
Neutrophil-to-Lymphocyte Ratio Is Not Associated with Severity of Coronary Artery Disease and Is Not Correlated with Vitamin D Level in Patients with a History of an Acute Coronary Syndrome

 ,
,  , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Population
2.2. Comorbidities Assessment
2.3. Coronary Angiography
2.4. Statistical Analysis
3. Results
3.1. Participants’ Characteristics
3.2. Difference in NLR between Patients with Stable CAD and Patients with ACS
3.3. Association between NLR and Severity of CAD
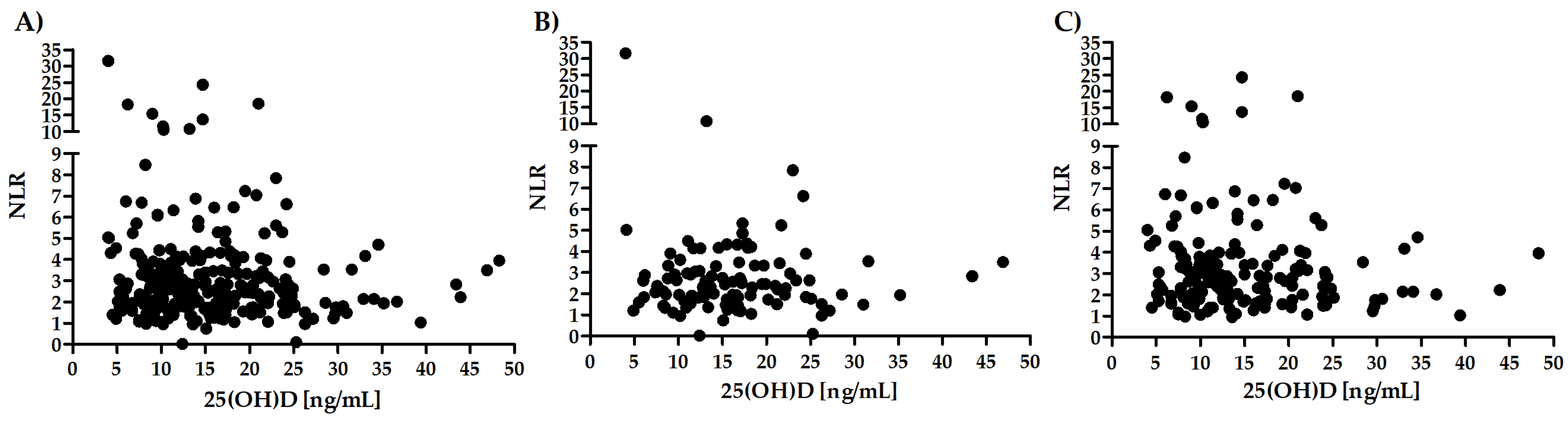
3.4. Correlation between Vitamin D Levels and NLR
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organisation. Global Health Estimates: Life Expectancy and Leading Causes of Death and Disability. Available online: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates (accessed on 30 March 2022).
- Barron, H.V.; Cannon, C.P.; Murphy, S.A.; Braunwald, E.; Gibson, C.M. Association between white blood cell count, epicardial blood flow, myocardial perfusion, and clinical outcomes in the setting of acute myocardial infarction: A thrombolysis in myocardial infarction 10 substudy. Circulation 2000, 102, 2329–2334. [Google Scholar] [CrossRef]
- Park, S.H. Regulation of Macrophage Activation and Differentiation in Atherosclerosis. J. Lipid Atheroscler. 2021, 10, 251–267. [Google Scholar] [CrossRef] [PubMed]
- Moriya, J. Critical roles of inflammation in atherosclerosis. J. Cardiol. 2019, 73, 22–27. [Google Scholar] [CrossRef] [Green Version]
- Pasceri, V.; Willerson, J.T.; Yeh, E.T. Direct proinflammatory effect of C-reactive protein on human endothelial cells. Circulation 2000, 102, 2165–2168. [Google Scholar] [CrossRef]
- Uzui, H.; Harpf, A.; Liu, M.; Doherty, T.M.; Shukla, A.; Chai, N.-N.; Tripathi, P.V.; Jovinge, S.; Wilkin, D.J.; Asotra, K.; et al. Increased expression of membrane type 3-matrix metalloproteinase in human atherosclerotic plaque: Role of activated macrophages and inflammatory cytokines. Circulation 2002, 106, 3024–3030. [Google Scholar] [CrossRef] [Green Version]
- Blaschke, F.; Bruemmer, D.; Yin, F.; Takata, Y.; Wang, W.; Fishbein, M.C.; Okura, T.; Higaki, J.; Graf, K.; Fleck, E.; et al. C-reactive protein induces apoptosis in human coronary vascular smooth muscle cells. Circulation 2004, 110, 579–587. [Google Scholar] [CrossRef]
- Möckel, M.; Danne, O.; Müller, R.; Vollert, J.O.; Müller, C.; Lueders, C.; Störk, T.; Frei, U.; Koenig, W.; Dietz, R.; et al. Development of an optimized multimarker strategy for early risk assessment of patients with acute coronary syndromes. Clin. Chim. Acta 2008, 393, 103–109. [Google Scholar] [CrossRef]
- Lemos, J.A.; Morrow, D.A.; Blazing, M.A.; Jarolim, P.; Wiviott, S.D.; Sabatine, M.S.; Califf, R.M.; Braunwald, E. Serial measurement of monocyte chemoattractant protein-1 after acute coronary syndromes: Results from the A to Z trial. J. Am. Coll. Cardiol. 2007, 50, 2117–2124. [Google Scholar] [CrossRef] [Green Version]
- Hatmi, Z.N.; Saeid, A.K.; Broumand, M.A.; Khoshkar, S.N.; Danesh, Z.F. Multiple inflammatory prognostic factors in acute coronary syndromes: A prospective inception cohort study. Acta Med. Iran. 2010, 48, 51–57. [Google Scholar]
