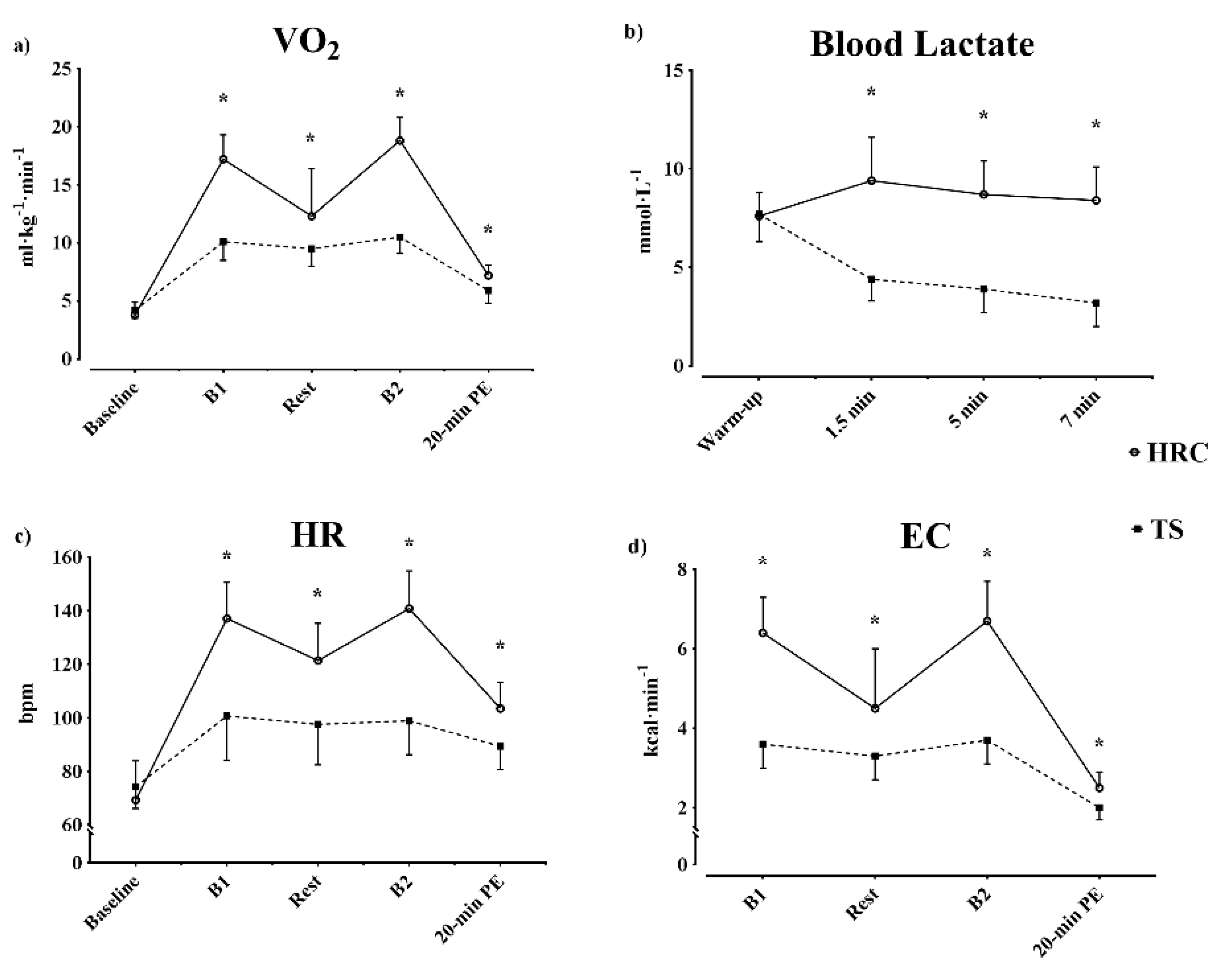
3.1. During the Training Session
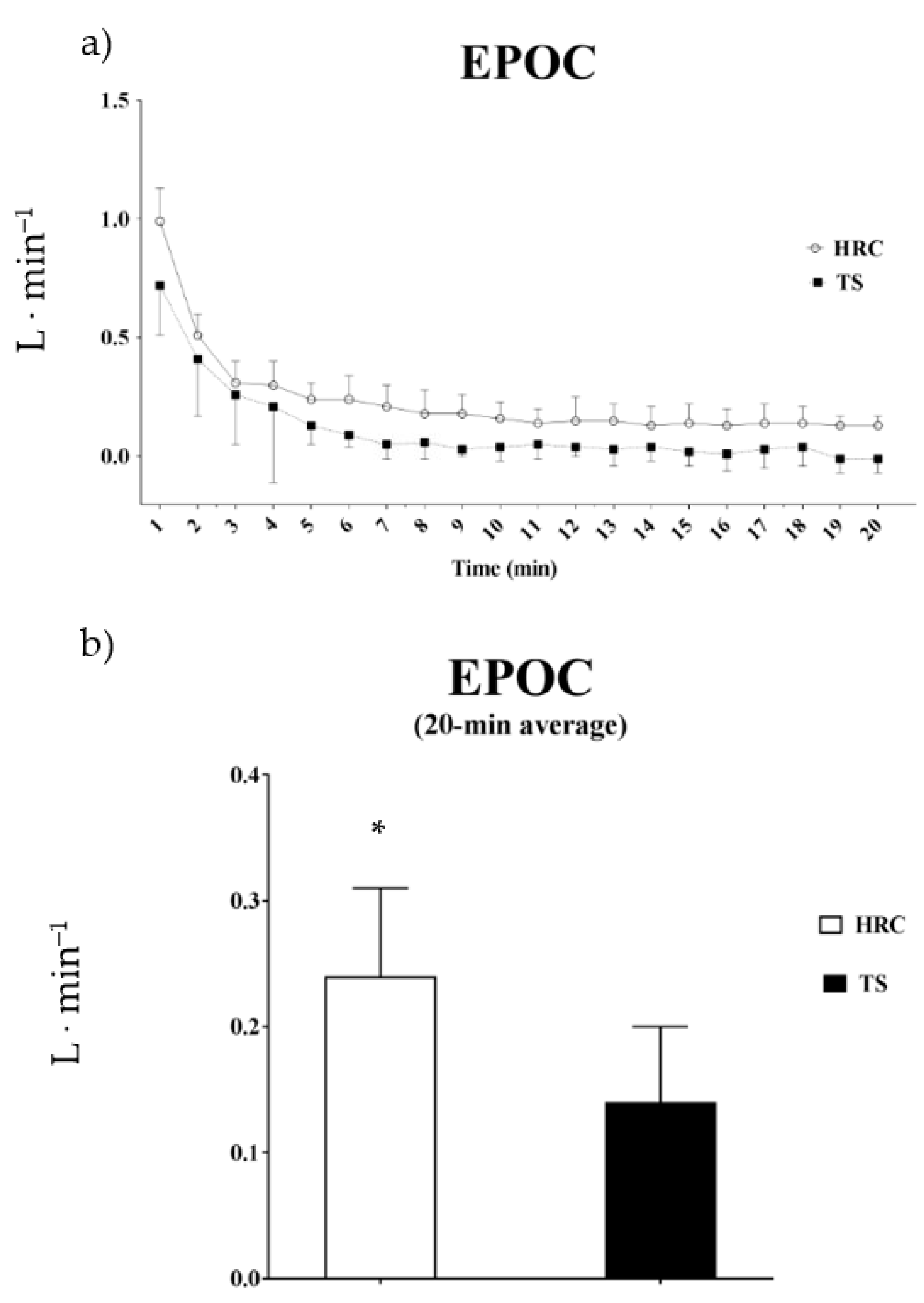
3.2. Post-Training Session
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mohr, M.; Krustrup, P.; Bangsbo, J. Match performance of high-standard soccer players with special reference to development of fatigue. J. Sports Sci. 2003, 21, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Dolci, F.; Hart, N.H.; Kilding, A.E.; Chivers, P.; Piggott, B.; Spiteri, T. Physical and Energetic Demand of Soccer: A Brief Review. Strength Cond. J. 2020, 42, 70–77. [Google Scholar] [CrossRef]
- Impellizzeri, F.M.; Rampinini, E.; Marcora, S.M. Physiological assessment of aerobic training in soccer. J. Sports Sci. 2005, 23, 583–592. [Google Scholar] [CrossRef] [PubMed]
- Bührle, M.; Schmidtbleicher, D. The influence of maximal strength training on movement velocity [in German]. Leistungssport 1977, 7, 3–10. [Google Scholar]
- Wisløff, U.; Castagna, C.; Helgerud, J.; Jones, R.; Hoff, J. Strong correlation of maximal squat strength with sprint performance and vertical jump height in elite soccer players. Br. J. Sports Med. 2004, 38, 285–288. [Google Scholar] [CrossRef]
- Requena, B.; González-Badillo, J.J.; de Villareal, E.S.S.; Ereline, J.; García, I.; Gapeyeva, H.; Pääsuke, M. Functional performance, maximal strength, and power characteristics in isometric and dynamic actions of lower extremities in soccer players. J. Strength Cond. Res. 2009, 23, 1391–1401. [Google Scholar] [CrossRef] [PubMed]
- Lehance, C.; Binet, J.; Bury, T.; Croisier, J.L. Muscular strength, functional performances and injury risk in professional and junior elite soccer players. Scand J. Med. Sci. Sports 2009, 19, 243–251. [Google Scholar] [CrossRef]
- Suchomel, T.J.; Nimphius, S.; Stone, M.H. The Importance of Muscular Strength in Athletic Performance. Sports Med. 2016, 46, 1419–1449. [Google Scholar] [CrossRef]
- Malone, S.; Hughes, B.; Doran, D.A.; Collins, K.; Gabbett, T.J. Can the workload–injury relationship be moderated by improved strength, speed and repeated-sprint qualities? J. Sci. Med. Sport 2019, 22, 29–34. [Google Scholar] [CrossRef]
- Cometti, G. La preparación Física en el Fútbol, 2nd ed.; Editorial Paidotribo: Badalona, Spain, 2007; p. 174. [Google Scholar]
