Modeling the Impact of Unreported Cases of the COVID-19 in the North African Countries



Simple Summary
Abstract
1. Introduction and Model Construction
2. Approximation of the Parameters
Predictive Results
3. The Impact of the COVID-19 Testing Efficacy in Egypt
4. The Influence of Relaxation of the Measures on the Spread of COVID 19 in the North African Countries
- Algeria:
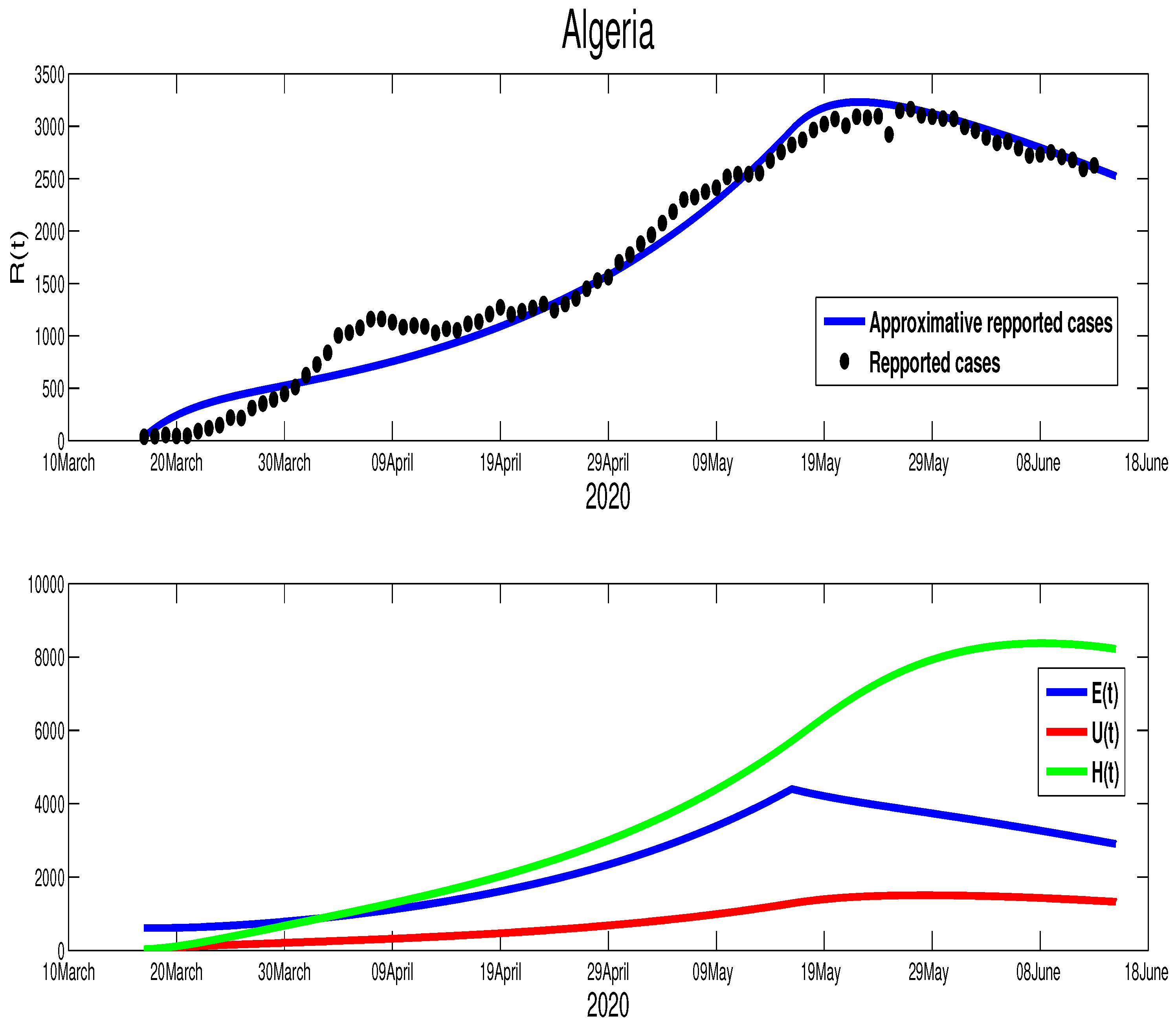
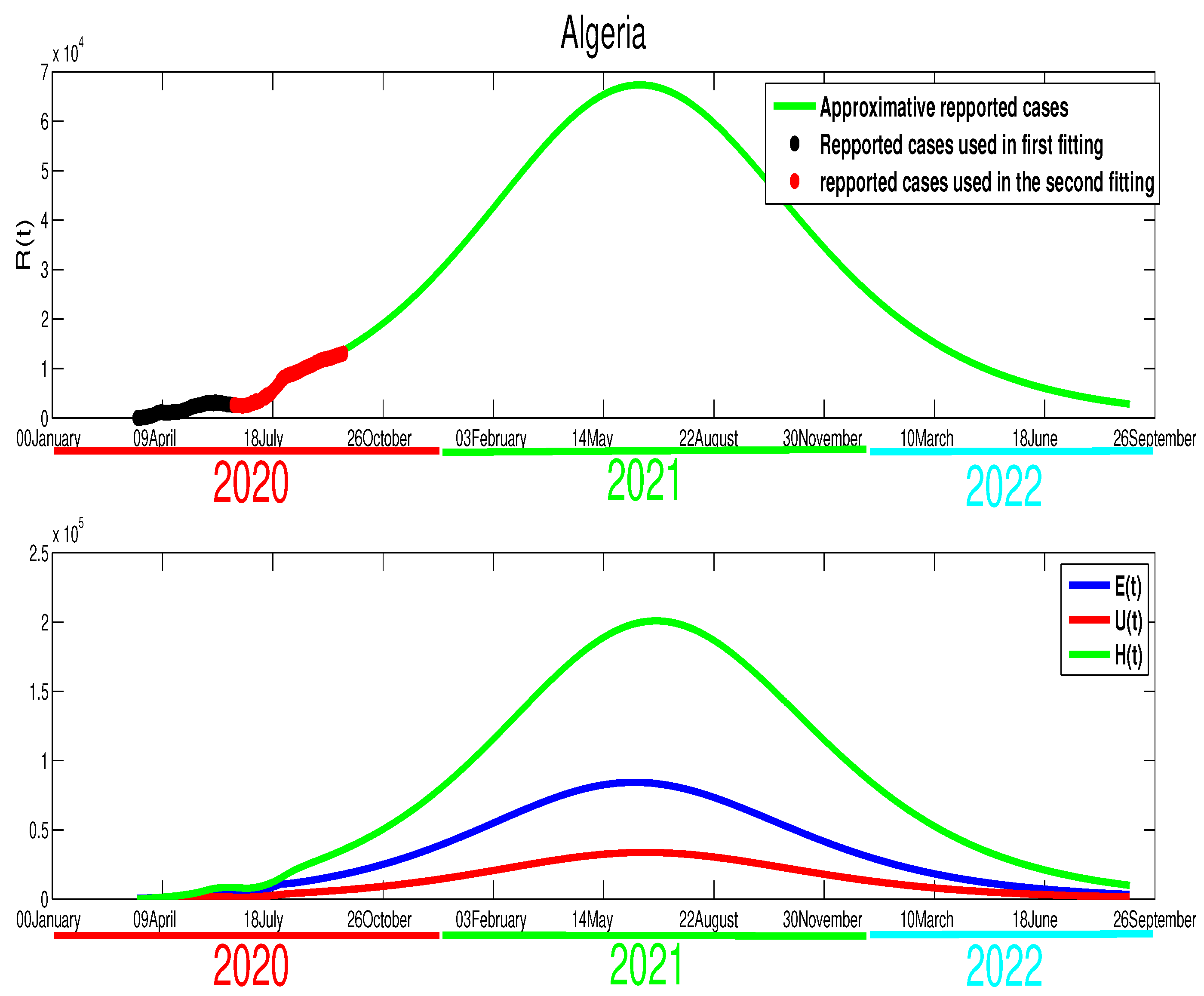
- In the previous section, our simulation showed that the COVID-19 epidemic in Algeria would be finished by the end of September, which has been highlighted clearly in Figure 10 by the figure in blue. However, because of the wrong time of relaxing the population mobility, the actual data highlighted in red points in the same figure suggest a different outcome. Indeed, as shown in Figure 10, there is an increase in infection cases (stage 3). After this holiday, the rate decreased slightly (stage 4). The relaxation of measures was inevitable because the lockdown made a huge economic deficit. It left no choice for the decision-makers to reduce the severity of the measures and try to live with the fact that COVID-19 will continue spreading in the Algerian community. The corresponding transmission rate that considered in the fourth stages in Figure 10 is expressed in the following manner,where , and , . In Figure 12, we can deduce that this decision will have a huge impact on the evolution of the infection cases, which needs to be revised again before losing control of the spread of this contagious disease. We predict a higher decrease in the first weeks of October because reopening the schools and universities on 20 September 2020 will lead to more acute infection cases.