- Ikonomidis, I.; Michalakeas, C.A.; Parissis, J.; Paraskevaidis, I.; Ntai, K.; Papadakis, I.; Anastasiou-Nana, M.; Lekakis, J. Inflammatory markers in coronary artery disease. BioFactors 2012, 38, 320–328. [Google Scholar] [CrossRef]
- Sabatine, M.S.; Morrow, D.A.; Cannon, C.P.; Murphy, S.A.; Demopoulos, L.A.; DiBattiste, P.M.; McCabe, C.H.; Braunwald, E.; Gibson, C.M. Relationship between baseline white blood cell count and degree of coronary artery disease and mortality in patients with acute coronary syndromes. J. Am. Coll. Cardiol. 2002, 40, 1761–1768. [Google Scholar] [CrossRef] [Green Version]
- Wolf, D.; Ley, K. Immunity and Inflammation in Atherosclerosis. Circ. Res. 2019, 124, 315–327. [Google Scholar] [CrossRef]
- Soehnlein, O. Multiple roles for neutrophils in atherosclerosis. Circ. Res. 2012, 110, 875–888. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawaguchi, H.; Mori, T.; Kawano, T.; Kono, S.; Sasaki, J.; Arakawa, K. Band neutrophil count and the presence and severity of coronary atherosclerosis. Am. Heart J. 1996, 132, 9–12. [Google Scholar] [CrossRef]
- Haybar, H.; Pezeshki, S.M.S.; Saki, N. Evaluation of complete blood count parameters in cardiovascular diseases: An early indicator of prognosis? Exp. Mol. Pathol. 2019, 110, 104267. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.D.; Folsom, A.R.; Nieto, F.J.; Chambless, L.E.; Shahar, E.; Wolfe, D.A. White blood cell count and incidence of coronary heart disease and ischemic stroke and mortality from cardiovascular disease in African-American and White men and women: Atherosclerosis risk in communities study. Am. J. Epidemiol. 2001, 154, 758–764. [Google Scholar] [CrossRef]
- Bressi, E.; Mangiacapra, F.; Ricottini, E.; Cavallari, I.; Colaiori, I.; Di Gioia, G.; Creta, A.; Capuano, M.; Viscusi, M.M.; Di Sciascio, G. Impact of Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio on 5-Year Clinical Outcomes of Patients with Stable Coronary Artery Disease Undergoing Elective Percutaneous Coronary Intervention. J. Cardiovasc. Transl. Res. 2018, 11, 517–523. [Google Scholar] [CrossRef]
- Kaya, H.; Ertaş, F.; İslamoğlu, Y.; Kaya, Z.; Atılgan, Z.A.; Çil, H.; Çalışkan, A.; Aydın, M.; Oylumlu, M.; Soydinç, M.S. Association between neutrophil to lymphocyte ratio and severity of coronary artery disease. Clin. Appl. Thromb. Hemost. 2014, 20, 50–54. [Google Scholar] [CrossRef] [Green Version]
- Song, M.; Graubard, B.I.; Rabkin, C.S.; Engels, E.A. Neutrophil-to-lymphocyte ratio and mortality in the United States general population. Sci. Rep. 2021, 11, 464. [Google Scholar] [CrossRef]
- Turak, O.; Ozcan, F.; Isleyen, A.; Tok, D.; Sokmen, E.; Buyukkaya, E.; Aydogdu, S.; Akpek, M.; Kaya, M.G. Usefulness of the neutrophil-to-lymphocyte ratio to predict bare-metal stent restenosis. Am. J. Cardiol. 2012, 110, 1405–1410. [Google Scholar] [CrossRef]
- Rosen, C.J.; Adams, J.S.; Bikle, D.D.; Black, D.M.; Demay, M.B.; Manson, J.E.; Murad, M.H.; Kovacs, C.S. The nonskeletal effects of vitamin D: An Endocrine Society scientific statement. Endocr. Rev. 2012, 33, 456–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kassi, E.; Adamopoulos, C.; Basdra, E.K.; Papavassiliou, A.G. Role of vitamin D in atherosclerosis. Circulation 2013, 128, 2517–2531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bishop, E.; Ismailova, A.; Dimeloe, S.K.; Hewison, M.; White, J.H. Vitamin D and immune regulation: Antibacterial, antiviral, anti-inflammatory. JBMR Plus 2020, 5, e10405. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [Green Version]