- Griffiths, B.; Grant, J.; Langdown, L.; Gentil, P. The Effect of In-Season Traditional and Explosive Resistance Training Programs on Strength, Jump Height, and Speed in Recreational Soccer Players. Res. Q. Exerc. Sport 2019, 90, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Almasbakk, B.; Hoff, J. Coordination, the determinant of velocity specificity? J. Appl. Physiol. 1996, 81, 2046–2052. [Google Scholar] [CrossRef] [PubMed]
- Kraemer, W.J.; Ratamess, N.A. Fundamentals of resistance training: Progression and exercise prescription. Med. Sci. Sports Exerc. 2004, 36, 674–688. [Google Scholar] [CrossRef]
- Fleck, S.J.; Kraemer, W.J. Resistance training: Physiological responses and adaptation (part 3 of 4). Physician Sportsmed. 1988, 16, 63–66. [Google Scholar] [CrossRef] [PubMed]
- Alcaraz, P.E.; Perez-Gomez, J.; Chavarrias, M.; Blazevich, A.J. Similarity in adaptations to high-resistance circuit vs. traditional strength training in resistance-trained men. J. Strength Cond. Res. 2011, 25, 2519–2527. [Google Scholar] [CrossRef] [PubMed]
- Heggelund, J.; Fimland, M.S.; Helgerud, J.; Hoff, J. Maximal strength training improves work economy, rate of force development and maximal strength more than conventional strength training. Eur. J. Appl. Physiol. 2013, 113, 1565–1573. [Google Scholar] [CrossRef]
- Hakkinen, K.; Newton, R.U.; Gordon, S.E.; McCormick, M.; Volek, J.S.; Nindl, B.C.; Gotshalk, L.A.; Campbell, W.W.; Evans, W.J.; Hakkinen, A.; et al. Changes in muscle morphology, electromyographic activity, and force production characteristics during progressive strength training in young and older men. J. Gerontol. A Biol. Sci. Med. Sci. 1998, 53, B415–B423. [Google Scholar] [CrossRef]
- Paavolainen, L.; Hakkinen, K.; Hamalainen, I.; Nummela, A.; Rusko, H. Explosive-strength training improves 5-km running time by improving running economy and muscle power. J. Appl. Physiol. 1999, 86, 1527–1533. [Google Scholar] [CrossRef]
- Bird, S.P.; Tarpenning, K.M.; Marino, F.E. Designing resistance training programmes to enhance muscular fitness: A review of the acute programme variables. Sports Med. 2005, 35, 841–851. [Google Scholar] [CrossRef]
- Blazevich, A.J.; Jenkins, D.G. Effect of the movement speed of resistance training exercises on sprint and strength performance in concurrently training elite junior sprinters. J. Sports Sci. 2002, 20, 981–990. [Google Scholar] [CrossRef]
