
Explainable AI for Oral Cancer Diagnosis: Multiclass Classification of Histopathology Images and Grad-CAM Visualization



Simple Summary
Abstract
1. Introduction
- a DL model for oral squamous cell carcinoma multiclass grading, which may enhance the objectiveness and repeatability of histopathological analysis and reduce the amount of time required for pathological inspections,
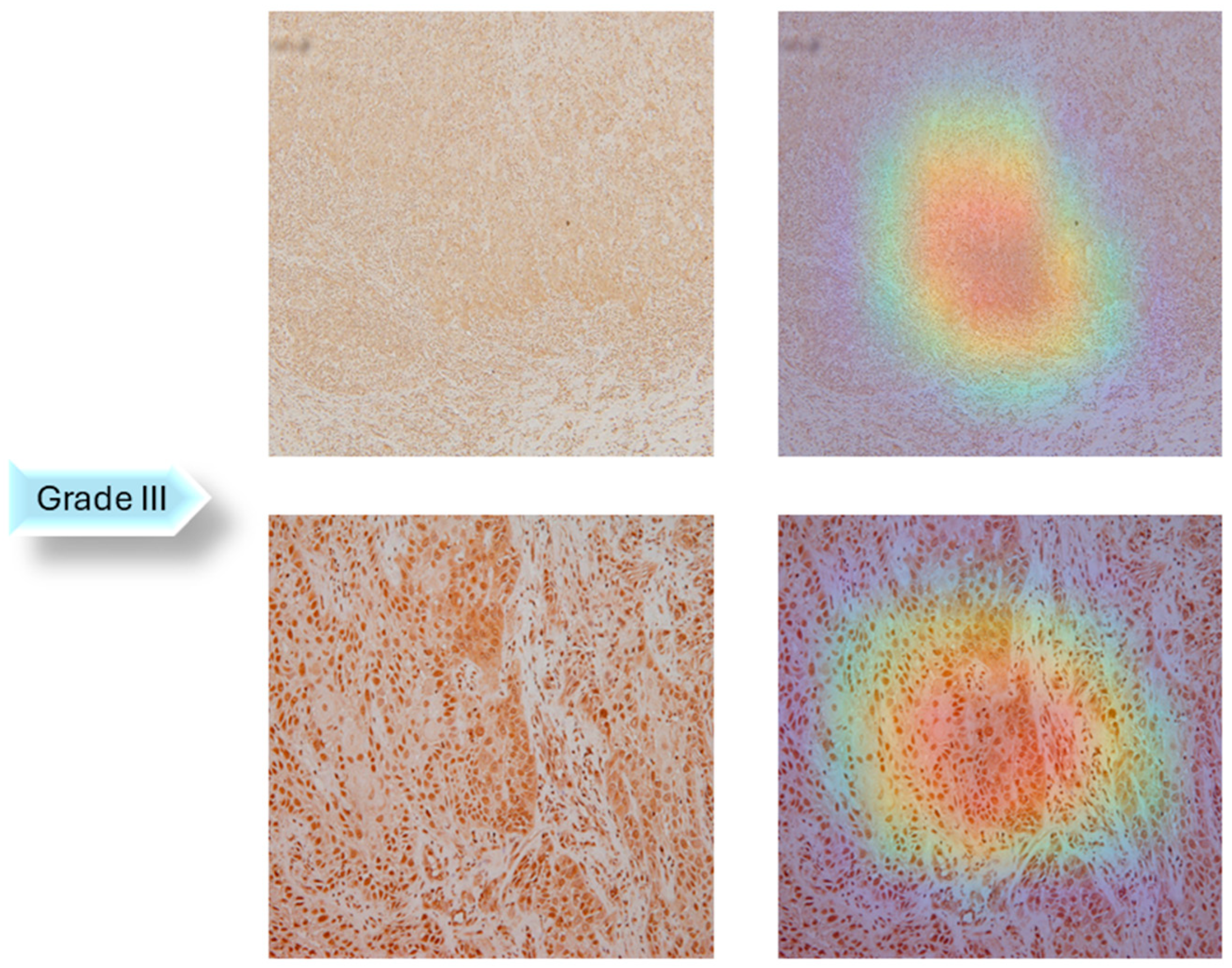
- improving trust and transparency in the AI-based diagnostic process by providing comprehensible insights utilizing Grad-CAM.
