Simple Summary
Health promotion is important in older adults. However, aging-induced frailty results in poor muscle activity in the upper limbs, leading to activity impairments. Fortunately, recent studies report that vibration is a safe approach for improving muscular function; however, different frequencies and directions of vibrations can result in inconsistencies in muscle function improvement, and further investigation is needed. We developed a handheld vibrator to determine the effect of vibration frequency and direction on upper-limb muscle activation. Nineteen qualified participants were exposed to vertical and horizontal vibrations with 0, 15, 30, 45, and 60 Hz frequencies for 60 s each. Surface electromyography measured the activities of the flexor digitorum superficialis (FDS), flexor carpi radialis (FCR), extensor carpi ulnaris (ECU), extensor carpi radialis (ECR), biceps, triceps, and deltoid anterior muscles. Muscle activity was significantly induced under vibration conditions in both vertical and horizontal directions. The 45-Hz horizontal vibration induced maximum muscle activations for the FDS, ECR, ECU, biceps, and triceps. The 60-Hz vertical and 30-Hz horizontal vibrations facilitated maximum muscle activations for the FCR and deltoid anterior, respectively. We therefore suggest different protocols of vibration for specific weak muscles to improve muscle function in the upper limbs of older adults.
Abstract
We aimed to determine the effect of vibration frequency and direction on upper-limb muscle activation using a handheld vibrator. We recruited 19 healthy participants who were instructed to hold a handheld vibrator in their dominant hand and maintain the elbow at 90° flexion, while vertical and horizontal vibrations were applied with frequencies of 15, 30, 45, and 60 Hz for 60 s each. Surface electromyography (EMG) measured the activities of the flexor digitorum superficialis (FDS), flexor carpi radialis (FCR), extensor carpi ulnaris (ECU), extensor carpi radialis (ECR), biceps, triceps, and deltoid anterior muscles. EMG changes were evaluated as the difference in muscle activity between vibration and no-vibration (0 Hz) conditions. Muscle activity was induced under vibration conditions in both vertical and horizontal (p < 0.05) directions. At 45 Hz, FDS and FCR activities increased during horizontal vibrations, compared with those during vertical vibrations. ECU activity significantly increased under 15-Hz vertical vibrations compared with that during horizontal vibrations. Vibrations from the handheld vibrator significantly induced upper-limb muscle activity. The maximum muscle activations for FDS, ECR, ECU, biceps, and triceps were induced by 45-Hz horizontal vibration. The 60-Hz vertical and 30-Hz horizontal vibrations facilitated maximum muscle activations for the FCR and deltoid anterior, respectively.
1. Introduction
Muscle activation and related upper-limb functions play important roles in performing activities of daily living such as feeding, bathing, and dressing. Aging or neurologic disorders may result in upper-limb motor control and functional impairment [1]. Many studies have indicated that older adults with degenerative conditions exhibit significant motor function deficits, which lead to frailty and long-term disabilities [2,3,4]. However, studies have also revealed that the frailty could result from the physiologic age-dependent changes in vicious loops [5,6] or lifestyle (sedentary behaviors) [7], leading to poor muscle strength and muscle atrophy (sarcopenia) [5,6]. This could result in muscle weakness, low physical activity, and impaired upper-limb function [5,6,7,8,9,10,11,12,13] and could increase dependency levels in daily living for older persons. Moreover, older adults are reportedly predisposed to developing muscle atrophy and weakness. Greenlund et al. reported that mortality due to stroke—one of the most common neurologic diseases in older adults—has decreased [14]; however, stroke-induced motor function deficits result in paretic upper limbs [15,16], which alter the daily functioning and quality of life and cause long-term disabilities in patients with stroke [17,18]. Only 15% of patients in the acute and subacute stages of stroke who undergo traditional rehabilitation interventions recover their paretic upper-limb motor function [19]. An appropriate rehabilitation intervention is required to improve upper-limb neuromuscular function and motor recovery in older adults and people after stroke.
The vibration approach is reportedly effective, easy, satisfactory, and safe for improving muscle strength, power, and function [20,21,22,23]. The mechanism for muscle function improvement is based on facilitating the activation of the efferent Ia muscle fibers during vibration approaches, leading to α-motor neuron excitation, which produces more muscle force output [24,25]. The vibration approach included asking the participants to sit on a chair or kneel on the ground and to place their hands or elbows on the vibratory platform [22,26,27,28,29,30,31,32] or to directly sit on the vibratory platform with two hands in the sideways position on the vibratory platform [33]. Studies have shown that different vibration approach protocols (frequencies between 5 and 60 Hz) and vibration directions (horizontal or vertical) lead to improvements in muscle strength [25,34,35,36]. However, contradictory findings were also reported in recent studies [22,37]. Vibration transmission is a complex process that is influenced by biomechanics [27,38]; beside the vibration frequencies, the different postures during vibration approaches may also affect upper-limb muscle activation [22,27]. This indicates that the force translation to the upper limbs may change because different postures may result in different vibration directions from the vibrator. Based on previous findings regarding the mechanism and inconsistent findings of vibration approaches, we speculated that vibration frequency and directions constitute key factors that facilitate muscle activation during vibration approaches. In addition, the outcome of vibration application on the upper-limb musculature remains inconclusive because of differences in the vibration stimuli applied and limited appropriate equipment; only a few studies have applied vibration-induced muscle activations in the upper limbs [27,28,39,40,41]. Furthermore, many studies have suggested that the efficacy of appropriate equipment with optimal vibration protocols to induce muscle activation should be established before applying these protocols clinically [23,24,25,42,43,44,45]. Furthermore, recent studies have suggested that vibration-induced changes in neuromuscular activation during different vibration stimuli can be evaluated directly using the root mean squares of surface electromyographic (EMG) signals (EMGrms), which reveal the effect of vibration stimuli on muscle strength enhancement [27]. Therefore, this study aimed to develop a handheld vibrator to determine the effect of vibration frequency and direction on upper-limb muscle activation.