- Moradi, M.; Foroutanfar, A. Evaluation of vitamin D levels in relation to coronary CT angiographic findings in an Iranian population. Vasc. Health Risk Manag. 2017, 13, 361–367. [Google Scholar] [CrossRef] [Green Version]
- Wu, Z.; Wang, T.; Zhu, S.; Li, L. Effects of vitamin D supplementation as an adjuvant therapy in coronary artery disease patients. Scand. Cardiovasc. J. 2016, 50, 9–16. [Google Scholar] [CrossRef]
- Dai, L.; Liu, M.; Chen, L. Association of Serum 25-Hydroxyvitamin D Concentrations With All-Cause and Cause-Specific Mortality Among Adult Patients With Existing Cardiovascular Disease. Front. Nutr. 2021, 8, 740855. [Google Scholar] [CrossRef]
- Scragg, R.; Stewart, A.W.; Waayer, D.; Lawes, C.M.M.; Toop, L.; Sluyter, J.; Murphy, J.; Khaw, K.-T.; Camargo, C.A. Effect of Monthly High-Dose Vitamin D Supplementation on Cardiovascular Disease in the Vitamin D Assessment Study: A Randomized Clinical Trial. JAMA Cardiol. 2017, 2, 608–616. [Google Scholar] [CrossRef] [Green Version]
- Akin, F.; Ayça, B.; Köse, N.; Duran, M.; Sari, M.; Uysal, O.K.; Karakukcu, C.; Arinc, H.; Covic, A.; Goldsmith, D.; et al. Serum vitamin D levels are independently associated with severity of coronary artery disease. J. Investig. Med. 2012, 60, 869–873. [Google Scholar] [CrossRef]
- Chen, W.R.; Qian, Y.; Chen, Y.D.; Shi, Y.; Da Yin, W.; Wang, H.; Zhu, P.; Liu, H.W.; Sha, Y. The effects of low vitamin D on coronary artery disease. Heart Lung Circ. 2014, 23, 314–319. [Google Scholar] [CrossRef]
- Sokol, S.I.; Srinivas, V.; Crandall, J.P.; Kim, M.; Tellides, G.; Lebastchi, A.H.; Lebastchi, A.; Yu, Y.; Gupta, A.K.; Alderman, M.H. The effects of vitamin D repletion on endothelial function and inflammation in patients with coronary artery disease. Vasc. Med. 2012, 17, 394–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ostadmohammadi, V.; Milajerdi, A.; Ghayour-Mobarhan, M.; Ferns, G.; Taghizadeh, M.; Badehnoosh, B.; Mirzaei, H.; Asemi, Z. The Effects of Vitamin D Supplementation on Glycemic Control, Lipid Profiles and C-Reactive Protein Among Patients with Cardiovascular Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Curr. Pharm. Des. 2019, 25, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Dobnig, H.; Pilz, S.; Scharnagl, H.; Renner, W.; Seelhorst, U.; Wellnitz, B.; Kinkeldei, J.; Boehm, B.O.; Weihrauch, G.; Maerz, W. Independent association of low serum 25-hydroxyvitamin d and 1,25-dihydroxyvitamin d levels with all-cause and cardiovascular mortality. Arch. Intern. Med. 2008, 168, 1340–1349. [Google Scholar] [CrossRef] [PubMed]
- Verdoia, M.; Nardin, M.; Rolla, R.; Negro, F.; Gioscia, R.; Afifeh, A.M.S.; Viglione, F.; Suryapranata, H.; Marcolongo, M.; Luca, G. Association of lower vitamin D levels with inflammation and leucocytes parameters in patients with and without diabetes mellitus undergoing coronary angiography. Eur. J. Clin. Invest. 2021, 51, e13439. [Google Scholar] [CrossRef]
