
The First Evaluation of Serum Levels of MGP, Gas6 and EGFR after First Dose of Chemotherapy in Lung Cancer

 ,
,  , and
, and
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Exclusion Criteria
2.3. Sample Preparation and Determination
CT Evaluation
2.4. Statistical Analysis
3. Results
3.1. General Characteristics of the Study Group
3.2. Biochemical and Hematological Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Globocan 2020. Lung Cancer. Available online: https://gco.iarc.fr/today/data/factsheets/cancers/15-Lung-fact-sheet.pdf (accessed on 10 October 2021).
- Murtaza, M.; Dawson, S.J.; Tsui, D.W.; Gale, D.; Forshew, T.; Piskorz, A.M.; Parkinson, C.; Chin, S.F.; Kingsbury, Z.; Wong, A.S.; et al. Non-invasive analysis of acquired resistance to cancer therapy by sequencing of plasma DNA. Nature 2013, 497, 108–112. [Google Scholar] [CrossRef]
- Rodriguez-Canales, J.; Parra-Cuentas, E.; Wistuba, I.I. Diagnosis and Molecular Classification of Lung Cancer. Cancer Treat Res. 2016, 170, 25–46. [Google Scholar] [CrossRef]
- Wen, L.; Chen, J.; Duan, L.; Li, S. Vitamin K-dependent proteins involved in bone and cardiovascular health (Review). Mol. Med. Rep. 2018, 18, 3–15. [Google Scholar] [CrossRef]
- Danziger, J. Vitamin K-dependent proteins, warfarin, and vascular calcification. Clin. J. Am. Soc. Nephrol. 2008, 3, 1504–1510. [Google Scholar] [CrossRef] [PubMed]
- O'Connor, E.M.; Durack, E. Osteocalcin: The extra-skeletal role of a vitamin K-dependent protein in glucose metabolism. J. Nutr. Interm. Metab. 2017, 7, 8–13. [Google Scholar] [CrossRef]
- Xiao, H.; Chen, J.; Duan, L.; Li, S. Role of emerging vitamin K-dependent proteins: Growth arrest-specific protein 6, Gla-rich protein and periostin (Review). Int. J. Mol. Med. 2021, 47, 2. [Google Scholar] [CrossRef] [PubMed]
- Hou, Y.; Guo, H.; Guo, Y.; Zhang, Y.; Han, H. Preliminary Study on the Biological Markers for I-IIb Stage Non-small Cell Lung Cancer Based on a Serum-peptidomics. Zhongguo Fei Ai Za Zhi 2019, 22, 20–25. [Google Scholar] [CrossRef]
- Ahn, H.H.; Carrington, C.; Hu, Y.; Liu, H.W.; Ng, C.; Nam, H.; Park, A.; Stace, C.; West, W.; Mao, H.Q.; et al. Nanoparticle-mediated tumor cell expression of mIL-12 via systemic gene delivery treats syngeneic models of murine lung cancers. Sci. Rep. 2021, 11, 9733. [Google Scholar] [CrossRef]
- Gopalakrishnan, R.; Ouyang, H.; Somerman, M.J.; McCauley, L.K.; Franceschi, R. Matrix gamma-carboxyglutamic acid protein is a key regulator of PTH-mediated inhibition of mineralization in MC3T3-E1 osteoblast-like cells. Endocrinology 2001, 142, 4379–4388. [Google Scholar] [CrossRef]
