
Evaluation of Hepatic Biochemical Parameters during Antiviral Treatment in COVID-19 Patients



 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
- -
- for Favipiravir, hepatocytolysis and cholestasis syndrome (GOT, GPT, GGT, ALP, and total as well as uric acid value)
- -
- for Remdesivir, hepatocytolysis and cholestasis syndrome (GOT, GPT, GGT, ALP, and total as well as the value of neutrophils and platelets)
- -
- for Lopinavir/Ritonavir, hepatocytolysis syndrome, cholestasis, as well as the value of neutrophils and platelets.
3. Results
3.1. Characteristics of the Population (Sex, Age, and Environment)
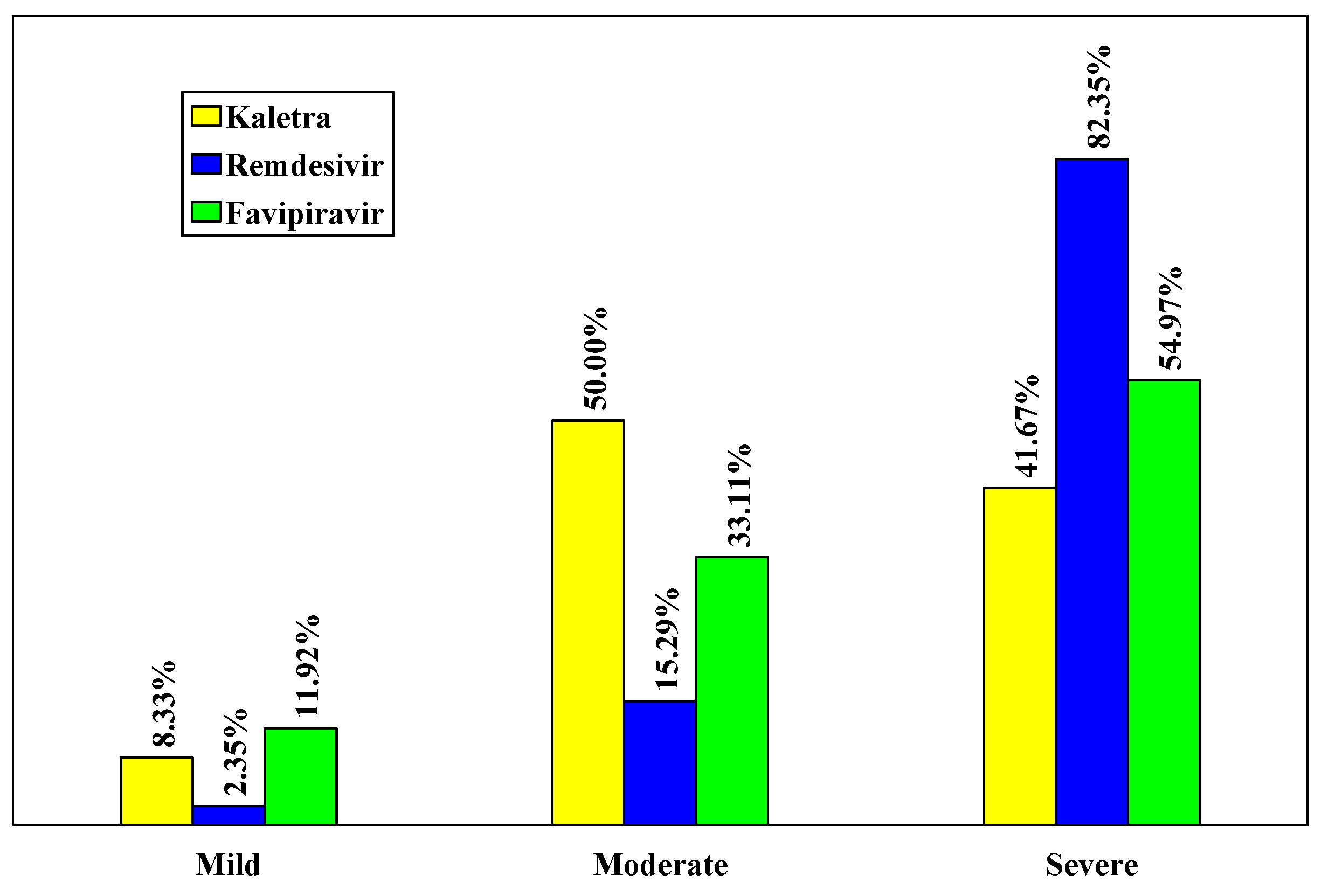
3.2. The Severity of the Disease
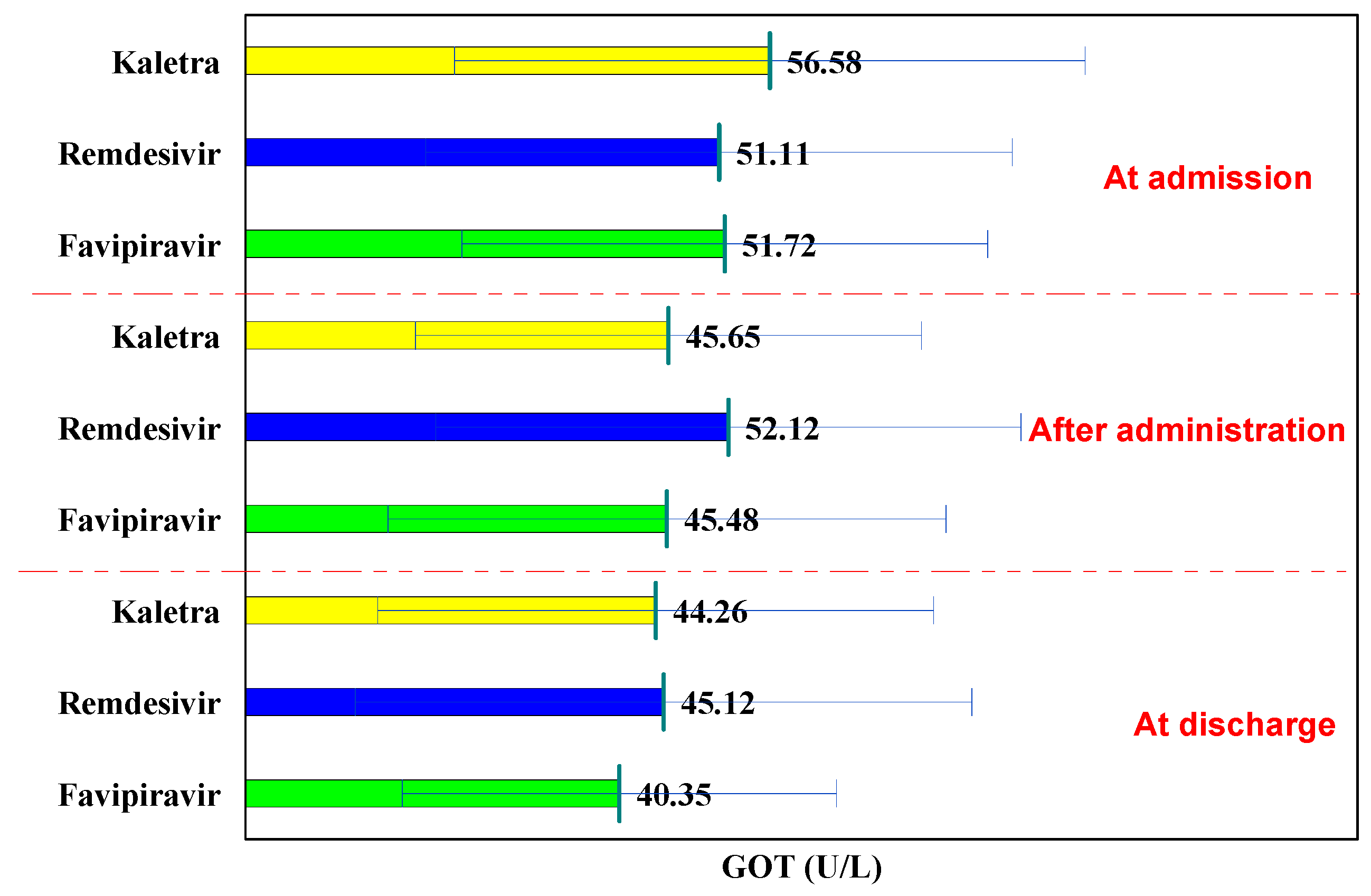
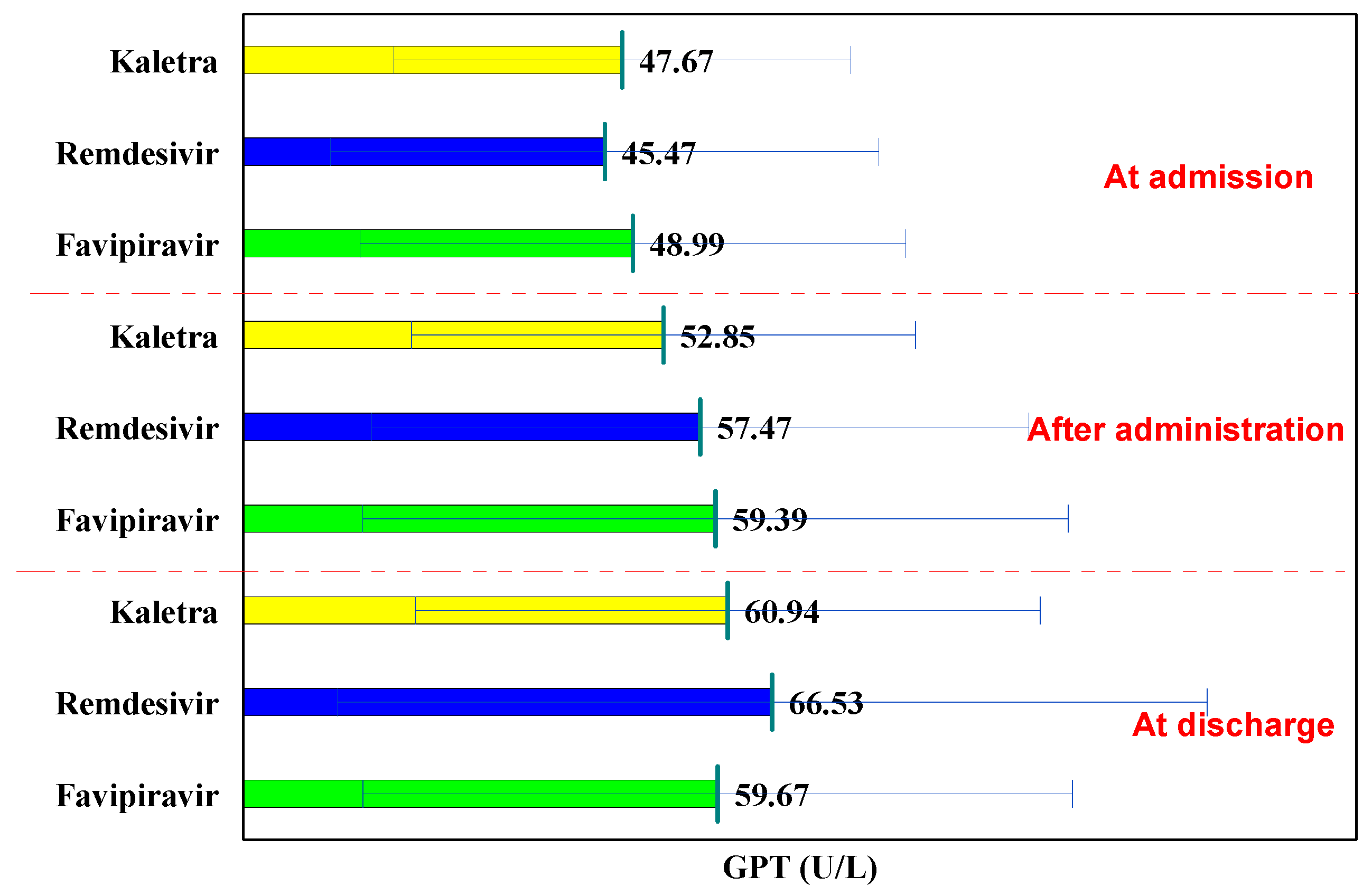
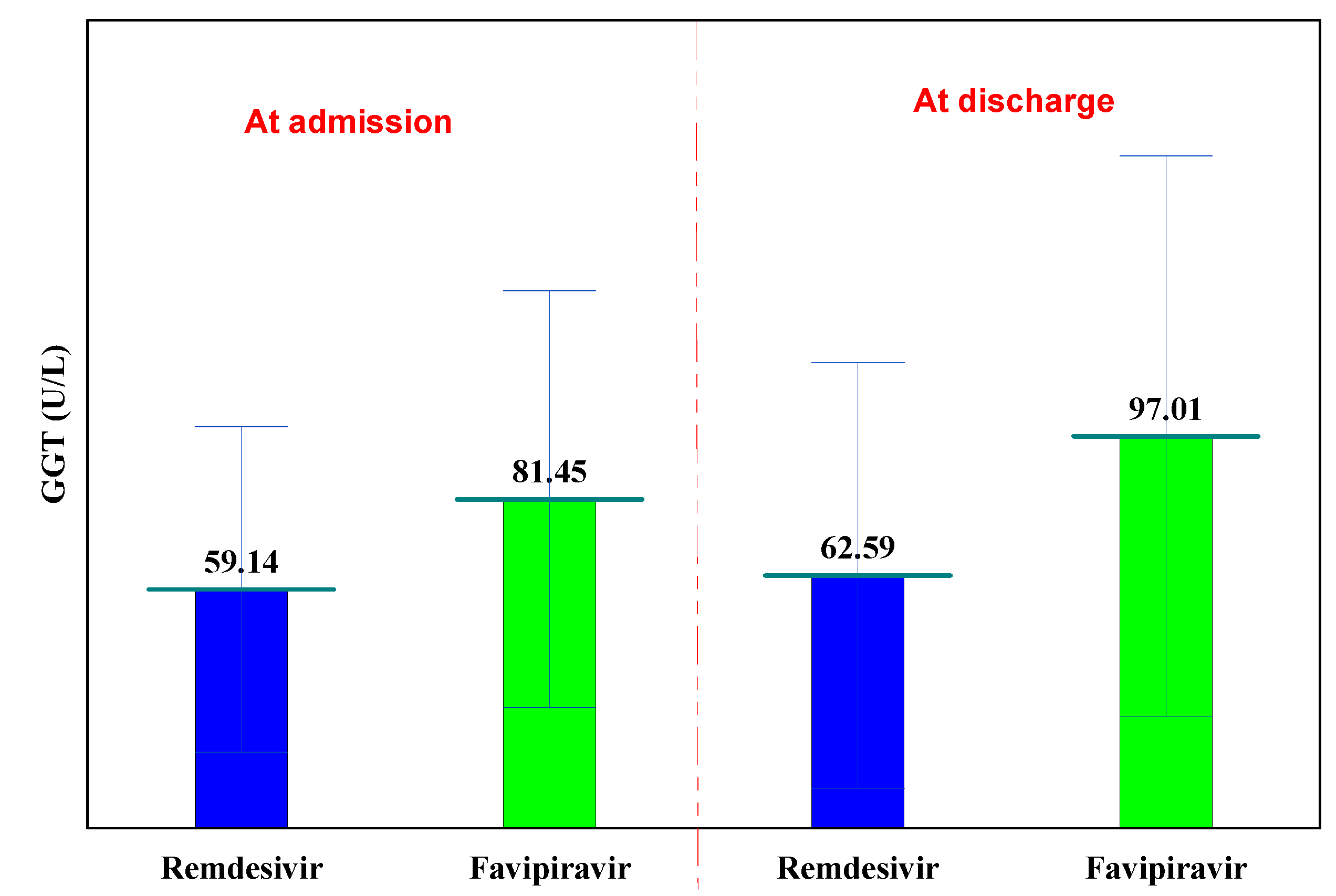
3.3. Evolution of Hepatic Function Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. China Novel Coronavirus Investigating and Research Team. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Van de Veerdonk, F.L.; Netea, M.G.; van Deuren, M.; van der Meer, J.W.; de Mast, Q.; Brüggemann, R.J.; van der Hoeven, H. Kallikrein-kinin blockade in patients with COVID-19 to prevent acute respiratory distress syndrome. Elife 2020, 9, e57555. [Google Scholar] [CrossRef]
- Leisman, D.E.; Ronner, L.; Pinotti, R.; Taylor, M.D.; Sinha, P.; Calfee, C.S.; Hirayama, A.V.; Mastroiani, F.; Turtle, C.J.; Harhay, M.O.; et al. Cytokine elevation in severe and critical COVID-19: A rapid systematic review, meta-analysis, and comparison with other inflammatory syndromes. Lancet Respir. Med. 2020, 8, 1233–1244. [Google Scholar] [CrossRef]
