
Effect of Riociguat on Adenine-Induced Chronic Kidney Disease in Rats

 , , ,
, , ,
Simple Summary
Abstract

1. Introduction
2. Material and Methods
2.1. Chemical Reagents
2.2. Animals
2.3. Experimental Design
2.4. Physiological Measurements
2.5. Biochemical Analysis
2.6. Histopathological Analysis
2.7. Statistical Analysis
3. Results
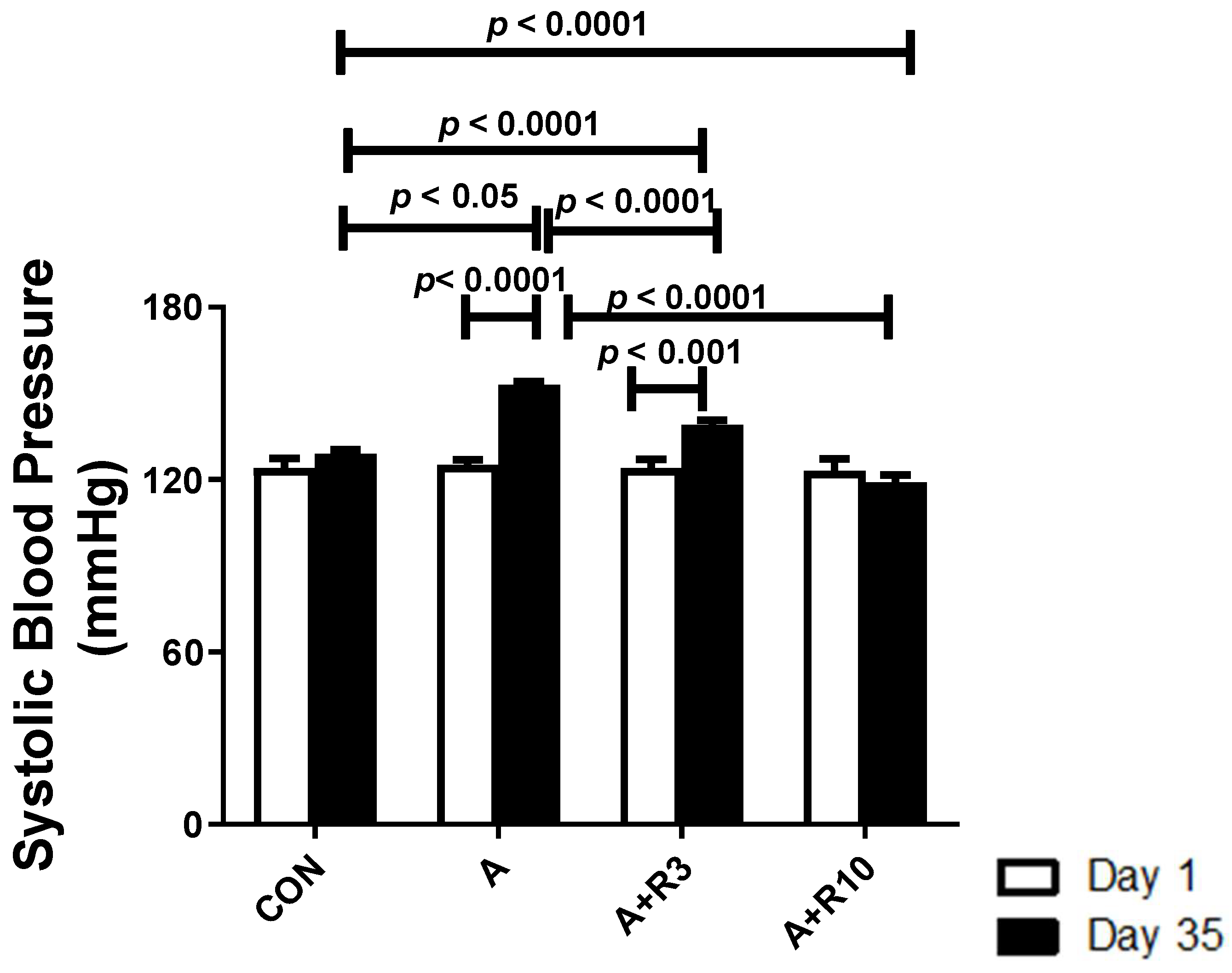
3.1. Physiological Parameters
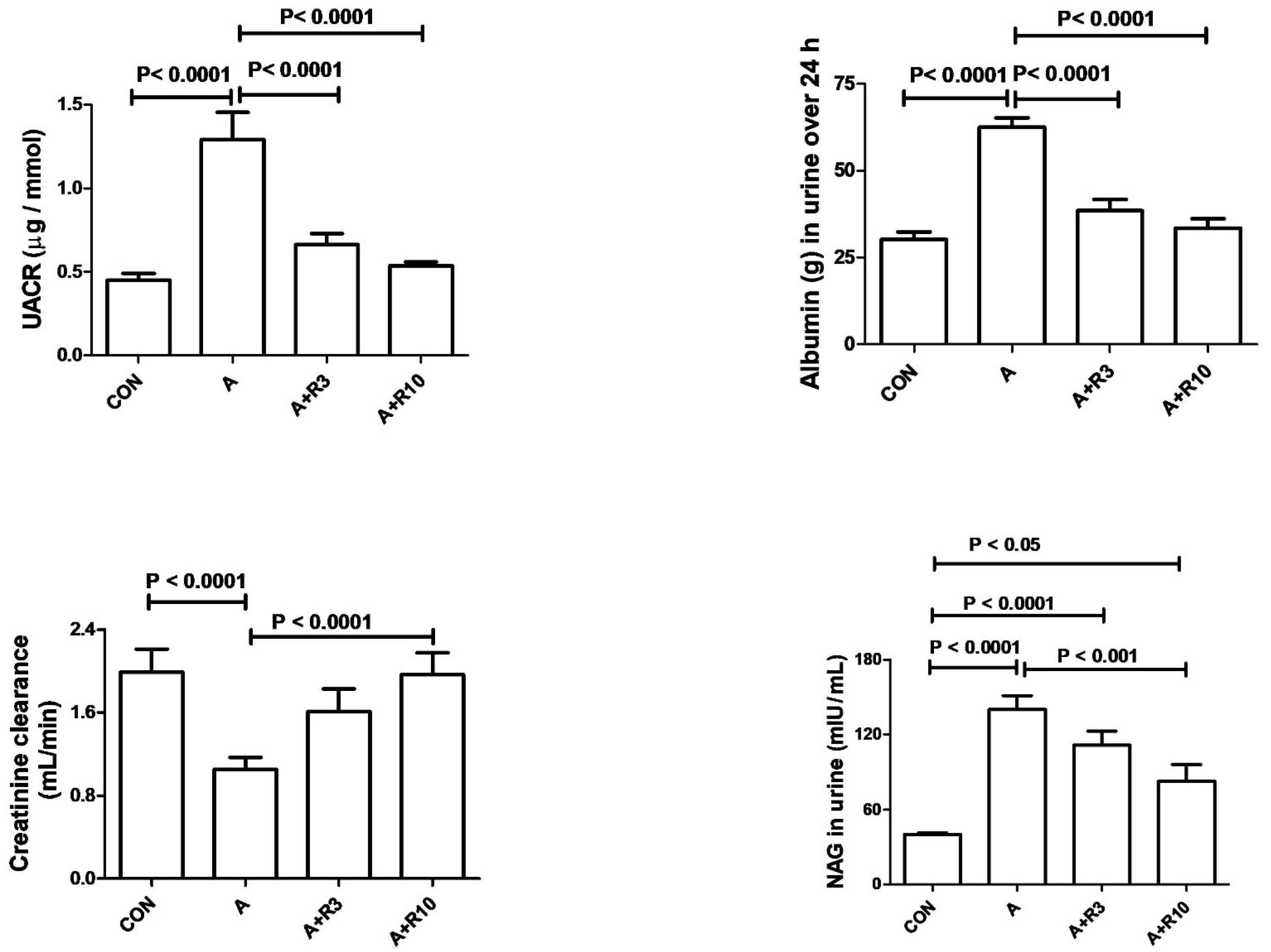
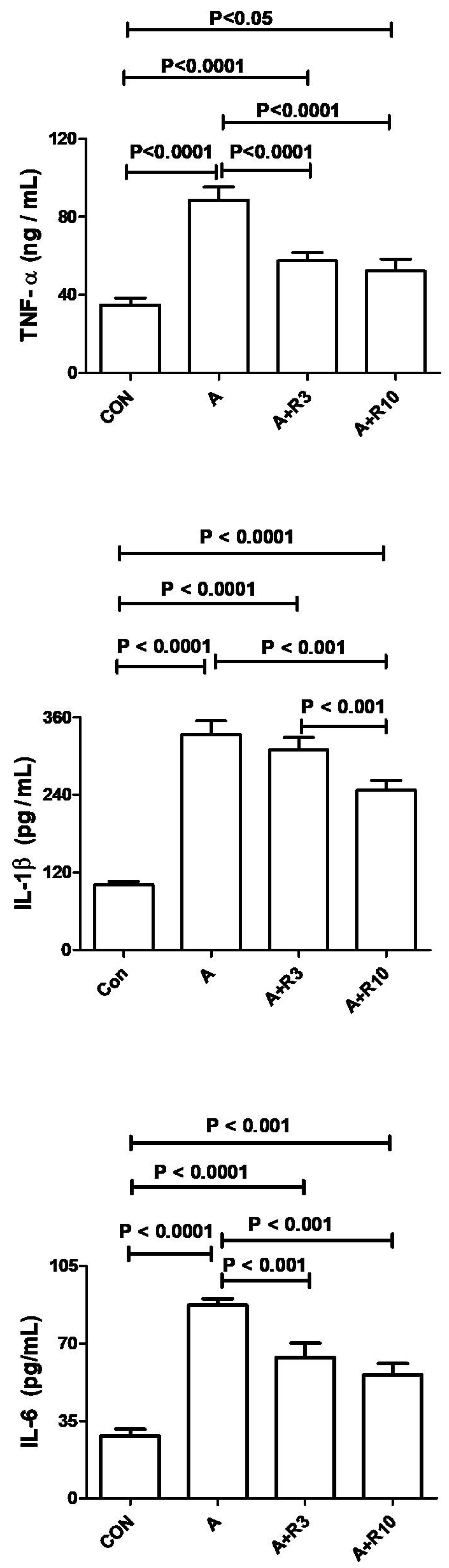
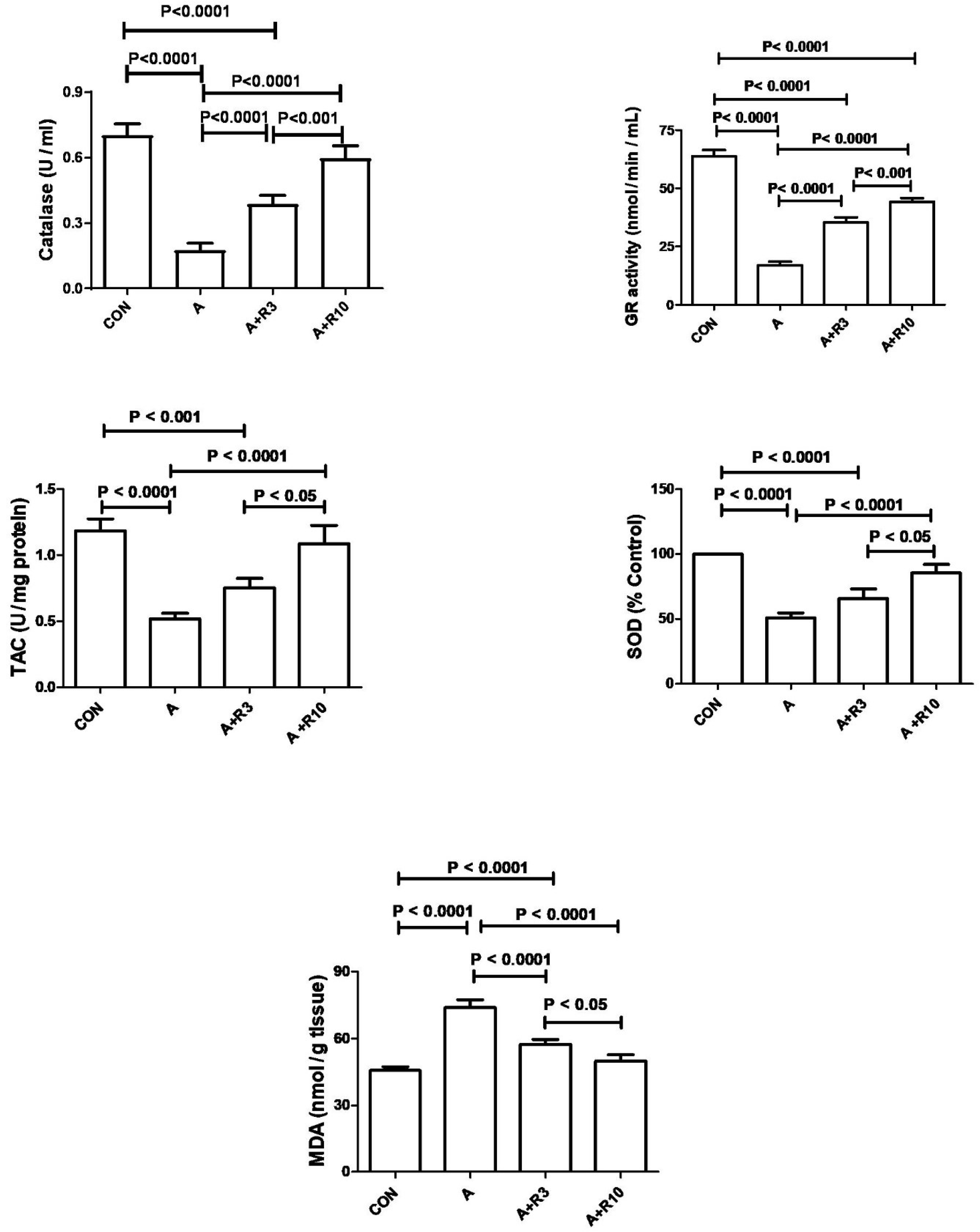
3.2. Kidney Function, Inflammatory Markers, and Oxidative Stress
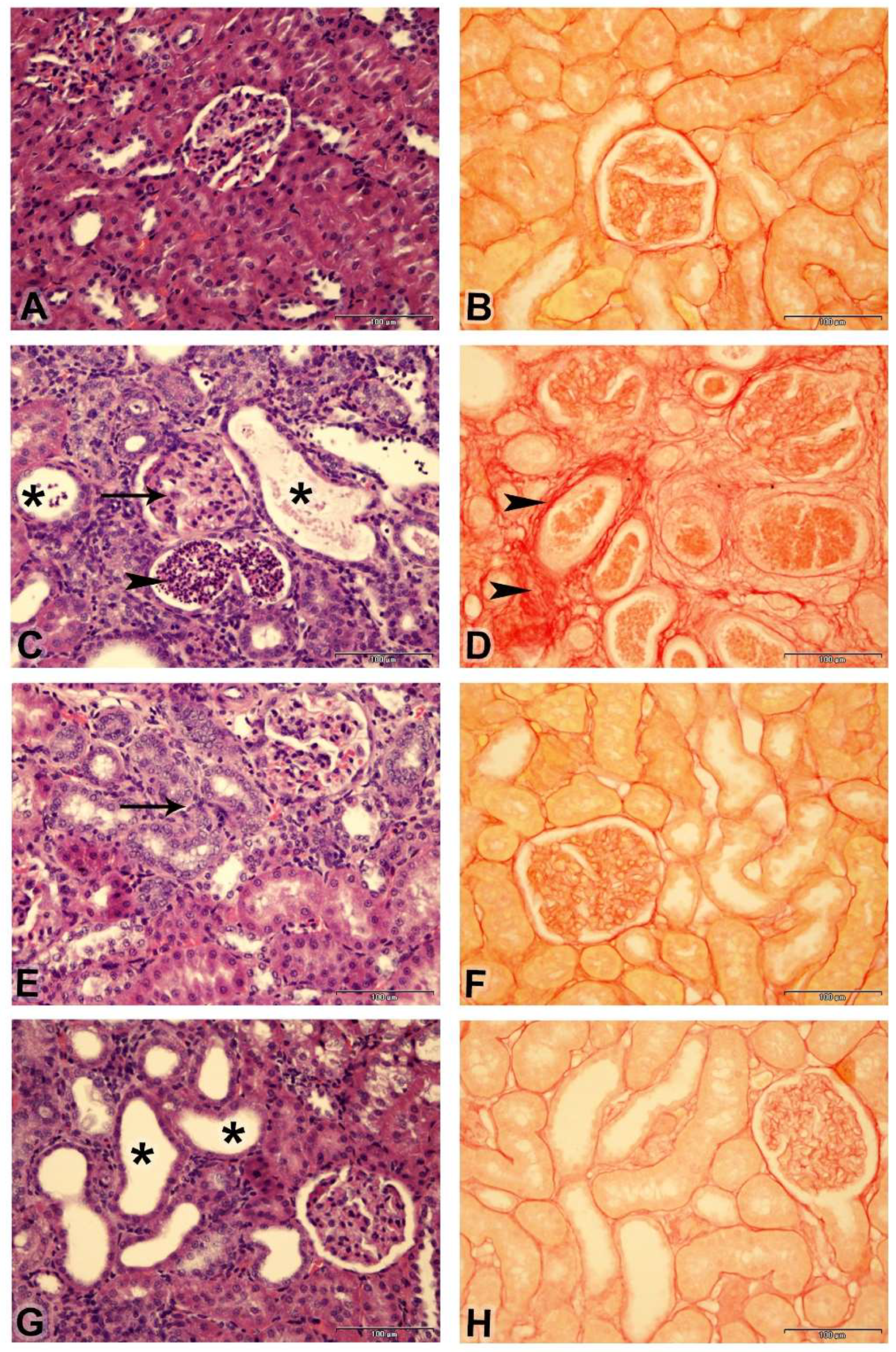
3.3. Histopathology
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rapa, S.F.; Di Iorio, B.R.; Campiglia, P.; Heidland, A.; Marzocco, S. Inflammation and Oxidative Stress in Chronic Kidney Disease-Potential Therapeutic Role of Minerals, Vitamins and Plant-Derived Metabolites. Int. J. Mol. Sci. 2019, 21, 263. [Google Scholar] [CrossRef] [PubMed]
- Annuk, M.; Zilmer, M.; Lind, L.; Linde, T.; Fellstrom, B. Oxidative stress and endothelial function in chronic renal failure. J. Am. Soc. Nephrol. 2001, 12, 2747–2752. [Google Scholar] [CrossRef] [PubMed]
- Naesheim, T.; How, O.J.; Myrmel, T. The effect of riociguat on cardiovascular function and efficiency in healthy, juvenile pigs. Physiol. Rep. 2020, 8, e14562. [Google Scholar] [CrossRef] [PubMed]
- Grześk, G.; Nowaczyk, A. Current modulation of guanylate cyclase pathway activity-mechanism and clinical implications. Molecules 2021, 26, 3418. [Google Scholar] [CrossRef] [PubMed]