- Helgerud, J.; Rodas, G.; Kemi, O.J.; Hoff, J. Strength and endurance in elite football players. Int. J. Sports Med. 2011, 32, 677–682. [Google Scholar] [CrossRef]
- Alcaraz, P.E.; Sanchez-Lorente, J.; Blazevich, A.J. Physical performance and cardiovascular responses to an acute bout of heavy resistance circuit training versus traditional strength training. J. Strength Cond. Res. 2008, 22, 667–671. [Google Scholar] [CrossRef]
- Kraemer, W.J.; Adams, K.; Cafarelli, E.; Dudley, G.A.; Dooly, C.; Feigenbaum, M.S.; Fleck, S.J.; Franklin, B.; Fry, A.C.; Hoffman, J.R.; et al. American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med. Sci. Sports Exerc. 2002, 34, 364–380. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Martínez, F.A.; Rubio-Arias, J.A.; Ramos-Campo, D.J.; Alcaraz, P.E. Effectiveness of resistance circuit-based training for maximum oxygen uptake and upper-body one-repetition maximum improvements: A systematic review and meta-analysis. Sports Med. 2017, 47, 2553–2568. [Google Scholar] [CrossRef]
- Camargo, M.D.; Stein, R.; Ribeiro, J.P.; Schvartzman, P.R.; Rizzatti, M.O.; Schaan, B.D. Circuit weight training and cardiac morphology: A trial with magnetic resonance imaging. Br. J. Sports Med. 2008, 42, 141–145, discussion 145. [Google Scholar] [CrossRef]
- Gamble, P. Strength and Conditioning for Team Sports: Sport-Specific Physical Preparation for High Performance; Taylor & Francis: Milton Park, UK, 2009. [Google Scholar]
- Ramos-Campo, D.J.; Rubio-Arias, J.Á.; Freitas, T.T.; Camacho, A.; Jiménez-Diaz, J.F.; Alcaraz, P.E. Acute physiological and performance responses to high-intensity resistance circuit training in hypoxic and normoxic conditions. J. Strength Cond. Res. 2017, 31, 1040–1047. [Google Scholar] [CrossRef]
- Márquez, G.; Romero-Arenas, S.; Marín-Pagán, C.; Vera-Ibañez, A.; FernáNdez Del Olmo, M.; Taube, W. Peripheral and central fatigue after high intensity resistance circuit training. Muscle Nerve 2017, 56, 152–159. [Google Scholar] [CrossRef]
- Freitas, T.T.; Calleja-González, J.; Alarcón, F.; Alcaraz, P.E. Acute effects of two different resistance circuit training protocols on performance and perceived exertion in semiprofessional basketball players. J. Strength Cond. Res. 2016, 30, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Wasserman, K.; Beaver, W.L.; Whipp, B.J. Gas exchange theory and the lactic acidosis (anaerobic) threshold. Circulation 1990, 81, II14–II30. [Google Scholar]
