
A Systematic Review of Traumatic Brain Injury in Modern Rodent Models: Current Status and Future Prospects

 , , , and
, , , and
Abstract
Simple Summary
Abstract
1. Introduction
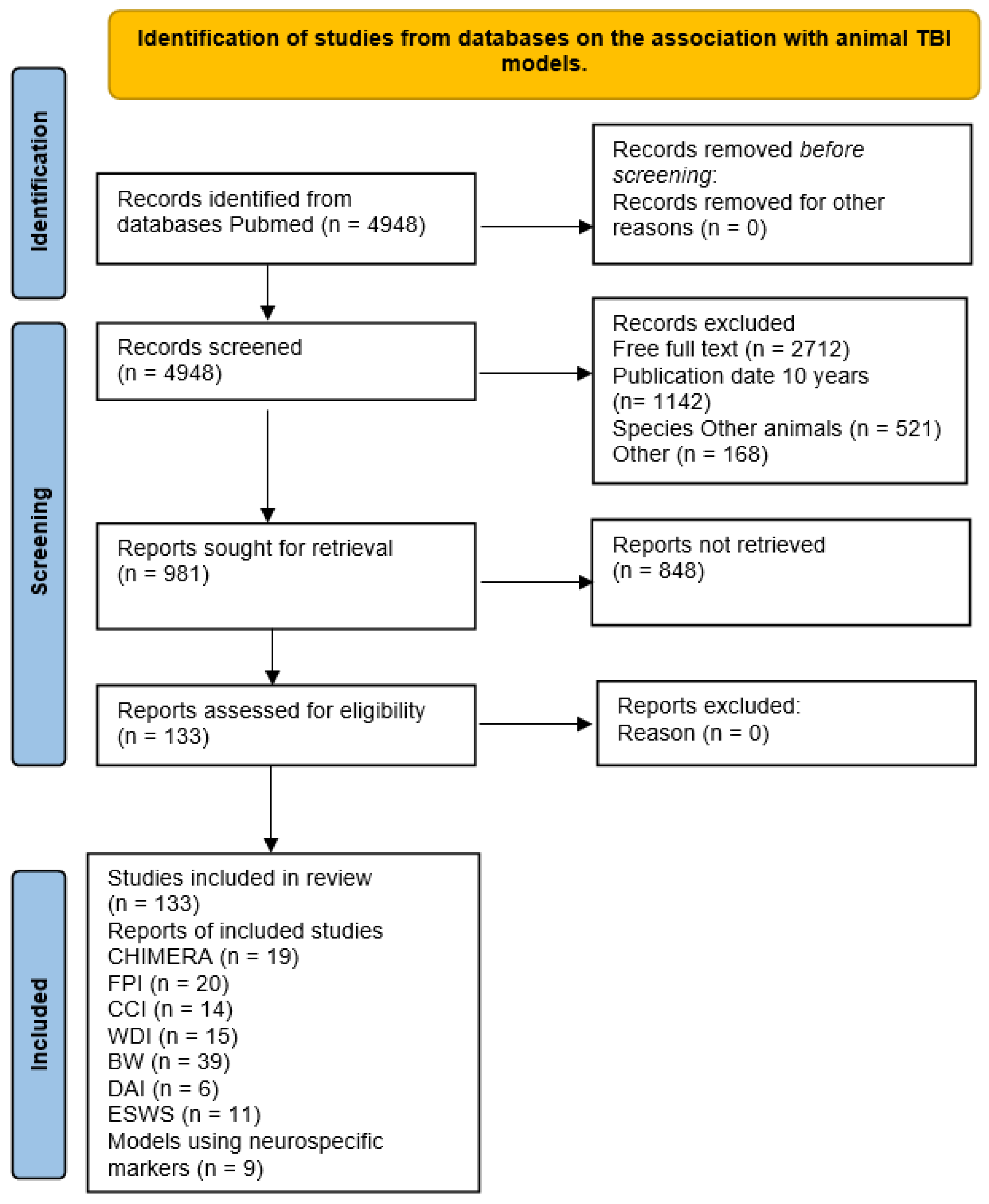
2. Materials and Methods
2.1. Search Criteria
2.2. Inclusion/Exclusion Criteria
2.3. Retrieval of Information from Full-Text Articles
3. Results
3.1. TBI Pathogenesis
3.2. Basic Requirements for an Experimental Model
3.3. TBI Models
3.4. Fluid Percussion Brain Injury (FPI) Model
3.5. Controlled Cortical Injury Model
3.6. Weight Drop Injury (WDI) Model of TBI
3.7. Diffuse Axonal Injury (DAI) Model of TBI
3.8. Blast Wave (BW) Model of TBI
3.9. Closed-Head Impact Model of Engineered Rotational Acceleration (CHIMERA) Model
3.10. Extracorporeal Shock Wave (ESW) Model
3.11. Blood Biomarkers in Animal TBI Models
4. Future Prospects for TBI Modeling
4.1. Modeling TBI in Aged Laboratory Animals
- The mean lifespan of rats and mice in studies ranged from 24 to 30 months. Thus, extrapolating human age as a fraction of the total lifespan, a 20-month-old mouse or rat is equivalent to a 50–60-year-old human. The use of animals in the “old” age will allow covering the heterogeneity of the geriatric population, which is a specialized branch of gerontology devoted to the examination, prevention, and treatment of diseases of the elderly population.
- Modeling TBI should replicate the special mechanical properties typical of injuries in older adults. This should include studies that emulate concussion and mild to moderate TBI, which are the most common forms of clinical injury.
- Modeling TBI in combination with comorbidities frequently seen in older adults (e.g., hypertension, diabetes, cardiovascular disease). These comorbidities may be present in inbred and transgenic animals or induced in the laboratory settings (e.g., obesity, inactivity). Modeling of multiple comorbidities should also be considered.
- Modeling TBI in combination with medications commonly prescribed to older adults (e.g., preinjury antiplatelet therapy).
- Development of more accurate age-specific measures of functional outcomes in aged animals.
- Response to TBI should be assessed from acute to chronic post-TBI period.
- Use of biomarkers as outcome indicators in aged animals: measurements to confirm cerebrovascular reactivity and brain metabolism (magnetic resonance spectroscopy).
- Inclusion of both sexes in aged animal studies of TBI (rather than predominant use of males).
- Larger animal models of TBI should also be considered, including animals with gyrencephalic brains, such as sheep, pigs, and primates.
4.2. The Problem of Modeling TBI in Laboratory Animals
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Parfenov, V.A. [E.I. Gusev, A.N. Konovalova, V.I. Skvortsova “Neurology and neurosurgery”. Textbook, 4th Ed]. Zhurnal Nevrol. I Psikhiatrii Im. SS Korsakova 2015, 115, 130–131. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, C.M.; Titus, D.J.; Wilson, N.M.; Freund, J.E.; Atkins, C.M. Early Life Stress Exacerbates Outcome after Traumatic Brain Injury. J. Neurotrauma 2021, 38, 555–565. [Google Scholar] [CrossRef]
- Cognitive Outcome 1 Year after Mild Traumatic Brain Injury: Results from the TRACK-TBI Study-PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/35173018/ (accessed on 25 July 2024).
- Klinicheskoe Rukovodstvo Po Cherepno-Mozgovoĭ Travme-NLM Catalog-NCBI. Available online: https://www.ncbi.nlm.nih.gov/nlmcatalog/100893725 (accessed on 23 July 2024).