2. Material and Methods
2.1. Participants
The sample size requirement was calculated using G*power (version 3.1.9.2, Heinrich-Heine-Universität, Düsseldorf, Germany) using an effect size of 0.25, an alpha of 0.05, and a power of 0.80. A total sample size of 34 participants was required. However, due to the coronavirus disease 2019 (COVID-19) pandemic, only 19 adults were recruited. The inclusion criteria required that participants be able to follow the researcher’s instructions and study procedures, be healthy with no cognitive disorders that could affect the vibration approach performance, be able to steadily hold a handheld vibrator using the dominant hand without pain or discomfort, and have good cognitive function. We excluded patients with acute or chronic neurologic or orthopedic impairments and those who experienced discomfort or had undergone surgery in the upper limbs within 6 months prior to the study onset. The dominant hand for each participant was considered the hand that was used to sign the informed consent form.
This study was conducted in communities and approved by the institutional review board of Taipei Medical University (approval number: N202007048). All participants signed an informed consent form before participating in this study. This study was carried out in accordance with the Declaration of Helsinki.
2.2. Research Device and Data Processing
A handheld vibrator (measuring 37 × 8.3 × 10.5 cm; weight, 1 kg) was designed and customized by ACCU BALANCES CORP. (New Taipei City, Taiwan). The handheld vibrator motor (ZYT3424D110; 1.833 V = 1 Hz) produced vibrations with a 5-mm amplitude and 0–60-Hz frequency range, and its validity was confirmed by analyzing the vibration frequencies generated by the vibrator between 0–60-Hz with APDM-collected vibration frequency data. The vibration frequency could be controlled using a vibration controller (rotary potentiometer) located on the right side of the vibration frequency control box; a frequency mechanical pointer located on the left side of the box showed the voltage applied to the vibration motor, which is correlated with the frequency measurement via APDM (Figure 1). To determine the effects of vibration on the upper limbs, a red line target indicated the position for holding the vibrator during vertical (up and down vibration in the sagittal plane) and horizontal (medial and lateral vibration in the horizontal plane) vibration approaches (Figure 2). The handheld vibrator was applied to generate vibration force to the entire upper limb rather than a specific muscle during the vibration tests.
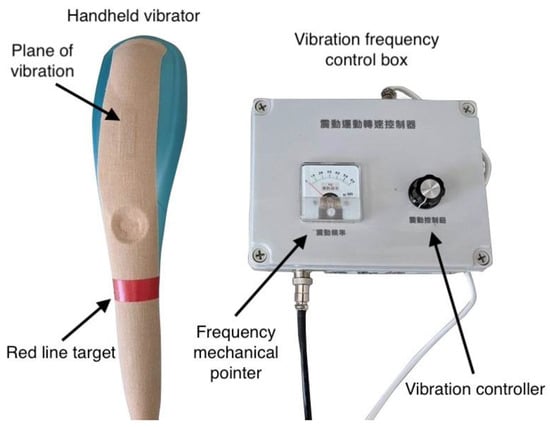
Figure 1.
Handheld vibrator and related component parts.
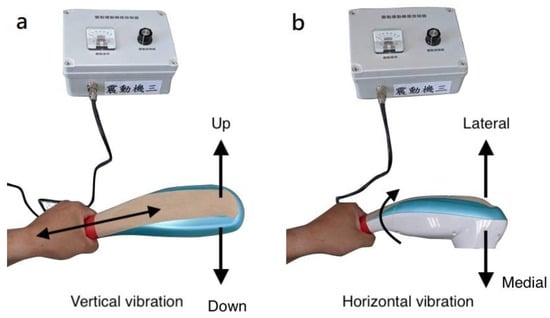
Figure 2.
Illustrations for vertical (a) and horizontal (b) vibration conditions.
The research device includes a handheld vibrator and vibration frequency control box. The researcher controls the vibration frequency, which is displayed on the mechanical pointer, using the vibration controller.
Participants used their dominant hand to hold the vibrator at the red line. Participants held the vibrator in two different ways (Figure 2a,b) so that the direction of vibration was either up–down or lateral–medial.
2.3. Experimental Procedures and Positioning of Participants
All participants were instructed to sit back on a high-fixed, no-arm support chair with their feet positioned flat on the floor. The dominant shoulder was positioned sideways, slightly apart from the trunk, and the elbow was fixed at 90° flexion as the standard vibration position (Figure 3). Thereafter, the researcher instructed the participants to hold the red line on the vibrator firmly with the dominant hand. Participants randomly performed all vibration tests comprising five vibration frequencies (0, 15, 30, 45, and 60 Hz) in the vertical and horizontal vibration directions. Moreover, participants were instructed to perform all vibration approaches while maintaining the elbow in the standard vibration position.
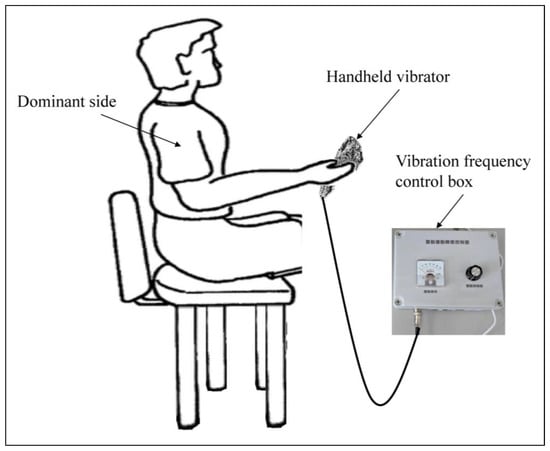
Figure 3.
Experimental setting for the vibration.
Based on our review of previous clinical studies on improving muscle strength, we used vibration protocols with vibration exposure between 30 and 60 s and with resting intervals between 15 and 60 s [46,47,48,49]. Studies have reported that fatigue [50], muscle adaption, and injury risk [24] can increase when vibrations last more than 1 min. Previous research also reported that the vibration approach has 30 s of maintained effects on facilitating muscle excitation [51]. Therefore, the vibration approach was performed for 60 s with a 1-min resting interval between sessions to avoid muscle fatigue.