- Morocco:
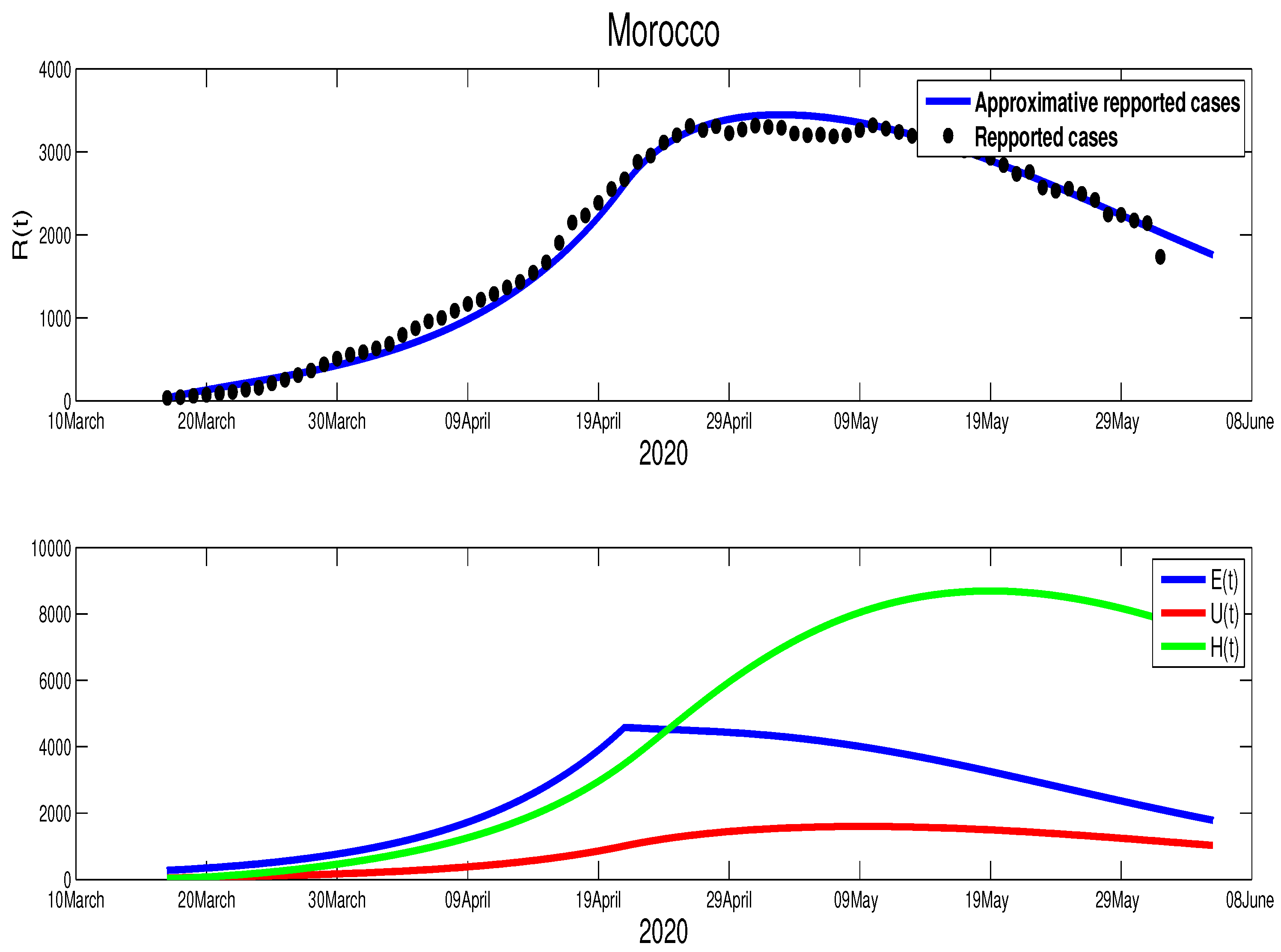
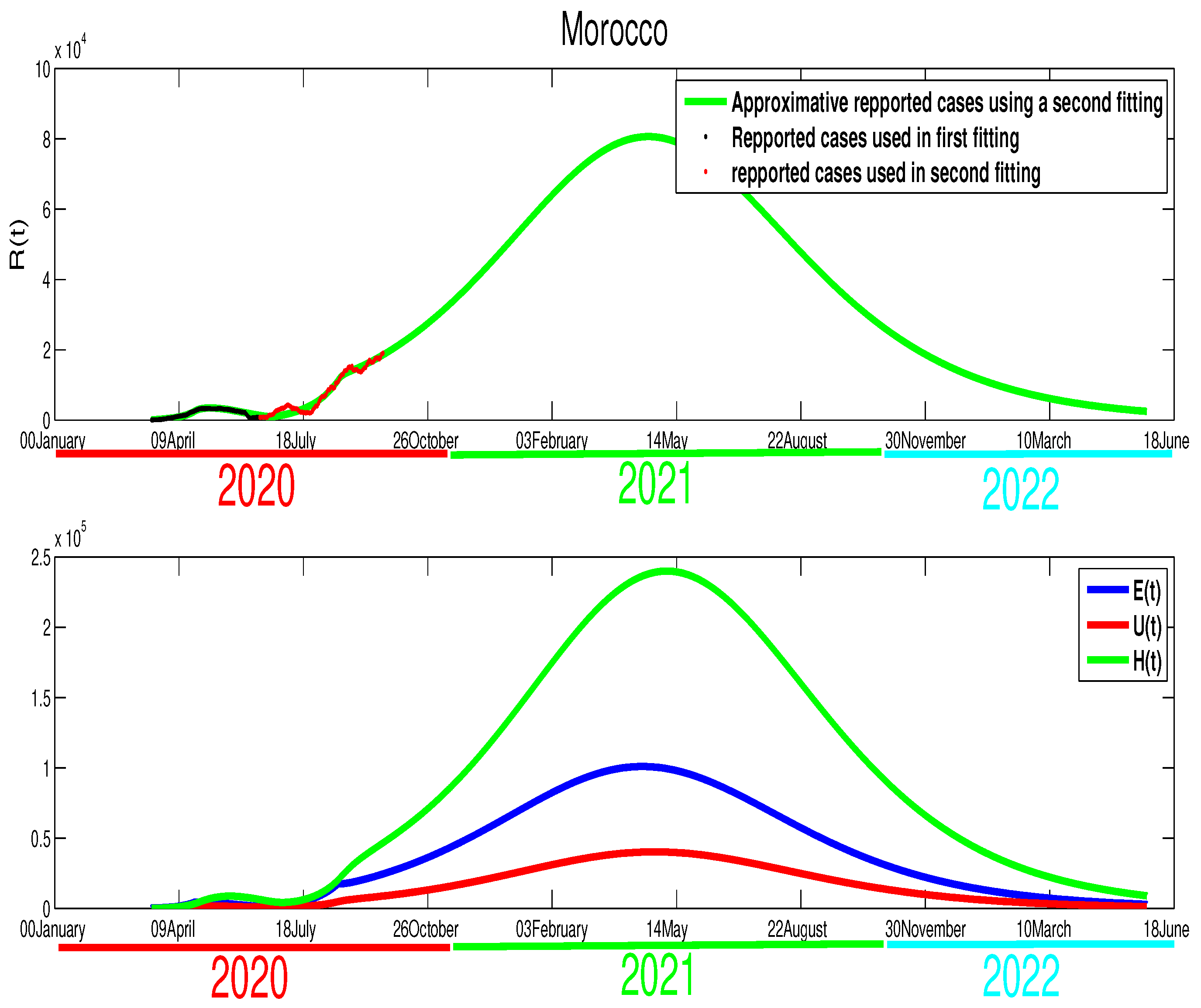
- As the data show, the similarity between the evolution of the infection cases in the two countries (Algeria and Morocco) can be seen clearly in Figure 10 and Figure 11, where it is obtained that the COVID-19 disease spreads in this country through four principal stages as it is highlighted in Figure 11. Morocco’s situation is similar to Algeria, where the Moroccan authorities decided to relax the population mobility before the Eid, which led to an increase in the number of acute infection cases. Based on these mentioned points, we can write the transmission rate aswhere , and , . It can be seen clearly that there is a continued increase in infection cases, as highlighted in Figure 13. If the disease’s progress goes in the same way, we also expect that the infection will disappear by the end of 2021.
- Egypt:
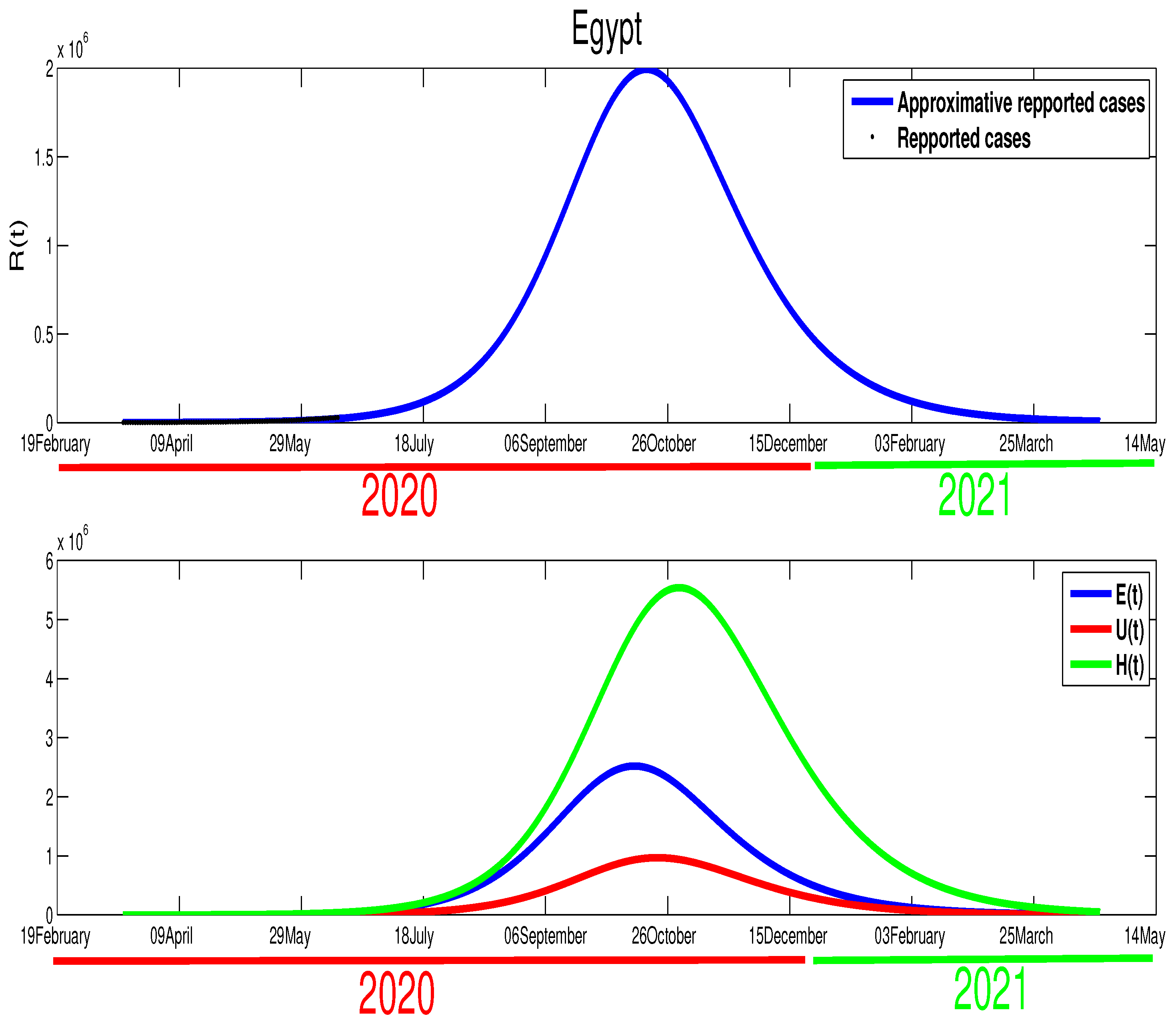
- The case in Egypt is entirely different than Algeria and Morocco. The relaxation of the measures in the Eid period did not make any difference in the number of cases. Our only explanation is the lack of reported cases. The evolution of infection cases follows three stages, as it is highlighted in Figure 14. It worth mentioning that there is a decrease in the number of in the period of Eid; this decrease continued until mid-September. If the situation continues in the same way, the infection will disappear by the end of 2020 or the beginning of 2021 as it is shown in Figure 15. Using Figure 14, we can consider that the transmission rate takes the following formulation,where , , .