- Peterson, A.B. Deaths from Fall-Related Traumatic Brain Injury—United States, 2008–2017. MMWR Morb. Mortal Wkly. Rep. 2020, 69, 225–230. [Google Scholar] [CrossRef]
- Yang, L.-Y.; Greig, N.H.; Tweedie, D.; Jung, Y.J.; Chiang, Y.-H.; Hoffer, B.J.; Miller, J.P.; Chang, K.-H.; Wang, J.-Y. The P53 Inactivators Pifithrin-μ and Pifithrin-α Mitigate TBI-Induced Neuronal Damage through Regulation of Oxidative Stress, Neuroinflammation, Autophagy and Mitophagy. Exp. Neurol. 2020, 324, 113135. [Google Scholar] [CrossRef]
- Covington, N.V.; Duff, M.C. Heterogeneity Is a Hallmark of Traumatic Brain Injury, Not a Limitation: A New Perspective on Study Design in Rehabilitation Research. Am. J. Speech Lang. Pathol. 2021, 30, 974–985. [Google Scholar] [CrossRef]
- Likhterman, L.B. Classification of Traumatic Brain Injury• Part II. Modern Principles of Classification of CCT. Zhurnal Sud. Meditsiny 2015, 1, 37–48. [Google Scholar]
- Silver, J.M.; McAllister, T.W.; Arciniegas, D.B. Textbook of Traumatic Brain Injury; American Psychiatric Pub: Washington, DC, USA, 2018; ISBN 978-1-61537-247-8. [Google Scholar]
- Lihterman, L.B.; Potapov, A.A.; Klevno, V.A.; Kravchuk, A.D.; Ohlopkov, V.A. Aftereffects of Head Injury. Russ. J. Forensic Med. 2016, 2, 4–20. [Google Scholar] [CrossRef]
- Domínguez-Oliva, A.; Hernández-Ávalos, I.; Martínez-Burnes, J.; Olmos-Hernández, A.; Verduzco-Mendoza, A.; Mota-Rojas, D. The Importance of Animal Models in Biomedical Research: Current Insights and Applications. Animals 2023, 13, 1223. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.J.; Fesharaki-Zadeh, A.; Takahashi, H.; Nies, S.H.; Smith, L.M.; Luo, A.; Chyung, A.; Chiasseu, M.; Strittmatter, S.M. Fyn Kinase Inhibition Reduces Protein Aggregation, Increases Synapse Density and Improves Memory in Transgenic and Traumatic Tauopathy. Acta Neuropathol. Commun. 2020, 8, 96. [Google Scholar] [CrossRef]
- Xiong, Y.; Mahmood, A.; Chopp, M. Animal Models of Traumatic Brain Injury. Nat. Rev. Neurosci. 2013, 14, 128–142. [Google Scholar] [CrossRef]
- Galgano, M.; Toshkezi, G.; Qiu, X.; Russell, T.; Chin, L.; Zhao, L.-R. Traumatic Brain Injury: Current Treatment Strategies and Future Endeavors. Cell Transpl. 2017, 26, 1118–1130. [Google Scholar] [CrossRef] [PubMed]
- Martin, G. Traumatic Brain Injury: The First 15 Milliseconds. Brain Inj. 2016, 30, 1517–1524. [Google Scholar] [CrossRef] [PubMed]
- [PDF] Reduced Mortality Rate in Patients with Severe Traumatic Brain Injury Treated with Brain Tissue Oxygen Monitoring.|Semantic Scholar. Available online: https://www.semanticscholar.org/paper/Reduced-mortality-rate-in-patients-with-severe-with-Stiefel-Spiotta/2ad355337c2d4b55d68586537b782d06af147a33 (accessed on 25 July 2024).
- Werner, C.; Engelhard, K. Pathophysiology of Traumatic Brain Injury. Br. J. Anaesth. 2007, 99, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Iverson, G.L. Outcome from Mild Traumatic Brain Injury. Curr. Opin. Psychiatry 2005, 18, 301–317. [Google Scholar] [CrossRef] [PubMed]
- Loane, D.J.; Pocivavsek, A.; Moussa, C.E.-H.; Thompson, R.; Matsuoka, Y.; Faden, A.I.; Rebeck, G.W.; Burns, M.P. Amyloid Precursor Protein Secretases as Therapeutic Targets for Traumatic Brain Injury. Nat. Med. 2009, 15, 377–379. [Google Scholar] [CrossRef]
- Monoubiquitination and Cellular Distribution of XIAP in Neurons after Traumatic Brain Injury|Semantic Scholar. Available online: https://www.semanticscholar.org/paper/Monoubiquitination-and-Cellular-Distribution-of-in-Lotocki-Alonso/1798ec9c891caccf4d363ff276a97608dcb7bef9 (accessed on 25 July 2024).
- Yao, X.; Liu, J.; McCabe, J.T. Ubiquitin and Ubiquitin-Conjugated Protein Expression in the Rat Cerebral Cortex and Hippocampus Following Traumatic Brain Injury (TBI). Brain Res. 2007, 1182, 116–122. [Google Scholar] [CrossRef]
- Traumatic Brain Injury and Mitochondrial Dysfunction—The American Journal of the Medical Sciences. Available online: https://www.amjmedsci.org/article/S0002-9629(15)41244-3/abstract (accessed on 26 July 2024).
- Bauman, R.A.; Ling, G.; Tong, L.; Januszkiewicz, A.; Agoston, D.; Delanerolle, N.; Kim, Y.; Ritzel, D.; Bell, R.; Ecklund, J.; et al. An Introductory Characterization of a Combat-Casualty-Care Relevant Swine Model of Closed Head Injury Resulting from Exposure to Explosive Blast. J. Neurotrauma 2009, 26, 841–860. [Google Scholar] [CrossRef] [PubMed]
- Boone, D.R.; Sell, S.L.; Micci, M.-A.; Crookshanks, J.M.; Parsley, M.; Uchida, T.; Prough, D.S.; DeWitt, D.S.; Hellmich, H.L. Traumatic Brain Injury-Induced Dysregulation of the Circadian Clock. PLoS ONE 2012, 7, e46204. [Google Scholar] [CrossRef]
- Freire, M.A.M.; Rocha, G.S.; Bittencourt, L.O.; Falcao, D.; Lima, R.R.; Cavalcanti, J.R.L.P. Cellular and Molecular Pathophysiology of Traumatic Brain Injury: What Have We Learned So Far? Biology 2023, 12, 1139. [Google Scholar] [CrossRef]
- Mannix, R.; Berglass, J.; Berkner, J.; Moleus, P.; Qiu, J.; Andrews, N.; Gunner, G.; Berglass, L.; Jantzie, L.L.; Robinson, S.; et al. Chronic Gliosis and Behavioral Deficits in Mice Following Repetitive Mild Traumatic Brain Injury. J. Neurosurg. 2014, 121, 1342–1350. [Google Scholar] [CrossRef]
- Tucker, L.B.; Fu, A.H.; McCabe, J.T. Performance of Male and Female C57BL/6J Mice on Motor and Cognitive Tasks Commonly Used in Pre-Clinical Traumatic Brain Injury Research. J. Neurotrauma 2016, 33, 880–894. [Google Scholar] [CrossRef] [PubMed]
- Single Cell Molecular Alterations Reveal Target Cells and Pathways of Concussive Brain Injury-PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/30254269/ (accessed on 25 July 2024).
- Traumatic Brain Injury Induces Genome-Wide Transcriptomic, Methylomic, and Network Perturbations in Brain and Blood Predicting Neurological Disorders-ScienceDirect. Available online: https://www.sciencedirect.com/science/article/pii/S2352396417300506 (accessed on 25 July 2024).