2.4. EMG Analysis
Seven muscle groups, including the flexor digitorum superficialis (FDS), flexor carpi radialis (FCR), extensor carpi radialis (ECR), extensor carpi ulnaris (ECU), biceps, triceps, and deltoid anterior, were selected to represent the performance of the upper limbs [22,52]. EMG signals were measured using the BTS FREEEMG 1000 with EMG-BTS EMG-Analyzer® (BTS Bioengineering, Milan, Italy) during vibration exposure, at a sampling frequency of 1000 Hz. Based on the Surface Electromyography for the Non-invasive Assessment of Muscles guidelines, pairs of bipolar Ag-AgCl electrodes (H124SG Covidien, Minneapolis, MN, USA) were placed over the belly of each muscle, with an inter-electrode distance of 2 cm [53]. Before placing the electrodes, each participant’s skin was thoroughly cleaned with alcohol swabs [27]. Electromyography (EMG) signals were amplified with a gain of 1000. EMG post-processing was performed using the EMG-Analyzer. We used bandpass EMG signals (20–400 Hz); a notch filter was used to remove the noise from the power line (60 Hz). EMGrms, with a 100-ms window, was used to process EMG data for each muscle during five vibration approaches sessions [27,30,39,54]. Further, the EMGrms values were normalized with respect to the percentage of maximum voluntary contraction of each corresponding muscle for each participant [39].
2.5. Statistical Analysis
The Shapiro–Wilk test was performed to test the normality of the sample data. The Mann–Whitney U test was performed to confirm whether the vibration approaches had a significant impact on individual muscle activation in the vertical and/or horizontal vibration directions. Further, the Friedman test was performed to compare the increase in muscle activation between vibration (15, 30, 45, and 60 Hz) and no-vibration (0 Hz) conditions. Lastly, the Wilcoxon signed-rank test was performed to compare vibration direction-related changes in muscle activation for each muscle with different vibration frequencies in the vertical and horizontal vibration directions. The alpha level was set at 0.05. Statistical Package for the Social Sciences software (version 17.0, SPSS Inc., Chicago, IL, USA) was used for statistical analysis.
3. Results
3.1. Participants
Nineteen adults (age 38.2 ± 14.0 years; 14 female and 5 male) were recruited in this study (Table 1).

Table 1.
Demographic characteristics.
3.2. EMG Analysis
All variables were assumed to be non-normally distributed (all p < 0.001, respectively), including FDS, FCR, ECR, ECU, biceps, triceps, and deltoid anterior.
On comparing the vibration direction-related changes in muscle activation for upper-arm and shoulder muscles, the results showed no statistically significant differences in muscle activation for the biceps, triceps, and deltoid anterior muscles at 0, 15, 30, 45, and 60 Hz vibration frequencies in the horizontal and vertical vibration directions (Table 2; Figure 4).
Table 2.
Vibration-induced changes in EMGrms (%) compared with those in the no-vibration condition.
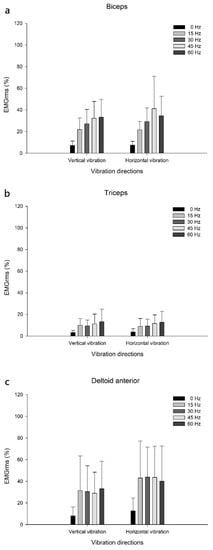
Figure 4.
Upper-arm and shoulder muscle activation. Muscle activations in the biceps (a), triceps (b), and deltoid anterior (c) at 0, 15, 30, 45 and 60 Hz vibration frequencies for vertical and horizontal vibration directions. EMGrms, root mean square of surface electromyographic signals.
However, the FDS and FCR muscles were more activated during the 45-Hz vibration approach in the horizontal vibration direction than in the vertical direction (p < 0.05). In addition, the ECU muscles were more activated during the 15-Hz vibration approach in the vertical vibration direction than in the horizontal direction (Table 2; Figure 5).
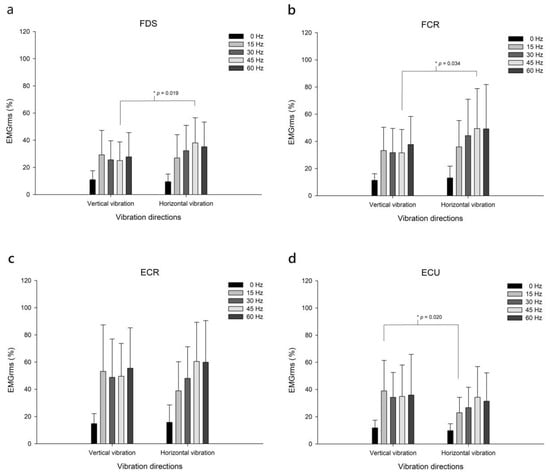
Figure 5.
Forearm muscle activation. Muscle activations in the FDS (a), FCR (b), ECR (c), and ECU (d) muscles of the forearm at 0, 15, 30, 45, and 60 Hz vibration frequencies in the vertical and horizontal vibration directions. EMGrms, root mean square of surface electromyographic signals. FDS, flexor digitorum superficialis; FCR, flexor carpi radialis; ECR, extensor carpi radialis; ECU, extensor carpi ulnaris.
The vibration approaches significantly impacted all individual muscle activations in the vertical (p < 0.05) and horizontal (p < 0.05) vibration directions (Table 2).
All muscle groups had significantly facilitated muscle activation in the vibration condition compared with that in the no-vibration condition, in both vibration directions (Table 2). Furthermore, compared with no-vibration (0 Hz), for both vertical and horizontal vibration directions, the maximum muscle activation for FCR was facilitated by 60 Hz vertical vibration (p < 0.001); the maximum muscle activations for FDS, ECR, ECU, biceps, and triceps were induced during 45 Hz horizontal vibration (p < 0.001), respectively. For the deltoid anterior, the maximum muscle activation frequency was induced during 30 Hz horizontal vibration (p < 0.001) (Table 2).