Related Work
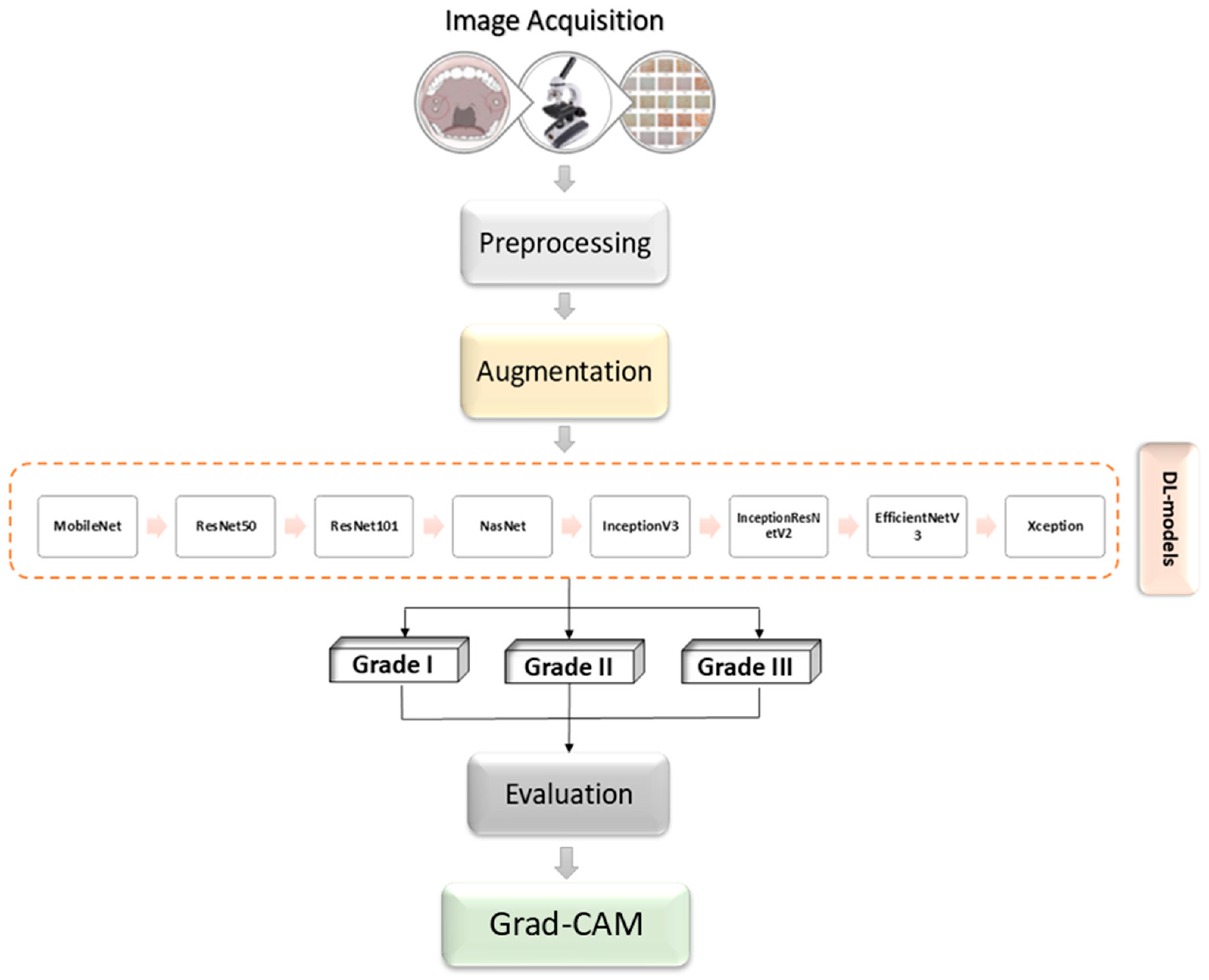
2. Materials and Methods
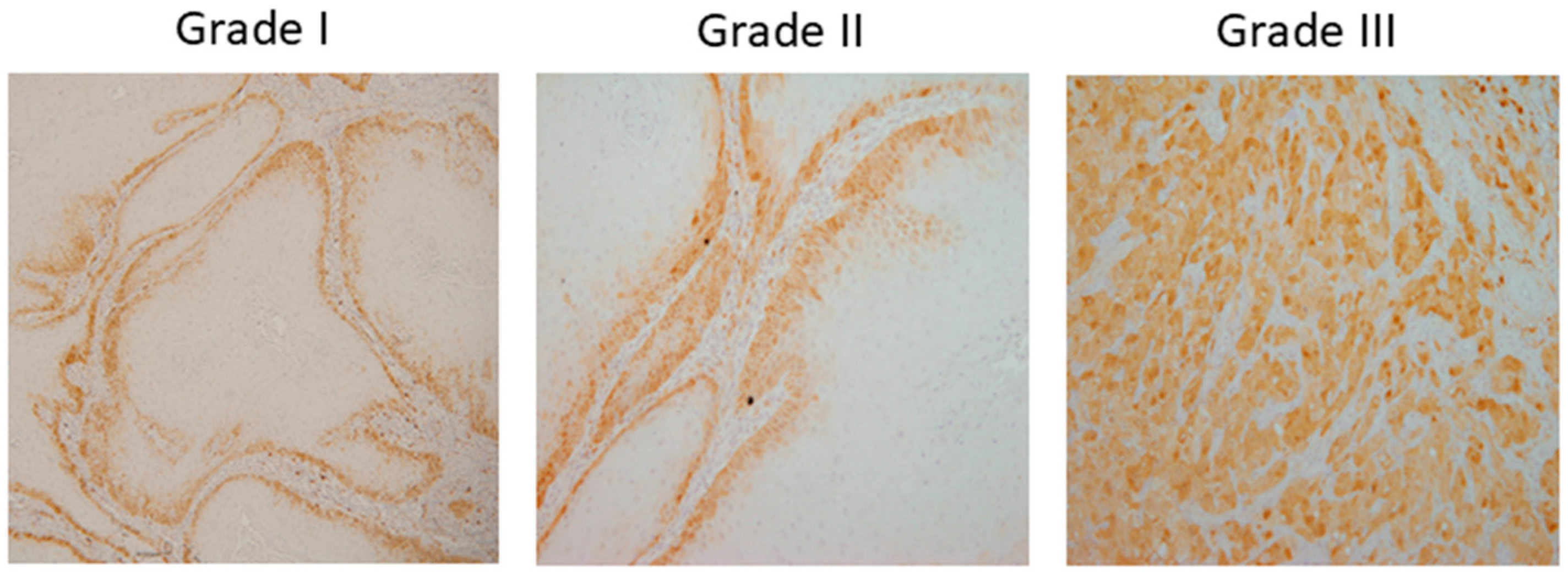
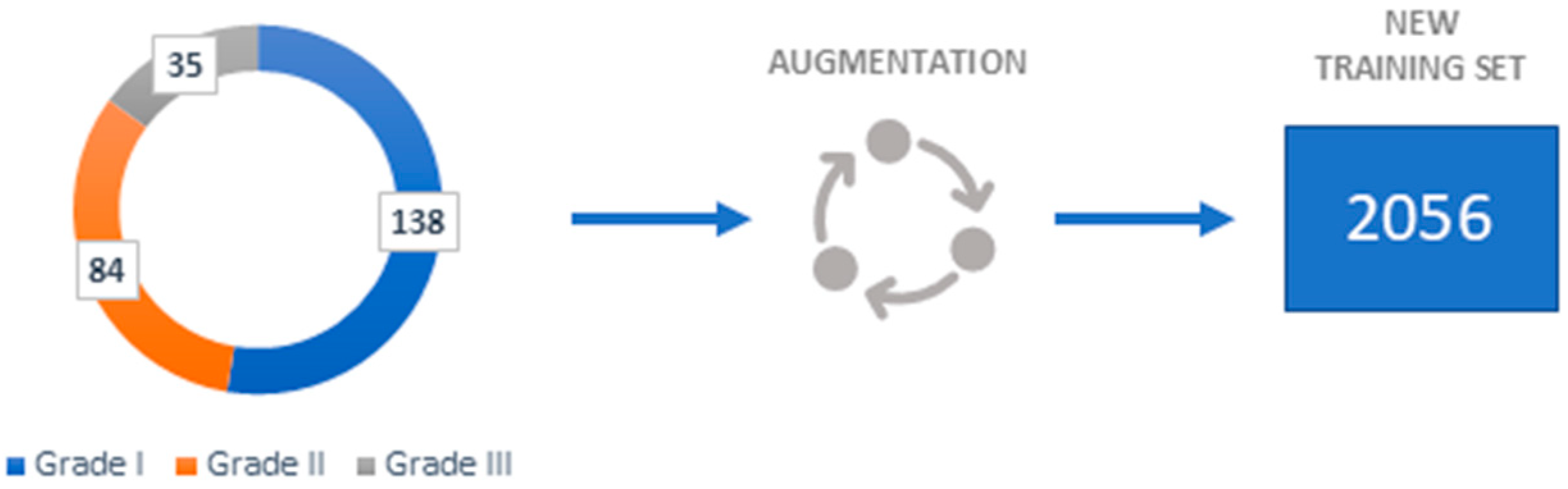
2.1. Dataset Description
2.2. Gradient Weighted Class Activation Mapping (Grad-CAM)
2.3. Deep Learning Models
- ResNet—Since training deep neural networks is challenging, He et al. (2016) introduce a residual learning system for training networks significantly deeper than previously used networks [25]. They evaluated residual nets with a depth of up to 152 layers on the ImageNet which resulted in a 3.57% error [25]
- MobileNetv2—Sandler et al. (2018) describe a new mobile architecture called MobileNetv2. Their basic building unit has many characteristics that make it especially well-suited for mobile applications [26]. The described architecture enhances the state-of-the-art for a wide range of performance points on the ImageNet dataset [26].