- Benson, J.C.; Madhavan, A.A.; Cutsforth-Gregory, J.K.; Johnson, D.R.; Carr, C.M. The Monro-Kellie Doctrine: A Review and Call for Revision. Am. J. Neuroradiol. 2022, 44, 2–6. [Google Scholar] [CrossRef]
- Sorby-Adams, A.J.; Vink, R.; Turner, R.J. Large Animal Models of Stroke and Traumatic Brain Injury as Translational Tools. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2018, 315, R165–R190. [Google Scholar] [CrossRef] [PubMed]
- Vink, R. Large Animal Models of Traumatic Brain Injury. J. Neurosci. Res. 2018, 96, 527–535. [Google Scholar] [CrossRef] [PubMed]
- Dai, J.-X.; Ma, Y.-B.; Le, N.-Y.; Cao, J.; Wang, Y. Large Animal Models of Traumatic Brain Injury. Int. J. Neurosci. 2018, 128, 243–254. [Google Scholar] [CrossRef] [PubMed]
- RU2641569C1. Method for Severe Craniocerebral Injury Simulation-Google Patents. Available online: https://patents.google.com/patent/RU2641569C1/en (accessed on 25 July 2024).
- Radkov, I.V.; Laptev, V.V.; Plekhova, N.G. Technologies of Modeling the Diffuse Traumatic Brain Injury. Sovremen. Probl. Nauk. Obraz. 2018, 4, 148. [Google Scholar]
- Eakin, K.; Rowe, R.K.; Lifshitz, J. Modeling Fluid Percussion Injury: Relevance to Human Traumatic Brain Injury. In Brain Neurotrauma: Molecular, Neuropsychological, and Rehabilitation Aspects; Kobeissy, F.H., Ed.; Frontiers in Neuroengineering; CRC Press/Taylor & Francis: Boca Raton, FL, USA, 2015; ISBN 978-1-4665-6598-2. [Google Scholar]
- Hayes, R.L.; Stalhammar, D.; Povlishock, J.T.; Allen, A.M.; Galinat, B.J.; Becker, D.P.; Stonnington, H.H. A New Model of Concussive Brain Injury in the Cat Produced by Extradural Fluid Volume Loading: II. Physiological and Neuropathological Observations. Brain Inj. 1987, 1, 93–112. [Google Scholar] [CrossRef]
- de Lanerolle, N.C.; Bandak, F.; Kang, D.; Li, A.Y.; Du, F.; Swauger, P.; Parks, S.; Ling, G.; Kim, J.H. Characteristics of an Explosive Blast-Induced Brain Injury in an Experimental Model. J. Neuropathol. Exp. Neurol. 2011, 70, 1046–1057. [Google Scholar] [CrossRef]
- Marmarou, A.; Shima, K. Comparative Studies of Edema Produced by Fluid Percussion Injury with Lateral and Central Modes of Injury in Cats. Adv. Neurol. 1990, 52, 233–236. [Google Scholar]
- Millen, J.E.; Glauser, F.L.; Fairman, R.P. A Comparison of Physiological Responses to Percussive Brain Trauma in Dogs and Sheep. J. Neurosurg. 1985, 62, 587–591. [Google Scholar] [CrossRef]
- Mechanisms of Blast Induced Brain Injuries, Experimental Studies in Rats—ScienceDirect. Available online: https://www.sciencedirect.com/science/article/abs/pii/S1053811910007639 (accessed on 26 July 2024).
- Säljö, A.; Bao, F.; Haglid, K.G.; Hansson, H.A. Blast Exposure Causes Redistribution of Phosphorylated Neurofilament Subunits in Neurons of the Adult Rat Brain. J. Neurotrauma 2000, 17, 719–726. [Google Scholar] [CrossRef] [PubMed]
- Shah, E.J.; Gurdziel, K.; Ruden, D.M. Mammalian Models of Traumatic Brain Injury and a Place for Drosophila in TBI Research. Front. Neurosci. 2019, 13, 409. [Google Scholar] [CrossRef] [PubMed]
- Thibault, L.E.; Meaney, D.F.; Anderson, B.J.; Marmarou, A. Biomechanical Aspects of a Fluid Percussion Model of Brain Injury. J. Neurotrauma 1992, 9, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Alder, J.; Fujioka, W.; Lifshitz, J.; Crockett, D.; Thakker-Varia, S. Lateral Fluid Percussion: Model of Traumatic Brain Injury in Mice. J. Vis. Exp. JoVE 2011, 54, e3063. [Google Scholar] [CrossRef]
- Briones, T.L. Chapter 3 Animal Models of Traumatic Brain Injury: Is There an Optimal Model That Parallels Human Brain Injury? Annu. Rev. Nurs. Res. 2015, 33, 31–73. [Google Scholar] [CrossRef]
- Liu, Y.R.; Cardamone, L.; Hogan, R.E.; Gregoire, M.C.; Williams, J.P.; Hicks, R.J.; Binns, D.; Koe, A.; Jones, N.C.; Myers, D.E.; et al. Progressive Metabolic and Structural Cerebral Perturbations after Traumatic Brain Injury: An in Vivo Imaging Study in the Rat. J. Nucl. Med. 2010, 51, 1788–1795. [Google Scholar] [CrossRef]
- Rostami, E.; Davidsson, J.; Ng, K.C.; Lu, J.; Gyorgy, A.; Walker, J.; Wingo, D.; Plantman, S.; Bellander, B.-M.; Agoston, D.V.; et al. A Model for Mild Traumatic Brain Injury That Induces Limited Transient Memory Impairment and Increased Levels of Axon Related Serum Biomarkers. Front. Neurol. 2012, 3, 115. [Google Scholar] [CrossRef]
- Dixon, C.E.; Lyeth, B.G.; Povlishock, J.T.; Findling, R.L.; Hamm, R.J.; Marmarou, A.; Young, H.F.; Hayes, R.L. A Fluid Percussion Model of Experimental Brain Injury in the Rat. J. Neurosurg. 1987, 67, 110–119. [Google Scholar] [CrossRef]
- Dixon, C.E.; Clifton, G.L.; Lighthall, J.W.; Yaghmai, A.A.; Hayes, R.L. A Controlled Cortical Impact Model of Traumatic Brain Injury in the Rat. J. Neurosci. Methods 1991, 39, 253–262. [Google Scholar] [CrossRef]
- Friess, S.H.; Lapidus, J.B.; Brody, D.L. Decompressive Craniectomy Reduces White Matter Injury after Controlled Cortical Impact in Mice. J. Neurotrauma 2015, 32, 791–800. [Google Scholar] [CrossRef]
- Hoogenboom, W.S.; Branch, C.A.; Lipton, M.L. Animal Models of Closed-Skull, Repetitive Mild Traumatic Brain Injury. Pharmacol. Ther. 2019, 198, 109–122. [Google Scholar] [CrossRef] [PubMed]
- Responses to Cortical Injury: II. Widespread Depression of the Activity of an Enzyme in Cortex Remote from a Focal Injury—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/6784887/ (accessed on 26 July 2024).