- Murr, C.; Pilz, S.; Grammer, T.B.; Kleber, M.E.; Meinitzer, A.; Boehm, B.O.; Marz, W.; Fuchs, D. Vitamin D deficiency parallels inflammation and immune activation, the Ludwigshafen Risk and Cardiovascular Health (LURIC) study. Clin. Chem. Lab. Med. 2012, 50, 2205–2212. [Google Scholar] [CrossRef]
- Dziedzic, E.A.; Gąsior, J.S.; Sowińska, I.; Dąbrowski, M.; Jankowski, P. Vitamin D Level in Patients with Consecutive Acute Coronary Syndrome Is Not Correlated with the Parameters of Platelet Activity. J. Clin. Med. 2022, 11, 707. [Google Scholar] [CrossRef]
- Dziedzic, E.A.; Gasior, J.S.; Saniewski, T.; Dabrowski, M. Vitamin D deficiency among Polish patients with angiographically confirmed coronary heart disease. Pol. Merkur. Lekarski 2021, 49, 278–282. [Google Scholar]
- Dziedzic, E.A.; Przychodzeń, S.; Dąbrowski, M. The effects of vitamin D on severity of coronary artery atherosclerosis and lipid profile of cardiac patients. Arch. Med. Sci. 2016, 12, 1199–1206. [Google Scholar] [CrossRef] [Green Version]
- Dziedzic, E.A.; Smyk, W.; Sowińska, I.; Dąbrowski, M.; Jankowski, P. Serum Level of Vitamin D Is Associated with Severity of Coronary Atherosclerosis in Postmenopausal Women. Biology 2021, 10, 1139. [Google Scholar] [CrossRef]
- Dziedzic, E.A.; Gąsior, J.S.; Pawłowski, M.; Wodejko-Kucharska, B.; Saniewski, T.; Marcisz, A.; Dąbrowski, M.J. Vitamin D level is associated with severity of coronary artery atherosclerosis and incidence of acute coronary syndromes in non-diabetic cardiac patients. Arch. Med. Sci. 2019, 15, 359–368. [Google Scholar] [CrossRef]
- Dziedzic, E.A.; Gąsior, J.S.; Pawłowski, M.; Dąbrowski, M. Association of Vitamin D Deficiency and Degree of Coronary Artery Disease in Cardiac Patients with Type 2 Diabetes. J. Diabetes Res. 2017, 2017, 3929075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yumuk, V.; Tsigos, C.; Fried, M.; Schindler, K.; Busetto, L.; Micic, D.; Toplak, H. European Guidelines for Obesity Management in Adults. Obes. Facts 2015, 8, 402–424. [Google Scholar] [CrossRef] [PubMed]
- Stergiou, G.S.; Palatini, P.; Parati, G.; O’Brien, E.; Januszewicz, A.; Lurbe, E.; Persu, A.; Mancia, G.; Kreutz, R. 2021 European Society of Hypertension practice guidelines for office and out-of-office blood pressure measurement. J. Hypertens. 2021, 39, 1293–1302. [Google Scholar] [CrossRef] [PubMed]
- Cosentino, F.; Grant, P.J.; Aboyans, V.; Bailey, C.J.; Ceriello, A.; Delgado, V.; Federici, M.; Filippatos, G.; Grobbee, D.E.; Hansen, T.B.; et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur. Heart J. 2020, 41, 255–323. [Google Scholar] [CrossRef] [Green Version]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; de Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef]
- Krzywanski, J.; Mikulski, T.; Krysztofiak, H.; Mlynczak, M.; Gaczynska, E.; Ziemba, A. Seasonal Vitamin D Status in Polish Elite Athletes in Relation to Sun Exposure and Oral Supplementation. PLoS ONE 2016, 11, e0164395. [Google Scholar] [CrossRef]