- Cummings, M.J.; Baldwin, M.R.; Abrams, D.; Jacobson, S.D.; Meyer, B.J.; Balough, E.M.; Aaron, J.G.; Claassen, J.; Rabbani, L.E.; Hastie, J.; et al. Epidemiology, clinical course, and outcomes of critically ill adults with COVID-19 in New York City: A prospective cohort study. Lancet 2020, 395, 1763–1770. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Liu, L.; Zhang, D.; Xu, J.; Dai, H.; Tang, N.; Su, X.; Cao, B. SARS-CoV-2 and viral sepsis: Observations and hypotheses. Lancet 2020, 395, 1517–1520. [Google Scholar] [CrossRef]
- Zou, X.; Chen, K.; Zou, J.; Han, P.; Hao, J.; Han, Z. Single-cell RNA-seq data analysis on the receptor ACE2 expression reveals the potential risk of different human organs vulnerable to 2019-nCoV infection. Front. Med. 2020, 14, 185–192. [Google Scholar] [CrossRef] [Green Version]
- Ruzzenetti, G.; Maloberti, A.; Giani, V.; Bolcati, M.; Leidi, F.; Monticelli, M.; Grasso, E.; Cartella, I.; Palazzini, M.; Garatti, L.; et al. Covid and Cardiovascular Diseases: Direct and Indirect Damages and Future Perspective. High Blood Press. Cardiovasc. Prev. 2021, 28, 439–445. [Google Scholar] [CrossRef]
- Yao, X.H.; Li, T.Y.; He, Z.C.; Ping, Y.F.; Liu, H.W.; Yu, S.C.; Mou, H.M.; Wang, L.H.; Zhang, H.R.; Fu, W.J.; et al. A pathological report of three COVID-19 cases by minimally invasive autopsies. Zhonghua Bing Li Xue Za Zhi 2020, 49, 411–417. [Google Scholar]
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L.; et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef]