- Feeney, D.M.; Boyeson, M.G.; Linn, R.T.; Murray, H.M.; Dail, W.G. Responses to Cortical Injury: I. Methodology and Local Effects of Contusions in the Rat. Brain Res. 1981, 211, 67–77. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhang, L.; Kallakuri, S.; Zhou, R.; Cavanaugh, J.M. Quantitative Relationship between Axonal Injury and Mechanical Response in a Rodent Head Impact Acceleration Model. J. Neurotrauma 2011, 28, 1767–1782. [Google Scholar] [CrossRef] [PubMed]
- Logsdon, A.F.; Lucke-Wold, B.P.; Turner, R.C.; Huber, J.D.; Rosen, C.L.; Simpkins, J.W. Role of Microvascular Disruption in Brain Damage from Traumatic Brain Injury. Compr. Physiol. 2015, 5, 1147–1160. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Aravind, A.; Pfister, B.J.; Chandra, N.; Haorah, J. Animal Models of Traumatic Brain Injury and Assessment of Injury Severity. Mol. Neurobiol. 2019, 56, 5332–5345. [Google Scholar] [CrossRef]
- Marmarou, A.; Foda, M.A.; van den Brink, W.; Campbell, J.; Kita, H.; Demetriadou, K. A New Model of Diffuse Brain Injury in Rats. Part I: Pathophysiology and Biomechanics. J. Neurosurg. 1994, 80, 291–300. [Google Scholar] [CrossRef]
- Morales, D.M.; Marklund, N.; Lebold, D.; Thompson, H.J.; Pitkanen, A.; Maxwell, W.L.; Longhi, L.; Laurer, H.; Maegele, M.; Neugebauer, E.; et al. Experimental Models of Traumatic Brain Injury: Do We Really Need to Build a Better Mousetrap? Neuroscience 2005, 136, 971–989. [Google Scholar] [CrossRef]
- Kabadi, S.V.; Hilton, G.D.; Stoica, B.A.; Zapple, D.N.; Faden, A.I. Fluid-Percussion-Induced Traumatic Brain Injury Model in Rats. Nat. Protoc. 2010, 5, 1552–1563. [Google Scholar] [CrossRef] [PubMed]
- Morales-Villagrán, A.; Salazar-Sánchez, J.C.; Chiprés-Tinajero, G.A.; Medina-Ceja, L.; Ortega-Ibarra, J. A Novel Hydro-Pneumatic Fluid Percussion Device for Inducing Traumatic Brain Injury: Assessment of Sensory, Motor, Cognitive, Molecular, and Morphological Outcomes in Rodents. Front. Mol. Neurosci. 2023, 16, 1208954. [Google Scholar] [CrossRef]
- Ouyang, W.; Wu, W.; Fan, Z.; Wang, J.; Pan, H.; Yang, W. Modified Device for Fluid Percussion Injury in Rodents. J. Neurosci. Res. 2018, 96, 1412–1429. [Google Scholar] [CrossRef]
- Chitturi, J.; Li, Y.; Santhakumar, V.; Kannurpatti, S.S. Early Behavioral and Metabolomic Change after Mild to Moderate Traumatic Brain Injury in the Developing Brain. Neurochem. Int. 2018, 120, 75–86. [Google Scholar] [CrossRef] [PubMed]
- Katz, P.S.; Molina, P.E. A Lateral Fluid Percussion Injury Model for Studying Traumatic Brain Injury in Rats. Methods Mol. Biol. 2018, 1717, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Petersen, A.; Soderstrom, M.; Saha, B.; Sharma, P. Animal Models of Traumatic Brain Injury: A Review of Pathophysiology to Biomarkers and Treatments. Exp. Brain Res. 2021, 239, 2939–2950. [Google Scholar] [CrossRef] [PubMed]
- A Systematic Review of Closed Head Injury Models of Mild Traumatic Brain Injury in Mice and Rats-PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/30661454/ (accessed on 26 July 2024).
- Lifshitz, J.; Rowe, R.K.; Griffiths, D.R.; Evilsizor, M.N.; Thomas, T.C.; Adelson, P.D.; McIntosh, T.K. Clinical Relevance of Midline Fluid Percussion Brain Injury: Acute Deficits, Chronic Morbidities, and the Utility of Biomarkers. Brain Inj. 2016, 30, 1293–1301. [Google Scholar] [CrossRef] [PubMed]
- Lyeth, B.G. Historical Review of the Fluid-Percussion TBI Model. Front. Neurol. 2016, 7, 217. [Google Scholar] [CrossRef]
- Dean, D.D.; Frank, J.A.; Turtzo, L.C. Controlled Cortical Impact in the Rat. Curr. Protoc. Neurosci. 2017, 81, 9.62.1–9.62.12. [Google Scholar] [CrossRef]
- Kawaguchi, M.; Furuya, H.; Patel, P.M. Neuroprotective Effects of Anesthetic Agents. J. Anesth. 2005, 19, 150–156. [Google Scholar] [CrossRef]
- Songarj, P.; Luh, C.; Staib-Lasarzik, I.; Engelhard, K.; Moosmann, B.; Thal, S.C. The Antioxidative, Non-Psychoactive Tricyclic Phenothiazine Reduces Brain Damage after Experimental Traumatic Brain Injury in Mice. Neurosci. Lett. 2015, 584, 253–258. [Google Scholar] [CrossRef]
- Talley Watts, L.; Sprague, S.; Zheng, W.; Garling, R.J.; Jimenez, D.; Digicaylioglu, M.; Lechleiter, J. Purinergic 2Y1 Receptor Stimulation Decreases Cerebral Edema and Reactive Gliosis in a Traumatic Brain Injury Model. J. Neurotrauma 2013, 30, 55–66. [Google Scholar] [CrossRef]
- Brody, D.L.; Mac Donald, C.; Kessens, C.C.; Yuede, C.; Parsadanian, M.; Spinner, M.; Kim, E.; Schwetye, K.E.; Holtzman, D.M.; Bayly, P.V. Electromagnetic Controlled Cortical Impact Device for Precise, Graded Experimental Traumatic Brain Injury. J. Neurotrauma 2007, 24, 657–673. [Google Scholar] [CrossRef]
- Fesharaki-Zadeh, A.; Miyauchi, J.T.; Laurent-Arriot, K.S.; Tsirka, S.E.; Bergold, P.J. Increased Behavioral Deficits and Inflammation in a Mouse Model of Co-Morbid Traumatic Brain Injury and Post-Traumatic Stress Disorder. 2020. Available online: https://journals.sagepub.com/doi/10.1177/1759091420979567 (accessed on 26 July 2024).
- Osier, N.D.; Dixon, C.E. The Controlled Cortical Impact Model: Applications, Considerations for Researchers, and Future Directions. Front. Neurol. 2016, 7, 134. [Google Scholar] [CrossRef] [PubMed]
- Siebold, L.; Obenaus, A.; Goyal, R. Criteria to Define Mild, Moderate, and Severe Traumatic Brain Injury in the Mouse Controlled Cortical Impact Model. Exp. Neurol. 2018, 310, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Schwulst, S.J.; Trahanas, D.M.; Saber, R.; Perlman, H. Traumatic Brain Injury-Induced Alterations in Peripheral Immunity. J. Trauma. Acute Care Surg. 2013, 75, 780–788. [Google Scholar] [CrossRef]
- Svirsky, S.E.; Henchir, J.; Li, Y.; Carlson, S.W.; Dixon, C.E. Temporal-Specific Sex and Injury-Dependent Changes on Neurogranin-Associated Synaptic Signaling After Controlled Cortical Impact in Rats. Mol. Neurobiol. 2024, 61, 7256–7268. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Gao, X.; Michalski, S.; Zhao, S.; Chen, J. Traumatic Brain Injury Severity Affects Neurogenesis in Adult Mouse Hippocampus. J. Neurotrauma 2016, 33, 721–733. [Google Scholar] [CrossRef] [PubMed]
- Kalish, B.T.; Whalen, M.J. Weight Drop Models in Traumatic Brain Injury. Methods Mol. Biol. 2016, 1462, 193–209. [Google Scholar] [CrossRef] [PubMed]
- Animal Models of Traumatic Brain Injury: Is There an Optimal Model to Reproduce Human Brain Injury in the Laboratory?—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/20416875/ (accessed on 26 July 2024).
