Simple Summary
Addiction to tobacco is a serious health and economical problem because it is one of the most addictive and the most consumed substance in the world. Although well documented, and despite the desire of numerous smokers to quit, maintenance of abstinence is a daily challenge for most of them. The heterogeneity in achieving this maintenance raises the question of potential differences in brain reactivity. An emerging field of research has been interested in brain markers helping to identify individuals who are the most likely to relapse. Using brain imaging techniques such as Magnetic Resonance Imaging (MRI), one can hope it will be possible to offer tailored care for each patient.
Abstract
Chronic tobacco smoking remains a major health problem worldwide. Numerous smokers wish to quit but most fail, even if they are helped. The possibility of identifying neuro-biomarkers in smokers at high risk of relapse could be of incredible progress toward personalized prevention therapy. Our aim is to provide a scoping review of this research topic in the field of Magnetic Resonance Imaging (MRI) and to review the studies that investigated if MRI defined markers predicted smoking cessation treatment outcome (abstainers versus relapsers). Based on the available literature, a meta-analysis could not be conducted. We thus provide an overview of the results obtained and take stock of methodological issues that will need to be addressed to pave the way toward precision medicine. Based on the most consistent findings, we discuss the pivotal role of the insula in light of the most recent neurocognitive models of addiction.
1. Introduction
Chronic tobacco smoking is one of the main risk factors of cancers and cardio-vascular diseases and contributes to the death of more than 8 million people every year [1,2]. Hence, it remains a major public health problem with huge economic consequences worldwide. Despite numerous public health campaigns about the deleterious effects of smoking, the recurrent increase of tobacco taxation and the ongoing development of different treatments, few smokers achieve abstinence. Numerically, while most smokers declare a willingness to quit, less than half of them will try, and only 5% will remain abstinent without any help at 6 months, a rate that will increase to about 50% using nicotine replacement therapies (NRT) and/or pharmacological treatment [3,4].
One critical question is, therefore, why is it so difficult for smokers to quit? Numerous factors with potential interactive effects have been associated with a higher risk of treatment failure or relapse, suggesting that a bio-psycho-social approach must be adopted to guide clinical practice [5].
First, at the psychological level, personality characteristics related to poor inhibition skills, such as sensation-seeking and impulsivity, or to increased hedonic sensitivity, such as reward dependence, are thought to impact the cessation attempt. Moreover, in line with the self-medication theory, smoking is commonly used as a coping strategy, to reduce internal stresses or feelings of psychological distress. Relying on such a mood regulation strategy could dampen the motivation to quit [6].
Second, at the behavioral level, routines in user behavior (such as lighting and holding a cigarette) and environmental cues (such as cigarette stores or social situations) might automatically launch the urge to smoke (i.e., the experience of craving [7]), which relates to relapse. The greater the number of years of smoking and/or the number of cigarettes smoked, the more difficult it is for smokers to quit.
Moreover, these psychosocial factors are supported by brain molecular changes. At the cerebral level, nicotine is one of the most addictive drugs and modulates the mesolimbic reward pathways [8]. Notably, each cigarette smoked triggers the release of an important quantity of dopamine in the nucleus accumbens that mediates the rewarding and pleasure effect of nicotine, which in turn reinforces tobacco dependence. However, the magnitude of this effect and its consequences on global brain functioning is different between subjects, depending on the individual genetic background encompassing a large setting of genes involved in drug metabolism, susceptibility to addictive behaviors or susceptibility to psychiatric diseases, but also changes in the brain structure and function [9].
Such consequences on the brain can be approached by neuroimaging studies, with already existing reviews demonstrating that the brain is structurally and functionally modified by chronic tobacco smoking [10,11]. Nowadays, there is hope that neuroimaging studies will also help to establish not only ‘where’ and ‘how’ in the brain smoking cessation treatments work, but also why their effectiveness varies between patients. Indeed, from a clinical perspective, it could improve, or even outperform, the current outcome predictive factors of who will be a responder or not to smoking cessation treatment, and thus use these biomarkers to tailor the treatment strategies. Until now, the major predictors used in clinical practice are the number of cigarettes smoked by days and/or a scale of dependence, such as the Fagerstrom Test for Nicotine Dependence (FTND) [12].
The idea that a given treatment should be provided according to the individual susceptibility to respond or not to such treatment is the cornerstone of the precision medicine concept, which “does not literally mean the creation of drugs or medical devices that are unique to a patient, but rather the ability to classify subpopulations that differ in their susceptibility to a particular disease, in the biology and/or prognosis of those diseases they may develop, or in their response to a specific treatment” (see Appendix E [13]). In this framework, the suggestion of using neurobiomarkers for predicting smoking cessation success is not new and was further supported by the results of Naqvi et al. in 2007 who reported the spontaneous cessation of smoking after a brutal acute insular brain insult in a cohort of 69 smokers [14]. However, due to the traumatic nature of stroke, these results are difficult to transpose to all the persons willing to stop smoking. Therefore, examining brain structures as well as cerebral anatomical and functional networks among treatment-seeking smokers, or nicotine-dependent individuals willing to quit, is important to understand which of these markers can be used to predict the success or failure of smoking cessation interventions.
The purpose of this article is thus to present an overview of the progress made in this field of research and what would remain to be improved for offering, in a longer term, more personalized programs.
2. Materials and Methods
We searched PubMed from MEDLINE for original articles for the following indication terms: (nicotine OR tobacco OR smoke*) AND (abstinence* OR cessation OR relapse*) AND (fMRI OR MRI OR “real-time fMRI” OR neuroimaging OR neurobiomarker). Papers had to be on humans, using brain magnetic resonance imaging (MRI), published in the English language between January 2007 (publication date of the above-mentioned seminal paper relating the beneficial effect of brain injury on successful smoking cessation) and December 2021 and restrained to tobacco consumption. We excluded studies with an endpoint other than comparing abstainers versus relapsers, such as studies interested in the change in smoking habits or tobacco craving or with an abstinence length of less than one week.
For each article, we reported the characteristics of the population, type and duration of therapies, length of abstinence, the proportion of relapse at follow-up, methodologies of brain MRI acquisition, and analysis and the conclusion from the authors.
3. Results
Twenty-four articles meeting our selection criteria were identified. Their main methodological characteristics are summarized in Table 1 (See Supplementary Material for the flowchart). In addition, the MRI findings are presented graphically in Figure 1 and Figure 2.

Table 1.
Main characteristics of included studies comparing future abstainers and relapsers.
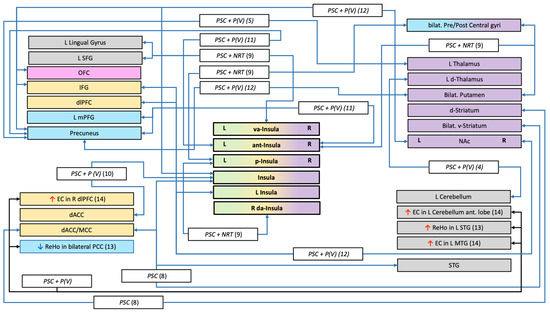
Figure 1.
Structures and connections highlighted as precursor to relapse after a quit attempt in resting-state studies. <—> = lower connectivity between structures; ↑ = greater fMRI activation; ↓ = lower fMRI activation; □ white rectangle = treatment use (NRT (Nicotine Replacement Therapy), P (Pharmacotherapy with: V = Varenicline, EVP = selective alpha-7 nicotinic acetylcholine receptor); PCS (Psychological Counselling Session)); □ coloured rectangles = network implicated (Blue = Default Mode Network; Gray = Undetermined network or not part of a specific network; Green = Salience Network; Orange = Executive Control Network; Pink = Reward network; Purple = Habit formation); (n) = number of the study (see Table 1); EC = Eigenvector centrality; ReHo = Regional Homogeneity; Ant = anterior; d = dorsal; dl=dorsolateral; L = Left; v = ventral; va = ventro-anterior; R = Right; m=medial; ACC = Anterior Cingular Cortex; IFG= Inferior Frontal Gyrus; OFC = Orbital Frontal Cortex; NAc= Nucleus accumbens; SFG = Superior Frontal Gyrus.