- De Brouwer, B.; Piscaer, I.; Von Der Thusen, J.H.; Grutters, J.C.; Schutgens, R.E.; Wouters, E.F.; Janssen, R. Should vitamin K be supplemented instead of antagonised in patients with idiopathic pulmonary fibrosis? Expert. Rev. Respir. Med. 2018, 12, 169–175. [Google Scholar] [CrossRef]
- Levedakou, E.N.; Strohmeyer, T.G.; Effert, P.J.; Liu, E.T. Expression of the matrix Gla protein in urogenital malignancies. Int. J. Cancer 1992, 52, 534–537. [Google Scholar] [CrossRef]
- Zandueta, C.; Ormazábal, C.; Perurena, N.; Martínez-Canarias, S.; Zalacaín, M.; Julián, M.S.; Grigoriadis, A.E.; Valencia, K.; Campos-Laborie, F.J.; Rivas, J.; et al. Matrix-Gla protein promotes osteosarcoma lung metastasis and associates with poor prognosis. J. Pathol. 2016, 239, 438–449. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Ruan, L.; Yang, Y.; Mei, Q. Analysis of gene expression changes associated with human carcinoma-associated fibroblasts in non-small cell lung carcinoma. Biol. Res. 2017, 50, 6. [Google Scholar] [CrossRef] [PubMed]
- Studer, R.A.; Opperdoes, F.R.; Nicolaes, G.A.; Mulder, A.B.; Mulder, R. Understanding the functional difference between growth arrest-specific protein 6 and protein S: An evolutionary approach. Open Biol. 2014, 4, 140121. [Google Scholar] [CrossRef] [PubMed]
- Tondo, G.; Perani, D.; Comi, C. TAM Receptor Pathways at the Crossroads of Neuroinflammation and Neurodegeneration. Dis. Markers 2019, 2019, 2387614. [Google Scholar] [CrossRef] [PubMed]
- Peng, C.K.; Wu, C.P.; Lin, J.Y.; Peng, S.C.; Lee, C.H.; Huang, K.L.; Shen, C.H. Gas6/Axl signaling attenuates alveolar inflammation in ischemia-reperfusion-induced acute lung injury by up-regulating SOCS3-mediated pathway. PLoS ONE 2019, 14, e0219788. [Google Scholar] [CrossRef]
- Lechertier, T.; Reynolds, L.E.; Kim, H.; Pedrosa, A.R.; Gómez-Escudero, J.; Muñoz-Félix, J.M.; Batista, S.; Dukinfield, M.; Demircioglu, F.; Wong, P.P.; et al. Pericyte FAK negatively regulates Gas6/Axl signalling to suppress tumour angiogenesis and tumour growth. Nat. Commun. 2020, 11, 2810. [Google Scholar] [CrossRef] [PubMed]
- Kanzaki, R.; Naito, H.; Kise, K.; Takara, K.; Eino, D.; Minami, M.; Shintani, Y.; Funaki, S.; Kawamura, T.; Kimura, T.; et al. Gas6 derived from cancer-associated fibroblasts promotes migration of Axl-expressing lung cancer cells during chemotherapy. Sci. Rep. 2017, 7, 10613. [Google Scholar] [CrossRef]