- Hohenstein, B.; Daniel, C.; Wagner, A.; Stasch, J.P.; Hugo, C. Stimulation of soluble guanylyl cyclase inhibits mesangial cell proliferation and matrix accumulation in experimental glomerulonephritis. Am. J. Physiol. Renal. Physiol. 2005, 288, F685–F693. [Google Scholar] [CrossRef]
- Krishnan, S.M.; Kraehling, J.R.; Eitner, F.; Bénardeau, A.; Sandner, P. The Impact of the Nitric Oxide (NO)/Soluble Guanylyl Cyclase (sGC) Signaling Cascade on Kidney Health and Disease: A Preclinical Perspective. Int. J. Mol. Sci. 2018, 19, 1712. [Google Scholar] [CrossRef]
- Harloff, M.; Prüschenk, S.; Seifert, R.; Schlossmann, J. Activation of soluble guanylyl cyclase signalling with cinaciguat improves impaired kidney function in diabetic mice. Br. J. Pharmacol. 2022, 179, 2460–2475. [Google Scholar] [CrossRef]
- Benza, R.L.; Grünig, E.; Sandner, P.; Stasch, J.P.; Simonneau, G. The nitric oxide-soluble guanylate cyclase-cGMP pathway in pulmonary hypertension: From PDE5 to soluble guanylate cyclase. Eur. Respir. Rev. 2024, 33, 230183. [Google Scholar] [CrossRef]
- Mittendorf, J.; Weigand, S.; Alonso-Alija, C.; Bischoff, E.; Feurer, A.; Gerisch, M.; Kern, A.; Knorr, A.; Lang, D.; Muenter, K.; et al. Discovery of riociguat (BAY 63-2521): A potent, oral stimulator of soluble guanylate cyclase for the treatment of pulmonary hypertension. Chem. Med. Chem. 2009, 4, 853–865. [Google Scholar] [CrossRef]
- Sravani, S.; Saifi, M.A.; Godugu, C. Riociguat ameliorates kidney injury and fibrosis in an animal model. Biochem. Biophys. Res. Commun. 2020, 530, 706–712. [Google Scholar] [CrossRef]