4. Discussion
Many studies have used whole-body vibration devices to investigate the impact of vibration approaches on upper-limb muscle activation [22,26,27,28,29,31,32]. In contrast, this study developed a frequency-controlled handheld vibrator with a focus on upper-limb muscle activation. We found that vibration approaches with specific frequencies (15, 30, 45, and 60 Hz) had a positive effect on muscle activation in all seven muscle groups i.e., FDS, FCR, ECR, ECU, biceps, triceps, and deltoid anterior in both the vertical and horizontal directions, unlike in the absence of vibration (0 Hz). Furthermore, horizontal and vertical vibrations had a significant facilitatory effect on the activation of upper-limb flexors (FDS and FCR muscles) and extensors (ECU muscles), respectively. To the best of our knowledge, this is the first study to report that different vibration directions induce the activation of different upper-limb muscles.
4.1. Vibrator Types and Applications in Upper-Limb Muscle Activity Induction
Most previous studies used vibratory platforms as the vibrator, and participants were instructed to take specific positions for upper-limb muscle activation. For instance, participants were instructed to sit on a chair or kneel on the ground and then support their upper limbs over the vibratory platform with their hands or elbows shoulder-width apart [22,26,27,28,29,30,31,32]. In other studies, participants were instructed to hold the handrail on the top of the vibratory platform [27] or sit on the vibratory platform with two hands in the sideways position [33]. The approaches used in previous studies may or may not have induced upper-limb muscle activation; however, they could cause vertigo or discomfort as the inappropriate and excess vibration force from whole-body vibration could be transmitted to the head [21]. Approximately 2.4–3.6% of individuals who undergo whole-body vibration approaches develop vertigo [21], muscle soreness [21,55] and discomfort [21,24,56]. Few studies have applied flexi-bar approaches for upper-limb muscle strength enhancement; nonetheless, the vibration frequency and amplitude derived from flexi-bar approaches cannot be used for vibration approaches because flexi-bar vibrations are generated, and their frequencies change based on the participant’s force and skill [57]. In this study, participants were instructed to hold the handheld vibrator in their dominant hand, with their trunk supported on a chair and to maintain their upper limbs in a specific vibration position. Unlike previous studies, our study found that the use of frequency-controlled vibrations from the handheld vibrator could significantly facilitate upper-limb muscle activation without the occurrence of adverse effects such as vertigo and discomfort.
4.2. Influence of Vibration Frequency on Upper-Limb Muscle Activation
We found that vibration approaches significantly facilitated upper-limb muscle activation in the vertical and horizontal vibration directions. Unlike no-vibration conditions, vibration conditions enhanced upper-limb muscle activation by 31.4–52.2% and 28.5–54.9% in the vertical and horizontal vibration directions, respectively. Specifically, the maximum muscle activation for FCR was facilitated at 60 Hz in the vertical vibration direction; the maximum muscle activations for FDS, ECR, ECU, biceps, and triceps were induced at 45 Hz in the horizontal vibration direction, respectively. For the deltoid anterior, the maximum muscle activation frequency was 30 Hz in the horizontal direction. Hence, vibration frequencies between 30 and 60 Hz may be used to facilitate maximum muscle activations, and more than half of the muscle groups were activated by high-frequency vibrations (45 and 60 Hz). Recent studies also reported similar findings and showed that a high-frequency vibration has a greater facilitatory effect on muscle activation than a low-frequency vibration in healthy participants and patients with stroke [39,43]. However, the increased muscle activation does not linearly correlate with increasing vibration frequencies [34]. For example, the activation of all muscles at 60 Hz increased the EMGrms by only 0.9–9% rather than doubling it in both vertical and horizontal vibration directions. This phenomenon may be the result of a damping reaction on muscle activation when performing vibration [34]. This corroborates the findings of a recent study, which reported that doubling the acceleration of the applied vibration only facilitates a 3–5% increase in EMGrms [58]. Our findings show that high-frequency vibrations facilitate upper-limb muscle activation, but they may lead to discomfort. For example, whole-body vibration can cause bone frailty, back pain [38,59], resonance injury, and dizziness [21,56]; a vibration frequency of >40 Hz may significantly affect posture control, which results in muscle fatigue [60] and an unstable posture sway [61]. In this study, no participants reported any discomfort or dizziness during or after vibration testing. This may be because the participants were asked to perform all vibration approaches while maintaining the upper limbs in the standard vibration position. Most of the vibration force was thus absorbed by the upper limbs, with little vibration force translating to the body and head. If individuals are unable to hold the vibrator and resist the vibration force during high-frequency vibration approaches, injuries may ensue [62]. Therefore, based on the findings of this study along with those of previous studies, we suggest that a 30-Hz vibration frequency in combination with active muscle participation may be the optimal and safe vibration approach for upper-limb muscle activation. Further studies should be conducted to confirm the benefits of this frequency toward improving muscle strength and function for people with disabilities.
4.3. Vibration Direction Affects Upper-Limb Muscle Activation
The FDS and FCR activities at a 45-Hz vibration frequency during horizontal vibrations increased by 9.7% and 6.2%, respectively, compared to that during vertical vibrations. In addition, ECU activation at a 15-Hz vibration frequency was significantly higher in the vertical than in the horizontal vibration direction, by 11.7%. Horizontal vibration has a greater facilitatory effect on FDS muscle activation probably because more muscle activation is required to maintain the handheld vibrator in a fixed position. Additionally, we found that many participants unconsciously flexed their wrists to maintain stability during vibration, which could result in a greater facilitatory effect on FCR activation. Vertical vibration tends to produce a greater facilitatory effect on extensor muscle activation, probably because the device vibrates in the direction of gravity; hence, extensors resist both gravity and the vibration force from the vibrator to maintain the vibration approach posture. Different postures may also result in different vibration directions for the upper limbs during vibration approaches; nonetheless, few studies have investigated the impact of different postures on upper-limb muscle activation. Two recent studies recruited healthy participants to perform vibration approaches in different postures, such as standing on the vibratory platform with arms along the body (squat posture), holding a handrail on top of the vibratory platform in the half-squatting position, and kneeling on the ground with both hands supported over the platform (push-up modified posture) [22,27]. These studies found that muscle strength increases in the push-up modified posture than in the half-squatting posture [27], and the EMGrms for the FDS muscle during squatting was significantly higher than that in the non-vibration condition by 23.3% [22]. However, these findings are difficult to compare with those of the present study because the vibration approaches were different, warranting further investigation.