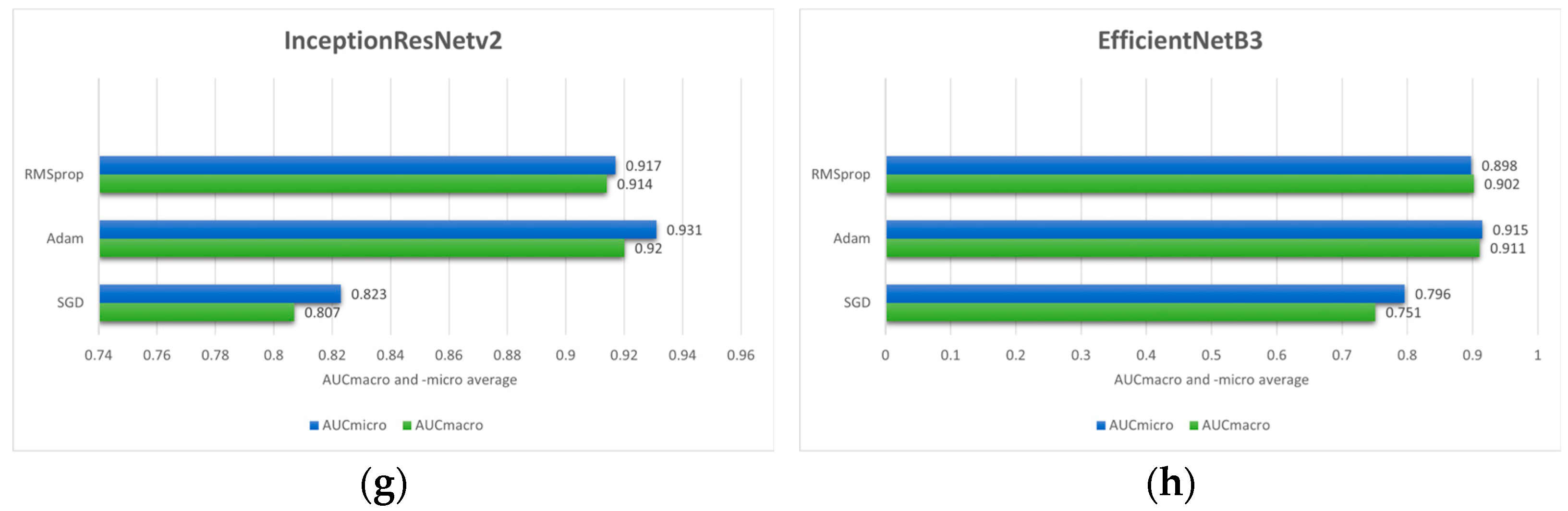
- EfficientNet—In their paper, Tan and Lee (2019) propose a novel scaling method called EfficientNet [28]. To scale up CNNs in a more structured manner, such a method employs a simple yet highly effective compound coefficient. EfficientNets, by significantly improving model efficiency could potentially serve as a new foundation for future computer vision tasks, according to the authors [28].
- InceptionV3—The concept of InceptionV3 was put forth by Szegedy et al. (2016) after InceptionV1 and InceptionV2. Its main goal is to reduce processing power by altering earlier Inception architectures. Several network optimization methods, including factorized convolutions, regularization, dimension reduction, and parallelized calculations, have been proposed in InceptionV3 that loosens the constraints for more straightforward model adaptation [29].
- InceptionResNetV2—InceptionResNetv2, which combines the Inception design with residual connections, was developed by Szegedy et al. (2017) since it has been proven that the Inception architecture produces good results at a comparatively cheap computational cost. The presented architecture significantly increased training speed and enhanced recognition performance [30].