- Geschka, S.; Kretschmer, A.; Sharkovska, Y.; Evgenov, O.V.; Lawrenz, B.; Hucke, A.; Hocher, B.; Stasch, J.P. Soluble guanylate cyclase stimulation prevents fibrotic tissue remodeling and improves survival in salt-sensitive Dahl rats. PLoS ONE 2011, 6, e21853. [Google Scholar] [CrossRef] [PubMed]
- Sharkovska, Y.; Kalk, P.; Lawrenz, B.; Godes, M.; Hoffmann, L.S.; Wellkisch, K.; Geschka, S.; Relle, K.; Hocher, B.; Stasch, J.P. Nitric oxide-independent stimulation of soluble guanylate cyclase reduces organ damage in experimental low-renin and high-renin models. J. Hypertens. 2010, 28, 1666–1675. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; Su, S.; Luo, N.; Cao, G. Adenine-induced animal model of chronic kidney disease: Current applications and future perspectives. Ren. Fail. 2024, 46, 2336128. [Google Scholar] [CrossRef] [PubMed]
- Yokozawa, T.; Zheng, P.D.; Oura, H.; Koizumi, F. Animal model of adenine-induced chronic renal failure in rats. Nephron. 1986, 44, 230–234. [Google Scholar] [CrossRef]
- Ali, B.H.; Al-Husseni, I.; Beegam, S.; Al-Shukaili, A.; Nemmar, A.; Schierling, S.; Queisser, N.; Schupp, N. Effect of gum arabic on oxidative stress and inflammation in adenine-induced chronic renal failure in rats. PLoS ONE 2013, 8, e55242. [Google Scholar] [CrossRef]
- Ali, B.H.; Al-Za’abi, M.; Ramkumar, A.; Al-Lawati, I.; Waly, M.I.; Beegam, S.; Nemmar, A.; Brand, S.; Schupp, N. The effect of activated charcoal on adenine-induced chronic renal failure in rats. Food Chem. Toxicol. 2014, 65, 321–328. [Google Scholar] [CrossRef]