5. Discussion and Concluding Remarks
- Egypt:
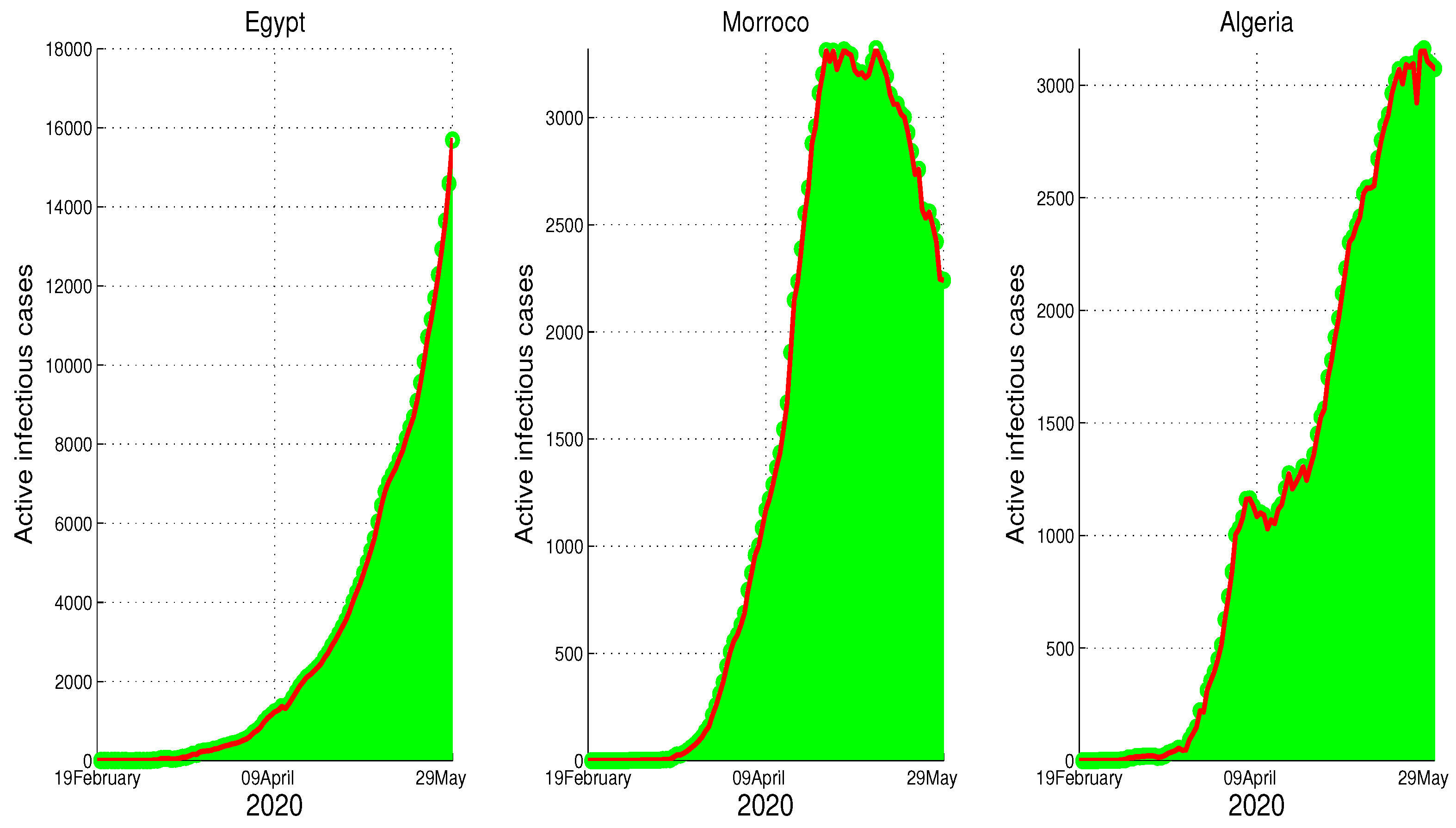
- The restrictions in this country were not well respected. This conclusion is based on the evolution of the infection cases presented in Figure 1 where all the infection cases (asymptomatic, reported, unreported, and hospitalized) continued to rise. This led us to claim that if not measure is taking, the infection will not disappear any time soon (see Figure 5). As the lockdown and restriction of human mobility can be costly on Egypt’s economy, it is important to find alternative measures to contain the spread of the COVID-19. For this purpose, we suggested having massive testing for the population. Augmenting the number of tests per day is one of the most useful tools to reduce the size of the epidemic and lower the burden on the public health facilities, Figure 9 shows that with T = 0.01, can reduce the number of unreported cases by and hospitalize by . As we could not track the number of tests performed by the Egyptian authorities, by increasing T to a level the fit the data after 14 June to 9 August, we could get the level of the infected case as of today. We also investigate the impact of the Eid holiday on the progress of the disease in Egypt. Our study showed no effect of the relaxation of the restriction on human mobility on the number of cases.
- Morocco:
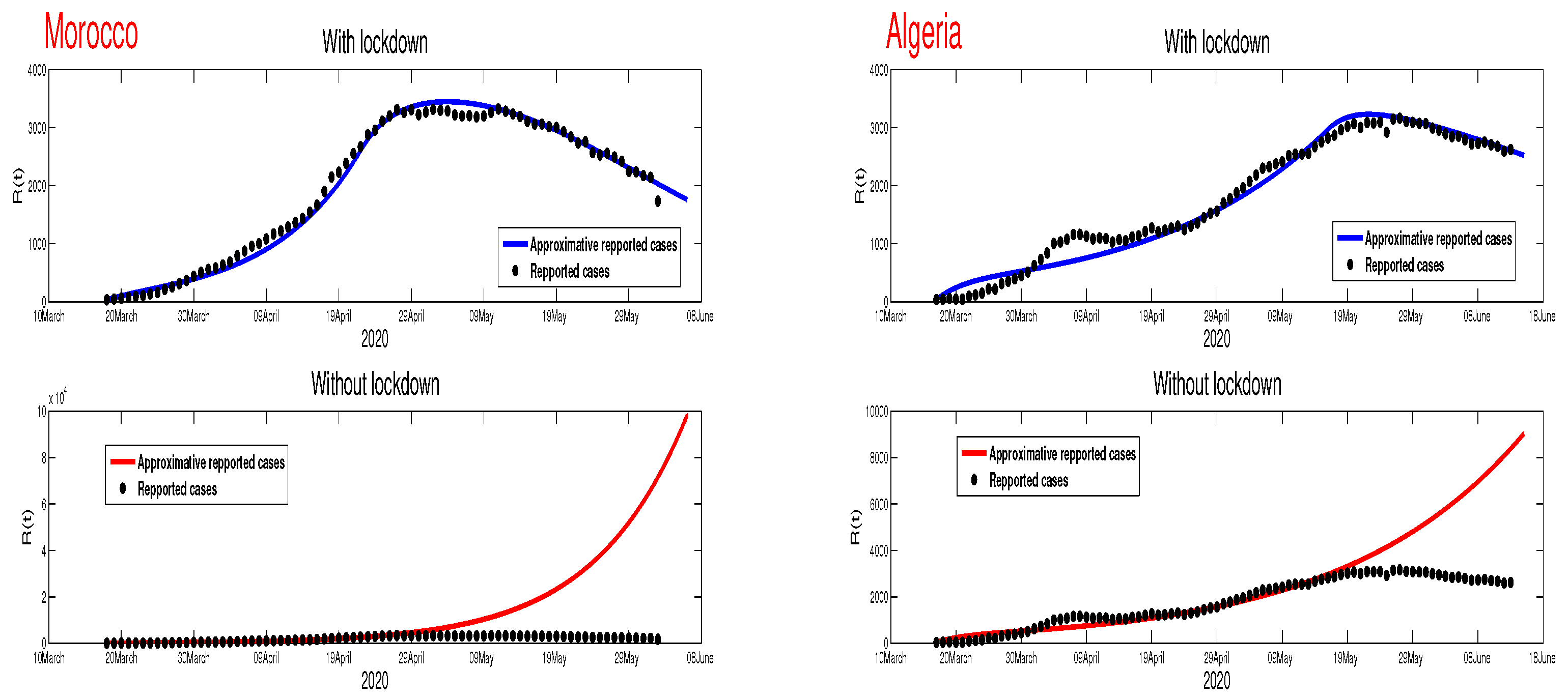