- NASNet—In their research, Zoph et al. (2018) demonstrated a method for directly learning model architectures on the relevant dataset. Since this approach is costly when the dataset is large, they propose utilizing a small dataset to identify an architectural building block that can subsequently be applied to a larger dataset. Designing a new search space that allows for transferability, which researchers refer to as the “NASNet search space” is the main contribution of their work [31].
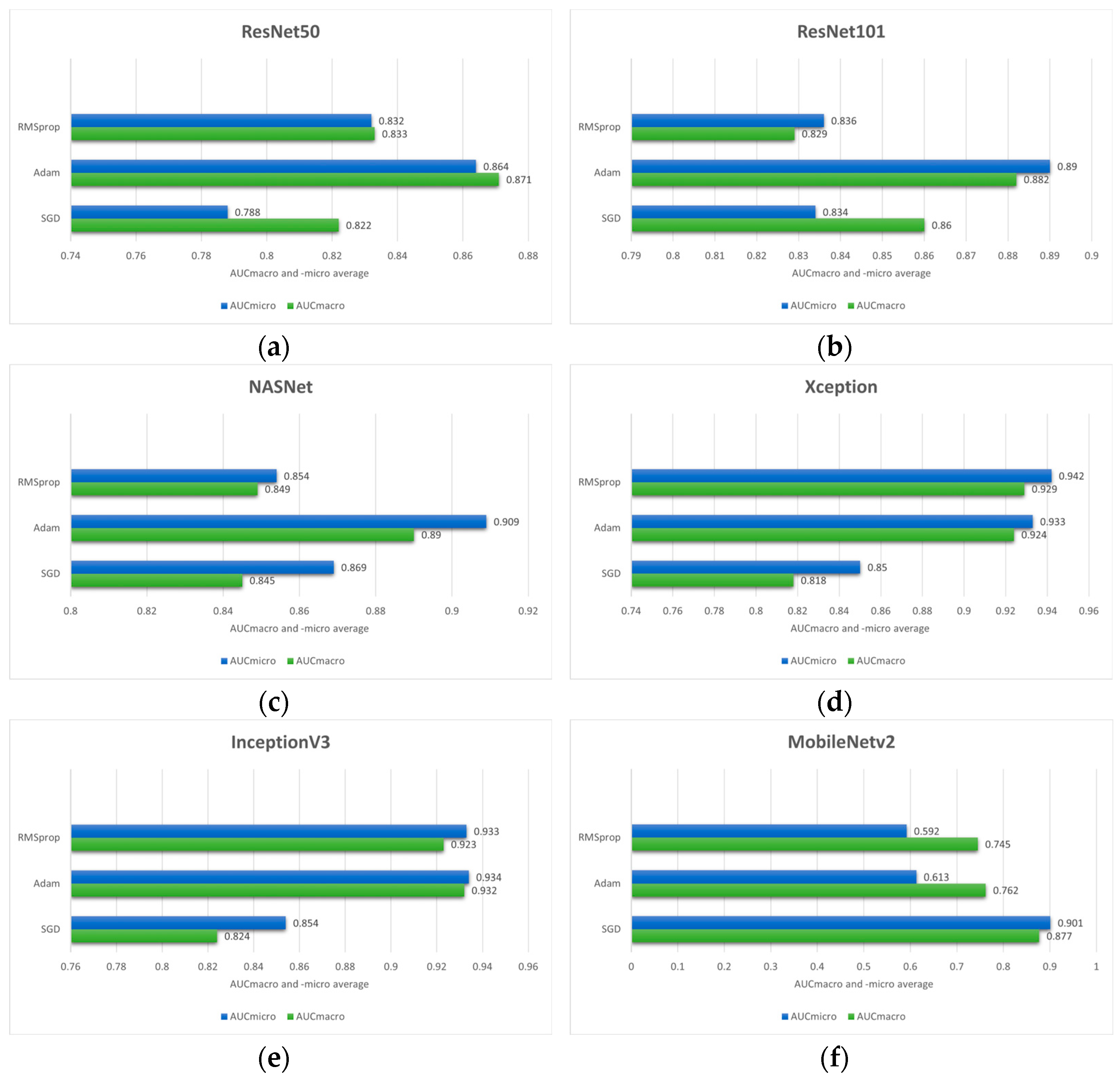
2.4. Evaluation Criteria
- true positive (TP) is when both the predicted and actual values are positive,
- true negative (TN) is when both the actual and predicted values are negative,
- false negative (FN) is when a negative prediction is made but the actual number is positive and,
- false positive (FP) is when a prediction is positive, but the actual value is negative [33].