4.4. Study Limitations and Future Perspectives
Our study has some limitations. We developed a frequency-controlled handheld vibrator and indicated the facilitatory effect of vibration approaches on upper-limb muscle activation; however, vibration force transmission and the activation of different upper-limb muscles are complex processes that are influenced by biomechanics [27,38] and vibration protocol parameters (frequency, amplitude, displacement, vibration time, types of vibration, and postures) [42]. Our study only evaluated the effects of vibration frequency and direction on upper-limb muscle activation; hence, the impacts of the other vibration protocol parameters require further investigation. In addition, we suggest that future studies use wearable accelerometers to directly measure the vibration-induced accelerations in target muscle groups of the upper limbs, with analysis of their relationship to muscle activation. For participants, the ratio of male to female participants was not equal in this study. A recent study reported that the body mass of males is higher than that of females and found that vibration-induced accelerations of the body in three dimensions are lower in males [63]. This finding suggests that sex-related differences in body properties and structure may impact the effects of vibration on muscle activation and should thus be considered when applying the vibration approach clinically. Additionally, participants were asked to maintain a firm grip of the vibration device during the experiments. We believe the grip force was approximately constant throughout the experiment, otherwise the participants would have lost grip of the device. However, we did not measure the grip force or pressure underneath, which may have affected the amount of vibration delivered. Future studies could investigate the effects of grip force levels on muscle strength gain due to vibration training. We found many participants unconsciously flexed their wrists to maintain the vibration position of the upper limbs during vibration, which could have been caused by the posture response-induced muscle activation. Future studies should design appropriate vibrators related to the upper limbs, rather than using whole-body vibrators. Furthermore, APDM was applied to validate the vibration frequencies generated by the vibrator between 0 and 60 Hz in this study. However, the maximum sampling frequency for APDM is 128 Hz. To measure vibration frequencies of 60 Hz, a sampling rate that is at least 10 times higher (i.e., ≥600 Hz) is ideal. Theoretically, using a sampling rate that is twice the frequency seems sufficient, but that is the bare minimum. Future studies should use a rate that is at least 10 times larger to collect more accurate measurement of vibration frequency. Meanwhile, due to the COVID-19 pandemic, participant recruitment was limited. Future studies should include a large sample size, along with optimal vibration frequencies and directions during training programs. This would facilitate muscle activation and improve muscle function and functional recovery in frail, older adults, and patients with stroke.
5. Conclusions
In this study, we developed a handheld vibrator and validated its positive effects on upper-limb muscle activation. The 45-Hz horizontal vibration approach can induce maximum activations for the FDS, ECR, ECU, biceps, and triceps muscles. Moreover, 60-Hz vertical and 30-Hz horizontal vibrations can facilitate the maximum muscle activations for the FCR and deltoid anterior, respectively. Further studies should be conducted to confirm the benefits of this frequency toward improving muscle strength and function for people with disabilities.
Author Contributions
Conceptualization, C.-H.N., Y.-H.L., C.-H.L. (Chia-Huei Lin) and C.-H.L. (Chueh-Ho Lin); Data curation, S.-F.K., L.-H.L. and X.-M.W.; Formal analysis, S.-F.K., C.-H.L. (Chia-Huei Lin) and J.-L.C.; Funding acquisition, C.-H.N. and C.-H.L. (Chueh-Ho Lin); Investigation, C.-H.N., Y.-H.L., L.-W.C., C.-H.L. (Chia-Huei Lin), S.-L.C., L.-H.L., X.-M.W., J.-L.C. and C.-H.L. (Chueh-Ho Lin); Methodology, C.-H.N., Y.-H.L., L.-W.C., S.-F.K., C.-H.L. (Chia-Huei Lin), S.-L.C., L.-H.L., X.-M.W., J.-L.C. and C.-H.L. (Chueh-Ho Lin); Project administration, C.-H.N., Y.-H.L. and C.-H.L. (Chueh-Ho Lin); Resources, C.-H.N., Y.-H.L., L.-W.C., C.-H.L., S.-L.C., L.-H.L., X.-M.W., J.-L.C. and C.-H.L. (Chueh-Ho Lin); Software, L.-W.C. and S.-F.K.; Supervision, C.-H.N., Y.-H.L., L.-W.C., S.-L.C. and C.-H.L. (Chueh-Ho Lin); Validation, C.-H.N., Y.-H.L., L.-W.C., S.-F.K., S.-L.C., L.-H.L., X.-M.W., J.-L.C. and C.-H.L. (Chueh-Ho Lin); Visualization, C.-H.N. and L.-W.C.; Writing—original draft, C.-H.N., Y.-H.L., L.-W.C., S.-F.K., C.-H.L. (Chia-Huei Lin), S.-L.C., L.-H.L., X.-M.W. and C.-H.L. (Chueh-Ho Lin); Writing—review & editing, C.-H.L. (Chueh-Ho Lin). All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Ministry of Science and Technology (MOST) of Taiwan (MOST 111-2221-E-038-015, MOST 111-2622-E-038-002, MOST 110-2221-E-038-016, MOST 109-2622-B-038-007) and Taipei Medical University—Wan Fang Hospital (108TMU-WFH-24).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Taipei Medical University (Approval Number: N202007048, 5 August 2022).
Informed Consent Statement
Written informed consent has been obtained from the patient(s) in this study.
Data Availability Statement
The datasets are available from the corresponding author upon reasonable request.
Acknowledgments
The authors would like to thank all study participants, research assistant Chia-Hui Kao who conducted this study, and the Editage team for English language editing. We acknowledge the (statistical/computational/technical) support of the Health Data Analytics and Statistics Center, Office of Data Science, Taipei Medical University, Taiwan.
Conflicts of Interest
The authors declare no competing interest.