- Weir, J.B. New methods for calculating metabolic rate with special reference to protein metabolism. J. Physiol. 1949, 109, 1–9. [Google Scholar] [CrossRef]
- American College of Sports Medicine. American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med. Sci. Sports Exerc. 2009, 41, 687–708. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: Abingdon, UK, 1988. [Google Scholar]
- Hopkins, W.; Marshall, S.; Batterham, A.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3. [Google Scholar] [CrossRef]
- ACSM. American College of Sports Medicine Position Stand. The recommended quantity and quality of exercise for developing and maintaining cardiorespiratory and muscular fitness, and flexibility in healthy adults. Med. Sci. Sports Exerc. 1998, 30, 975–991. [Google Scholar]
- Astrand, P.O.; Rodahl, K. Textbook of Work Physiology; McGraw-Hill Book Company: New York, NY, USA, 1986. [Google Scholar]
- Tomlin, D.L.; Wenger, H.A. The relationship between aerobic fitness and recovery from high intensity intermittent exercise. Sports Med. 2001, 31, 1–11. [Google Scholar] [CrossRef]
- Helgerud, J.; Engen, L.C.; Wisloff, U.; Hoff, J. Aerobic endurance training improves soccer performance. Med. Sci. Sports Exerc. 2001, 33, 1925–1931. [Google Scholar] [CrossRef] [PubMed]
- Shephard, R.J. Biology and medicine of soccer: An update. J. Sports Sci. 1999, 17, 757–786. [Google Scholar] [CrossRef]
- Thomas, V.; Reilly, T. Fitness assessment of English league soccer players through the competitive season. Br. J. Sports Med. 1979, 13, 103–109. [Google Scholar] [CrossRef]
- Stolen, T.; Chamari, K.; Castagna, C.; Wisloff, U. Physiology of soccer: An update. Sports Med. 2005, 35, 501–536. [Google Scholar] [CrossRef]
- Fleck, S.J. Cardiovascular adaptations to resistance training. Med. Sci. Sports Exerc. 1988, 20, S146–S151. [Google Scholar] [CrossRef] [PubMed]
- Halouani, J.; Chtourou, H.; Gabbett, T.; Chaouachi, A.; Chamari, K. Small-sided games in team sports training: A brief review. J. Strength Cond. Res. 2014, 28, 3594–3618. [Google Scholar] [CrossRef]
- Abel, M.G.; Mortara, A.J.; Pettitt, R.W. Evaluation of circuit-training intensity for firefighters. J. Strength Cond. Res. 2011, 25, 2895–2901. [Google Scholar] [CrossRef]