- Up to relaxing the lockdown, Morocco was doing great in obligating citizens to respect the lockdown. The infection cases were going remarkably down, and the population mobility in the public places was substantially reduced. We also predicted that the infection would disappear from the Moroccan community by 7 August 2020. The lockdown in Morocco was more effective than one done in Algeria and Egypt, which is reflected by the high rate of the lockdown efficiently . It was proved that the lockdown had a huge role in reducing the number of infection cases in this country and reducing hospitals’ pressure. Without the restrictions, there would have been a drastic increase in infection cases, as highlighted in Figure 8 as the restriction had a very bad influence on the economy. Therefore, many countries, including Morocco, tried to ease its lockdown by removing some bans on the population mobility, which led to an unavoidable increase in infection cases due to the mobility’s augmentation. In fact, the authorities relaxed the restriction one month before the Eid, and the country could not manage the aftermath of the lockdown (See Figure 11), and the country is having a second wave of the COVID-19 disease. As of the 14 June, the number of unreported cases was over 1000 and the number of asymptomatic was around 3000. By increasing the number of tests COVID-19 capacity in the country, it is unavoidable to see a huge increase in the number of the COVID-19 cases. With this trend of daily increase of cases, our simulation projects the end of 2021 ( see Figure 13).
- Algeria:
- As mentioned before, this country is similar to Morocco. It exhibited an effective lockdown with less efficiency (). We predicted that, if the aftermath of the lockdown was managed adequately, the COVID-19 epidemic would end by 1 October 2020. In a similar fashion, the Algerian authorities tried to relax the lockdown by reducing the severity of the restriction population mobility between regions and opening stores and parks in the cities that did not report any infection cases. However, such a decision should be strictly observed by the population and mandate everyone to follow the government guideline. The relaxation of the restriction before the Eid was the reason for the second wave of the COVID-19 (See Figure 10). In fact, by 14 June, the number of unreported cases was over 1500, and the number of asymptomatic was around 3300). By increasing the number of tests COVID-19 in Algeria, we see a continued increase in the number of the COVID-19 cases. Our simulation projects the end of 2021 ( see Figure 12).
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
References
- Galvani, A.P.; May, R.M. Dimensions of superspreading. Nature 2005, 438, 293–295. [Google Scholar] [PubMed]
- Cave, E. COVID-19 super-spreaders: Definitional quandaries and implications. Asian Bioeth. Rev. 2020, 12, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.K.; Liu, X.F.; Wu, Y.; Ali, S.T.; Du, Z.; Bosetti, P.; Lau, E.H.; Cowling, B.J.; Wang, L. Reconstruction of transmission pairs for novel coronavirus disease 2019 (COVID-19) in mainland China: Estimation of super-spreading events, serial interval, and hazard of infection. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Al-Tawfiq, J.; Rodriguez-Morales, A. Super-spreading events and contribution to transmission of MERS, SARS, and COVID-19. J. Hosp. Infect. 2020, 105, 111–112. [Google Scholar] [CrossRef] [PubMed]
- Günther, T.; Czech-Sioli, M.; Indenbirken, D.; Robitailles, A.; Tenhaken, P.; Exner, M.; Ottinger, M.; Fischer, N.; Grundhoff, A.; Brinkmann, M.M. Investigation of a Superspreading Event Preceding the Largest Meat Processing Plant-Related SARS-Coronavirus 2 Outbreak in Germany. Available at SSRN 3654517. 2020. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3654517 (accessed on 9 October 2020).
- Roser, M.; Ritchie, H.; Ortiz-Ospina, E.; Hasell, J. Coronavirus Pandemic (COVID-19); Our World in Data: 2020. Available online: https://ourworldindata.org/coronavirus (accessed on 9 October 2020).
- Kuniya, T. Prediction of the epidemic peak of coronavirus disease in Japan, 2020. J. Clin. Med. 2020, 9, 789. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Magal, P.; Seydi, O.; Webb, G. Understanding unreported cases in the COVID-19 epidemic outbreak in Wuhan, China, and the importance of major public health interventions. Biology 2020, 9, 50. [Google Scholar] [CrossRef] [PubMed]
- Magal, P.; Webb, G. Predicting the Number of Reported and Unreported Cases for the COVID-19 Epidemic in South Korea, Italy, France and Germany. 2020. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3557360 (accessed on 9 October 2020).