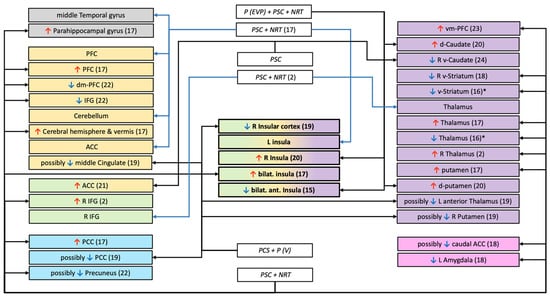
Figure 2.
Structures and connections highlighted as precursor to relapse after a quit attempt in task-based studies (drugs-cues, monetary reward, or inhibition tasks). ↑ = greater fMRI activation; ↓ = lower fMRI activation; □ white rectangle = treatment use (NRT (Nicotine Replacement Therapy), P (Pharmacotherapy with: V = Varenicline, EVP = selective alpha-7 nicotinic acetylcholine receptor); PCS (Psychological Counselling Session)); □ coloured rectangles = network implicated (Blue = Default Mode Network; Gray = Undetermined network or not part of a specific network; Green = Salience Network; Orange = Executive Control Network; Pink = Reward network Purple = Habit formation); * = visual inspection of the figure; (n) = number of the study (see Table 1); d = dorsal; dm = dorso-median; L = Left; v = ventral; vm = ventro-median; R = Right; ACC = Anterior Cingular Cortex; IFG = Inferior Frontal Gyrus; PCC = Posterior Cingular Cortex; PFC = Pre Frontal Cortex.
In all these studies, participants had at least one MRI acquisition before any therapeutic intervention and a predefined quit date. Nevertheless, the time-lapse between MRI acquisition and the beginning of treatment varied across studies. Moreover, therapeutic modalities (type of treatment and duration), as well as the definition of abstinence, were specific to each study. Given this heterogeneity, it was not possible to conduct a meta-analysis and we focused on a descriptive analysis and critical synthesis.
The different studies were first grouped according to the MRI acquisition: anatomical, resting state (RS), and task-based. They were further layered by the type of cessation treatment used: NRT (but independently from the route of administration and dosage), pharmacological treatment (but independently from the drug subtypes and dosage), and psychological counselling sessions (PCS) (but independently from the number of sessions, the qualification of the therapist, and the method used).
3.1. Anatomical
Five studies [15,16,17,18,19] addressed the question of macrostructural anatomical differences underlying the ability to achieve abstinence. They differed in both the type of treatment and the length of abstinence. Three used a whole brain (WB) voxel-based morphometry (VBM [20]) analysis [15,16,18] and the other used different regions of interest (ROIs) [17,19]. The two studies from Froeliger et al. reported differences in grey matter volume (GMV) between abstainers and relapsers, either in different regions or in opposite direction (Table 1). In the three studies using varenicline and PCS, relapse was associated with decreased GMV in the right post-central gyrus, right dorsal striatum, and left OFC in one study [18], and with increased left thalamic GMV in another one [19]. The third study found no association between GMV in insular subregion (TIV corrected) and treatment outcome [17].
Two studies from the same research team investigated if microstructural anatomical alterations are associated with treatment outcome (varenicline + PCS) [21,22]. Using a whole brain approach and comparing 28 abstainers and 38 relapsers, relapse was associated with higher fractional anisotropy in the cerebellum and post-central gyrus [21]. In a further study including as many relapsers but fewer abstainers and an insular ROI, no differences were observed between the two groups [22].
3.2. Restings State (RS)
Functional MRI RS connectivity analyses are based on the demonstration of strong temporal correlations between the spontaneous, intrinsic fluctuations at rest of the BOLD signal (reflecting neuronal activity while people lie still and think of nothing in particular) in different regions. The time-course of this signal from the seed-region is correlated with the BOLD signal time-course in every other voxel in the brain. These communicating regions tend to be engaged simultaneously throughout daily tasks and sustain a communication activity even in resting conditions [23].
Brain networks reconstructed by RS analyses are highly consistent within and between individuals and present high functional and anatomical coherence [24].
The more frequently reported and consistent networks across studies are the Default Mode Network (DMN), the task-positive (in opposition of the DMN), the sensorimotor network, the visual network, the fronto-parietal network (sometimes named the attentional network), and the auditory network.
We identified nine studies that examined if the pre-cessation brain activity at rest would predict the treatment outcome.
In the Sweitzer et al. (2016) study, participants underwent two fMRI sessions before the initiation of a PCS: the first after smoking ad libidum and the second after 24 h of abstinence. These authors used a whole-brain connectivity approach with the ventral and dorsal striatum as seed regions and modelled age, sex, cigarettes smoked per day and session order as covariates. Relapse was independently associated with weaker connectivity after abstinence (relative to satiety) between the bilateral ventral striatum and the insula, the superior temporal gyrus (STG), and the anterior/mid cingulate cortex [25].
In a study combining NRT and PCS, Addicott et al. (2015) focused on insula-based networks and used treatment group and FTND scores as covariates. Relapse was independently associated with weaker functional connectivity between (i) the posterior insula and pre-central gyrus, the post-central gyrus, and bilateral putamen; (ii) the ventral anterior insula and left superior frontal gyrus (SFG) and lingual gyrus; (iii) the right dorso-anterior insula and left posterior insula [26].
The study by Wilcox et al. (2017) that included people treated either by pharmacotherapy or placebo focused on the functional connectivity between six ROIs (Table 1) [27]. Taking the treatment group into account, they found no differences between the relapsers and abstainers. Nonetheless, irrespective of treatment group, lower levels of connectivity between the insula and dorsal anterior cingular cortex (dACC) predicted greater smoking quantity prior the endpoint, and this was the case independently from the FTND score.
In four studies conducted by the same research team, the treatment combined varenicline and PCS [18,19,28,29]. All studies used a whole brain approach but different seed regions. Two studies assessed the association with baseline connectivity only [18,19], and the two others compared post- versus pre-treatment changes in connectivity [28,29]. Relapse was associated with reduced baseline functional connectivity between the thalamus and cerebellum in the Qian et al. (2019) study, and between the thalamus and precuneus in the Wang et al. (2020a) study. During treatment, relapse was associated with decreased connectivity (from before to after the treatment) between the insula and the precuneus as well as the medial frontal gyrus [28], and between the striatum and the insula, orbito-frontal cortex (OFC), dorsolateral PFC, inferior frontal gyrus (IFG) and precuneus [29], while abstainers showed the opposite pattern of changes.
Another voxel-wise method to evaluate local functional connectivity is the measure of regional homogeneity (ReHo), which is defined as the average functional connectivity values of a voxel with its surrounding voxels and reflects how much each region is connected to its neighbors [30]. Using this method, Wang et al. (2017) demonstrated that, among people who received a pharmacological treatment combined to PCS, relapse was associated with a decreased ReHo in the bilateral posterior cingulate cortex (PCC) as well as an increased ReHo in the left STG, independently from baseline smoking and FTND score [31].
Finally, Shen et al. (2017) used a voxel-wise eigenvector centrality (EC) measure to identify key functional brain networks. EC gives information about the wide-reaching influence of a functional area. The eigenvector value is relative to the number of connections to other highly connected areas [32]. In a sample under pharmacological treatment, independently from baseline smoking, relapse was associated with increased EC in the middle frontal gyrus (MFG) and SFG, the left middle temporal gyrus (MTG) and STG, and the left anterior cerebellum [33].