- Beckham, S.G.; Earnest, C.P. Metabolic cost of free weight circuit weight training./Cout metabolique d’ un entrainement de musculation a charge libre en circuit. J. Sports Med. Phys. Fit. 2000, 40, 118–125. [Google Scholar]
- Gotshalk, L.A.; Berger, R.A.; Kraemer, W.J. Cardiovascular responses to a high-volume continuous circuit resistance training protocol. J. Strength Cond. Res. 2004, 18, 760–764. [Google Scholar] [CrossRef] [PubMed]
- Wilmore, J.H.; Parr, R.B.; Ward, P.; Vodak, P.A.; Barstow, T.J.; Pipes, T.V.; Grimditch, G.; Leslie, P. Energy cost of circuit weight training. Med. Sci. Sports 1978, 10, 75–78. [Google Scholar]
- Machado, M.; Koch, A.J.; Willardson, J.M.; Pereira, L.S.; Cardoso, M.I.; Motta, M.K.; Pereira, R.; Monteiro, A.N. Effect of varying rest intervals between sets of assistance exercises on creatine kinase and lactate dehydrogenase responses. J. Strength Cond. Res. 2011, 25, 1339–1345. [Google Scholar] [CrossRef] [PubMed]
- Paoli, A.; Moro, T.; Marcolin, G.; Neri, M.; Bianco, A.; Palma, A.; Grimaldi, K. High-Intensity Interval Resistance Training (HIRT) influences resting energy expenditure and respiratory ratio in non-dieting individuals. J. Transl. Med. 2012, 10, 237. [Google Scholar] [CrossRef]
- Romero-Arenas, S.; Blazevich, A.J.; Martinez-Pascual, M.; Perez-Gomez, J.; Luque, A.J.; Lopez-Roman, F.J.; Alcaraz, P.E. Effects of high-resistance circuit training in an elderly population. Exp. Gerontol. 2013, 48, 334–340. [Google Scholar] [CrossRef]
- Harber, M.P.; Fry, A.C.; Rubin, M.R.; Smith, J.C.; Weiss, L.W. Skeletal muscle and hormonal adaptations to circuit weight training in untrained men. Scand. J. Med. Sci. Sports 2004, 14, 176–185. [Google Scholar] [CrossRef]
- Faigenbaum, A.D.; Kraemer, W.J.; Blimkie, C.J.; Jeffreys, I.; Micheli, L.J.; Nitka, M.; Rowland, T.W. Youth resistance training: Updated position statement paper from the national strength and conditioning association. J. Strength Cond. Res. 2009, 23, S60–S79. [Google Scholar] [CrossRef]
- Kraemer, W.J.; Marchitelli, L.; Gordon, S.E.; Harman, E.; Dziados, J.E.; Mello, R.; Frykman, P.; McCurry, D.; Fleck, S.J. Hormonal and growth factor responses to heavy resistance exercise protocols. J. Appl. Physiol. 1990, 69, 1442–1450. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Age (y) | Height (cm) | Mass (kg) | O2max (mL·kg−1·min−1) | VT2 (% of O2max) | HRmax (Beats·min−1) |