- Li, H.; Chen, C.; Hu, F.; Wang, J.; Zhao, Q.; Gale, R.P.; Liang, Y. Impact of corticosteroid therapy on outcomes of persons with SARS-CoV-2, SARS-CoV, or MERS-CoV infection: A systematic review and meta-analysis. Leukemia 2020, 34, 1503–1511. [Google Scholar] [CrossRef] [PubMed]
- Luke, T.C.; Kilbane, E.M.; Jackson, J.L.; Hoffman, S.L. Meta-analysis: Convalescent blood products for Spanish influenza pneumonia: A future H5N1 treatment? Ann. Intern. Med. 2006, 145, 599–609. [Google Scholar] [CrossRef] [PubMed]
- Davey, R.T.; Fernández-Cruz, E.; Markowitz, N.; Pett, S.; Babiker, A.G.; Wentworth, D.; Khurana, S.; Engen, N.; Gordin, F.; Jain, M.K.; et al. Anti-influenza hyperimmune intravenous immunoglobulin for adults with influenza A or B infection (FLU-IVIG): A double-blind, randomised, placebo-controlled trial. Lancet Respir. Med. 2019, 7, 951–963. [Google Scholar] [CrossRef] [Green Version]
- Rojas, M.; Rodríguez, Y.; Monsalve, D.M.; Acosta-Ampudia, Y.; Camacho, B.; Gallo, J.E.; Rojas-Villarraga, A.; Ramírez-Santana, C.; Díaz-Coronado, J.C.; Manrique, R.; et al. Convalescent plasma in Covid-19: Possible mechanisms of action. Autoimmun. Rev. 2020, 19, 102554. [Google Scholar] [CrossRef]
- Zhang, Y.; Xiao, M.; Zhang, S.; Xia, P.; Cao, W.; Jiang, W.; Chen, H.; Ding, X.; Zhao, H.; Zhang, H.; et al. Coagulopathy and antiphospholipid antibodies in patients with Covid-19. N. Engl. J. Med. 2020, 382, e38. [Google Scholar] [CrossRef] [PubMed]
- Tang, N.; Bai, H.; Chen, X.; Gong, J.; Li, D.; Sun, Z. Anticoagulant treatment is associated with decreased mortality in severe Coronavirus disease 2019 patients with coagulopathy. J. Thromb. Haemost. 2020, 18, 1094–1099. [Google Scholar] [CrossRef]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef] [Green Version]