- Diwan, V.; Brown, L.; Gobe, G. Adenine-induced chronic kidney disease in rats. Nephrology 2018, 23, 5–11. [Google Scholar] [CrossRef]
- Abdelrahman, A.M.; Ali, B.H.; Ali, H.; Manoj, P.; Al-Suleimani, Y. The effect of diminazene, an angiotensin-converting enzyme 2 activator, on adenine-induced chronic kidney disease in rats. Fundam. Clin. Pharmacol. 2023, 37, 235–244. [Google Scholar] [CrossRef]
- Al Suleimani, Y.; Al-Maskari, R.; Ali, B.H.; Ali, H.; Manoj, P.; Al-Khamiyasi, A.; Abdelrahman, A.M. Nephroprtective effects of diminazene on doxorubicin-induced acute kidney injury in rats. Toxicol. Rep. 2023, 11, 460–468. [Google Scholar] [CrossRef]
- Kovesdy, C.P. Epidemiology of chronic kidney disease: An update 2022. Kidney Int. Suppl. 2022, 12, 7–11. [Google Scholar] [CrossRef]
- Bénardeau, A.; Kahnert, A.; Schomber, T.; Meyer, J.; Pavkovic, M.; Kretschmer, A.; Lawrenz, B.; Hartmann, E.; Mathar, I.; Hueser, J.; et al. Runcaciguat, a novel soluble guanylate cyclase activator, shows renoprotection in hypertensive, diabetic, and metabolic preclinical models of chronic kidney disease. Naunyn Schmiedebergs Arch. Pharmacol. 2021, 394, 2363–2379. [Google Scholar] [CrossRef] [PubMed]
- Sandner, P.; Zimmer, D.P.; Milne, G.T.; Follmann, M.; Hobbs, A.; Stasch, J.P. Soluble guanylate cyclase stimulators and activators. Handb. Exp. Pharmacol. 2021, 264, 355–394. [Google Scholar] [PubMed]
- Ali, B.H.; Al Salam, S.; Al-Suleimani, Y.; Al-Za’abi, M.; Abdelrahman, A.M.; Ashique, M.; Manoj, P.; Adham, S.A.; Hartmann, C.; Schupp, N.; et al. Effects of the SGLT-2 inhibitor canagliflozin on adenine-induced chronic kidney disease in rats. Cell Physiol. Biochem. 2019, 52, 27–39. [Google Scholar] [PubMed]