3.3. Task-Based Studies
3.3.1. Functional Activation
Functional activation studies exploit endogenous brain activity for mapping brain responses during periodic and specific cognitive/emotional tasks.
Inhibition
Several models consider that the development and maintenance of addiction is tightly linked to impaired inhibitory control (IC) following exposure to a representation of the substance. We found two articles that examined if the pre-cessation brain reactivity during IC tasks predicted treatment outcome using an ROI approach.
Froeliger et al. (2017) investigated the activation of the right inferior frontal gyrus (IFG), bilateral thalamus, subthalamic nucleus, presupplementary motor area, and left primary motor cortex during a Go/NoGo task with various neutral stimuli. Following a combined treatment of NRT and PCS, relapse was associated with increased activation in the right IFG and thalamus, and this was the case independently from FTND score [15]. Moreover, greater right IFG activity was associated with worse behavioral performances.
Gilman et al. (2018) also used a Go/NoGo task with tobacco-related (versus neutral) images and a ROI approach among people under four different treatments (pharmacotherapy EVP-6124 and/or NRT in addition to PCS). Relapse was associated with decreased activation in the bilateral anterior insula with tobacco-related stimuli NoGo trials independently from FTND score but without taking the treatment group into account [34].
Drug Cues or Healthy Messages
Because people with a substance use disorder are more sensitive to environmental cues specifically related to their drug consumption, drug-cues reactivity paradigms are considered an ideal way to observe engaged pathways of reward- and/or cognitive-control-related regions to predict substance use disorders treatment outcomes [35].
Smoking Cues vs. Neutral
Out of the six studies that were identified, all but three [36,37,38] used an ROI approach but different ones.
Three studies included patients treated with NRT combined to PCS [37,39,40]. The McClernon et al. study (2007) involved three fMRI sessions (baseline, quit date, 2–4 weeks following quitting). At baseline, relative to abstainers, relapsers seemed to have lower smoking cue reactivity in the ventral striatum and thalamus. Moreover, there was a Scan session X Stimulus type X Treatment outcome interaction. For relapsers, the differences between responses to smoking and control cues were negligible at all three scans; for abstainers, there was a greater activation to smoking than control cues in the thalamus and ventral striatum before treatment, and this pattern was reversed after treatment. In the Jane et al. study (2010), relapse was associated with greater smoking cue reactivity in the bilateral insula, PCC, parahippocampal gyrus, thalamus, putamen, cerebellar hemispheres and vermis, and prefrontal cortex (PFC). In the most recent study, relapse was associated with lower smoking cue reactivity in the ventral striatum and amygdala independently of the level of craving before and during the scanning session [40].
Two studies were conducted among smokers treated by pharmacotherapy either alone [36] or in combination with NRT [41]. In the study by Janes et al. (2017), relapse was associated with greater reactivity in the right insula and dorsal striatum (dorsolateral putamen and dorsal caudate). Hartwell et al. (2013) designed a more complex paradigm involving two fMRI sessions (baseline and post quit) with two experimental conditions each [36]: while being allowed to experience craving, and conversely when being asked to resist the craving. A whole-brain analysis at baseline revealed no specific brain activation associated with smoking cessation outcome when participants were allowed to crave. Conversely, during craving resistance at baseline, relapse was associated with a lower reactivity in the insular cortex, putamen, anterior thalamus, middle cingulate, and PCC. When contrasting the baseline and post-quit sessions, no differences were found for either the crave or resist conditions among the relapsers, while, for the abstainers, greater activation was found at baseline in the bilateral SFG (extending into the PFC) but in the resist condition only.
Finally, Allenby et al. (2020) also used two fMRI sessions during cue exposure but both at baseline: the first after smoking ad libidum, and the second after 24 h of abstinence. Using a whole-brain analysis, and contrasting the sessions (abstinence versus smoking), relapse was associated with a greater cue reactivity in the ACC in people treated by PCS independently from abstinence-induced changes in craving and withdrawal, sex, age, and baseline smoking [38].
Health Messages
The two studies that investigated the brain reactivity to messages on the negative health consequences of tobacco used a ROI approach in people under NRT combined with PCS [42,43].
Based on the general evidence that tailored interventions are more effective than generic ones, Chua et al. (2011) used audio-visual blocks of personally tailored, untailored and neutral messages. Relapse was associated with decreased activation in the medial PFC, IFG, and possibly in the precuneus following tailored (versus neutral) messages specifically, and independently from number of cigarettes per day at baseline. Owens et al. (2017) focused on the difference between graphic warning labels or text only warning labels and control images. Relapse was associated with greater activation in the ventromedial PFC during graphic warning labels (versus control images), and this was the case beyond the influence of FTND score.
Reward
While smoking is known to be associated with a dysregulation of the reward system, determining if a global (i.e., to multiple rewards, such as monetary and food stimuli) or a domain-specific dysfunction (the substance) predicts the issue of the quit attempt is believed to facilitate the identification of more targeted interventions such as contingency management (i.e., providing monetary incentives for periods of abstinence).
This question was addressed by Sweitzer et al. in the same study sample described above (see section B.Resting state) [44]. Relapse was associated with a decreased activity in the striatum (right ventral caudate) with monetary reward anticipation during abstinence (versus satiety), but not in the smoking anticipation condition. This effect remained after controlling for age, sex, and the number of cigarettes smoked per day, as well as the level of craving during the 24 h of abstinence.
Based on the consistent finding that substance use disorders are associated with poor abilities to delay gratification (e.g., choose 10 euros immediately over 30 euros in 3 months, also called temporal discounting), Grosskopf et al., (2020) examined if post- versus pre-treatment changes in brain activity during a temporal discounting task is associated with treatment outcome. No significant differences were observed between relapsers and abstainers [45].
3.3.2. Functional Connectivity
Cerebral areas’ interactions allow the study of the brain as a network justifying connectivity approach. Using functional imaging data, researchers can investigate not only which individual brain areas are involved in a task, but also how information flows between brain areas [46] and how functional areas change their connectivity to participate in different networks at different times (Smith et al., 2012) or under different behavioral circumstances.
We identified three studies that examined if the pre-cessation task-based functional connectivity (tbFC) predicted treatment outcome.
Two included participants treated by a combination of NRT and PCS [15,37]. Janes et al., (2010) used the presentation of smoking cues (vs neutral ones) and two Independent Component Analysis (ICA) defined ROIs and found that relapse was associated with weaker tbFC between left insula, PFC, ACC, cerebellum, and MTG [37]. Finally, using functionally defined ROIs selected from the data collected during the IC task that has been described above (NoGo versus Go trials, see section C.1.a) and baseline FTND scores as nuisance covariates, Froeliger et al. reported that relapse was associated with a decreased tbFC between the right IFG and the thalamus [15]. Notably, the tbFC mediated the association between behavioral inbibitory control performances and treatment cessation outcome.
4. Discussion
Despite the implementation and enforcement of tobacco control policies and the development of different types of interventions, smoking remains a defining challenge in global health with huge individual and economic consequences. Even with the help of treatment, still about one out of two smokers fail to achieve successful abstinence. Tailored strategies allowing the early identification of patients at high risk of relapse are urgently required. Magnetic Resonance Imaging, which is able to capture brain anatomy and activity in targeted areas and networks, might be one of the most interesting tools providing biomarkers for this purpose.