- Pruijssers, A.J.; George, A.S.; Schäfer, A.; Leist, S.R.; Gralinksi, L.E.; Dinnon, K.H.; Yount, B.L.; Agostini, M.L.; Stevens, L.J.; Chappell, J.D.; et al. Remdesivir inhibits SARS-CoV-2 in human lung cells and chimeric SARS-CoV expressing the SARS-CoV-2 RNA polymerase in mice. Cell Rep. 2020, 32, 107940. [Google Scholar] [CrossRef]
- Yoo, J.H. Uncertainty about the efficacy of Remdesivir on COVID-19. J. Korean Med. Sci. 2020, 35, e221. [Google Scholar] [CrossRef]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): A review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Jaiswal, P.; Kerakhan, Y.; Saravanan, L.; Murtaza, Z.; Zergham, A.; Honganur, N.S.; Akbar, A.; Deol, A.; Franci, B.; et al. Liver disease and outcomes among COVID-19 hospitalized patients—A systematic review and meta-analysis. Ann. Hepatol. 2021, 21, 100273. [Google Scholar] [CrossRef]
- Li, L.; Li, S.; Xu, M.; Yu, P.; Zheng, S.; Duan, Z.; Liu, J.; Chen, Y.; Li, J. Risk factors related to hepatic injury in patients with corona virus disease 2019. medRxiv 2020. [Google Scholar] [CrossRef]
- Sahin, T.T.; Akbulut, S.; Yilmaz, S. COVID-19 pandemic: Its impact on liver disease and liver transplantation. World J. Gastroenterol. 2020, 26, 2987–2999. [Google Scholar] [CrossRef] [PubMed]
- Altunisik, T.S.; Bayindir, Y.; Yilmaz, S.; Yalçınsoy, M.; Otlu, B.; Kose, A.; Sahin, T.T.; Akbulut, S.; Isik, B.; Başkiran, A.; et al. Short-term experiences of a liver transplant centre before and after the COVID-19 pandemic. Int. J. Clin. Pract. 2021, 75, e14668. [Google Scholar]