- Abdel-Wareth, L.; Haq, A.; Turner, A.; Khan, S.; Salem, A.; Mustafa, F.; Hussein, N.; Pallinalakam, F.; Grundy, L.; Patras, G.; et al. Total vitamin D assay comparison of the Roche Diagnostics “Vitamin D total” electrochemiluminescence protein binding assay with the Chromsystems HPLC method in a population with both D2 and D3 forms of vitamin D. Nutrients 2013, 5, 971–980. [Google Scholar] [CrossRef]
- Knudsen, C.S.; Nexo, E.; Højskov, C.S.; Heickendorff, L. Analytical validation of the Roche 25-OH Vitamin D Total assay. Clin. Chem. Lab. Med. 2012, 50, 1965–1968. [Google Scholar] [CrossRef]
- Trimboli, F.; Rotundo, S.; Armili, S.; Mimmi, S.; Lucia, F.; Montenegro, N.; Antico, G.C.; Cerra, A.; Gaetano, M.; Galato, F.; et al. Serum 25-hydroxyvitamin D measurement: Comparative evaluation of three automated immunoassays. Pract. Lab. Med. 2021, 26, e00251. [Google Scholar] [CrossRef]
- Sahota, O. Understanding vitamin D deficiency. Age Ageing 2014, 43, 589–591. [Google Scholar] [CrossRef] [Green Version]
- Al-Khalidi, B.; Kimball, S.M.; Rotondi, M.A.; Ardern, C.I. Standardized serum 25-hydroxyvitamin D concentrations are inversely associated with cardiometabolic disease in U.S. adults: A cross-sectional analysis of NHANES, 2001–2010. Nutr. J. 2017, 16, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engelsen, O. The relationship between ultraviolet radiation exposure and vitamin D status. Nutrients 2010, 2, 482–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawton, J.S.; Tamis-Holland, J.E.; Bangalore, S.; Bates, E.R.; Beckie, T.M.; Bischoff, J.M.; Bittl, J.A.; Cohen, M.G.; DiMaio, J.M.; Don, C.W.; et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2022, 79, e21–e129. [Google Scholar] [CrossRef]
- Collet, J.-P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef]
- Monteiro Júnior, J.G.d.M.; Torres, D.d.O.C.; Da Silva, M.C.F.C.; Ramos, T.M.d.B.; Alves, M.L.; Nunes Filho, W.J.; Damasceno, E.P.; Brunet, A.F.; Bittencourt, M.S.; Pedrosa, R.P.; et al. Nucleated Red Blood Cells as Predictors of All-Cause Mortality in Cardiac Intensive Care Unit Patients: A Prospective Cohort Study. PLoS ONE 2015, 10, e0144259. [Google Scholar] [CrossRef] [PubMed]
- Fan, L.; Gui, L.; Chai, E.-Q.; Wei, C.-J. Routine hematological parameters are associated with short- and long-term prognosis of patients with ischemic stroke. J. Clin. Lab. Anal. 2018, 32, e22244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Núñez, J.; Núñez, E.; Bodí, V.; Sanchis, J.; Mainar, L.; Miñana, G.; Fácila, L.; Bertomeu, V.; Merlos, P.; Darmofal, H.; et al. Low lymphocyte count in acute phase of ST-segment elevation myocardial infarction predicts long-term recurrent myocardial infarction. Coronary Artery Dis. 2010, 21, 1–7. [Google Scholar] [CrossRef]
- Maxwell, S.R.J.; Lip, G.Y.H. Reperfusion injury: A review of the pathophysiology, clinical manifestations and therapeutic options. Int. J. Cardiol. 1997, 58, 95–117. [Google Scholar] [CrossRef]
- Sheridan, F.M.; Cole, P.G.; Ramage, D. Leukocyte adhesion to the coronary microvasculature during ischemia and reperfusion in an in vivo canine model. Circulation 1996, 93, 1784–1787. [Google Scholar] [CrossRef]
- Bhat, T.; Teli, S.; Rijal, J.; Bhat, H.; Raza, M.; Khoueiry, G.; Meghani, M.; Akhtar, M.; Costantino, T. Neutrophil to lymphocyte ratio and cardiovascular diseases: A review. Expert Rev. Cardiovasc. Ther. 2013, 11, 55–59. [Google Scholar] [CrossRef]