In this overview on the characterization of MRI cerebral biomarkers predictive of smoking cessation treatment outcome, we identified 25 studies including about 1250 patients that investigated this topic over the past 15 years. The fact that we did our research only in PubMed could have reduced our findings. However, as we also included studies that were identified from reference lists, we think this had little impact on our findings. Two main observations can be drawn from these data: (i) the insula, along with its associated networks, is the structure the most consistently associated with the ability to quit smoking, and (ii) the methodology used in these studies is highly heterogeneous, impeding a quantitative synthesis despite the significant number of patients evaluated.
While a meta-analysis could not be practicable, the insula appeared tightly involved in smoking cessation treatment outcomes. This finding reinforces the observation from the seminal work of Naqvi et al. (2007) showing that insular damage increased the likelihood to quit smoking abruptly and easily. This was confirmed and extended by further prospective studies [47] with an impact on longer abstinence [48] together with increased motivation for remaining abstinent [49], less frequent and severe withdrawal symptoms [50], and decreased smoking urges [51]. Notably, as summarized graphically in Figure 3, specific patterns of connectivity of the insula were predictive of treatment outcome. This observation adds to the evidence implicating the insula in tobacco addiction through the dysregulation of a complex network rather than a mere macrostructural insular change.
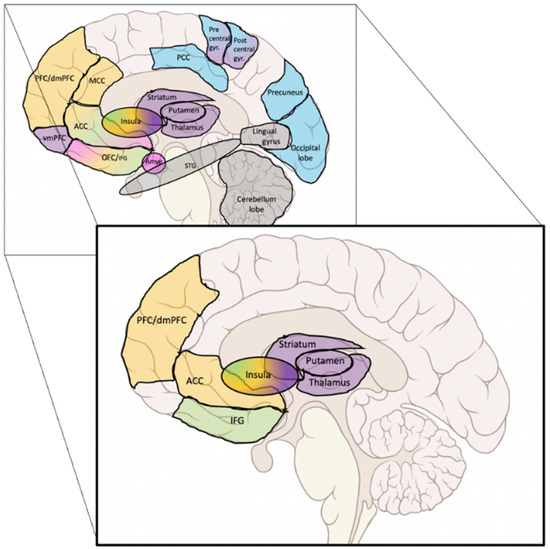
Figure 3.
Main results of the structures and networks that predicted treatment outcome. Background rectangle: graphical summary of all the findings. Forefront rectangle: most consistently reported findings. Colours = network (Blue = Default Mode Network; Orange = Executive Control Network; Green = Salience Network; Purple = Habit formation; Pink = Reward network; Gray = Undetermined network or not part of a specific network).
At the anatomical and histological level, three major subdivisions of the insula have been identified in humans and animals, including the granular insula, located in the posterior dorsal portion, the agranular insula in the anterior ventral portion, and the dysgranular part in the middle portion. Each subdivision has different connectivity features and therefore differs functionally. In humans, the insula has been described as the main node of the saliency network and as an integral hub in mediating dynamic interactions between other large-scale brain networks involved in externally oriented attention and internally oriented cognition [52]. RS fMRI studies have also pointed out its rich connectivity both with other regions and between its functional subdivisions, which may explain how the saliency network participates in so many diverse functions. Interestingly, latency analyses have revealed that insula activity temporally precedes activity in the other nodes of the executive and Default Mode Network (DMN). This new understanding of the insula as a critical node for network switching may explain its implication in substance use disorder. Indeed, it has been proposed that, first, sensory features of interoceptive signals are processed in the posterior insular cortex, then, the corresponding information is passed to the anterior insular cortex where it is remapped by integrating the motivational, emotional, and cognitive inputs from its subcortical and cortical connections and then further translated into a subjective feeling and/or conscious thought. This feeling will, in turn, influence homeostatic goals and approach/avoidance behaviors by connecting to different prefrontal regions.
Besides the insula and prefrontal cortex, our review also points to an important role of the basal ganglia and thalamus in smoking cessation. The ventral striatum has classically been considered to play an important role in addiction through its role in the anticipation and immediate response to rewards [53,54], as well as in abstinence-induced craving [55,56,57]. A recent study showed that acquired damage in the dorsal striatum is associated with an increased likelihood to quit smoking easily and immediately and to remain abstinent [58]. The ventral striatum directly receives the projection of glutamate neurons from the orbitofrontal cortex, while the dorsal striatum interacts with thalamic-cortical circuits that are involved in the planning and execution of motor responses. Because smoking behavior becomes highly automatic in people with smoking addiction, the entire striatum might be a key determinant of addiction and relapse processes. Interestingly, in a prospective lesion study on the combined effects of insula and basal ganglia lesions (versus damage elsewhere) on smoking cessation, lesions including both regions were associated with higher rates of abstinence over a one-year period. Moreover, the proportion of abstainers over the follow-up period was 75% in the group with both basal ganglia and insula lesions, while it was the case for 37% of the group with lesions to the basal ganglia alone [59].
Overall, the findings highlighted in our graphical summary (Figure 3) support recent integrative models of addiction. In the neurocognitive triadic model [60], the insula has been described as a core hub, where the anterior part of the insula converts a bottom-up interoceptive message into a subjective emotional state, which in turn modulates the activity of both a subcortical “impulsive” (i.e., amygdalo-striatal) and a cortical “reflexive” (i.e., prefrontal cortex) systems. In the integrated theoretical model from Naqvi and Bechara [47], the insula is also viewed as a hub, playing a critical role in the balance between a subcortical automatic mode of drug seeking (largely stimulus/cue driven) and a cortical goal-directed one (manifested by cravings and the tendency to relapse), by engaging representations of interoceptive drug effects in order to overcome drug-associated subjective risks and conflicts (such as dealing with negative consequences or competing goals). From a clinical perspective, these authors suggest that the most effective approach would be a two-step treatment, first by promoting the goal-directed mode with interventions that foster awareness/insight (i.e., heightened subjective riskiness of drug use) and second to buffer the insula function with neuromodulatory medications or interventions.
Unfortunately, a relatively high proportion of the studies that have been conducted up to now have methodological weaknesses that preclude strong conclusion(s) that could help to guide clinical management.
First, the definition of abstinence is variable between studies and sometimes mixed up with successful quitting. Because the determinants of early and late relapse are different [61], and as relapses occur most often within the first year following smoking cessation [62], the clinical endpoint should be at least evaluated after this delay to maximize the predictive power of the brain marker.
Second, while a significant proportion of the studies were randomized clinical trials, cessation outcome groups were defined regardless of the type of treatment, and this potentially confounding variable was not systematically accounted for.
Third, there is a need for better phenotyping of the study population. Owing to the cost of this approach, a biomarker designed to be used in patient’s treatment stratification has to improve the prediction of success of the intervention on top of the simplest and/or already known clinical factors. Accordingly, none of the neuroimaging findings should be interpreted without considering the level of impregnation (i.e., the number of cigarettes smoked per day, the number of years of exposure, carbon monoxide level, cotinine, etc…) or the severity of the nicotine addiction (i.e., the level of dependence to the substance, the frequency and intensity of craving episodes and withdrawal symptoms, etc…). Unfortunately, not all the studies from this review used these factors as covariates, which mitigates the interpretation of the results. In addition, because poly-drug use is not only frequent among smokers but also a source of consumption cessation failure as well as a condition that impacts the brain, this parameter should be better documented and considered. In this regard, investigating potential interactions between the patients’ age and addictive profile could be an important issue. In fact, nowadays, we witness in clinical practice that smoking tobacco is increasingly associated with cannabis consumption among the youngest, while alcohol daily consumption is most frequently observed in older patients. Moreover, mood factors and their associated clinical conditions such as depression and anxiety disorders, which are known to be associated with the susceptibility for relapse and with functional brain changes, need to be investigated and modelled. This point might be particularly critical as a recent metanalysis [63] further emphasized a bidirectional link between smoking behavior and depression/anxiety, baseline depression/anxiety being associated with future smoking consumption, while smoking exposure contributed to the occurrence of later depression/anxiety. Besides the dysphoric state, other psychological factors have still not yet received attention in the fMRI literature we reviewed. Other cognitive functions than inhibition and cue-reactivity are considered to play a role in addiction, notably interoceptive awareness and/or metacognitive skills [64,65]. This point is actually raised in the new metacognitive hub model of craving defended by Flaudias et al. [66] who proposed to refine the triadic neurocognitive model of addiction by considering craving as a multidimensional phenomenon instead of a unitary process. These authors argue for a triadic model that includes not only physiological craving (mediated by the interoceptive system), but also automatic craving (mediated by the impulsive system) and cognitive craving (mediated by the reflective system) as well as their interactions and reinterpretation by metacognitive skills (playing the role of a hub between the systems).