- Kishimoto, Y.; Shishido, H.; Sawanishi, M.; Toyota, Y.; Ueno, M.; Kubota, T.; Kirino, Y.; Tamiya, T.; Kawai, N. Data on Amyloid Precursor Protein Accumulation, Spontaneous Physical Activity, and Motor Learning after Traumatic Brain Injury in the Triple-Transgenic Mouse Model of Alzheimer׳s Disease. Data Brief. 2016, 9, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.P.; Cai, J.; Shields, L.B.E.; Liu, N.; Xu, X.-M.; Shields, C.B. Traumatic Brain Injury Using Mouse Models. Transl. Stroke Res. 2014, 5, 454–471. [Google Scholar] [CrossRef]
- Statler, K.D.; Alexander, H.; Vagni, V.; Dixon, C.E.; Clark, R.S.B.; Jenkins, L.; Kochanek, P.M. Comparison of Seven Anesthetic Agents on Outcome after Experimental Traumatic Brain Injury in Adult, Male Rats. J. Neurotrauma 2006, 23, 97–108. [Google Scholar] [CrossRef]
- Fesharaki-Zadeh, A.; Datta, D. An Overview of Preclinical Models of Traumatic Brain Injury (TBI): Relevance to Pathophysiological Mechanisms. Front. Cell Neurosci. 2024, 18, 1371213. [Google Scholar] [CrossRef]
- Osier, N.D.; Korpon, J.R.; Dixon, C.E. Controlled Cortical Impact Model. In Brain Neurotrauma: Molecular, Neuropsychological, and Rehabilitation Aspects; Kobeissy, F.H., Ed.; Frontiers in Neuroengineering; CRC Press/Taylor & Francis: Boca Raton, FL, USA, 2015; ISBN 978-1-4665-6598-2. [Google Scholar]
- Smith, D.H.; Soares, H.D.; Pierce, J.S.; Perlman, K.G.; Saatman, K.E.; Meaney, D.F.; Dixon, C.E.; McIntosh, T.K. A Model of Parasagittal Controlled Cortical Impact in the Mouse: Cognitive and Histopathologic Effects. J. Neurotrauma 1995, 12, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.H.; Hicks, R.R.; Johnson, V.E.; Bergstrom, D.A.; Cummings, D.M.; Noble, L.J.; Hovda, D.; Whalen, M.; Ahlers, S.T.; LaPlaca, M.; et al. Pre-Clinical Traumatic Brain Injury Common Data Elements: Toward a Common Language Across Laboratories. J. Neurotrauma 2015, 32, 1725–1735. [Google Scholar] [CrossRef] [PubMed]
- Axelsson, H.; Hjelmqvist, H.; Medin, A.; Persson, J.K.; Suneson, A. Physiological Changes in Pigs Exposed to a Blast Wave from a Detonating High-Explosive Charge. Mil. Med. 2000, 165, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Guley, N.H.; Rogers, J.T.; Del Mar, N.A.; Deng, Y.; Islam, R.M.; D’Surney, L.; Ferrell, J.; Deng, B.; Hines-Beard, J.; Bu, W.; et al. A Novel Closed-Head Model of Mild Traumatic Brain Injury Using Focal Primary Overpressure Blast to the Cranium in Mice. J. Neurotrauma 2016, 33, 403–422. [Google Scholar] [CrossRef] [PubMed]
- Kallakuri, S.; Desai, A.; Feng, K.; Tummala, S.; Saif, T.; Chen, C.; Zhang, L.; Cavanaugh, J.M.; King, A.I. Neuronal Injury and Glial Changes Are Hallmarks of Open Field Blast Exposure in Swine Frontal Lobe. PLoS ONE 2017, 12, e0169239. [Google Scholar] [CrossRef]
- Nakagawa, A.; Manley, G.T.; Gean, A.D.; Ohtani, K.; Armonda, R.; Tsukamoto, A.; Yamamoto, H.; Takayama, K.; Tominaga, T. Mechanisms of Primary Blast-Induced Traumatic Brain Injury: Insights from Shock-Wave Research. J. Neurotrauma 2011, 28, 1101–1119. [Google Scholar] [CrossRef]
- Cernak, I.; Merkle, A.C.; Koliatsos, V.E.; Bilik, J.M.; Luong, Q.T.; Mahota, T.M.; Xu, L.; Slack, N.; Windle, D.; Ahmed, F.A. The Pathobiology of Blast Injuries and Blast-Induced Neurotrauma as Identified Using a New Experimental Model of Injury in Mice. Neurobiol. Dis. 2011, 41, 538–551. [Google Scholar] [CrossRef]
- Koliatsos, V.; Cernak, I.; Xu, L.; Song, Y.; Savonenko, A.; Crain, B.; Eberhart, C.; Frangakis, C.; Melnikova, T.; Kim, H.; et al. A Mouse Model of Blast Injury to Brain: Initial Pathological, Neuropathological, and Behavioral Characterization. J. Neuropathol. Exp. Neurol. 2011, 70, 399–416. [Google Scholar] [CrossRef]
- Rafaels, K.A.; ‘Dale’ Bass, C.R.; Panzer, M.B.; Salzar, R.S.; Woods, W.A.; Feldman, S.H.; Walilko, T.; Kent, R.W.; Capehart, B.P.; Foster, J.B.; et al. Brain Injury Risk from Primary Blast. J. Trauma. Acute Care Surg. 2012, 73, 895. [Google Scholar] [CrossRef]
- Garman, R.H.; Jenkins, L.W.; Switzer, R.C.; Bauman, R.A.; Tong, L.C.; Swauger, P.V.; Parks, S.A.; Ritzel, D.V.; Dixon, C.E.; Clark, R.S.B.; et al. Blast Exposure in Rats with Body Shielding Is Characterized Primarily by Diffuse Axonal Injury. J. Neurotrauma 2011, 28, 947–959. [Google Scholar] [CrossRef]
- Reneer, D.V.; Hisel, R.D.; Hoffman, J.M.; Kryscio, R.J.; Lusk, B.T.; Geddes, J.W. A Multi-Mode Shock Tube for Investigation of Blast-Induced Traumatic Brain Injury. J. Neurotrauma 2011, 28, 95–104. [Google Scholar] [CrossRef] [PubMed]
- (PDF) Blast Traumatic Brain Injury in the Rat Using a Blast Overpressure Model. Available online: https://www.researchgate.net/publication/234124806_Blast_Traumatic_Brain_Injury_in_the_Rat_Using_a_Blast_Overpressure_Model (accessed on 26 July 2024).
- Iacono, D.; Murphy, E.K.; Stimpson, C.D.; Leonessa, F.; Perl, D.P. Double Blast Wave Primary Effect on Synaptic, Glymphatic, Myelin, Neuronal and Neurovascular Markers. Brain Sci. 2023, 13, 286. [Google Scholar] [CrossRef] [PubMed]
- (PDF) Blast Overpressure in Rats: Recreating a Battlefield Injury in the Laboratory. Available online: https://www.researchgate.net/publication/24364547_Blast_Overpressure_in_Rats_Recreating_a_Battlefield_Injury_in_the_Laboratory (accessed on 26 July 2024).
- Modeling the Neurobehavioral Consequences of Blast-Induced Traumatic Brain Injury Spectrum Disorder and Identifying Related Biomarkers—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/26269904/ (accessed on 26 July 2024).