- Wu, X.; Ma, W.; Zhou, Q.; Yan, H.; Lim, Z.F.; Huang, M.; Deng, C.; Yu, X.; Su, H.; Komo, S.; et al. AXL-GAS6 expression can predict for adverse prognosis in non-small cell lung cancer with brain metastases. J. Cancer Res. Clin. Oncol. 2017, 143, 1947–1957. [Google Scholar] [CrossRef]
- Han, L.; Kong, R.; Yin, D.D.; Zhang, E.B.; Xu, T.P.; De, W.; Shu, Y.Q. Low expression of long noncoding RNA GAS6-AS1 predicts a poor prognosis in patients with NSCLC. Med. Oncol. 2013, 30, 694. [Google Scholar] [CrossRef]
- Iida, S.; Miki, Y.; Suzuki, T.; Mori, K.; Saito, M.; Niikawa, H.; Kondo, T.; Yamada-Okabe, H.; Sasano, H. Activation of AXL and antitumor effects of a monoclonal antibody to AXL in lung adenocarcinoma. Anticancer Res. 2014, 34, 1821–1827. [Google Scholar]
- Huang, L.; Fu, L. Mechanisms of resistance to EGFR tyrosine kinase inhibitors. Acta Pharm. Sin. B 2015, 5, 390–401. [Google Scholar] [CrossRef] [PubMed]
- Kohno, T.; Nakaoku, T.; Tsuta, K.; Tsuchihara, K.; Matsumoto, S.; Yoh, K.; Goto, K. Beyond ALK-RET, ROS1 and other oncogene fusions in lung cancer. Transl. Lung Cancer Res. 2015, 4, 156–164. [Google Scholar] [CrossRef]
- Zhang, Z.; Lee, J.C.; Lin, L.; Olivas, V.; Au, V.; La Framboise, T.; Abdel-Rahman, M.; Wang, X.; Levine, A.D.; Rho, J.K.; et al. Activation of the AXL kinase causes resistance to EGFR-targeted therapy in lung cancer. Nat. Genet. 2012, 44, 852–860. [Google Scholar] [CrossRef] [PubMed]
- Perez, R.; Crombet, T.; de Leon, J.; Moreno, E. A view on EGFR-targeted therapies from the oncogene-addiction perspective. Front Pharmacol. 2013, 4, 53. [Google Scholar] [CrossRef]
- Metro, M.; Crinò, L. Advances on EGFR mutation for lung cancer. TLCR 2012, 1, 5–13. [Google Scholar] [CrossRef]
- van Persijn, E.L.; Gelderblom, H.; Bloem, J.L. RECIST revised: Implications for the radiologist. A review article on the modified RECIST guideline. Eur. Radiol. 2020, 20, 1456–1467. [Google Scholar] [CrossRef] [PubMed]
- Myers, D.J.; Wallen, J.M. Lung Adenocarcinoma; StatPearls Publishing: Treasure Island, FL, USA, 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK519578/ (accessed on 10 October 2021).
- Lokich, J.; Anderson, N. Carboplatin versus cisplatin in solid tumors: An analysis of the literature. Ann. Oncol. 1998, 9, 13–21. [Google Scholar] [CrossRef]
- Choy, H.; Akerley, W.; Devore, R. Paclitaxel, carboplatin and radiation therapy for non-small-cell lung cancer. Oncology 1998, 12, 80–86. [Google Scholar]