Fourth, there are some cerebral potential confounding factors that should be given consideration. With BOLD analysis, two main factors should be more systematically taken into account: baseline perfusion status and the cortical brain volume. Arterial Spin Labeling studies have reported decreased perfusion in multiple brain regions among chronic smokers, including the orbito-frontal cortices and parietal lobules [67]. In addition, several studies have highlighted that smoking constitutes a hypertension risk factor [68], which has been found to reduce cerebrovascular reactivity [69] in brain networks such as the DMN. This chronic perfusion deficit could underlie the smaller total gray matter volume reported in people that ever smoked regularly [70,71]. In addition, as white matter connections are at the foundation of neural networks, functional network analysis should also consider the structural integrity of white matter bundles before drawing any firm conclusion. It is of importance to note that smoking has been associated with a progression of white matter hyperintensities [72,73], as well as with microstructural changes in the normal-appearing white matter [21,70]. Most importantly, these microstructural brain changes have been found to predict smoking cessation outcomes after pharmacological intervention [21,28]. Altogether, these data support the need to assess more systematically brain morphological data as potential confounders in functional neuroimaging results, a methodological precaution that has been ignored in most of the studies.
In addition to the chronic perfusion changes observed in daily smokers, the significant influence of short-term abstinence on regional cerebral blood flow [74] highlights the need to standardize the acquisition of brain MRI in this population, ideally with a first acquisition after overnight abstinence and a second after few cigarettes. Indeed, the physiological changes associated with craving (i.e., transient increase in blood pressure and heart rate) might also influence the regional cerebral blood flow.
Besides the consideration of these different biomarkers, any metanalysis is also precluded by the heterogeneity in methodologies used to evaluate brain activity. Not only ROI and WB analysis were used, but also different types of images processing that follow the recent advances in brain imaging. While interesting at a pathophysiological level, the replication of former results using the same methods would have been an important first step. Moreover, the different tasks used to evaluate baseline brain networks recruit different brain areas depending on their cognitive and/or emotional load, while the type of stimulation, using visual, auditory or olfactory primary integration might simulate different pathways and could account for the discrepancies observed between studies. In addition, the interpretation of the results has to take into account that participants were treatment-seeking and may not necessarily be generalizable to all smokers. The fact that the participants were volunteers could imply a strong involvement of prefrontal networks (Control Executive Network) that could modulate RS and task-related brain activations networks.
Finally, the main objective of these studies has to be clarified, focusing either on the investigation of the pathophysiological mechanisms of smoking relapse or the identification of individual risk biomarkers that could be used in daily practice, this latter needing the development of individual parameters rather than group analysis.
5. Conclusions
Although gaining knowledge on the neural substrates involved in smoking cessation outcomes is crucial to guide treatments, our narrative synthesis of the literature emphasizes that this field of research is still in its infancy, with too little empirical evidence and important methodological heterogeneity. However, it is noteworthy that the findings reported here seem to converge towards a pivotal role of the insula in the modulation of inter-related brain networks. Adequately powered studies, allowing to take into account heterogeneity across treatment-seeking smokers are needed to confirm this suggestion. In addition, if functional connectivity analyses appear the most promising strategy, up to now only static connectivity patterns have been examined. Given that the insula is a well-known hub that exhibits versatile and highly flexible connectivity patterns with disparate brain networks [75], we believe that characterizing its dynamic connectivity patterns (i.e, modular architectures of evolving networks analyses, also called time-varying changes in functional connectivity) would be a more ecologically valid and informative method for understanding the timing of the balance between the implicated networks.
Supplementary Materials
The following are available online at https://www.mdpi.com/article/10.3390/biology11010035/s1, Figure S1: Study flow diagram.
Author Contributions
All authors had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Conceptualization, S.B., I.S. and Y.R.; Investigation, S.B., S.C., M.A. and Y.R. Writing-Original Draft, S.B., S.C. and Y.R.; Writing-Review & Editing, S.B., I.S., S.C. and Y.R.; Supervision, S.B. and I.S. All authors have read and agreed to the published version of the manuscript.
Funding
Yolaine Rabat is a PhD fellow funded by the Ministry of Research and Higher Education.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
Yolaine Rabat and Majd Abdallah declare no conflict of interest. Sandra Chanraud has received fees for editorial activities with Wiley. Igor Sibon has received fees for editorial activities with Elsevier, has served as an advisor for Servier and Boehringer Ingelheim, has received teaching honoraria from Medtronic and Bayer. Sylvie Berthoz has received fees for editorial activities with Elsevier. The French Ministry of Research and Higher Education had no role in the design, execution, interpretation, or writing of the study.
Abbreviations
| ACC | anterior cingular cortex |
| DMN | Default Mode Network |
| FTND | Fagerstrom Test for Nicotine Dependence |
| GMV | grey matter volume |
| IC | inhibitory control |
| IFG | inferior frontal gyrus |
| MFG | middle frontal gyrus |
| MRI | Magnetic Resonance Imaging |
| MTG | middle temporal gyrus |
| NRT | nicotine replacement therapies |
| PCC | posterior cingulate cortex |
| PCS | psychological counselling sessions |