References
- Shumway-Cook, A.; Woollacott, M.H. Motor Control: Theory and Practical Applications; Lippincqtt Williams & Wilkins: Philadelphia, PA, USA, 1995. [Google Scholar]
- Roos, M.R.; Rice, C.L.; Vandervoort, A.A. Age-related changes in motor unit function. Muscle Nerve 1997, 20, 679–690. [Google Scholar] [CrossRef]
- Desrosiers, J.; Hebert, R.; Bravo, G.; Rochette, A. Age-related changes in upper extremity performance of elderly people: A longitudinal study. Exp. Gerontol. 1999, 34, 393–405. [Google Scholar] [CrossRef] [PubMed]
- Woo, J.; Yu, R.; Wong, M.; Yeung, F.; Wong, M.; Lum, C. Frailty Screening in the Community Using the FRAIL Scale. J. Am. Med. Dir. Assoc. 2015, 16, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Mühlberg, W.; Sieber, C. Sarcopenia and frailty in geriatric patients: Implications for training and prevention. Z. Gerontol. Geriatr. 2004, 37, 2–8. [Google Scholar] [CrossRef]
- Seene, T.; Kaasik, P. Muscle weakness in the elderly: Role of sarcopenia, dynapenia, and possibilities for rehabilitation. Eur. Rev. Aging Phys. Act. 2012, 9, 109–117. [Google Scholar] [CrossRef]
- Teixeira-Santos, L.; Bobrowicz-Campos, E.; Parola, V.; Coelho, A.; Gil, I.; Almeida, M.d.L.; Apóstolo, J.L. What Is the Relationship between Lifestyle and Frailty Status? Data from the Portuguese Multicentre Descriptive Study. Nurs. Rep. 2022, 12, 39–49. [Google Scholar] [CrossRef]
- Shechtman, O.; Mann, W.C.; Justiss, M.D.; Tomita, M. Grip strength in the frail elderly. Am. J. Phys. Med. Rehabil. 2004, 83, 819–826. [Google Scholar] [CrossRef]
- Lin, C.H.; Chou, L.W.; Wei, S.H.; Lieu, F.K.; Chiang, S.L.; Sung, W.H. Influence of aging on bimanual coordination control. Exp. Gerontol. 2014, 53, 40–47. [Google Scholar] [CrossRef]
- Lee, S.C.; Wu, L.C.; Chiang, S.L.; Lu, L.H.; Chen, C.Y.; Lin, C.H.; Ni, C.H.; Lin, C.H. Validating the Capability for Measuring Age-Related Changes in Grip-Force Strength Using a Digital Hand-Held Dynamometer in Healthy Young and Elderly Adults. BioMed Res. Int. 2020, 2020, 6936879. [Google Scholar] [CrossRef]
- Lin, C.H.; Sung, W.H.; Chiang, S.L.; Lee, S.C.; Lu, L.H.; Wang, P.C.; Wang, X.M. Influence of aging and visual feedback on the stability of hand grip control in elderly adults. Exp. Gerontol. 2019, 119, 74–81. [Google Scholar] [CrossRef]
- Kao, C.-H.; Chiang, S.-L.; Chou, L.-W.; Lin, C.-H.; Lu, Y.-H.; Lu, L.-H.; Wang, X.-M.; Lin, C.-H. Validation of Vibration Exercises on Enhancing Muscle Strength and Upper Limb Functionality among Pre-Frail Community-Dwelling Older Adults. Int. J. Environ. Res. Public Health 2022, 19, 14509. [Google Scholar] [CrossRef] [PubMed]
- Lin, B.-S.; Kuo, S.-F.; Lee, I.; Lu, L.-H.; Chen, P.-Y.; Wang, P.-C.; Lai, C.-H.; Wang, X.-M.; Lin, C.-H. The impact of aging and reaching movements on grip stability control during manual precision tasks. BMC Geriatr. 2021, 21, 703. [Google Scholar] [CrossRef] [PubMed]
- Greenlund, K.J.; Keenan, N.L.; Clayton, P.F.; Pandey, D.K.; Hong, Y. Public Health Options for Improving Cardiovascular Health Among Older Americans. Am. J. Public Health 2012, 102, 1498–1507. [Google Scholar] [CrossRef] [PubMed]
- Hewett, T.E.; Ford, K.R.; Levine, P.; Page, S.J. Reaching kinematics to measure motor changes after mental practice in stroke. Top. Stroke Rehabil. 2007, 14, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Page, S.J.; Levine, P.; Leonard, A.; Szaflarski, J.P.; Kissela, B.M. Modified constraint-induced therapy in chronic stroke: Results of a single-blinded randomized controlled trial. Phys. Ther. 2008, 88, 333–340. [Google Scholar] [CrossRef]
- Cirstea, M.C.; Levin, M.F. Improvement of arm movement patterns and endpoint control depends on type of feedback during practice in stroke survivors. Neurorehabil. Neural Repair 2007, 21, 398–411. [Google Scholar] [CrossRef]
- Lai, C.H.; Sung, W.H.; Chiang, S.L.; Lu, L.H.; Lin, C.H.; Tung, Y.C.; Lin, C.H. Bimanual coordination deficits in hands following stroke and their relationship with motor and functional performance. J. Neuroeng. Rehabil. 2019, 16, 101. [Google Scholar] [CrossRef]
- Hendricks, H.T.; van Limbeek, J.; Geurts, A.C.; Zwarts, M.J. Motor recovery after stroke: A systematic review of the literature. Arch. Phys. Med. Rehabil. 2002, 83, 1629–1637. [Google Scholar] [CrossRef]
- Bogaerts, A.C.; Delecluse, C.; Claessens, A.L.; Troosters, T.; Boonen, S.; Verschueren, S.M. Effects of whole body vibration training on cardiorespiratory fitness and muscle strength in older individuals (a 1-year randomised controlled trial). Age Ageing 2009, 38, 448–454. [Google Scholar] [CrossRef]
- Pang, M.Y.; Lau, R.W.; Yip, S.P. The effects of whole-body vibration therapy on bone turnover, muscle strength, motor function, and spasticity in chronic stroke: A randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2013, 49, 439–450. [Google Scholar]