- Lück, H.J.; Roché, H. Weekly paclitaxel: An effective and well-tolerated treatment in patients with advanced breast cancer. Crit. Rev. Oncol. Hematol. 2002, 44, S15–S30. [Google Scholar] [CrossRef]
- Scagliotti, G.V.; Smit, E.; Bosquee, L.; O'Brien, M.; Ardizzoni, A.; Zatloukal, P.; Eberhardt, W.; Smid-Geirnaerdt, M.; de Bruin, H.G.; Dussenne, S.; et al. A phase II study of paclitaxel in advanced bronchioloalveolar carcinoma (EORTC trial 08956). Lung Cancer 2005, 50, 91–96. [Google Scholar] [CrossRef]
- Strauss, G.M.; Herndon, J.E., 2nd; Maddaus, M.A.; Johnstone, D.W.; Johnson, E.A.; Harpole, D.H.; Gillenwater, H.H.; Watson, D.M.; Sugarbaker, D.J.; Schilsky, R.L.; et al. Adjuvant paclitaxel plus carboplatin compared with observation in stage IB non-small-cell lung cancer: CALGB 9633 with the Cancer and Leukemia Group B, Radiation Therapy Oncology Group, and North Central Cancer Treatment Group Study Groups. J. Clin. Oncol. 2008, 26, 5043–5051. [Google Scholar] [CrossRef]
- Okamoto, I.; Nokihara, H.; Nomura, S.; Niho, S.; Sugawara, S.; Horinouchi, H.; Azuma, K.; Yoneshima, Y.; Murakami, H.; Hosomi, Y.; et al. Comparison of Carboplatin Plus Pemetrexed Followed by Maintenance Pemetrexed with Docetaxel Monotherapy in Elderly Patients with Advanced Nonsquamous Non-Small Cell Lung Cancer: A Phase 3 Randomized Clinical Trial. JAMA Oncol. 2020, 6, e196828. [Google Scholar] [CrossRef]
- Noronha, V.; Patil, V.M.; Joshi, A.; Menon, N.; Chougule, A.; Mahajan, A.; Janu, A.; Purandare, N.; Kumar, R.; More, S.; et al. Gefitinib Versus Gefitinib Plus Pemetrexed and Carboplatin Chemotherapy in EGFR-Mutated Lung Cancer. J. Clin. Oncol. 2020, 38, 124–136. [Google Scholar] [CrossRef]
- Zhou, C.; Chen, G.; Huang, Y.; Zhou, J.; Lin, L.; Feng, J.; Wang, Z.; Shu, Y.; Shi, J.; Hu, Y.; et al. Camrelizumab plus carboplatin and pemetrexed versus chemotherapy alone in chemotherapy-naive patients with advanced non-squamous non-small-cell lung cancer (CameL): A randomised, open-label, multicentre, phase 3 trial. Lancet Respir. Med. 2021, 9, 305–314. [Google Scholar] [CrossRef]
- Schüll, B.; Scheithauer, W.; Kornek, G.V. Capecitabine as salvage therapy for a breast cancer patient with extensive liver metastases and associated impairment of liver function. Onkologie 2003, 26, 578–580. [Google Scholar] [CrossRef]