| PFC | prefrontal cortex |
| ReHo | regional homogeneity |
| ROIs | regions of interests |
| RS | resting-state |
| SFG | superior frontal gyrus |
| STG | superior temporal gyrus |
| STG | superior temporal gyrus |
| tbFC | task-based functional connectivity |
| VBM | voxel-based morphometry |
| WB | whole brain |
References
- Reitsma, M.B.; Kendrick, P.J.; Ababneh, E.; Abbafati, C.; Abbasi-Kangevari, M.; Abdoli, A.; Abedi, A.; Abhilash, E.S.; Abila, D.B.; Aboyans, V.; et al. Spatial, Temporal, and Demographic Patterns in Prevalence of Smoking Tobacco Use and Attributable Disease Burden in 204 Countries and Territories, 1990–2019: A Systematic Analysis from the Global Burden of Disease Study 2019. Lancet 2021, 397, 2337–2360. [Google Scholar] [CrossRef]
- Ribassin-Majed, L.; Hill, C. Trends in Tobacco-Attributable Mortality in France. Eur. J. Public Health 2015, 25, 824–828. [Google Scholar] [CrossRef] [PubMed]
- Hughes, J.R.; Keely, J.; Naud, S. Shape of the Relapse Curve and Long-Term Abstinence among Untreated Smokers. Addiction 2004, 99, 29–38. [Google Scholar] [CrossRef]
- Livingstone-Banks, J.; Norris, E.; Hartmann-Boyce, J.; West, R.; Jarvis, M.; Hajek, P. Relapse Prevention Interventions for Smoking Cessation. Cochrane Database Syst. Rev. 2019, 2019. [Google Scholar] [CrossRef]
- Piazza, P.V.; Deroche-Gamonet, V. A Multistep General Theory of Transition to Addiction. Psychopharmacology 2013, 229, 387–413. [Google Scholar] [CrossRef] [PubMed]
- Mathew, A.R.; Hogarth, L.; Leventhal, A.M.; Cook, J.W.; Hitsman, B. Cigarette Smoking and Depression Comorbidity: Systematic Review & Proposed Theoretical Model. Addiction 2017, 112, 401–412. [Google Scholar] [PubMed]
- Fatseas, M.; Serre, F.; Alexandre, J.-M.; Debrabant, R.; Auriacombe, M.; Swendsen, J. Craving and Substance Use among Patients with Alcohol, Tobacco, Cannabis or Heroin Addiction: A Comparison of Substance- and Person-Specific Cues: Cues, Craving and Substance Use. Addiction 2015, 110, 1035–1042. [Google Scholar] [CrossRef]
- Cahill, K.; Stevens, S.; Perera, R.; Lancaster, T. Pharmacological Interventions for Smoking Cessation: An Overview and Network Meta-Analysis. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef]
- Garcia-Rivas, V.; Deroche-Gamonet, V. Not All Smokers Appear to Seek Nicotine for the Same Reasons: Implications for Preclinical Research in Nicotine Dependence. Addict. Biol. 2019, 24, 317–334. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Xu, X.; Qian, W.; Shen, Z.; Zhang, M. Altered Human Brain Anatomy in Chronic Smokers: A Review of Magnetic Resonance Imaging Studies. Neurol. Sci. 2015, 36, 497–504. [Google Scholar] [CrossRef]
- Zhou, S.; Xiao, D.; Peng, P.; Wang, S.-K.; Liu, Z.; Qin, H.-Y.; Li, S.-S.; Wang, C. Effect of Smoking on Resting-State Functional Connectivity in Smokers: An FMRI Study: Effects of Smoking on Brain Function. Respirology 2017, 22, 1118–1124. [Google Scholar] [CrossRef]
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Fagerstrom, K.-O. The Fagerstrom Test for Nicotine Dependence: A Revision of the Fagerstrom Tolerance Questionnaire. Addiction 1991, 86, 1119–1127. [Google Scholar] [CrossRef]
- National Research Council (US) Committee on A Framework for Developing a New Taxonomy of Disease. Toward Precision Medicine: Building a Knowledge Network for Biomedical Research and a New Taxonomy of Disease; National Academies Press: Washington, DC, USA, 2011; p. 13284. [Google Scholar] [CrossRef]
- Naqvi, N.H.; Rudrauf, D.; Damasio, H.; Bechara, A. Damage to the Insula Disrupts Addiction to Cigarette Smoking. Science 2007, 315, 531–534. [Google Scholar] [CrossRef]
- Froeliger, B.; McConnell, P.A.; Bell, S.; Sweitzer, M.; Kozink, R.V.; Eichberg, C.; Hallyburton, M.; Kaiser, N.; Gray, K.M.; McClernon, F.J. Association Between Baseline Corticothalamic-Mediated Inhibitory Control and Smoking Relapse Vulnerability. JAMA Psychiatry 2017, 74, 379. [Google Scholar] [CrossRef]
- Froeliger, B.; Kozink, R.V.; Rose, J.E.; Behm, F.M.; Salley, A.N.; McClernon, F.J. Hippocampal and Striatal Gray Matter Volume Are Associated with a Smoking Cessation Treatment Outcome: Results of an Exploratory Voxel-Based Morphometric Analysis. Psychopharmacology 2010, 210, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Huang, P.; Shen, Z.; Qian, W.; Li, K.; Luo, X.; Zeng, Q.; Guo, T.; Yu, H.; Yang, Y.; et al. Gray Matter Volumes of Insular Subregions Are Not Correlated with Smoking Cessation Outcomes but Negatively Correlated with Nicotine Dependence Severity in Chronic Smokers. Neurosci. Lett. 2019, 696, 7–12. [Google Scholar] [CrossRef]
- Qian, W.; Huang, P.; Shen, Z.; Wang, C.; Yang, Y.; Zhang, M. Brain Gray Matter Volume and Functional Connectivity Are Associated With Smoking Cessation Outcomes. Front. Hum. Neurosci. 2019, 13, 361. [Google Scholar] [CrossRef]
- Wang, C.; Wang, S.; Shen, Z.; Qian, W.; Jiaerken, Y.; Luo, X.; Li, K.; Zeng, Q.; Gu, Q.; Yang, Y.; et al. Increased Thalamic Volume and Decreased Thalamo-Precuneus Functional Connectivity Are Associated with Smoking Relapse. NeuroImage Clin. 2020, 28, 102451. [Google Scholar] [CrossRef] [PubMed]
- Good, C.D.; Johnsrude, I.S.; Ashburner, J.; Henson, R.N.A.; Friston, K.J.; Frackowiak, R.S.J. A Voxel-Based Morphometric Study of Ageing in 465 Normal Adult Human Brains. NeuroImage 2001, 14, 21–36. [Google Scholar] [CrossRef] [PubMed]
- Huang, P.; Shen, Z.; Wang, C.; Qian, W.; Zhang, H.; Yang, Y.; Zhang, M. Altered White Matter Integrity in Smokers Is Associated with Smoking Cessation Outcomes. Front. Hum. Neurosci. 2017, 11, 438. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Wang, S.; Huang, P.; Shen, Z.; Qian, W.; Luo, X.; Li, K.; Zeng, Q.; Gu, Q.; Yu, H.; et al. Abnormal White Matter Tracts of Insula in Smokers. Brain Imaging Behav. 2021, 15, 1955–1965. [Google Scholar] [CrossRef] [PubMed]
- Biswal, B.B. Resting State FMRI: A Personal History. NeuroImage 2012, 62, 938–944. [Google Scholar] [CrossRef] [PubMed]
- Buckner, R.L.; Krienen, F.M. The Evolution of Distributed Association Networks in the Human Brain. Trends Cogn. Sci. 2013, 17, 648–665. [Google Scholar] [CrossRef] [PubMed]
- Sweitzer, M.; Geier, C.F.; Denlinger, R.; Forbes, E.E.; Raiff, B.R.; Dallery, J.; McClernon, F.J.; Donny, E.C. Blunted Striatal Response to Monetary Reward Anticipation during Smoking Abstinence Predicts Lapse during a Contingency-Managed Quit Attempt. Psychopharmacology 2016, 233, 751–760. [Google Scholar] [CrossRef]