- Wojnarowicz, M.W.; Fisher, A.M.; Minaeva, O.; Goldstein, L.E. Considerations for Experimental Animal Models of Concussion, Traumatic Brain Injury, and Chronic Traumatic Encephalopathy-These Matters Matter. Front. Neurol. 2017, 8, 240. [Google Scholar] [CrossRef] [PubMed]
- Biomechanical Responses of a Pig Head under Blast Loading: A Computational Simulation|Semantic Scholar. Available online: https://www.semanticscholar.org/paper/Biomechanical-responses-of-a-pig-head-under-blast-Zhu-Skelton/7b575cf48e8d26b552c03cf4471932af57e1f508 (accessed on 26 July 2024).
- Albert-Weißenberger, C.; Várrallyay, C.; Raslan, F.; Kleinschnitz, C.; Sirén, A.-L. An Experimental Protocol for Mimicking Pathomechanisms of Traumatic Brain Injury in Mice. Exp. Transl. Stroke Med. 2012, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Earle, S.A.; de Moya, M.A.; Zuccarelli, J.E.; Norenberg, M.D.; Proctor, K.G. Cerebrovascular Resuscitation after Polytrauma and Fluid Restriction. J. Am. Coll. Surg. 2007, 204, 261. [Google Scholar] [CrossRef] [PubMed]
- Margulies, S.S.; Thibault, L.E.; Gennarelli, T.A. Physical Model Simulations of Brain Injury in the Primate. J. Biomech. 1990, 23, 823–836. [Google Scholar] [CrossRef]
- The Window of Risk in Repeated Head Injury—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/23259734/ (accessed on 26 July 2024).
- Ultrastructural Brain Abnormalities and Associated Behavioral Changes in Mice after Low-Intensity Blast Exposure-ScienceDirect. Available online: https://www.sciencedirect.com/science/article/abs/pii/S0166432818300718 (accessed on 26 July 2024).
- Cernak, I. Blast Injuries and Blast-Induced Neurotrauma: Overview of Pathophysiology and Experimental Knowledge Models and Findings. In Brain Neurotrauma: Molecular, Neuropsychological, and Rehabilitation Aspects; Kobeissy, F.H., Ed.; Frontiers in Neuroengineering; CRC Press/Taylor & Francis: Boca Raton, FL, USA, 2015; ISBN 978-1-4665-6598-2. [Google Scholar]
- Rutter, B.; Song, H.; DePalma, R.G.; Hubler, G.; Cui, J.; Gu, Z.; Johnson, C.E. Shock Wave Physics as Related to Primary Non-Impact Blast-Induced Traumatic Brain Injury. Mil. Med. 2021, 186, 601–609. [Google Scholar] [CrossRef]
- Iacono, D.; Hatch, K.; Murphy, E.K.; Cole, R.N.; Post, J.; Leonessa, F.; Perl, D.P. Proteomic Changes in the Hippocampus after Repeated Explosive-Driven Blasts. J. Proteome Res. 2024, 23, 397–408. [Google Scholar] [CrossRef]
- Liu, Y.; Lu, Y.; Shao, Y.; Wu, Y.; He, J.; Wu, C. Mechanism of the Traumatic Brain Injury Induced by Blast Wave Using the Energy Assessment Method. Med. Eng. Phys. 2022, 101, 103767. [Google Scholar] [CrossRef]
- Liu, W.; Chai, J.K.; Qin, B.; Han, S.F.; Wang, X.T.; Jiang, S.; Bai, H.L.; Liu, L.Y.; Chang, Y.; Yue, X.T.; et al. Effects of Blast Wave-Induced Biomechanical Changes on Lung Injury in Rats. Biomed. Environ. Sci. 2020, 33, 338–349. [Google Scholar] [CrossRef]
- Song, H.; Cui, J.; Simonyi, A.; Johnson, C.E.; Hubler, G.K.; DePalma, R.G.; Gu, Z. Linking Blast Physics to Biological Outcomes in Mild Traumatic Brain Injury: Narrative Review and Preliminary Report of an Open-Field Blast Model. Behav. Brain Res. 2018, 340, 147–158. [Google Scholar] [CrossRef] [PubMed]
- Song, H.; Chen, M.; Chen, C.; Cui, J.; Johnson, C.E.; Cheng, J.; Wang, X.; Swerdlow, R.H.; DePalma, R.G.; Xia, W.; et al. Proteomic Analysis and Biochemical Correlates of Mitochondrial Dysfunction after Low-Intensity Primary Blast Exposure. J. Neurotrauma 2019, 36, 1591–1605. [Google Scholar] [CrossRef] [PubMed]
- Song, H.; Konan, L.M.; Cui, J.; Johnson, C.E.; Hubler, G.K.; DePalma, R.G.; Gu, Z. Nanometer Ultrastructural Brain Damage Following Low Intensity Primary Blast Wave Exposure. Neural Regen. Res. 2018, 13, 1516–1519. [Google Scholar] [CrossRef] [PubMed]
- Panzer, M.B.; Matthews, K.A.; Yu, A.W.; Morrison, B.; Meaney, D.F.; Bass, C.R. A Multiscale Approach to Blast Neurotrauma Modeling: Part I–Development of Novel Test Devices for in Vivo and in Vitro Blast Injury Models. Front. Neurol. 2012, 3, 46. [Google Scholar] [CrossRef] [PubMed]
- Dogan, G.; Karaca, O. Evaluation of Neuroprotective Effect of Sevoflurane in Acute Traumatic Brain Injury: An Experimental Study in Rats. Turk. Neurosurg. 2020, 30, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Statler, K.D.; Alexander, H.; Vagni, V.; Holubkov, R.; Dixon, C.E.; Clark, R.S.B.; Jenkins, L.; Kochanek, P.M. Isoflurane Exerts Neuroprotective Actions at or near the Time of Severe Traumatic Brain Injury. Brain Res. 2006, 1076, 216–224. [Google Scholar] [CrossRef]
- Namjoshi, D.R.; Cheng, W.H.; McInnes, K.A.; Martens, K.M.; Carr, M.; Wilkinson, A.; Fan, J.; Robert, J.; Hayat, A.; Cripton, P.A.; et al. Merging Pathology with Biomechanics Using CHIMERA (Closed-Head Impact Model of Engineered Rotational Acceleration): A Novel, Surgery-Free Model of Traumatic Brain Injury. Mol. Neurodegener. 2014, 9, 55. [Google Scholar] [CrossRef]
- Viano, D.C.; Hamberger, A.; Bolouri, H.; Säljö, A. Concussion in Professional Football: Animal Model of Brain Injury—Part 15. Neurosurgery 2009, 64, 1162–1173, discussion 1173. [Google Scholar] [CrossRef]
- Cheng, W.H.; Martens, K.M.; Bashir, A.; Cheung, H.; Stukas, S.; Gibbs, E.; Namjoshi, D.R.; Button, E.B.; Wilkinson, A.; Barron, C.J.; et al. CHIMERA Repetitive Mild Traumatic Brain Injury Induces Chronic Behavioural and Neuropathological Phenotypes in Wild-Type and APP/PS1 Mice. Alzheimers Res. Ther. 2019, 11, 6. [Google Scholar] [CrossRef]
- Defining the Biomechanical and Biological Threshold of Murine Mild Traumatic Brain Injury Using CHIMERA (Closed Head Impact Model of Engineered Rotational Acceleration)—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/28274861/ (accessed on 26 July 2024).