- Verdoia, M.; Barbieri, L.; Di Giovine, G.; Marino, P.; Suryapranata, H.; Luca, G. Neutrophil to Lymphocyte Ratio and the Extent of Coronary Artery Disease: Results From a Large Cohort Study. Angiology 2016, 67, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Uysal, H.B.; Dağlı, B.; Akgüllü, C.; Avcil, M.; Zencir, C.; Ayhan, M.; Sönmez, H.M. Blood count parameters can predict the severity of coronary artery disease. Korean J. Intern. Med. 2016, 31, 1093–1100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Ji, Y.; Kang, J.; Fang, N. Association between blood neutrophil-to-lymphocyte ratio and severity of coronary artery disease: Evidence from 17 observational studies involving 7017 cases. Medicine 2018, 97, e12432. [Google Scholar] [CrossRef] [PubMed]
- Maleki, M.; Tajlil, A.; Separham, A.; Sohrabi, B.; Pourafkari, L.; Roshanravan, N.; Aslanabadi, N.; Najjarian, F.; Mashayekhi, S.; Ghaffari, S. Association of neutrophil to lymphocyte ratio (NLR) with angiographic SYNTAX score in patients with non-ST-Segment elevation acute coronary syndrome (NSTE-ACS). J. Cardiovasc. Thorac. Res. 2021, 13, 216–221. [Google Scholar] [CrossRef]
- Li, D.-b.; Hua, Q.; Liu, Z.; Li, J.; Xu, L.-q.; Wang, S.; Jin, W.-y. Association between inflammatory mediators and angiographic morphologic features indicating thrombus formation in patients with acute myocardial infarction. Chin. Med. J.-Peking 2009, 122, 1738–1742. [Google Scholar]
- Nalbant, A.; Cinemre, H.; Kaya, T.; Varim, C.; Varim, P.; Tamer, A. Neutrophil to lymphocyte ratio might help prediction of acute myocardial infarction in patients with elevated serum creatinine. Pak. J. Med. Sci. 2016, 32, 106–110. [Google Scholar] [CrossRef]
- Ipek, G.; Onuk, T.; Karatas, M.B.; Güngör, B.; Atasoy, I.; Murat, A.; Aldag, M.; Yelgec, N.S.; Dayi, S.U.; Bolca, O. Relationship between Neutrophil-to-Lymphocyte Ratio and Left Ventricular Free Wall Rupture in Acute Myocardial Infarction. Cardiology 2015, 132, 105–110. [Google Scholar] [CrossRef]
- Pan, W.; Zhao, D.; Zhang, C.; Li, W.; Yu, J.; Wang, S.; Li, Z.; Wang, Z.; Sun, X.; Liu, H.; et al. Application of neutrophil/lymphocyte ratio in predicting coronary blood flow and mortality in patients with ST-elevation myocardial infarction undergoing percutaneous coronary intervention. J. Cardiol. 2015, 66, 9–14. [Google Scholar] [CrossRef] [Green Version]
- Chatterjee, S.; Chandra, P.; Guha, G.; Kalra, V.; Chakraborty, A.; Frankel, R.; Shani, J. Pre-procedural Elevated White Blood Cell Count and Neutrophil-Lymphocyte (N/L) Ratio are Predictors of Ventricular Arrhythmias During Percutaneous Coronary Intervention. Cardiovasc. Hematol. Disord. Drug Targets 2011, 11, 58–60. [Google Scholar] [CrossRef]
- Poludasu, S.; Cavusoglu, E.; Khan, W.; Marmur, J.D. Neutrophil to lymphocyte ratio as a predictor of long-term mortality in African Americans undergoing percutaneous coronary intervention. Clin. Cardiol. 2009, 32, E6–E10. [Google Scholar] [CrossRef]
- Cho, K.H.; Jeong, M.H.; Ahmed, K.; Hachinohe, D.; Choi, H.S.; Chang, S.Y.; Kim, M.C.; Hwang, S.H.; Park, K.-H.; Lee, M.G.; et al. Value of early risk stratification using hemoglobin level and neutrophil-to-lymphocyte ratio in patients with ST-elevation myocardial infarction undergoing primary percutaneous coronary intervention. Am. J. Cardiol. 2011, 107, 849–856. [Google Scholar] [CrossRef] [PubMed]