- Morel, D.S.; Marín, P.J.; Moreira-Marconi, E.; Dionello, C.F.; Bernardo-Filho, M. Can Whole-Body Vibration Exercises in Different Positions Change Muscular Activity of Upper Limbs? A Randomized Trial. Dose-Response 2018, 16, 1559325818804361. [Google Scholar] [CrossRef] [PubMed]
- Stania, M.; Juras, G.; Słomka, K.; Chmielewska, D.; Król, P. The application of whole-body vibration in physiotherapy—A narrative review. Acta Physiol. Hung. 2016, 103, 133–145. [Google Scholar] [CrossRef] [PubMed]
- Cochrane, D.J. Vibration exercise: The potential benefits. Int. J. Sports Med. 2011, 32, 75–99. [Google Scholar] [CrossRef] [PubMed]
- Alam, M.M.; Khan, A.A.; Farooq, M. Effect of whole-body vibration on neuromuscular performance: A literature review. Work 2018, 59, 571–583. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, U.; Villagra, H.A.; Oliva, L.L.; Marconi, N.F. EMG activity of upper limb on spinal cord injury individuals during whole-body vibration. Physiol. Int. 2016, 103, 361–367. [Google Scholar] [CrossRef]
- Cristino de Souza, A.L.; Mendonca, V.A.; Coelho de Oliveira, A.C.; Ferreira da Fonseca, S.; Mello Santos, L.M.; Cunha Fernandes, J.S.; Leite, H.R.; Luiz de Mendonca Martins, F.; Marcia Dos Santos, J.; de Fatima Silva, A.; et al. Whole body vibration in the static modified push-up position in untrained healthy women stimulates neuromuscular system potentiating increased handgrip myogenic response. J. Bodyw. Mov. Ther. 2020, 24, 233–238. [Google Scholar] [CrossRef]
- Jones, M.T.; Martin, J.R.; Jagim, A.R.; Oliver, J.M. Effect of Direct Whole-Body Vibration on Upper-Body Muscular Power in Recreational, Resistance-Trained Men. J. Strength Cond. Res. 2017, 31, 1371–1377. [Google Scholar] [CrossRef]
- Ashnagar, Z.; Shadmehr, A.; Hadian, M.; Talebian, S.; Jalaei, S. The effects of whole body vibration on EMG activity of the upper extremity muscles in static modified push up position. J. Back Musculoskelet. Rehabil. 2016, 29, 557–563. [Google Scholar] [CrossRef]
- Costa, V.; da Silva, F.F.; de Lima, R.M.; Mezêncio, B.; Ferreira, J.C. Mechanical Vibration Increases EMG Activity But Does Not Affect Strength Resistance Performance. J. Prof. Exerc. Physiol. 2019, 16, 120–129. [Google Scholar]
- Lee, J.S.; Kim, C.Y.; Kim, H.D. Short-Term Effects of Whole-Body Vibration Combined with Task-Related Training on Upper Extremity Function, Spasticity, and Grip Strength in Subjects with Poststroke Hemiplegia: A Pilot Randomized Controlled Trial. Am. J. Phys. Med. Rehabil. 2016, 95, 608–617. [Google Scholar] [CrossRef]
- Ahn, J.Y.; Kim, H.; Park, C.B. Effects of Whole-Body Vibration on Upper Extremity Function and Grip Strength in Patients with Subacute Stroke: A Randomised Single-Blind Controlled Trial. Occup. Ther. Int. 2019, 2019, 5820952. [Google Scholar] [CrossRef] [PubMed]
- Boo, J.A.; Moon, S.H.; Lee, S.M.; Choi, J.H.; Park, S.E. Effect of whole-body vibration exercise in a sitting position prior to therapy on muscle tone and upper extremity function in stroke patients. J. Phys. Ther. Sci. 2016, 28, 558–562. [Google Scholar] [CrossRef] [PubMed]
- Pollock, R.D.; Woledge, R.C.; Mills, K.R.; Martin, F.C.; Newham, D.J. Muscle activity and acceleration during whole body vibration: Effect of frequency and amplitude. Clin. Biomech. 2010, 25, 840–846. [Google Scholar] [CrossRef] [PubMed]
- Cardinale, M.; Wakeling, J. Whole body vibration exercise: Are vibrations good for you? Br. J. Sports Med. 2005, 39, 585–589. [Google Scholar] [CrossRef]
- Lee, G. Does whole-body vibration training in the horizontal direction have effects on motor function and balance of chronic stroke survivors? A preliminary study. J. Phys. Ther. Sci. 2015, 27, 1133–1136. [Google Scholar] [CrossRef]
- Morel, D.S.; Moreira-Marconi, E.; Neto, S.B.S.; Domingos, L.L.P.; de Souza, P.L.; Caputo, D.; Costa, G.D.; de Figueiredo, C.F.; Carmo, R.C.R.; de Paiva, P.C.; et al. Effects of Whole Body Vibration Intervention on Handgrip Strength of Brazilian Healthy Soldiers. Afr. J. Tradit. Complement. Altern. Med. 2017, 14, 28–32. [Google Scholar] [CrossRef]
- Kiiski, J.; Heinonen, A.; Jarvinen, T.L.; Kannus, P.; Sievanen, H. Transmission of vertical whole body vibration to the human body. J. Bone Miner. Res. 2008, 23, 1318–1325. [Google Scholar] [CrossRef]
- Hazell, T.J.; Jakobi, J.M.; Kenno, K.A. The effects of whole-body vibration on upper- and lower-body EMG during static and dynamic contractions. Appl. Physiol. Nutr. Metab. 2007, 32, 1156–1163. [Google Scholar] [CrossRef]
- Kurt, C.; Pekunlu, E. Acute effect of whole body vibration on isometric strength, squat jump, and flexibility in well-trained combat athletes. Biol. Sport 2015, 32, 115–122. [Google Scholar] [CrossRef]
- Cochrane, D.J.; Hawke, E.J. Effects of acute upper-body vibration on strength and power variables in climbers. J. Strength Cond. Res. 2007, 21, 527–531. [Google Scholar] [CrossRef]