|---|---|---|---|---|---|
| 23.1 ± 3.8 | 176.3 ± 6.3 | 70.0 ± 6.2 | 58.2 ± 1.9 | 81.9 ± 4.4 | 196.5 ± 8.4 |
| Variable | HRC | TS | ES (95% CI) |
|---|---|---|---|
| O2/BM (mL·kg−1·min−1) | 18.0 ± 1.9 * | 10.3 ± 1.5 | 4.31 (2.71–5.91) |
| O2 relative to O2máx (%) | 30.9 ± 3.0 * | 17.7 ± 2.5 | 4.58 (2.91–6.25) |
| O2 relative to VO2VT2 (%) | 37.8 ± 3.5 * | 21.6 ± 2.8 | 4.90 (3.14–6.65) |
| HR (beats·min−1) | 139.0 ± 13.2 * | 100.8 ± 13.8 | 2.71 (1.50–3.92) |
| HR relative to HRmáx (%) | 70.6 ± 7.3 * | 51.4 ± 6.7 | 2.62 (1.43–3.82) |
| HR relative to HRVT2 (%) | 76.9 ± 7.6 * | 55.7 ± 6.1 | 2.95 (1.68–4.21) |
| RER | 1.12 ± 0.03 * | 1.05 ± 0.02 | 2.63 (1.43–3.83) |
| EC (kcal·min−1) | 5.8 ± 1.0 * | 3.5 ± 0.6 | 2.67 (1.47–3.88) |
| Variable | HRC | TS | ES (95% CI) |
|---|---|---|---|
| EC (kcal·min−1) | 2.5 ± 0.4 * | 2.0 ± 0.3 | 1.35 (0.38–2.33) |
| EPOC (L O2) | 5.2 ± 1.4 * | 2.3 ± 0.9 | 2.36 (1.22–3.50) |
| HR (beats·min−1) | 103.6 ± 9.5 * | 89.4 ± 8.7 | 1.49 (0.50–2.48) |
| RER | 0.92 ± 0.05 | 0.91 ± 0.06 | 0.17 (−0.70–1.05) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marín-Pagán, C.; Blazevich, A.J.; Chung, L.H.; Romero-Arenas, S.; Freitas, T.T.; Alcaraz, P.E. Acute Physiological Responses to High-Intensity Resistance Circuit Training vs. Traditional Strength Training in Soccer Players. Biology 2020, 9, 383. https://doi.org/10.3390/biology9110383
Marín-Pagán C, Blazevich AJ, Chung LH, Romero-Arenas S, Freitas TT, Alcaraz PE. Acute Physiological Responses to High-Intensity Resistance Circuit Training vs. Traditional Strength Training in Soccer Players. Biology. 2020; 9(11):383. https://doi.org/10.3390/biology9110383
Chicago/Turabian StyleMarín-Pagán, Cristian, Anthony J. Blazevich, Linda H. Chung, Salvador Romero-Arenas, Tomás T. Freitas, and Pedro E. Alcaraz. 2020. "Acute Physiological Responses to High-Intensity Resistance Circuit Training vs. Traditional Strength Training in Soccer Players" Biology 9, no. 11: 383. https://doi.org/10.3390/biology9110383
APA StyleMarín-Pagán, C., Blazevich, A. J., Chung, L. H., Romero-Arenas, S., Freitas, T. T., & Alcaraz, P. E. (2020). Acute Physiological Responses to High-Intensity Resistance Circuit Training vs. Traditional Strength Training in Soccer Players. Biology, 9(11), 383. https://doi.org/10.3390/biology9110383