- Abdelrahman, A.M.; Al-Suleimani, Y.; Al-Za’abi, M.; Ashique, M.; Manoj, P.; Hartmann, C.; Nemmar, A.; Schupp, N.; Ali, B.H. The renoprotective effect of the dipeptidyl peptidase-4 inhibitor sitagliptin on adenine-induced kidney disease in rats. Biomed. Pharmacother. 2019, 110, 667–676. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.N.; Hou, C.Y.; Chang-Chien, G.P.; Lin, S.; Yang, H.W.; Tain, Y.L. Sodium Thiosulfate improves hypertension in rats with adenine-induced chronic kidney disease. Antioxidants 2022, 11, 147. [Google Scholar] [CrossRef]
- Tain, Y.L.; Yang, H.W.; Hou, C.Y.; Chang-Chien, G.P.; Lin, S.; Hsu, C.N. Anti-hypertensive property of an NO nanoparticle in an adenine-induced chronic kidney disease young rat model. Antioxidants 2023, 12, 513. [Google Scholar] [CrossRef]
- Follmann, M.; Ackerstaff, J.; Redlich, G.; Wunder, F.; Lang, D.; Kern, A.; Fey, P.; Griebenow, N.; Kroh, W.; Becker-Pelster, E.M.; et al. Discovery of the soluble guanylate cyclase stimulator Vericiguat (BAY 1021189) for the treatment of chronic heart failure. J. Med. Chem. 2017, 60, 5146–5161. [Google Scholar] [CrossRef]
- Ohata, K.; Kamijo-Ikemori, A.; Sugaya, T.; Hibi, C.; Nakamura, T.; Murase, T.; Oikawa, T.; Hoshino, S.; Katayama, K.; Asano, J.; et al. Renoprotective effect of the xanthine oxidoreductase inhibitor topiroxostat under decreased angiotensin II type 1a receptor expression. Eur. J. Pharmacol. 2017, 815, 88–97. [Google Scholar] [CrossRef]