- Krieg, J.L.; Leonard, A.V.; Tuner, R.J.; Corrigan, F. Characterization of Traumatic Brain Injury in a Gyrencephalic Ferret Model Using the Novel Closed Head Injury Model of Engineered Rotational Acceleration (CHIMERA). Neurotrauma Rep. 2023, 4, 761–780. [Google Scholar] [CrossRef]
- Sauerbeck, A.D.; Fanizzi, C.; Kim, J.H.; Gangolli, M.; Bayly, P.V.; Wellington, C.L.; Brody, D.L.; Kummer, T.T. modCHIMERA: A Novel Murine Closed-Head Model of Moderate Traumatic Brain Injury. Sci. Rep. 2018, 8, 7677. [Google Scholar] [CrossRef] [PubMed]
- Increased Severity of the CHIMERA Model Induces Acute Vascular Injury, Sub-Acute Deficits in Memory Recall, and Chronic White Matter Gliosis—ScienceDirect. Available online: https://www.sciencedirect.com/science/article/abs/pii/S0014488619302638 (accessed on 26 July 2024).
- Vonder Haar, C.; Martens, K.M.; Bashir, A.; McInnes, K.A.; Cheng, W.H.; Cheung, H.; Stukas, S.; Barron, C.; Ladner, T.; Welch, K.A.; et al. Repetitive Closed-Head Impact Model of Engineered Rotational Acceleration (CHIMERA) Injury in Rats Increases Impulsivity, Decreases Dopaminergic Innervation in the Olfactory Tubercle and Generates White Matter Inflammation, Tau Phosphorylation and Degeneration. Exp. Neurol. 2019, 317, 87–99. [Google Scholar] [CrossRef] [PubMed]
- Browne, K.D.; Chen, X.-H.; Meaney, D.F.; Smith, D.H. Mild Traumatic Brain Injury and Diffuse Axonal Injury in Swine. J. Neurotrauma 2011, 28, 1747–1755. [Google Scholar] [CrossRef] [PubMed]
- Song, H.; McEwan, P.P.; Ameen-Ali, K.E.; Tomasevich, A.; Kennedy-Dietrich, C.; Palma, A.; Arroyo, E.J.; Dolle, J.-P.; Johnson, V.E.; Stewart, W.; et al. Concussion Leads to Widespread Axonal Sodium Channel Loss and Disruption of the Node of Ranvier. Acta Neuropathol. 2022, 144, 967–985. [Google Scholar] [CrossRef]
- Cullen, D.K.; Harris, J.P.; Browne, K.D.; Wolf, J.A.; Duda, J.E.; Meaney, D.F.; Margulies, S.S.; Smith, D.H. A Porcine Model of Traumatic Brain Injury via Head Rotational Acceleration. Methods Mol. Biol. 2016, 1462, 289–324. [Google Scholar] [CrossRef]
- Solomon, D.; Kim, B.; Scultetus, A.; Arnaud, F.; Auker, C.; Freilich, D.; McCarron, R. The Effect of rFVIIa on Pro- and Anti-Inflammatory Cytokines in Serum and Cerebrospinal Fluid in a Swine Model of Traumatic Brain Injury. Cytokine 2011, 54, 20–23. [Google Scholar] [CrossRef] [PubMed]
- Zhan, X.; Oeur, A.; Liu, Y.; Zeineh, M.M.; Grant, G.A.; Margulies, S.S.; Camarillo, D.B. Translational Models of Mild Traumatic Brain Injury Tissue Biomechanics. Curr. Opin. Biomed. Eng. 2022, 24, 100422. [Google Scholar] [CrossRef]
- Zheng, Z.; Morykwas, M.; Campbell, D.; McGee, M.; Hollingsworth, C.; Adams, F.; Mays, J.; Tatter, S.; Argenta, L. Mechanical Tissue Resuscitation at the Site of Traumatic Brain Injuries Reduces the Volume of Injury and Hemorrhage in a Swine Model. Neurosurgery 2014, 75, 152–162. [Google Scholar] [CrossRef]
- Duhaime, A.C. Large animal models of traumatic injury to the immature brain. Dev. Neurosci. 2006, 28, 380–387. [Google Scholar] [CrossRef]
- Pareja, J.C.M.; Keeley, K.; Duhaime, A.-C.; Dodge, C.P. Modeling Pediatric Brain Trauma: Piglet Model of Controlled Cortical Impact. Methods Mol. Biol. 2016, 1462, 345–356. [Google Scholar] [CrossRef]
- Microbubble Gas Volume: A Unifying Dose Parameter in Blood-Brain Barrier Opening by Focused Ultrasound—PMC. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5196892/ (accessed on 26 July 2024).
- Ultrasound Physics and Instrumentation—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/34033355/ (accessed on 26 July 2024).
- Alhelfi, A.; Sundén, B. Predictions of Temperature and Pressure Fields Due to Collapse of a Bubble in Sulfuric Acid Solution Under Ultrasound. J. Therm. Sci. Eng. Appl. 2016, 8, 041010. [Google Scholar] [CrossRef]
- Bachmann, C.E.; Gruber, G.; Konermann, W.; Arnold, A.; Gruber, G.M.; Ueberle, F.; Gerdesmeyer, L. ESWT and Ultrasound Imaging of the Musculoskeletal System; Steinkopff: Heidelberg, Germany, 2001; ISBN 978-3-7985-1252-8. [Google Scholar]
- Prieur, F.; Pialoux, V.; Mestas, J.-L.; Mury, P.; Skinner, S.; Lafon, C. Evaluation of Inertial Cavitation Activity in Tissue through Measurement of Oxidative Stress. Ultrason. Sonochem. 2015, 26, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Blast-Associated Shock Waves Result in Increased Brain Vascular Leakage and Elevated ROS Levels in a Rat Model of Traumatic Brain Injury. PLoS ONE 2015, 10, e0127971. [CrossRef]
- Wang, C.-J. Extracorporeal Shockwave Therapy in Musculoskeletal Disorders. J. Orthop. Surg. Res. 2012, 7, 11. [Google Scholar] [CrossRef] [PubMed]
- Huang, A.P.-H.; Lai, D.-M.; Hsu, Y.-H.; Kung, Y.; Lan, C.; Yeh, C.-S.; Tsai, H.-H.; Lin, C.-F.; Chen, W.-S. Cavitation-Induced Traumatic Cerebral Contusion and Intracerebral Hemorrhage in the Rat Brain by Using an off-the-Shelf Clinical Shockwave Device. Sci. Rep. 2019, 9, 15614. [Google Scholar] [CrossRef] [PubMed]
- Kung, Y.; Lan, C.; Hsiao, M.-Y.; Sun, M.-K.; Hsu, Y.-H.; Huang, A.P.-H.; Liao, W.-H.; Liu, H.-L.; Inserra, C.; Chen, W.-S. Focused Shockwave Induced Blood-Brain Barrier Opening and Transfection. Sci. Rep. 2018, 8, 2218. [Google Scholar] [CrossRef]
- Takeuchi, S.; Nawashiro, H.; Sato, S.; Kawauchi, S.; Nagatani, K.; Kobayashi, H.; Otani, N.; Osada, H.; Wada, K.; Shima, K. A Better Mild Traumatic Brain Injury Model in the Rat. Acta Neurochir. Suppl. 2013, 118, 99–101. [Google Scholar] [CrossRef]
- Induction of a Transmissible Tau Pathology by Traumatic Brain Injury—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/30084913/ (accessed on 26 July 2024).