- Addicott, M.A.; Sweitzer, M.M.; Froeliger, B.; Rose, J.E.; McClernon, F.J. Increased Functional Connectivity in an Insula-Based Network Is Associated with Improved Smoking Cessation Outcomes. Neuropsychopharmacology 2015, 40, 2648–2656. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, C.E.; Calhoun, V.D.; Rachakonda, S.; Claus, E.D.; Littlewood, R.A.; Mickey, J.; Arenella, P.B.; Hutchison, K.E. Functional Network Connectivity Predicts Treatment Outcome during Treatment of Nicotine Use Disorder. Psychiatry Res. Neuroimaging 2017, 265, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Shen, Z.; Huang, P.; Qian, W.; Zhou, C.; Li, K.; Zeng, Q.; Luo, X.; Gu, Q.; Yu, H.; et al. Increased Interregional Functional Connectivity of Anterior Insula Is Associated with Improved Smoking Cessation Outcome. Brain Imaging Behav. 2019, 14, 408–415. [Google Scholar] [CrossRef]
- Wang, C.; Huang, P.; Shen, Z.; Qian, W.; Wang, S.; Jiaerken, Y.; Luo, X.; Li, K.; Zeng, Q.; Zhou, C.; et al. Increased Striatal Functional Connectivity Is Associated with Improved Smoking Cessation Outcomes: A Preliminary Study. Addict. Biol. 2021, 26, e12919. [Google Scholar] [CrossRef] [PubMed]
- Zang, Y.; Jiang, T.; Lu, Y.; He, Y.; Tian, L. Regional Homogeneity Approach to FMRI Data Analysis. NeuroImage 2004, 22, 394–400. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Shen, Z.; Huang, P.; Qian, W.; Yu, X.; Sun, J.; Yu, H.; Yang, Y.; Zhang, M. Altered Spontaneous Activity of Posterior Cingulate Cortex and Superior Temporal Gyrus Are Associated with a Smoking Cessation Treatment Outcome Using Varenicline Revealed by Regional Homogeneity. Brain Imaging Behav. 2017, 11, 611–618. [Google Scholar] [CrossRef]
- Lohmann, G.; Margulies, D.S.; Horstmann, A.; Pleger, B.; Lepsien, J.; Goldhahn, D.; Schloegl, H.; Stumvoll, M.; Villringer, A.; Turner, R. Eigenvector Centrality Mapping for Analyzing Connectivity Patterns in FMRI Data of the Human Brain. PLoS ONE 2010, 5, e10232. [Google Scholar] [CrossRef] [PubMed]
- Shen, Z.; Huang, P.; Wang, C.; Qian, W.; Yang, Y.; Zhang, M. Increased Network Centrality as Markers of Relapse Risk in Nicotine-Dependent Individuals Treated with Varenicline. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2017, 75, 142–147. [Google Scholar] [CrossRef]
- Gilman, J.M.; Radoman, M.; Schuster, R.M.; Pachas, G.; Azzouz, N.; Fava, M.; Evins, A.E. Anterior Insula Activation during Inhibition to Smoking Cues Is Associated with Ability to Maintain Tobacco Abstinence. Addict. Behav. Rep. 2018, 7, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Courtney, K.E.; Schacht, J.P.; Hutchison, K.; Roche, D.J.O.; Ray, L.A. Neural Substrates of Cue Reactivity: Association with Treatment Outcomes and Relapse: Cue Reactivity and Outcomes. Addict. Biol. 2016, 21, 3–22. [Google Scholar] [CrossRef] [PubMed]
- Hartwell, K.J.; LeMatty, T.; McRae-Clark, A.L.; Gray, K.M.; George, M.S.; Brady, K.T. Resisting the Urge to Smoke and Craving during a Smoking Quit Attempt on Varenicline: Results from a Pilot FMRI Study. Am. J. Drug Alcohol Abus. 2013, 39, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Janes, A.C.; Pizzagalli, D.A.; Richardt, S.; de Frederick, B.B.; Chuzi, S.; Pachas, G.; Culhane, M.A.; Holmes, A.J.; Fava, M.; Evins, A.E.; et al. Brain Reactivity to Smoking Cues Prior to Smoking Cessation Predicts Ability to Maintain Tobacco Abstinence. Biol. Psychiatry 2010, 67, 722–729. [Google Scholar] [CrossRef]
- Allenby, C.; Falcone, M.; Wileyto, E.P.; Cao, W.; Bernardo, L.; Ashare, R.L.; Janes, A.; Loughead, J.; Lerman, C. Neural Cue Reactivity during Acute Abstinence Predicts Short-term Smoking Relapse. Addict. Biol. 2020, 25, e12733. [Google Scholar] [CrossRef] [PubMed]
- McClernon, F.J.; Hiott, F.B.; Liu, J.; Salley, A.N.; Behm, F.M.; Rose, J.E. Selectively Reduced Responses to Smoking Cues in Amygdala Following Extinction-Based Smoking Cessation: Results of a Preliminary Functional Magnetic Resonance Imaging Study. Addict. Biol. 2007, 12, 503–512. [Google Scholar] [CrossRef] [PubMed]
- Owens, M.M.; MacKillop, J.; Gray, J.C.; Beach, S.R.H.; Stein, M.D.; Niaura, R.S.; Sweet, L.H. Neural Correlates of Tobacco Cue Reactivity Predict Duration to Lapse and Continuous Abstinence in Smoking Cessation Treatment: Neural Correlates of Tobacco Cue Reactivity. Addict. Biol. 2018, 23, 1189–1199. [Google Scholar] [CrossRef] [PubMed]
- Janes, A.C.; Gilman, J.M.; Radoman, M.; Pachas, G.; Fava, M.; Evins, A.E. Revisiting the Role of the Insula and Smoking Cue-Reactivity in Relapse: A Replication and Extension of Neuroimaging Findings. Drug Alcohol Depend. 2017, 179, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Chua, H.F.; Ho, S.S.; Jasinska, A.J.; Polk, T.A.; Welsh, R.C.; Liberzon, I.; Strecher, V.J. Self-Related Neural Response to Tailored Smoking-Cessation Messages Predicts Quitting. Nat. Neurosci. 2011, 14, 426–427. [Google Scholar] [CrossRef] [PubMed]
- Owens, M.M.; MacKillop, J.; Gray, J.C.; Hawkshead, B.E.; Murphy, C.M.; Sweet, L.H. Neural Correlates of Graphic Cigarette Warning Labels Predict Smoking Cessation Relapse. Psychiatry Res. Neuroimaging 2017, 262, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Sweitzer, M.M.; Geier, C.F.; Addicott, M.A.; Denlinger, R.; Raiff, B.R.; Dallery, J.; McClernon, F.J.; Donny, E.C. Smoking Abstinence-Induced Changes in Resting State Functional Connectivity with Ventral Striatum Predict Lapse During a Quit Attempt. Neuropsychopharmacology 2016, 41, 2521–2529. [Google Scholar] [CrossRef]
- Grosskopf, C.M.; Kroemer, N.B.; Pooseh, S.; Böhme, F.; Smolka, M.N. Temporal Discounting and Smoking Cessation: Choice Consistency Predicts Nicotine Abstinence in Treatment-Seeking Smokers. Psychopharmacology 2021, 238, 399–410. [Google Scholar] [CrossRef]
- Friston, K.J. Functional and Effective Connectivity: A Review. Brain Connect. 2011, 1, 13–36. [Google Scholar] [CrossRef]
- Naqvi, N.H.; Bechara, A. The Role of the Insula in Goal-Directed Drug Seeking and Choice in Addiction. In Addiction and Choice; Heather, N., Segal, G., Eds.; Oxford University Press: Oxford, UK, 2016; pp. 205–224. [Google Scholar] [CrossRef]
- Abdolahi, A.; Williams, G.C.; Benesch, C.G.; Wang, H.Z.; Spitzer, E.M.; Scott, B.E.; Block, R.C.; van Wijngaarden, E. Smoking Cessation Behaviors Three Months Following Acute Insular Damage from Stroke. Addict. Behav. 2015, 51, 24–30. [Google Scholar] [CrossRef]