- Stehle, D.; Xu, M.Z.; Schomber, T.; Hahn, M.G.; Schweda, F.; Feil, S.; Kraehling, J.R.; Eitner, F.; Patzak, A.; Sandner, P.; et al. Novel soluble guanylyl cyclase activators increase glomerular cGMP, induce vasodilation and improve blood flow in the murine kidney. Br. J. Pharmacol. 2022, 179, 2476–2489. [Google Scholar] [CrossRef]
- Novak, R.; Salai, G.; Hrkac, S.; Vojtusek, I.K.; Grgurevic, L. Revisiting the role of NAG across the continuum of kidney disease. Bioengineering 2023, 10, 444. [Google Scholar] [CrossRef]
- Ott, I.M.; Alter, M.L.; von Websky, K.; Kretschmer, A.; Tsuprykov, O.; Sharkovska, Y.; Krause-Relle, K.; Raila, J.; Henze, A.; Stasch, J.P.; et al. Effects of stimulation of soluble guanylate cyclase on diabetic nephropathy in diabetic eNOS knockout mice on top of angiotensin II receptor blockade. PLoS ONE 2012, 7, e42623. [Google Scholar] [CrossRef] [PubMed]
- Stasch, J.P.; Schlossmann, J.; Hocher, B. Renal effects of soluble guanylate cyclase stimulators and activators: A review of the preclinical evidence. Curr. Opin. Pharmacol. 2015, 21, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Tchernychev, B.; Li, H.; Lee, S.K.; Gao, X.; Ramanarasimhaiah, R.; Liu, G.; Hall, K.C.; Bernier, S.G.; Jones, J.E.; Feil, S.; et al. Olinciguat, a stimulator of soluble guanylyl cyclase, attenuates inflammation, vaso-occlusion and nephropathy in mouse models of sickle cell disease. Br. J. Pharmacol. 2021, 178, 3463–3475. [Google Scholar] [CrossRef] [PubMed]