- Gibson, P.H.; Cuthbertson, B.H.; Croal, B.L.; Rae, D.; El-Shafei, H.; Gibson, G.; Jeffrey, R.R.; Buchan, K.G.; Hillis, G.S. Usefulness of neutrophil/lymphocyte ratio as predictor of new-onset atrial fibrillation after coronary artery bypass grafting. Am. J. Cardiol. 2010, 105, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Benites-Zapata, V.A.; Hernandez, A.V.; Nagarajan, V.; Cauthen, C.A.; Starling, R.C.; Tang, W.H.W. Usefulness of neutrophil-to-lymphocyte ratio in risk stratification of patients with advanced heart failure. Am. J. Cardiol. 2015, 115, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Akbas, E.M.; Gungor, A.; Ozcicek, A.; Akbas, N.; Askin, S.; Polat, M. Vitamin D and inflammation: Evaluation with neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio. Arch. Med. Sci. 2016, 12, 721–727. [Google Scholar] [CrossRef]
- Bouillon, R.; Carmeliet, G.; Verlinden, L.; van Etten, E.; Verstuyf, A.; Luderer, H.F.; Lieben, L.; Mathieu, C.; Demay, M. Vitamin D and human health: Lessons from vitamin D receptor null mice. Endocr. Rev. 2008, 29, 726–776. [Google Scholar] [CrossRef]
- Shah, A.K.; Dhalla, N.S. Effectiveness of Some Vitamins in the Prevention of Cardiovascular Disease: A Narrative Review. Front. Physiol. 2021, 12, 729255. [Google Scholar] [CrossRef]
- Ng, L.L.; Sandhu, J.K.; Squire, I.B.; Davies, J.E.; Jones, D.J.L. Vitamin D and prognosis in acute myocardial infarction. Int. J. Cardiol. 2013, 168, 2341–2346. [Google Scholar] [CrossRef]
- Ross, R. Atherosclerosis—An inflammatory disease. N. Engl. J. Med. 1999, 340, 115–126. [Google Scholar] [CrossRef]
- Aktürk, S.; Büyükavcı, R. Evaluation of blood neutrophil-lymphocyte ratio and platelet distribution width as inflammatory markers in patients with fibromyalgia. Clin. Rheumatol. 2017, 36, 1885–1889. [Google Scholar] [CrossRef]
- Cataudella, E.; Giraffa, C.M.; Di Marca, S.; Pulvirenti, A.; Alaimo, S.; Pisano, M.; Terranova, V.; Corriere, T.; Ronsisvalle, M.L.; Di Quattro, R.; et al. Neutrophil-To-Lymphocyte Ratio: An Emerging Marker Predicting Prognosis in Elderly Adults with Community-Acquired Pneumonia. J. Am. Geriatr. Soc. 2017, 65, 1796–1801. [Google Scholar] [CrossRef]
- Lee, H.; Kim, I.; Kang, B.H.; Um, S.-J. Prognostic value of serial neutrophil-to-lymphocyte ratio measurements in hospitalized community-acquired pneumonia. PLoS ONE 2021, 16, e0250067. [Google Scholar] [CrossRef] [PubMed]
- Ruta, V.M.; Man, A.M.; Alexescu, T.G.; Motoc, N.S.; Tarmure, S.; Ungur, R.A.; Todea, D.A.; Coste, S.C.; Valean, D.; Pop, M.C. Neutrophil-To-Lymphocyte Ratio and Systemic Immune-Inflammation Index-Biomarkers in Interstitial Lung Disease. Medicina 2020, 56, 381. [Google Scholar] [CrossRef] [PubMed]
- Taşoğlu, Ö.; Bölük, H.; Şahin Onat, Ş.; Taşoğlu, İ.; Özgirgin, N. Is blood neutrophil-lymphocyte ratio an independent predictor of knee osteoarthritis severity? Clin. Rheumatol. 2016, 35, 1579–1583. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Variable | Values |
|---|---|
| Age [years] | 67.0 ± 11.2 |