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| OC | Oral cancer |
| OSCC | Oral squamous cell carcinoma |
| COE | Conventional oral examination |
| DL | Deep Learning |
| Grad-CAM | Gradient-weighted class activation mapping |
| AI | Artificial Intelligence |
| CNN | Convolutional neural network |
| AHA | Artificial hummingbird algorithm |
| XAI | Explainable Artificial Intelligence |
| CV | Computer vision |
| WHO | World Health Organization |
| IHC | Immunohistochemistry |
| AUC | Area Under the Curve |
| KNN | K-nearest neighbors |
References
- Cirillo, N. Precursor lesions, overdiagnosis, and oral cancer: A critical review. Cancers 2024, 16, 1550. [Google Scholar] [CrossRef] [PubMed]
- Torre, L.A.; Siegel, R.L.; Ward, E.M.; Jemal, A. Global cancer incidence and mortality rates and trends—An update. Cancer Epidemiol. Prev. Biomark. 2016, 25, 16–27. [Google Scholar] [CrossRef] [PubMed]
- de França, G.M.; da Silva, W.R.; Medeiros, C.K.S.; Júnior, J.F.; de Moura Santos, E.; Galvão, H.C. Five-year survival and prognostic factors for oropharyngeal squamous cell carcinoma: Retrospective cohort of a cancer center. Oral Maxillofac. Surg. 2022, 26, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Marur, S.; Forastiere, A.A. Head and neck cancer: Changing epidemiology, diagnosis, and treatment. Mayo Clin. Proc. 2008, 83, 489–501. [Google Scholar] [CrossRef] [PubMed]
- Bagan, J.; Sarrion, G.; Jimenez, Y. Oral cancer: Clinical features. Oral Oncol. 2010, 46, 414–417. [Google Scholar] [CrossRef] [PubMed]
- Essat, M.; Cooper, K.; Bessey, A.; Clowes, M.; Chilcott, J.B.; Hunter, K.D. Diagnostic accuracy of conventional oral examination for detecting oral cavity cancer and potentially malignant disorders in patients with clinically evident oral lesions: Systematic review and meta-analysis. Head Neck 2022, 44, 998–1013. [Google Scholar] [CrossRef] [PubMed]
- Warnakulasuriya, S.; Reibel, J.; Bouquot, J.; Dabelsteen, E. Oral epithelial dysplasia classification systems: Predictive value, utility, weaknesses and scope for improvement. J. Oral Pathol. Med. 2008, 37, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Mehlum, C.S.; Larsen, S.R.; Kiss, K.; Groentved, A.M.; Kjaergaard, T.; Möller, S.; Godballe, C. Laryngeal precursor lesions: Interrater and intrarater reliability of histopathological assessment. Laryngoscope 2018, 128, 2375–2379. [Google Scholar] [CrossRef] [PubMed]
- Bruschini, R.; Maffini, F.; Chiesa, F.; Lepanto, D.; De Berardinis, R.; Chu, F.; Tagliabue, M.; Giugliano, G.; Ansarin, M. Oral cancer: Changing the aim of the biopsy in the age of precision medicine. A review. ACTA Otorhinolaryngol. Ital. 2021, 41, 108. [Google Scholar] [CrossRef] [PubMed]
- Litjens, G.; Kooi, T.; Bejnordi, B.E.; Setio, A.A.A.; Ciompi, F.; Ghafoorian, M.; van der Laak, J.A.W.M.; van Ginneken, B.; Sánchez, C.I. A survey on deep learning in medical image analysis. Med. Image Anal. 2017, 42, 60–88. [Google Scholar] [CrossRef] [PubMed]
- Alanazi, A.A.; Khayyat, M.M.; Khayyat, M.M.; Elamin Elnaim, B.M.; Abdel-Khalek, S. Intelligent deep learning enabled oral squamous cell carcinoma detection and classification using biomedical images. Comput. Intell. Neurosci. 2022, 2022, 7643967. [Google Scholar] [CrossRef] [PubMed]
- Musulin, J.; Štifanić, D.; Zulijani, A.; Ćabov, T.; Dekanić, A.; Car, Z. An enhanced histopathology analysis: An ai-based system for multiclass grading of oral squamous cell carcinoma and segmenting of epithelial and stromal tissue. Cancers 2021, 13, 1784. [Google Scholar] [CrossRef] [PubMed]