- Hossain, M.; Tabassum, J.; Rahman, S.B.; Roy, U.; Mitra, S.; Rafi, M.; Islam, M.R.; Nesa, M.; Emran, T.B. Clinical Efficacy and Safety of Antiviral Drugs in the Extended Use against COVID-19: What We Know So Far. Biologics 2021, 1, 252–284. [Google Scholar] [CrossRef]
- Sanders, J.M.; Monogue, M.L.; Jodlowski, T.Z.; Cutrell, J.B. Pharmacologic Treatments for Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 323, 1824–1836. [Google Scholar] [CrossRef] [PubMed]
- Lepage, M.-A.; Rozza, N.; Kremer, R.; Grunbaum, A. Safety and effectiveness concerns of lopinavir/ritonavir in COVID-19 affected patients: A retrospective series. Clin. Toxicol. 2021, 59, 644–647. [Google Scholar] [CrossRef] [PubMed]
- Parvathaneni, V.; Gupta, V. Utilizing drug repurposing against COVID-19—Efficacy, limitations, and challenges. Life Sci. 2020, 259, 118275. [Google Scholar] [CrossRef] [PubMed]
- Marra, F.; Smolders, E.J.; El-Sherif, O.; Boyle, A.; Davidson, K.; Sommerville, A.J.; Marzolini, C.; Siccardi, M.; Burger, D.; Gibbons, S.; et al. Recommendations for Dosing of Repurposed COVID-19 Medications in Patients with Renal and Hepatic Impairment. Drugs R&D 2021, 21, 9–27. [Google Scholar]
- Li, Y.; Xie, Z.; Lin, W.; Cai, W.; Wen, C.; Guan, Y.; Mo, X.; Wang, J.; Wang, Y.; Peng, P.; et al. An Exploratory Randomized Controlled Study on the Efficacy and Safety of Lopinavir/ritonavir or Arbidol Treating Adult Patients Hospitalized with Mild/moderate COVID-19 (ELACOI). medRxiv 2020. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, D.; Du, G.; Du, R.; Zhao, J.; Jin, Y.; Fu, S.; Gao, L.; Cheng, Z.; Lu, Q.; et al. Remdesivir in Adults with Severe COVID-19: A Randomised, Double-Blind, Placebo-Controlled, Multicentre Trial. Lancet 2020, 395, 1569–1578. [Google Scholar] [CrossRef]
- Zhai, G.; Li, M.; Wang, Y.; Jian, W. Drug-induced liver disturbance during treatment of Covid-19. Front. Pharmacol. 2021, 12, 719308. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | % | Min/Max | MD ± DS | |
|---|---|---|---|---|
| Sex (F/M) | 139/133 | 51.10/48.90 | ||
| Age (years) | 26–88 | 60.18 ± 13.06 | ||
| Environment (U/R) | 152/120 | 55.88/44.12 |
| Severity of the Disease | Lopinavir/Ritonavir (Kaletra) | Remdesivir | Favipiravir | |||
|---|---|---|---|---|---|---|
| Mild | 3 | 8.33% | 2 | 2.35% | 18 | 11.92% |
| Moderate | 18 | 50.00 | 13 | 15.29 | 50 | 33.11 |
| Severe | 15 | 41.67 | 70 | 82.35 | 83 | 54.97 |
| GOT | at Hospitalization | after Administration | P1−2 | at Discharge | P1−3 | P2−3 |
|---|---|---|---|---|---|---|
| Lopinavir/Ritonavir (Kaletra) | 56.58 ± 34.01 | 45.65 ± 27.30 | 0.142 | 44.26 ± 29.99 | 0.112 | 0.843 |
| Remdesivir | 51.11 ± 31.65 | 52.12 ± 31.57 | 0.834 | 45.12 ± 33.27 | 0.231 | 0.161 |
| Favipiravir | 51.72 ± 28.36 | 45.48 ± 30.11 | 0.066 | 40.35 ± 23.41 | <0.001 | 0.102 |
| pK-R | 0.412 | 0.268 | 0.892 | |||
| pK-F | 0.432 | 0.975 | 0.480 | |||
| pR-F | 0.882 | 0.117 | 0.246 |
| GPT | at Hospitalization | after Administration | P1−2 | at Discharge | P1−3 | P2−3 |
|---|---|---|---|---|---|---|
| Lopinavir/Ritonavir (Kaletra) | 47.67 ± 28.75 | 52.85 ± 31.72 | 0.477 | 60.94 ± 39.32 | 0.114 | 0.354 |