| BMI [kg/m2] | 28.0 ± 4.4 |
| Diabetes mellitus [yes/pre-diabetes/no] | 100/10/158 |
| Hyperlipidemia [yes/no] | 145/107 |
| Hypertension [yes/no] | 233/35 |
| Smoking [active/former smoker/no] | 85/28/155 |
| Season during the examination [November to April/May to October] | 200/68 |
| CASSS [0/1/2/3] | 13/79/83/93 |
| Serum 25(OH)D [ng/mL] | 14.0 (4.0–48.3) |
| Neutrophils [thousand cells/µL] | 4.9 (1.4–23.8) |
| Lymphocytes [thousand cells/µL] | 1.9 (0.3–189.0) |
| NLR | 2.6 (0.03–31.6) |
| Variable | Stable CAD | ACS | p-Value |
|---|---|---|---|
| Number of participants | 108 | 160 | - |
| Sex (♀/♂) | 27/81 | 60/100 | <0.05 |
| Age (years) | 68.4 ± 9.4 | 66.1 ± 12.2 | 0.10 |
| BMI (kg/m2) | 27.7 ± 4.3 | 28.3 ± 4.6 | 0.34 |
| BMI class (1/2/3) * | 28/52/28 | 33/59/47 | 0.41 |
| Diabetes (No/Yes/prediabetes) | 63/36/9 | 95/64/1 | <0.01 |
| TC (mg/dL) | 162.5 (84.8–327.3) | 171.9 (70.9–338.3) | 0.07 |
| HDL (mg/dL) | 46.5 (14.6–113.2) | 44.5 (19.5–92.9) | 0.11 |
| LDL (mg/dL) | 81.9 (27.3–257.9) | 101.4 (24.4–244.3) | <0.05 |
| TG (mg/dL) | 111.8 (37.9–417.0) | 115.4 (42.6–391.8) | 0.58 |
| Hyperlipidemia (No/Yes) | 54/50 | 53/95 | <0.05 |
| Hypertension (No/Yes) | 15/93 | 20/140 | 0.74 |
| Smoking (No/Yes/Ex-smokers) | 62/24/22 | 93/61/6 | <0.001 |
| CASSS (0/1/2/3) | 6/25/39/38 | 7/54/44/55 | 0.24 |
| Serum 25(OH)D (ng/mL) | 15.8 (4.0–46.9) | 13.1 (4.0–48.3) | <0.05 |
| Season of the examination (November to April/May to October) | 78/30 | 122/38 | 0.46 |
| NLR | CASSS | |||
|---|---|---|---|---|
| 0 | 1 | 2 | 3 | |
| All patients | 2.9 (1.1–31.6) | 2.4 (1.0–24.3) | 2.4 (0.03–18.2) | 2.7 (1.0–11.6) |
| Stable CAD | 2.5 (1.1–31.6) | 2.4 (1.0–7.9) | 2.0 (0.03–5.3) | 2.5 (1.2–10.8) |
| ACS | 2.9 (2.2–18.6) | 2.4 (1.0–24.3) | 2.6 (1.1–18.2) | 3.1 (1.0–11.6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dziedzic, E.A.; Gąsior, J.S.; Tuzimek, A.; Dąbrowski, M.; Jankowski, P. Neutrophil-to-Lymphocyte Ratio Is Not Associated with Severity of Coronary Artery Disease and Is Not Correlated with Vitamin D Level in Patients with a History of an Acute Coronary Syndrome. Biology 2022, 11, 1001. https://doi.org/10.3390/biology11071001
Dziedzic EA, Gąsior JS, Tuzimek A, Dąbrowski M, Jankowski P. Neutrophil-to-Lymphocyte Ratio Is Not Associated with Severity of Coronary Artery Disease and Is Not Correlated with Vitamin D Level in Patients with a History of an Acute Coronary Syndrome. Biology. 2022; 11(7):1001. https://doi.org/10.3390/biology11071001
Chicago/Turabian StyleDziedzic, Ewelina A., Jakub S. Gąsior, Agnieszka Tuzimek, Marek Dąbrowski, and Piotr Jankowski. 2022. "Neutrophil-to-Lymphocyte Ratio Is Not Associated with Severity of Coronary Artery Disease and Is Not Correlated with Vitamin D Level in Patients with a History of an Acute Coronary Syndrome" Biology 11, no. 7: 1001. https://doi.org/10.3390/biology11071001
APA StyleDziedzic, E. A., Gąsior, J. S., Tuzimek, A., Dąbrowski, M., & Jankowski, P. (2022). Neutrophil-to-Lymphocyte Ratio Is Not Associated with Severity of Coronary Artery Disease and Is Not Correlated with Vitamin D Level in Patients with a History of an Acute Coronary Syndrome. Biology, 11(7), 1001. https://doi.org/10.3390/biology11071001