- Dixit, S.; Kumar, A.; Srinivasan, K. A current review of machine learning and deep learning models in oral cancer diagnosis: Recent technologies, open challenges, and future research directions. Diagnostics 2023, 13, 1353. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Sengupta, S.; Lakshminarayanan, V. Explainable deep learning models in medical image analysis. J. Imaging 2020, 6, 52. [Google Scholar] [CrossRef] [PubMed]
- Chaddad, A.; Peng, J.; Xu, J.; Bouridane, A. Survey of explainable AI techniques in healthcare. Sensors 2023, 23, 634. [Google Scholar] [CrossRef] [PubMed]
- Rahman, A.U.; Alqahtani, A.; Aldhafferi, N.; Nasir, M.U.; Khan, M.F.; Khan, M.A.; Mosavi, A. Histopathologic oral cancer prediction using oral squamous cell carcinoma biopsy empowered with transfer learning. Sensors 2022, 22, 3833. [Google Scholar] [CrossRef] [PubMed]
- Mohan, R.; Rama, A.; Raja, R.K.; Shaik, M.R.; Khan, M.; Shaik, B.; Rajinikanth, V. OralNet: Fused optimal deep features framework for oral squamous cell carcinoma detection. Biomolecules 2023, 13, 1090. [Google Scholar] [CrossRef] [PubMed]
- Das, M.; Dash, R.; Mishra, S.K.; Dalai, A.K. An Ensemble deep learning model for oral squamous cell carcinoma detection using histopathological image analysis. IEEE Access 2024, 12, 127185–127197. [Google Scholar] [CrossRef]
- Suara, S.; Jha, A.; Sinha, P.; Sekh, A.A. Is grad-cam explainable in medical images? In Proceedings of the International Conference on Computer Vision and Image Processing, Jammu, India, 3–5 November 2023; Springer Nature: Cham, Switzerland, 2023; pp. 124–135. [Google Scholar] [CrossRef]
- Oya, K.; Kokomoto, K.; Nozaki, K.; Toyosawa, S. Oral squamous cell carcinoma diagnosis in digitized histological images using convolutional neural network. J. Dent. Sci. 2023, 18, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Afify, H.M.; Mohammed, K.K.; Hassanien, A.E. Novel prediction model on OSCC histopathological images via deep transfer learning combined with Grad-CAM interpretation. Biomed. Signal Process. Control 2023, 83, 104704. [Google Scholar] [CrossRef]
- Da Silva, A.V.B.; Saldivia-Siracusa, C.; de Souza, E.S.C.; Araújo, A.L.D.; Lopes, M.A.; Vargas, P.A.; Kowalski, L.P.; Santos-Silva, A.R.; de Carvalho, A.C.P.L.F.; Quiles, M.G. Enhancing Explainability in Oral Cancer Detection with Grad-CAM Visualizations. In Proceedings of the International Conference on Computational Science and Its Applications, Hanoi, Vietnam, 1–4 July 2024; Springer Nature: Cham, Switzerland, 2024; pp. 151–164. [Google Scholar] [CrossRef]
- El-Naggar, A.K.; Chan, J.K.; Grandis, J.R.; Takata, T.; Slootweg, P.J. (Eds.) WHO Classification of Head and Neck Tumours; International Agency for Research on Cancer (IARC): Lyon, France, 2017. [Google Scholar] [CrossRef]
- Selvaraju, R.R.; Cogswell, M.; Das, A.; Vedantam, R.; Parikh, D.; Batra, D. Grad-CAM: Visual explanations from deep networks via gradient-based localization. Int. J. Comput. Vis. 2020, 128, 336–359. [Google Scholar] [CrossRef]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar] [CrossRef]
- Sandler, M.; Howard, A.; Zhu, M.; Zhmoginov, A.; Chen, L.C. Mobilenetv2: Inverted residuals and linear bottlenecks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018; pp. 4510–4520. [Google Scholar] [CrossRef]
- Chollet, F. Xception: Deep learning with depthwise separable convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 1251–1258. [Google Scholar] [CrossRef]
- Tan, M.; Le, Q. Efficientnet: Rethinking model scaling for convolutional neural networks. In Proceedings of the International Conference on Machine Learning (PMLR), Long Beach, CA, USA, 9–15 June 2019; pp. 6105–6114. [Google Scholar] [CrossRef]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the Inception architecture for computer vision. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016. [Google Scholar] [CrossRef]