- Suñer-Soler, R.; Grau, A.; Gras, M.E.; Font-Mayolas, S.; Silva, Y.; Dávalos, A.; Cruz, V.; Rodrigo, J.; Serena, J. Smoking Cessation 1 Year Poststroke and Damage to the Insular Cortex. Stroke 2012, 43, 131–136. [Google Scholar] [CrossRef]
- Abdolahi, A.; Williams, G.C.; Benesch, C.G.; Wang, H.Z.; Spitzer, E.M.; Scott, B.E.; Block, R.C.; van Wijngaarden, E. Damage to the Insula Leads to Decreased Nicotine Withdrawal during Abstinence: Insular Damage and Withdrawal during Abstinence. Addiction 2015, 110, 1994–2003. [Google Scholar] [CrossRef]
- Abdolahi, A.; Williams, G.C.; Benesch, C.G.; Wang, H.Z.; Spitzer, E.M.; Scott, B.E.; Block, R.C.; van Wijngaarden, E. Immediate and Sustained Decrease in Smoking Urges After Acute Insular Cortex Damage. Nicotine Tob. Res. 2017, 19, 756–762. [Google Scholar] [CrossRef]
- Menon, V.; Uddin, L.Q. Saliency, Switching, Attention and Control: A Network Model of Insula Function. Brain Struct Funct 2010, 214, 655–667. [Google Scholar] [CrossRef]
- Hariri, A.R.; Brown, S.M.; Williamson, D.E.; Flory, J.D.; de Wit, H.; Manuck, S.B. Preference for Immediate over Delayed Rewards is Associated with Magnitude of Ventral Striatal Activity. J. Neurosci. 2006, 26, 13213–13217. [Google Scholar] [CrossRef]
- Luijten, M.; Schellekens, A.F.; Kühn, S.; Machielse, M.W.J.; Sescousse, G. Disruption of Reward Processing in Addiction: An Image-Based Meta-Analysis of Functional Magnetic Resonance Imaging Studies. JAMA Psychiatry 2017, 74, 387. [Google Scholar] [CrossRef] [PubMed]
- David, S.P.; Munafò, M.R.; Johansen-Berg, H.; Smith, S.M.; Rogers, R.D.; Matthews, P.M.; Walton, R.T. Ventral Striatum/Nucleus Accumbens Activation to Smoking-Related Pictorial Cues in Smokers and Nonsmokers: A Functional Magnetic Resonance Imaging Study. Biol. Psychiatry 2005, 58, 488–494. [Google Scholar] [CrossRef]
- Franklin, T.R.; Wang, Z.; Wang, J.; Sciortino, N.; Harper, D.; Li, Y.; Ehrman, R.; Kampman, K.; O’Brien, C.P.; Detre, J.A.; et al. Limbic Activation to Cigarette Smoking Cues Independent of Nicotine Withdrawal: A Perfusion FMRI Study. Neuropsychopharmacol 2007, 32, 2301–2309. [Google Scholar] [CrossRef]
- Wang, Z.; Faith, M.; Patterson, F.; Tang, K.; Kerrin, K.; Wileyto, E.P.; Detre, J.A.; Lerman, C. Neural Substrates of Abstinence-Induced Cigarette Cravings in Chronic Smokers. J. Neurosci. 2007, 27, 14035–14040. [Google Scholar] [CrossRef]
- Jing, C.; Jing, C.; Zheng, L.; Hong, G.; Zheng, J.; Yu, L.; Song, N.; Zhang, T.; Ma, Q.; Fang, J. Disruption of Cigarette Smoking Addiction After Dorsal Striatum Damage. Front. Behav. Neurosci. 2021, 15, 646337. [Google Scholar] [CrossRef]
- Gaznick, N.; Tranel, D.; McNutt, A.; Bechara, A. Basal Ganglia plus Insula Damage Yields Stronger Disruption of Smoking Addiction than Basal Ganglia Damage Alone. Nicotine Tob. Res. 2014, 16, 445–453. [Google Scholar] [CrossRef] [PubMed]
- Noël, X.; Brevers, D.; Bechara, A. A Triadic Neurocognitive Approach to Addiction for Clinical Interventions. Front. Psychiatry 2013, 4, 179. [Google Scholar] [CrossRef]
- Piasecki, T.M. Relapse to Smoking. Clin. Psychol. Rev. 2006, 26, 196–215. [Google Scholar] [CrossRef]
- Alboksmaty, A.; Agaku, I.T.; Odani, S.; Filippidis, F.T. Prevalence and Determinants of Cigarette Smoking Relapse among US Adult Smokers: A Longitudinal Study. BMJ Open 2019, 9, e031676. [Google Scholar] [CrossRef]
- Fluharty, M.; Taylor, A.E.; Grabski, M.; Munafò, M.R. The Association of Cigarette Smoking With Depression and Anxiety: A Systematic Review. Nicotine Tob. Res. 2017, 19, 3–13. [Google Scholar] [CrossRef]
- Paulus, M.P.; Stewart, J.L. Interoception and Drug Addiction. Neuropharmacology 2014, 76, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Spada, M.M.; Caselli, G.; Nikčević, A.V.; Wells, A. Metacognition in Addictive Behaviors. Addict. Behav. 2015, 44, 9–15. [Google Scholar] [CrossRef]
- Flaudias, V.; Heeren, A.; Brousse, G.; Maurage, P. Toward a Triadic Approach to Craving in Addictive Disorders: The Metacognitive Hub Model. Harv. Rev. Psychiatry 2019, 27, 326–331. [Google Scholar] [CrossRef] [PubMed]
- Durazzo, T.; Meyerhoff, D.; Murray, D. Comparison of Regional Brain Perfusion Levels in Chronically Smoking and Non-Smoking Adults. Int. J. Environ. Res. Public Health 2015, 12, 8198–8213. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, R.C.; Baldoni, P.L.; Strizich, G.M.; Pérez-Stable, E.J.; Saccone, N.L.; Peralta, C.A.; Perreira, K.M.; Gellman, M.D.; Williams-Nguyen, J.S.; Rodriguez, C.J.; et al. Current Smoking Raises Risk of Incident Hypertension: Hispanic Community Health Study–Study of Latinos. Am. J. Hypertens. 2021, 34, 190–197. [Google Scholar] [CrossRef]
- Haight, T.J.; Bryan, R.N.; Erus, G.; Davatzikos, C.; Jacobs, D.R.; D’Esposito, M.; Lewis, C.E.; Launer, L.J. Vascular Risk Factors, Cerebrovascular Reactivity, and the Default-Mode Brain Network. NeuroImage 2015, 115, 7–16. [Google Scholar] [CrossRef]
- Gray, J.C.; Thompson, M.; Bachman, C.; Owens, M.M.; Murphy, M.; Palmer, R. Associations of Cigarette Smoking with Gray and White Matter in the UK Biobank. Neuropsychopharmacol 2020, 45, 1215–1222. [Google Scholar] [CrossRef]
- Sutherland, M.T.; Riedel, M.C.; Flannery, J.S.; Yanes, J.A.; Fox, P.T.; Stein, E.A.; Laird, A.R. Chronic Cigarette Smoking Is Linked with Structural Alterations in Brain Regions Showing Acute Nicotinic Drug-Induced Functional Modulations. Behav. Brain Funct. 2016, 12, 16. [Google Scholar] [CrossRef]
- Kim, S.H.; Yun, C.-H.; Lee, S.-Y.; Choi, K.; Kim, M.B.; Park, H.-K. Age-Dependent Association between Cigarette Smoking on White Matter Hyperintensities. Neurol. Sci. 2012, 33, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Power, M.C.; Deal, J.A.; Sharrett, A.R.; Jack, C.R.; Knopman, D.; Mosley, T.H.; Gottesman, R.F. Smoking and White Matter Hyperintensity Progression: The ARIC-MRI Study. Neurology 2015, 84, 841–848. [Google Scholar] [CrossRef] [PubMed]
- Zubieta, J.-K.; Heitzeg, M.M.; Xu, Y.; Koeppe, R.A.; Ni, L.; Guthrie, S.; Domino, E.F. Regional Cerebral Blood Flow Responses to Smoking in Tobacco Smokers After Overnight Abstinence. Am. J. Psychiatry 2005, 162, 567–577. [Google Scholar] [CrossRef] [PubMed]
- Nomi, J.S.; Farrant, K.; Damaraju, E.; Rachakonda, S.; Calhoun, V.D.; Uddin, L.Q. Dynamic Functional Network Connectivity Reveals Unique and Overlapping Profiles of Insula Subdivisions: Dynamic Connections of Insula Subdivisions. Hum. Brain Mapp. 2016, 37, 1770–1787. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).