| Remdesivir | 45.47 ± 34.49 | 57.47 ± 41.36 | 0.042 | 66.53 ± 54.74 | 0.003 | 0.225 |
| Favipiravir | 48.99 ± 34.33 | 59.39 ± 44.40 | 0.025 | 59.67 ± 44.64 | 0.022 | 0.957 |
| pK-R | 0.719 | 0.514 | 0.535 | |||
| pK-F | 0.812 | 0.322 | 0.869 | |||
| pR-F | 0.453 | 0.740 | 0.328 |
| GGT | at Hospitalization | at Discharge | P1−3 |
|---|---|---|---|
| Remdesivir | 59.14 ± 40.27 | 62.59 ± 52.77 | 0.633 |
| Favipiravir | 81.45 ± 51.56 | 97.01 ± 69.41 | 0.437 |
| pR-F | 0.055 | 0.067 |
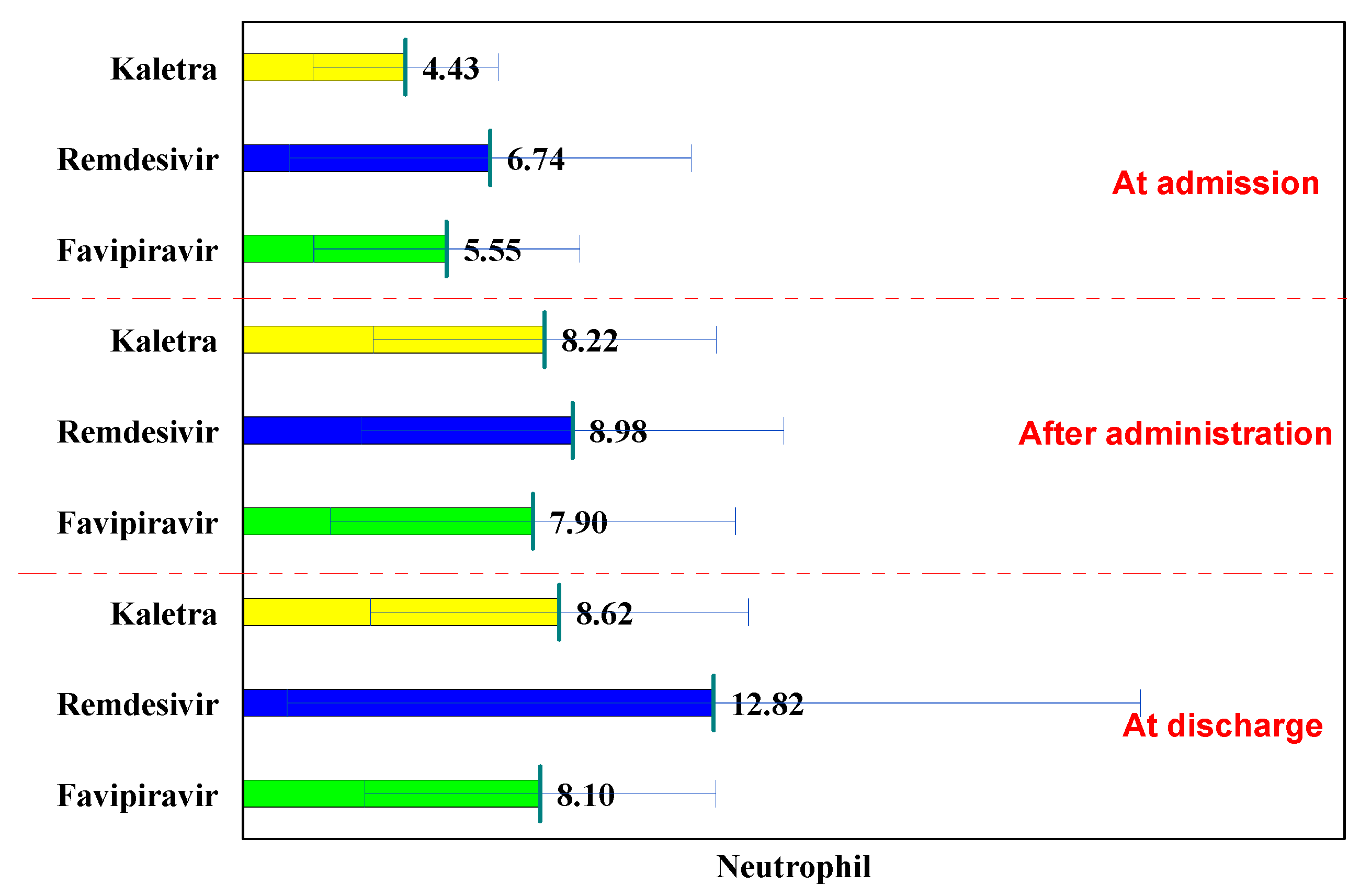
| Neutrophils | at Hospitalization | after Administration | P1−2 | at Discharge | P1−3 | P2−3 |
|---|---|---|---|---|---|---|
| Lopinavir/Ritonavir (Kaletra) | 4.43 ± 2.52 | 8.22 ± 4.67 | <0.001 | 8.62 ± 5.15 | <0.001 | 0.740 |
| Remdesivir | 6.74 ± 5.47 | 8.98 ± 5.75 | 0.010 | 12.82 ± 11.62 | <0.001 | 0.007 |
| Favipiravir | 5.55 ± 3.62 | 7.90 ± 5.51 | <0.001 | 8.10 ± 4.78 | <0.001 | 0.737 |
| pK-R | 0.002 | 0.460 | 0.007 | |||
| pK-F | 0.034 | 0.727 | 0.595 | |||
| pR-F | 0.077 | 0.165 | 0.001 |
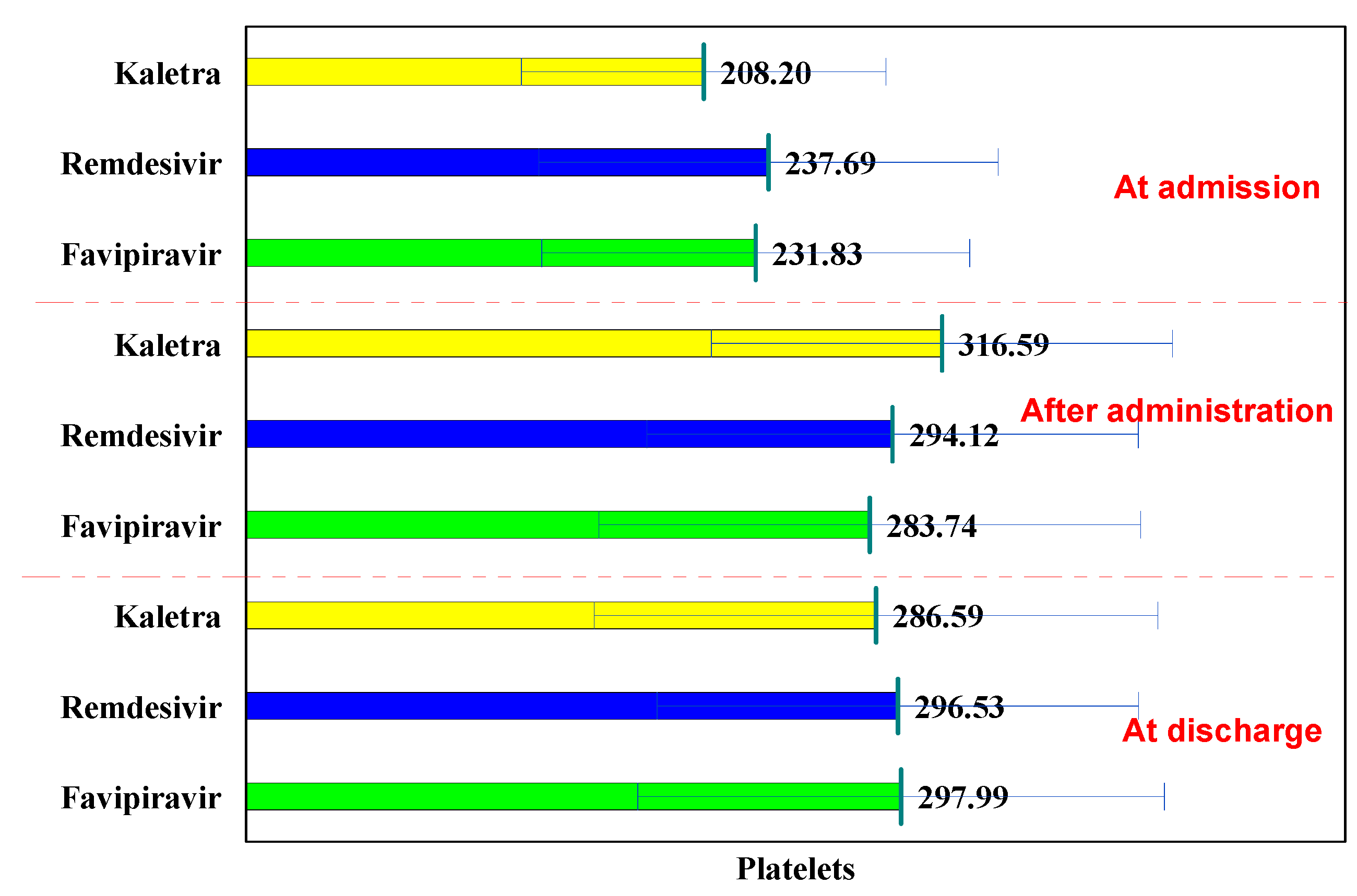
| Platelets | at Hospitalization | after Administration | P1−2 | at Discharge | P1−3 | P2−3 |
|---|---|---|---|---|---|---|
| Lopinavir/Ritonavir (Kaletra) | 208.20 ± 82.90 | 316.59 ± 104.85 | <0.001 | 286.59 ± 128.22 | 0.004 | 0.295 |
| Remdesivir | 237.69 ± 104.47 | 294.12 ± 111.79 | 0.001 | 296.53 ± 109.53 | <0.001 | 0.887 |
| Favipiravir | 231.83 ± 97.34 | 283.74 ± 123.27 | <0.001 | 297.99 ± 119.79 | <0.001 | 0.316 |
| pK-R | 0.106 | 0.304 | 0.692 | |||
| pK-F | 0.148 | 0.117 | 0.639 | |||