- Szegedy, C.; Ioffe, S.; Vanhoucke, V.; Alemi, A.A. Inception-v4, inception-resnet and the impact of residual connections on learning. In Proceedings of the Thirty-First AAAI Conference on Artificial Intelligence, San Francisco, CA, USA, 4–9 February 2017. [Google Scholar] [CrossRef]
- Zoph, B.; Vasudevan, V.; Shlens, J.; Le, Q.V. Learning transferable architectures for scalable image recognition. In Proceedings of the 2018 IEEE/CVF Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018. [Google Scholar] [CrossRef]
- Tharwat, A. Classification assessment methods. Appl. Comput. Inform. 2020, 17, 168–192. [Google Scholar] [CrossRef]
- Leonard, L.C. Web-Based Behavioral Modeling for Continuous User Authentication (CUA). Adv. Comput. 2017, 105, 1–44. [Google Scholar] [CrossRef]
- Prusty, S.; Patnaik, S.; Dash, S.K. SKCV: Stratified K-fold cross-validation on ML classifiers for predicting cervical cancer. Front. Nanotechnol. 2022, 4, 972421. [Google Scholar] [CrossRef]
- Hamm, C.A.; Baumgärtner, G.L.; Biessmann, F.; Beetz, N.L.; Hartenstein, A.; Savic, L.J.; Froböse, K.; Dräger, F.; Schallenberg, S.; Rudolph, M.; et al. Interactive explainable deep learning model informs prostate cancer diagnosis at MRI. Radiology 2023, 307, e222276. [Google Scholar] [CrossRef] [PubMed]
- Brunese, L.; Mercaldo, F.; Reginelli, A.; Santone, A. Explainable deep learning for pulmonary disease and coronavirus COVID-19 detection from X-rays. Comput. Methods Programs Biomed. 2020, 196, 105608. [Google Scholar] [CrossRef] [PubMed]
- Alshazly, H.; Linse, C.; Barth, E.; Martinetz, T. Explainable COVID-19 detection using chest CT scans and deep learning. Sensors 2021, 21, 455. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic of the Patients | n = 40 (100%) | |
|---|---|---|
| Sex | F | 30 |
| M | 70 | |
| Age | To 49 | 5 |
| 50–59 | 13 | |
| 60–69 | 55 | |
| +70 | 27 | |
| Smoking | Y | 55 |
| N | 45 | |
| Alcohol | Y | 38 |
| N | 62 | |
| Lymph Node Metastases | Y | 52 |
| N | 48 | |
| Grading | I | 45 |
| II | 40 | |
| III | 15 |
| Algorithm | AUCmacro ± σ | AUCmicro ± σ |
|---|---|---|
| ResNet50 | 0.871 ± 0.105 | 0.864 ± 0.090 |
| ResNet101 | 0.882 ± 0.125 | 0.890 ± 0.112 |
| NASNet | 0.890 ± 0.054 | 0.909 ± 0.043 |
| Xception | 0.929 ± 0.087 | 0.942 ± 0.074 |
| InceptionV3 | 0.932 ± 0.081 | 0.938 ± 0.088 |
| MobileNetv2 | 0.877 ± 0.062 | 0.900 ± 0.049 |
| InceptionResNetV2 | 0.920 ± 0.059 | 0.931 ± 0.0.064 |
| EfficientNetB3 | 0.911 ± 0.148 | 0.915 ± 0.148 |
| Logistic Regression | 0.509 ± 0.060 | 0.634 ± 0.059 |
| KNN | 0.539 ± 0.052 | 0.658 ± 0.035 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Štifanić, J.; Štifanić, D.; Anđelić, N.; Car, Z. Explainable AI for Oral Cancer Diagnosis: Multiclass Classification of Histopathology Images and Grad-CAM Visualization. Biology 2025, 14, 909. https://doi.org/10.3390/biology14080909
Štifanić J, Štifanić D, Anđelić N, Car Z. Explainable AI for Oral Cancer Diagnosis: Multiclass Classification of Histopathology Images and Grad-CAM Visualization. Biology. 2025; 14(8):909. https://doi.org/10.3390/biology14080909
Chicago/Turabian StyleŠtifanić, Jelena, Daniel Štifanić, Nikola Anđelić, and Zlatan Car. 2025. "Explainable AI for Oral Cancer Diagnosis: Multiclass Classification of Histopathology Images and Grad-CAM Visualization" Biology 14, no. 8: 909. https://doi.org/10.3390/biology14080909
APA StyleŠtifanić, J., Štifanić, D., Anđelić, N., & Car, Z. (2025). Explainable AI for Oral Cancer Diagnosis: Multiclass Classification of Histopathology Images and Grad-CAM Visualization. Biology, 14(8), 909. https://doi.org/10.3390/biology14080909