- Czirok, S.; Fang, L.; Radovits, T.; Szabó, G.; Szénási, G.; Rosivall, L.; Merkely, B.; Kökény, G. Cinaciguat ameliorates glomerular damage by reducing ERK1/2 activity and TGF-ß expression in type-1 diabetic rats. Sci. Rep. 2017, 7, 11218. [Google Scholar] [CrossRef]
- Heerspink, H.J.L.; Cherney, D.; Gafor, A.H.A.; Górriz, J.L.; Pergola, P.E.; Tang, S.C.W.; Desch, M.; Iliev, H.; Sun, Z.; Steubl, D.; et al. Effect of avenciguat on albuminuria in patients with CKD: Two randomized placebo-controlled trials. J. Am. Soc. Nephrol. 2024, 35, 1227–1239. [Google Scholar] [CrossRef]
- Gansevoort, R.T.; Wheeler, D.C.; Debén, F.M.; Speeckaert, M.; Thomas, D.; Berger, M.; Klein, S.; Friedrichs, F.; Paraschin, K.; Schmieder, R.E. The soluble guanylate cyclase activator runcaciguat significantly improves albuminuria in patients with chronic kidney disease: A randomized placebo-controlled clinical trial. Nephrol. Dial. Transpl. 2024, gfae261. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters/Treatment | Control | A | A + R3 | A + R10 |
|---|---|---|---|---|
| Baseline body weight (g) | 350 ± 15.19 | 350 ± 14.26 | 350 ± 16.57 | 350 ± 17.40 |
| Final body weight (g) | 369.7 ± 16.4 | 346.2 ± 14.7 | 360 ± 19.2 | 361.8 ± 16.3 |
| Body weight change (%) | 5.55 ± 0.81 | −0.98 ± 0.42 a | 2.68 ± 1.22 b | 3.43 ± 0.81 b |
| Total kidney weight (g) | 1.81 ± 0.08 | 2.58 ± 0.17 a | 2.18 ± 0.2 | 2.03 ± 0.09 |
| Relative kidney weight (%) | 0.49 ± 0.01 | 0.75 ± 0.06 a | 0.60 ± 0.03 | 0.57 ± 0.04 b |
| Water intake (mL/24 h) | 20.2 ± 1.96 | 39.2 ± 1.74 a | 26.5 ± 0.85 b | 22.3 ± 1.8 b |
| Urine output (mL/24 h) | 10.3 ± 0.96 | 31.2 ± 1.22 a | 19.0 ± 1.15 a,b | 17.7 ± 1.58 a,b |