- Sun, H.; Qiu, Y.; Yan, H.; Huang, Y.; Zhu, Y.; Chen, S.X. Tracking and predicting COVID-19 epidemic in china mainland. medRxiv 2020. [Google Scholar] [CrossRef]
- Hellewell, J.; Abbott, S.; Gimma, A.; Bosse, N.I.; Jarvis, C.I.; Russell, T.W.; Munday, J.D.; Kucharski, A.J.; Edmunds, W.J.; Sun, F.; et al. Feasibility of controlling COVID-19 outbreaks by isolation of cases and contacts. Lancet Glob. Health 2020, 8, e488–e496. [Google Scholar] [CrossRef]
- Choi, S.; Ki, M. Estimating the reproductive number and the outbreak size of COVID-19 in Korea. Epidemiol. Health 2020, 42, e2020011. [Google Scholar] [CrossRef] [PubMed]
- Kucharski, A.J.; Russell, T.W.; Diamond, C.; Liu, Y.; Edmunds, J.; Funk, S.; Eggo, R.M.; Sun, F.; Jit, M.; Munday, J.D.; et al. Early dynamics of transmission and control of COVID-19: A mathematical modelling study. Lancet Infect. Dis. 2020, 20, 553–558. [Google Scholar] [CrossRef]
- Lin, Q.; Zhao, S.; Gao, D.; Lou, Y.; Yang, S.; Musa, S.S.; Wang, M.H.; Cai, Y.; Wang, W.; Yang, L.; et al. A conceptual model for the outbreak of Coronavirus disease 2019 (COVID-19) in Wuhan, China with individual reaction and governmental action. Int. J. Infect. Dis. 2020, 93, 211–216. [Google Scholar] [CrossRef]
- Xie, J.; Tong, Z.; Guan, X.; Du, B.; Qiu, H.; Slutsky, A.S. Critical care crisis and some recommendations during the COVID-19 epidemic in China. Intensive Care Med. 2020, 46, 837–840. [Google Scholar] [CrossRef]
- Improta, G.; Russo, M.A.; Triassi, M.; Converso, G.; Murino, T.; Santillo, L.C. Use of the AHP methodology in system dynamics: Modelling and simulation for health technology assessments to determine the correct prosthesis choice for hernia diseases. Math. Biosci. 2018, 299, 19–27. [Google Scholar] [CrossRef]
- Cotta, R.M.; Naveira-Cotta, C.P.; Magal, P. Mathematical Parameters of the COVID-19 Epidemic in Brazil and Evaluation of the Impact of Different Public Health Measures. Biology 2020, 9, 220. [Google Scholar] [CrossRef]
- Aktay, A.; Bavadekar, S.; Cossoul, G.; Davis, J.; Desfontaines, D.; Fabrikant, A.; Gabrilovich, E.; Gadepalli, K.; Gipson, B.; Guevara, M.; et al. Google COVID-19 Community Mobility Reports; Google: Mountain View, CA, USA, 2020. [Google Scholar]
- Apple. Mobility Trend Reports; Apple: Cupertino, CA, USA, 2020. [Google Scholar]
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- WHO. Coronavirus Disease (COVID-2019) Situation Reports; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Wadvalla, B.A. How Africa has tackled COVID-19. BMJ 2020, 370, m2830. [Google Scholar] [CrossRef] [PubMed]
- Peto, J. Covid-19 mass testing facilities could end the epidemic rapidly. BMJ 2020, 368. [Google Scholar] [CrossRef] [PubMed]
- Bentout, S.; Tridane, A.; Djilali, S.; Touaoula, T.M. Age-structured modeling of COVID-19 epidemic in the USA, UAE and Algeria. Alex. Eng. J. 2020. [Google Scholar] [CrossRef]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | Stage 1 | Stage 2 | Stage 3 | Stage 4 |
|---|---|---|---|---|
| Egypt () | 1.3641 | 1.1919 | ||
| Morocco () | 1.6141 | 1.3493 | 1.0971 | |
| Algeria () | 1.2859 | 1.2563 | 1.0819 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Djilali, S.; Benahmadi, L.; Tridane, A.; Niri, K. Modeling the Impact of Unreported Cases of the COVID-19 in the North African Countries. Biology 2020, 9, 373. https://doi.org/10.3390/biology9110373
Djilali S, Benahmadi L, Tridane A, Niri K. Modeling the Impact of Unreported Cases of the COVID-19 in the North African Countries. Biology. 2020; 9(11):373. https://doi.org/10.3390/biology9110373
Chicago/Turabian StyleDjilali, Salih, Lahbib Benahmadi, Abdessamad Tridane, and Khadija Niri. 2020. "Modeling the Impact of Unreported Cases of the COVID-19 in the North African Countries" Biology 9, no. 11: 373. https://doi.org/10.3390/biology9110373
APA StyleDjilali, S., Benahmadi, L., Tridane, A., & Niri, K. (2020). Modeling the Impact of Unreported Cases of the COVID-19 in the North African Countries. Biology, 9(11), 373. https://doi.org/10.3390/biology9110373