| pR-F | 0.673 | 0.513 | 0.925 |
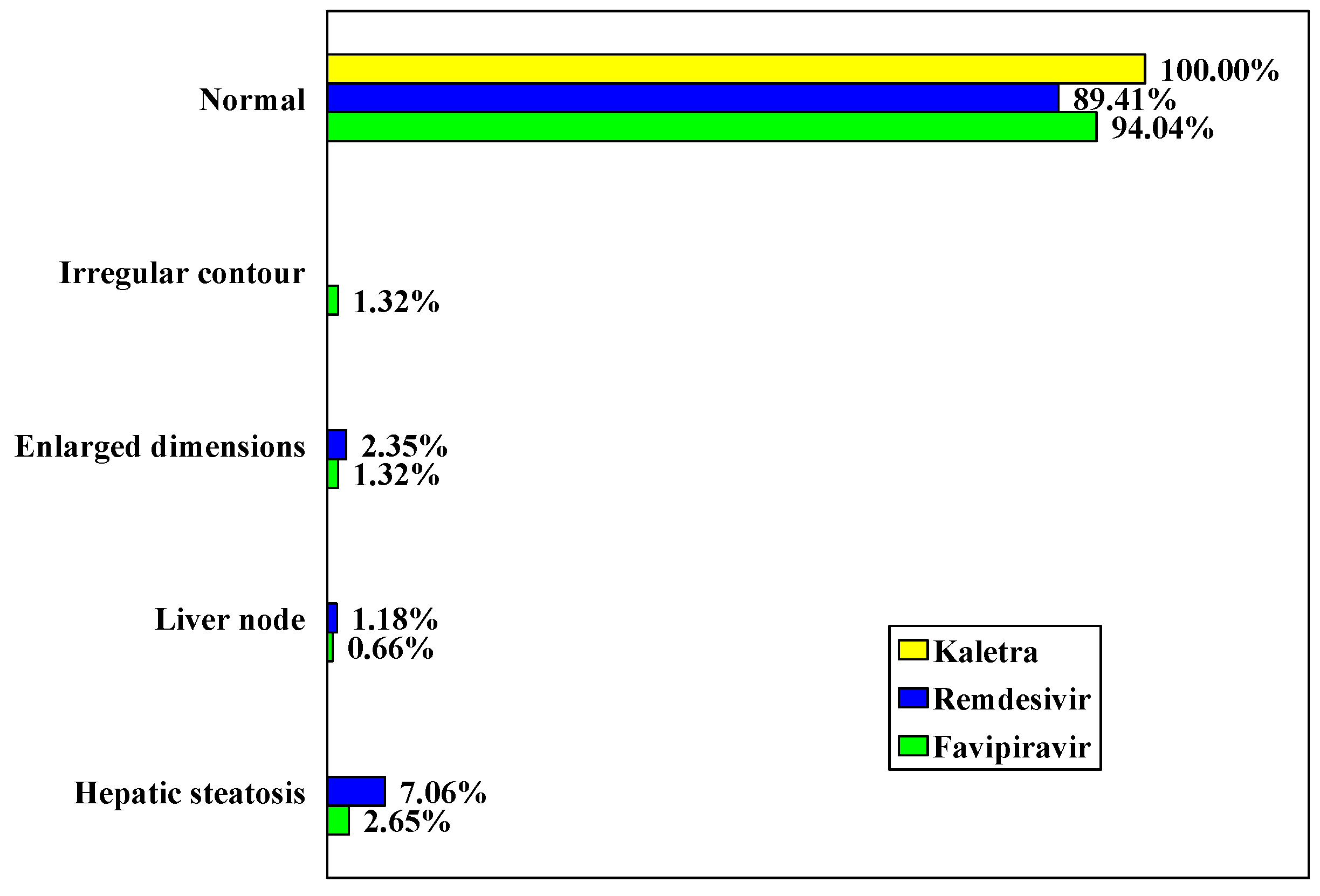
| Lopinavir/Ritonavir (Kaletra) | Remdesivir | Favipiravir | ||||
|---|---|---|---|---|---|---|
| Normal | 36 | 100.00 | 76 | 89.41 | 142 | 94.04 |
| Irregular contour | 0 | 0.00 | 0 | 0.00 | 2 | 1.32 |
| Increased dimensions | 0 | 0.00 | 2 | 2.35 | 2 | 1.32 |
| Liver nodules | 0 | 0.00 | 1 | 1.18 | 1 | 0.66 |
| Hepatic steatosis | 0 | 0.00 | 6 | 7.06 | 4 | 2.65 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marc, F.; Moldovan, C.; Hoza, A.; Restea, P.; Sachelarie, L.; Romila, L.E.; Suteu, C.; Farcas, D.M. Evaluation of Hepatic Biochemical Parameters during Antiviral Treatment in COVID-19 Patients. Biology 2022, 11, 13. https://doi.org/10.3390/biology11010013
Marc F, Moldovan C, Hoza A, Restea P, Sachelarie L, Romila LE, Suteu C, Farcas DM. Evaluation of Hepatic Biochemical Parameters during Antiviral Treatment in COVID-19 Patients. Biology. 2022; 11(1):13. https://doi.org/10.3390/biology11010013
Chicago/Turabian StyleMarc, Felicia, Corina Moldovan, Anica Hoza, Patricia Restea, Liliana Sachelarie, Laura Ecaterina Romila, Corina Suteu, and Dorina Maria Farcas. 2022. "Evaluation of Hepatic Biochemical Parameters during Antiviral Treatment in COVID-19 Patients" Biology 11, no. 1: 13. https://doi.org/10.3390/biology11010013
APA StyleMarc, F., Moldovan, C., Hoza, A., Restea, P., Sachelarie, L., Romila, L. E., Suteu, C., & Farcas, D. M. (2022). Evaluation of Hepatic Biochemical Parameters during Antiviral Treatment in COVID-19 Patients. Biology, 11(1), 13. https://doi.org/10.3390/biology11010013