| Parameters/Treatment | Control | A | A + R3 | A + R10 |
|---|---|---|---|---|
| Urea (mmol/L) | 4.33 ± 0.21 | 11.00 ± 0.60 a | 7.09 ± 0.53 a,b | 5.21 ± 0.19 b |
| Creatinine (μmol/L) | 24.4 ± 0.98 | 34.3 ± 1.38 a | 26.5 ± 1.21 b | 22.4 ± 0.37 b |
| Uric acid (μmol/L) | 32.4 ± 1.17 | 71.8 ± 5.75 a | 60.5 ± 3.5 a,b | 46.8 ± 1.54 a,b |
| NGAL (ng/mL) | 34.32 ± 3.26 | 83.73 ± 5.18 a | 60.4 ± 5.04 a,b | 54.1 ± 4.8 a,b |
| Groups/Finding | Lesion Score (Tubular Necrosis) | Fibrosis Index % |
|---|---|---|
| Control | 0 | 5.2 |
| Adenine | 4 | 27.07 |
| Adenine + R3 | 2 | 14.16 |
| Adenine + R10 | 3 | 15.77 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdelrahman, A.M.; Al Maskari, R.; Ali, H.; Manoj, P.; Al Suleimani, Y. Effect of Riociguat on Adenine-Induced Chronic Kidney Disease in Rats. Biology 2025, 14, 161. https://doi.org/10.3390/biology14020161
Abdelrahman AM, Al Maskari R, Ali H, Manoj P, Al Suleimani Y. Effect of Riociguat on Adenine-Induced Chronic Kidney Disease in Rats. Biology. 2025; 14(2):161. https://doi.org/10.3390/biology14020161
Chicago/Turabian StyleAbdelrahman, Aly M., Raya Al Maskari, Haytham Ali, Priyadarsini Manoj, and Yousuf Al Suleimani. 2025. "Effect of Riociguat on Adenine-Induced Chronic Kidney Disease in Rats" Biology 14, no. 2: 161. https://doi.org/10.3390/biology14020161
APA StyleAbdelrahman, A. M., Al Maskari, R., Ali, H., Manoj, P., & Al Suleimani, Y. (2025). Effect of Riociguat on Adenine-Induced Chronic Kidney Disease in Rats. Biology, 14(2), 161. https://doi.org/10.3390/biology14020161