- Kuchuk, M.; Addison, C.L.; Clemons, M.; Kuchuk, I.; Wheatley-Price, P. Incidence and consequences of bone metastases in lung cancer patients. J. Bone Oncol. 2013, 2, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Sterzyńska, K.; Klejewski, A.; Wojtowicz, K.; Świerczewska, M.; Andrzejewska, M.; Rusek, D.; Sobkowski, M.; Kędzia, W.; Brązert, J.; Nowicki, M.; et al. The Role of Matrix Gla Protein (MGP) Expression in Paclitaxel and Topotecan Resistant Ovarian Cancer Cell Lines. Int. J. Mol. Sci. 2018, 19, 2901. [Google Scholar] [CrossRef] [PubMed]
- Nowacka, M.; Sterzynska, K.; Andrzejewska, M.; Nowicki, M.; Januchowski, R. Drug resistance evaluation in novel 3D in vitro model. Biomed. Pharmacother. 2021, 138, 111536. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, M.; Sonobe, M.; Nakayama, E.; Kobayashi, M.; Kikuchi, R.; Kitamura, J.; Imamura, N.; Date, H. Higher expression of receptor tyrosine kinase Axl, and differential expression of its ligand, Gas6, predict poor survival in lung adenocarcinoma patients. Ann. Surg. Oncol. 2013, 20 (Suppl. 3), S467–S476. [Google Scholar] [CrossRef]
- Balogh, I.; Hafizi, S.; Stenhoff, J.; Hansson, K.; Dahlbäck, B. Analysis of Gas6 in human platelets and plasma. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 1280–1286. [Google Scholar] [CrossRef] [PubMed]
- Auyez, A.; Sayan, A.E.; Kriajevska, M.; Tulchinsky, E. AXL Receptor in Cancer Metastasis and Drug Resistance: When Normal Functions Go Askew. Cancers 2021, 13, 4864. [Google Scholar] [CrossRef]
- Tanaka, M.; Siemann, D.W. Therapeutic Targeting of the Gas6/Axl Signaling Pathway in Cancer. Int. J. Mol. Sci. 2021, 22, 9953. [Google Scholar] [CrossRef] [PubMed]
- Nonagase, Y.; Takeda, M.; Azuma, K.; Hayashi, H.; Haratani, K.; Tanaka, K.; Yonesaka, K.; Ishii, H.; Hoshino, T.; Nakagawa, K. Tumor tissue and plasma levels of AXL and GAS6 before and after tyrosine kinase inhibitor treatment in EGFR-mutated non-small cell lung cancer. Thorac. Cancer 2019, 10, 1928–1935. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Dai, Y.; Chen, L.A. The Prediction Of Epidermal Growth Factor Receptor Mutation And Prognosis Of EGFR Tyrosine Kinase Inhibitor By Serum Ferritin In Advanced NSCLC. Cancer Manag. Res. 2019, 11, 8835–8843. [Google Scholar] [CrossRef] [PubMed]
- Mohan, A.; Ansari, A.; Masroor, M.; Saxena, A.; Pandey, R.M.; Upadhyay, A.; Luthra, K.; Khilnani, G.C.; Jain, D.; Kumar, R.; et al. Measurement of Serum EGFR mRNA Expression is a Reliable Predictor of Treatment Response and Survival Outcomes in Non- Small Cell Lung Cancer. Asian Pac. J. Cancer Prev. APJCP 2020, 21, 3153–3163. [Google Scholar] [CrossRef] [PubMed]