- Sanudo, B.; Taiar, R.; Furness, T.; Bernardo-Filho, M. Clinical Approaches of Whole-Body Vibration Exercises in Individuals with Stroke: A Narrative Revision. Rehabil. Res. Pract. 2018, 2018, 8180901. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.; Pang, M.Y.C. Muscle activity and vibration transmissibility during whole-body vibration in chronic stroke. Scand. J. Med. Sci. Sports 2019, 29, 816–825. [Google Scholar] [CrossRef]
- Lu, J.; Xu, G.; Wang, Y. Effects of whole body vibration training on people with chronic stroke: A systematic review and meta-analysis. Top. Stroke Rehabil. 2015, 22, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.; Liao, L.R.; Pang, M.Y. Effects of whole body vibration on muscle spasticity for people with central nervous system disorders: A systematic review. Clin. Rehabil. 2017, 31, 23–33. [Google Scholar] [CrossRef]
- Bogaerts, A.; Delecluse, C.; Claessens, A.L.; Coudyzer, W.; Boonen, S.; Verschueren, S.M. Impact of whole-body vibration training versus fitness training on muscle strength and muscle mass in older men: A 1-year randomized controlled trial. J. Gerontol. A Biol. Sci. Med. Sci. 2007, 62, 630–635. [Google Scholar] [CrossRef] [PubMed]
- Bissonnette, D.R.; Weir, P.L.; Leigh, L.; Kenno, K. The Effects of a Whole-Body Advanced Vibration Exercise Program on Flexibility, Balance, and Strength in Seniors. Phys. Occup. Ther. Geriatr. 2010, 28, 225–234. [Google Scholar] [CrossRef]
- Marin, P.J.; Ferrero, C.M.; Menendez, H.; Martin, J.; Herrero, A.J. Effects of whole-body vibration on muscle architecture, muscle strength, and balance in stroke patients: A randomized controlled trial. Am. J. Phys. Med. Rehabil. 2013, 92, 881–888. [Google Scholar] [CrossRef]
- Tihanyi, T.K.; Horvath, M.; Fazekas, G.; Hortobagyi, T.; Tihanyi, J. One session of whole body vibration increases voluntary muscle strength transiently in patients with stroke. Clin. Rehabil. 2007, 21, 782–793. [Google Scholar] [CrossRef]
- Armstrong, W.J.; Nestle, H.N.; Grinnell, D.C.; Cole, L.D.; Van Gilder, E.L.; Warren, G.S.; Capizzi, E.A. The acute effect of whole-body vibration on the hoffmann reflex. J. Strength Cond. Res. 2008, 22, 471–476. [Google Scholar] [CrossRef]
- Sayenko, D.G.; Masani, K.; Alizadeh-Meghrazi, M.; Popovic, M.R.; Craven, B.C. Acute effects of whole body vibration during passive standing on soleus H-reflex in subjects with and without spinal cord injury. Neurosci. Lett. 2010, 482, 66–70. [Google Scholar] [CrossRef]
- Dias, J.A.; Ovando, A.C.; Külkamp, W.; Borges Junior, N.G. Força de preensão palmar: Métodos de avaliação e fatores que influenciam a medida. Rev. Bras. Cineantropometria Desempenho Hum. 2010, 12, 209–216. [Google Scholar]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of recommendations for SEMG sensors and sensor placement procedures. J. Electromyogr. Kinesiol. 2000, 10, 361–374. [Google Scholar] [CrossRef] [PubMed]
- Pujari, A.N.; Neilson, R.D.; Aphale, S.S.; Cardinale, M. Upper limb vibration prototype with sports and rehabilitation applications: Development, evaluation and preliminary study. Healthc. Technol. Lett. 2017, 4, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.Y.; Ju, Y.Y.; Chen, C.L.; Chuang, L.L.; Cheng, C.H. Effects of whole body vibration on spasticity and lower extremity function in children with cerebral palsy. Hum. Mov. Sci. 2015, 39, 65–72. [Google Scholar] [CrossRef]
- Lau, R.W.; Yip, S.P.; Pang, M.Y. Whole-body vibration has no effect on neuromotor function and falls in chronic stroke. Med. Sci. Sports Exerc. 2012, 44, 1409–1418. [Google Scholar] [CrossRef]
- Lee, D.K.; Han, J.W. Effects of active vibration exercise using a Flexi-Bar on balance and gait in patients with chronic stroke. J. Phys. Ther. Sci. 2018, 30, 832–834. [Google Scholar] [CrossRef][Green Version]
- Liao, L.R.; Ng, G.Y.; Jones, A.Y.; Chung, R.C.; Pang, M.Y. Effects of Vibration Intensity, Exercise, and Motor Impairment on Leg Muscle Activity Induced by Whole-Body Vibration in People With Stroke. Phys Ther. 2015, 95, 1617–1627. [Google Scholar] [CrossRef]
- Bovenzi, M. Metrics of whole-body vibration and exposure-response relationship for low back pain in professional drivers: A prospective cohort study. Int. Arch. Occup. Environ. Health 2009, 82, 893–917. [Google Scholar] [CrossRef]
- Cardinale, M.; Lim, J. The acute effects of two different whole body vibration frequencies on vertical jump performance. Med. Dello Sport 2003, 56, 287–292. [Google Scholar]
- Hwang, K.J.; Ryu, Y.U. Whole body vibration may have immediate adverse effects on the postural sway of stroke patients. J. Phys. Ther. Sci. 2016, 28, 473–477. [Google Scholar] [CrossRef]
- Liao, L.R.; Ng, G.Y.; Jones, A.Y.; Huang, M.Z.; Pang, M.Y. Whole-Body Vibration Intensities in Chronic Stroke: A Randomized Controlled Trial. Med. Sci. Sports Exerc. 2016, 48, 1227–1238. [Google Scholar] [CrossRef] [PubMed]
- Nawayseh, N.; Sinan, H.A.; Alteneiji, S.; Hamdan, S. Effect of gender on the biodynamic responses to vibration induced by a whole-body vibration training machine. Proc. Inst. Mech. Eng. H—J. Eng. Med. 2019, 233, 383–392. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).