- Agoston, D.V.; Shutes-David, A.; Peskind, E.R. Biofluid Biomarkers of Traumatic Brain Injury. Brain Inj. 2017, 31, 1195–1203. [Google Scholar] [CrossRef]
- Agoston, D.V.; Helmy, A. Fluid-Based Protein Biomarkers in Traumatic Brain Injury: The View from the Bedside. Int. J. Mol. Sci. 2023, 24, 16267. [Google Scholar] [CrossRef]
- Mahan, M.Y.; Thorpe, M.; Ahmadi, A.; Abdallah, T.; Casey, H.; Sturtevant, D.; Judge-Yoakam, S.; Hoover, C.; Rafter, D.; Miner, J.R.; et al. Glial Fibrillary Acidic Protein (GFAP) Outperforms S100 Calcium-Binding Protein B (S100B) and Ubiquitin C-Terminal Hydrolase L1 (UCH-L1) as Predictor for Positive Computed Tomography of the Head in Trauma Subjects. World Neurosurg. 2019, 128, e434–e444. [Google Scholar] [CrossRef]
- Svingos, A.M.; Robicsek, S.A.; Hayes, R.L.; Wang, K.K.; Robertson, C.S.; Brophy, G.M.; Papa, L.; Gabrielli, A.; Hannay, H.J.; Bauer, R.M.; et al. Predicting Clinical Outcomes 7–10 Years after Severe Traumatic Brain Injury: Exploring the Prognostic Utility of the IMPACT Lab Model and Cerebrospinal Fluid UCH-L1 and MAP-2. Neurocritical Care 2022, 37, 172–183. [Google Scholar] [CrossRef] [PubMed]
- Trauma Diagnostic-Related Target Proteins and Their Detection Techniques—PMC. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11062145/ (accessed on 26 July 2024).
- Distribution of Five Clinically Important Neuroglial Proteins in the Human Brain—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/35765081/ (accessed on 26 July 2024).
- The Use and Potential of pNF-H as a General Blood Biomarker of Axonal Loss: An Immediate Application for CNS Injury—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/26269910/ (accessed on 26 July 2024).
- Increasing Rigor of Preclinical Research to Maximize Opportunities for Translation. Neurotherapeutics 2023, 20, 1433–1445. [CrossRef] [PubMed]
- Smith, D.H.; Kochanek, P.M.; Rosi, S.; Meyer, R.; Ferland-Beckham, C.; Prager, E.M.; Ahlers, S.T.; Crawford, F. Roadmap for Advancing Pre-Clinical Science in Traumatic Brain Injury. J. Neurotrauma 2021, 38, 3204–3221. [Google Scholar] [CrossRef] [PubMed]
- Iboaya, A.; Harris, J.L.; Arickx, A.N.; Nudo, R.J. Models of Traumatic Brain Injury in Aged Animals: A Clinical Perspective. Neurorehabil. Neural Repair. 2019, 33, 975–988. [Google Scholar] [CrossRef]

{kind=link}
| Method | Advantages | Disadvantages | Key Findings | References |
|---|---|---|---|---|
| FPI | A good model for assessing focal, diffuse, or mixed, focal and diffuse, TBI | Experimental reproducibility depends on the accuracy of craniectomy | A limitation of animal TBI models on the basis of CCI, WD, and FPI methods is that injuries are usually induced by direct impact to the brain through a craniectomy, with the animal’s head being fixed. In this case, these conditions are not typical of human TBI. The size and location of a craniectomy are significant factors that can dramatically change the severity of injury, even when the same device is used to remove the aponeurosis. | [13,37,39,40,44,45,46,47,48] |
| Possibility to assess behavioral outcomes in an animal model | Complex procedure | |||
| Evaluation of the efficiency of therapeutic remedies for translation into clinical practice | Development of pathological processes not associated with TBI | |||
| High mortality due to brainstem damage | ||||
| CCI | An animal focal injury model is the method of choice for studying TBI caused by direct blunt impact | A 5 mm trephination (injury window) is required | [13,49,50,51,52] | |
| Control and uniformity of injury | Hemorrhage and ischemia | |||
| No risk of re-injury | Blood–brain barrier disruption caused by tissue destruction | |||
| Damages persist up to 1 year due to brain atrophy and a progressive decrease in cerebral blood flow | ||||
| Development of an acute or chronic neurodegenerative condition | ||||
| Study reproducibility | Cognitive decline | |||
| WDI | Severity of TBI is controlled via the height and weight of the load | Unintentional skull fracture | [13,46,48,53,54,55,56,57,58] | |
| Risk of a second rebound injury | ||||
| A cost-effective and relatively easy to use model | Increased mortality rate | |||
| Lack of repeatability of the animal model |
| Method | Advantages | Disadvantages | Key Findings | References |
|---|---|---|---|---|
| Shock tube | Generated energy does not dissipate | Injury in rodents should be scaled to comparable injury in humans | Differences in rodent models and human injury become noticeable when modeling repeated mild TBI, which requires accounting for differences in temporal pathology. In particular, an increase in vulnerability in rodents occurs at the hourly scale, whereas that in humans occurs at the daily scale. Additionally, injury classification in animal TBI models (mild, moderate, and severe) is not standardized. | [98,101,102,103,104,105,106] |
| High repeatability of the animal model | There is no possibility to create peak pressure of the same intensity as that from a blast in an open field | |||
| There are no secondary or tertiary effects of blast injury | Differences between animals and humans in the brain surface, mass, geometry, white/gray matter ratio, and size | |||
| Provides precise control of blast wave intensity | No opportunity to generate a polytrauma model | |||
| No standards of explosivs, tube design, species, location in the tube, body shielding, and head mobility | ||||
| Open-field blast (BI) | Impulse shock wave (DAS) | Dissipation of generated energy | [66,107,108,109,110,111,112,113] | |
| Exponential pressure reduction (MPA method) | Blast source is quickly weakened | |||
| Possibility of a polytrauma model | Prolonged preparation for the experiment | |||
| Friedlander signal generation and MPA method | No standards of explosives | |||
| Spherical distribution of the blast wave in three-dimensional space | Differences between animals and humans in the brain surface, mass, geometry, white/gray matter ratio, and their sizes |
| Intensity Level | 8 | 10 | 16 | 20 |
|---|---|---|---|---|
| Negative peak pressure (MPa) | −10.92 | −12.9 | −14.21 | −18.7 |
| Positive peak pressure (MPa) | 23.1 | 28.5 | 48.1 | 77.7 |
| Energy flux density (total) (MJ/mm2) | 0.27 | 0.35 | 0.6 | 0.82 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balakin, E.; Yurku, K.; Fomina, T.; Butkova, T.; Nakhod, V.; Izotov, A.; Kaysheva, A.; Pustovoyt, V. A Systematic Review of Traumatic Brain Injury in Modern Rodent Models: Current Status and Future Prospects. Biology 2024, 13, 813. https://doi.org/10.3390/biology13100813
Balakin E, Yurku K, Fomina T, Butkova T, Nakhod V, Izotov A, Kaysheva A, Pustovoyt V. A Systematic Review of Traumatic Brain Injury in Modern Rodent Models: Current Status and Future Prospects. Biology. 2024; 13(10):813. https://doi.org/10.3390/biology13100813
Chicago/Turabian StyleBalakin, Evgenii, Ksenia Yurku, Tatiana Fomina, Tatiana Butkova, Valeriya Nakhod, Alexander Izotov, Anna Kaysheva, and Vasiliy Pustovoyt. 2024. "A Systematic Review of Traumatic Brain Injury in Modern Rodent Models: Current Status and Future Prospects" Biology 13, no. 10: 813. https://doi.org/10.3390/biology13100813
APA StyleBalakin, E., Yurku, K., Fomina, T., Butkova, T., Nakhod, V., Izotov, A., Kaysheva, A., & Pustovoyt, V. (2024). A Systematic Review of Traumatic Brain Injury in Modern Rodent Models: Current Status and Future Prospects. Biology, 13(10), 813. https://doi.org/10.3390/biology13100813