- Romero-Ventosa, E.Y.; Blanco-Prieto, S.; González-Piñeiro, A.L.; Rodríguez-Berrocal, F.J.; Piñeiro-Corrales, G.; Páez de la Cadena, M. Pretreatment levels of the serum biomarkers CEA, CYFRA 21-1, SCC and the soluble EGFR and its ligands EGF, TGF-alpha, HB-EGF in the prediction of outcome in erlotinib treated non-small-cell lung cancer patients. SpringerPlus 2015, 4, 171. [Google Scholar] [CrossRef] [PubMed]
- Haghgoo, S.M.; Khosravi, A.; Mortaz, E.; Pourabdollah-Toutkaboni, M.; Seifi, S.; Sabour, S.; Allameh, A. Prognostic value of rare and complex mutations in EGFR and serum levels of soluble EGFR and its ligands in non-small cell lung carcinoma patients. Clin. Biochem. 2017, 50, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Serilmez, M.; Özgür, E.; Karaman, S.; Gezer, U.; Duranyıldız, D. Detection of serum protein and circulating mRNA of cMET, HGF EGF and EGFR levels in lung cancer patients to guide individualized therapy. Cancer Biomark. 2019, 25, 177–184. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Pre-Treatment | Post-Treatment | p a |
|---|---|---|---|
| Hemoglobin (g/dL) | 12.25 [11.82–14.35] | 12.4 [10.87–14.15] | 0.695 |
| Platelet count (×109/L) | 249.5 [183.5–312] | 234 [189.7–331] | 0.586 |
| WBC (×109/L) | 8.13 [5.28–10.28] | 5.2 [4.09–7.38] | 0.007 * |
| Creatinine (mg/dL) | 0.92 [0.7–1.07] | 0.86 [0.73–1.11] | 0.763 |
| Urea (mg/dL) | 36.2 [29.2–49.7] | 36.2 [26.4–41.5] | 0.163 |
| Total Bilirubin (mg/dL) | 0.41 [0.29–0.54] | 0.51 [0.32–0.61] | 0.014 * |
| ASAT (U/L) | 21 [16.2–24.9] | 18 [13–23.5] | 0.669 |
| ALAT (U/L) | 25.5 [11.5–36.2] | 22 [17.5–27] | 0.722 |
| GGT (U/L) | 47 [26.2–116.5] | 60.5 [26.5–81.5] | 0.311 |
| Calcium (mg/dL) | 9.3 [8.9–9.8] | 9.5 [9.1–10] | 0.019 * |
| Neutrophils (%) | 69.2 [58.65–81.03] | 58.25 [50.38–72.95] | 0.032 * |
| Lymphocytes (%) | 18.4 [11.07–29.8] | 27.75 [12.72–34.9] | 0.09 |
| ALP (U/L) | 92 [81–125.5] | 98 [79.5–125.7] | 0.401 |
| LDH (U/L) | 211.5 [182.2–280.2] | 166 [146.2–253.5] | 0.094 |
| K (mmol/L) | 4.5 [4–4.9] | 4.5 [3.6–4.8] | 0.220 |
| Na (mmol/L) | 138 [136–140] | 138 [135–138] | 0.090 |
| Mg (mg/dL) | 1.8 [1.7–1.9] | 1.8 [1.7–2] | 0.638 |
| Glucose (mg/dL) | 101 [95–115] | 102 [95–123] | 0.816 |
| Variable | Pre-Treatment | Post-Treatment | p a |
|---|---|---|---|
| Gas6 (pg/mL) | 311.5 [121.1–368.5] | 286.7 [94.5–366.8] | 0.647 |
| EGFR (pg/mL) | 45.6 [23.4–63.5] | 32.1 [23.3–50.7] | 0.401 |
| VK1 (ng/mL) | 9.4 [8–10.6] | 8.89 [8.4–10.6] | 0.614 |
| MGP (pg/mL) | 1196 [1099–1328.5] | 1191 [1102–1290.7] | 0.709 |
| Pre- and Post-Treatment Variables | MGP Pre-Treatment | MGP Post-Treatment | ||
|---|---|---|---|---|
| r (95%CI) | p a | r (95%CI) | p a | |
| Gas6 (pg/mL) | −0.167 (−0.507; −0.223) | 0.482 | 0.018 (−0.417; 0.498) | 0.940 |
| EGFR (pg/mL) | −0.316 (−0.784; 0.146) | 0.175 | 0.087 (−0.377; 0.533) | 0.717 |
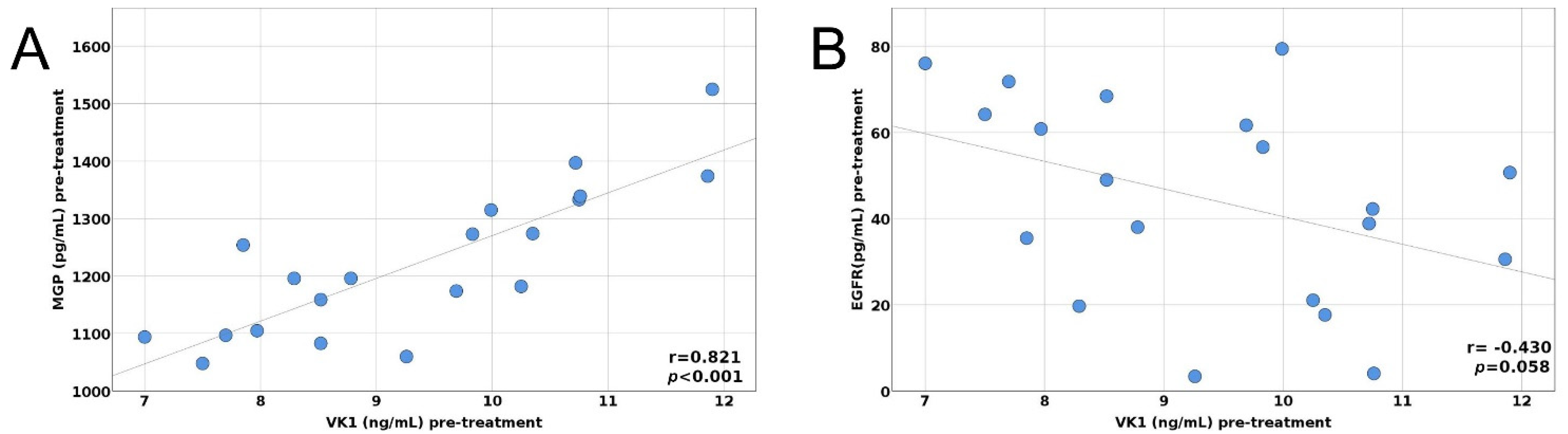
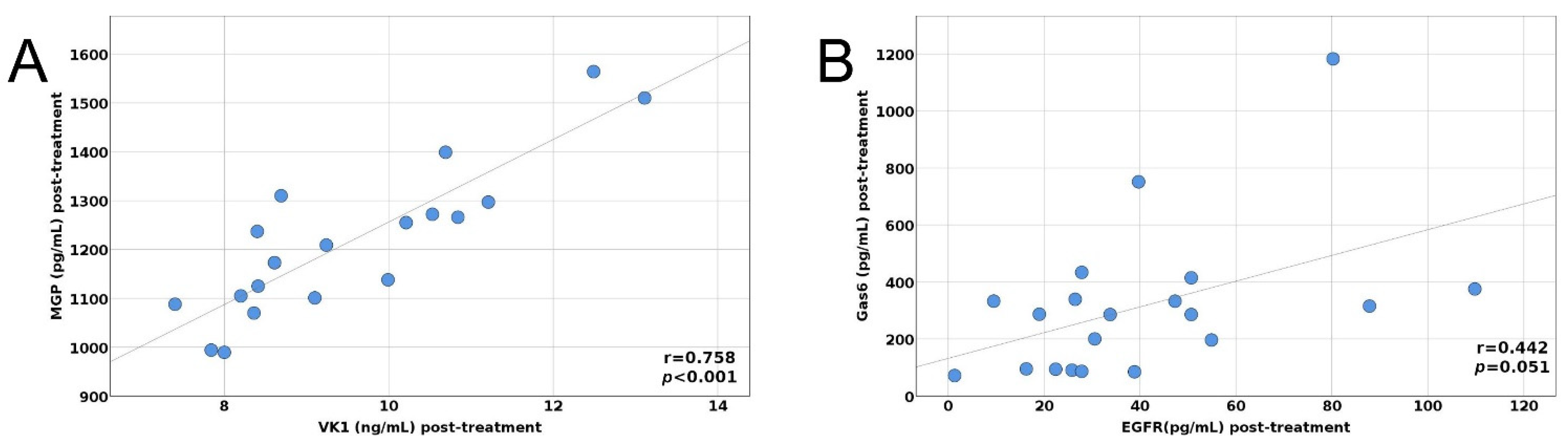
| VK1 (ng/mL) | 0.821 (0.523; 0.954) | <0.001 * | 0.857 (0.609; 0.950) | p < 0.001 * |
| Variable | β | Standard Error | p | 95%CI for β |
|---|---|---|---|---|
| Gas6 (pg/mL) pre-treatment | 0.853 | 0.128 | <0.001 | 0.581; 1.124 |
| Age | 9.587 | 3.395 | 0.018 | 2.023; 17.151 |
| VK1 (ng/mL) pre-treatment | −79.712 | 22.650 | 0.006 | −130.179; −29.245 |
| Smoking | 66.233 | 33.419 | 0.076 | 8.229; 140.694 |
| Variable | β | Standard error | p | 95%CI for β |
|---|---|---|---|---|
| MGP (pg/mL) pre-treatment | −1.299 | 0.391 | 0.005 | −2.132; −0.466 |
| EGFR (pg/mL) pre-treatment | 5.070 | 2.180 | 0.034 | 0.424; 9.717 |
| VK1 (ng/mL) pre-treatment | 130.985 | 37.702 | 0.003 | 50.624; 211.345 |
| Variable | β | Standard Error | p | 95%CI for β |
|---|---|---|---|---|
| MGP (pg/mL) post-treatment | −0.448 | 0.169 | 0.017 | −0.806; −0.090 |
| EGFR (pg/mL) post-treatment | 4.245 | 1.740 | 0.027 | 0.556; 7.935 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crintea, A.; Dutu, A.G.; Constantin, A.-M.; Fekete, Z.; Samasca, G.; Lupan, I.; Florian, I.A.; Silaghi, C.N.; Craciun, A.M. The First Evaluation of Serum Levels of MGP, Gas6 and EGFR after First Dose of Chemotherapy in Lung Cancer. Biology 2022, 11, 82. https://doi.org/10.3390/biology11010082
Crintea A, Dutu AG, Constantin A-M, Fekete Z, Samasca G, Lupan I, Florian IA, Silaghi CN, Craciun AM. The First Evaluation of Serum Levels of MGP, Gas6 and EGFR after First Dose of Chemotherapy in Lung Cancer. Biology. 2022; 11(1):82. https://doi.org/10.3390/biology11010082
Chicago/Turabian StyleCrintea, Andreea, Alina Gabriela Dutu, Anne-Marie Constantin, Zsolt Fekete, Gabriel Samasca, Iulia Lupan, Ioan Alexandru Florian, Ciprian Nicolae Silaghi, and Alexandra Marioara Craciun. 2022. "The First Evaluation of Serum Levels of MGP, Gas6 and EGFR after First Dose of Chemotherapy in Lung Cancer" Biology 11, no. 1: 82. https://doi.org/10.3390/biology11010082
APA StyleCrintea, A., Dutu, A. G., Constantin, A.-M., Fekete, Z., Samasca, G., Lupan, I., Florian, I. A., Silaghi, C. N., & Craciun, A. M. (2022). The First Evaluation of Serum Levels of MGP, Gas6 and EGFR after First Dose of Chemotherapy in Lung Cancer. Biology, 11(1), 82. https://doi.org/10.3390/biology11010082