
Survival Analysis after Living Donor Liver Transplantation for Hepatocellular Carcinoma: A Single Center Cohort Study


Abstract
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Study Patient Selection
2.2. Pretransplant Imaging Work-Up for Recipient
2.3. Living Donor Protocol
2.4. Recipient Liver Transplantation
2.5. Postoperative Complications, Follow-Up, and Surveillance
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Association of Milan Criteria with Explanted Liver Pathology
3.3. Postoperative Complications
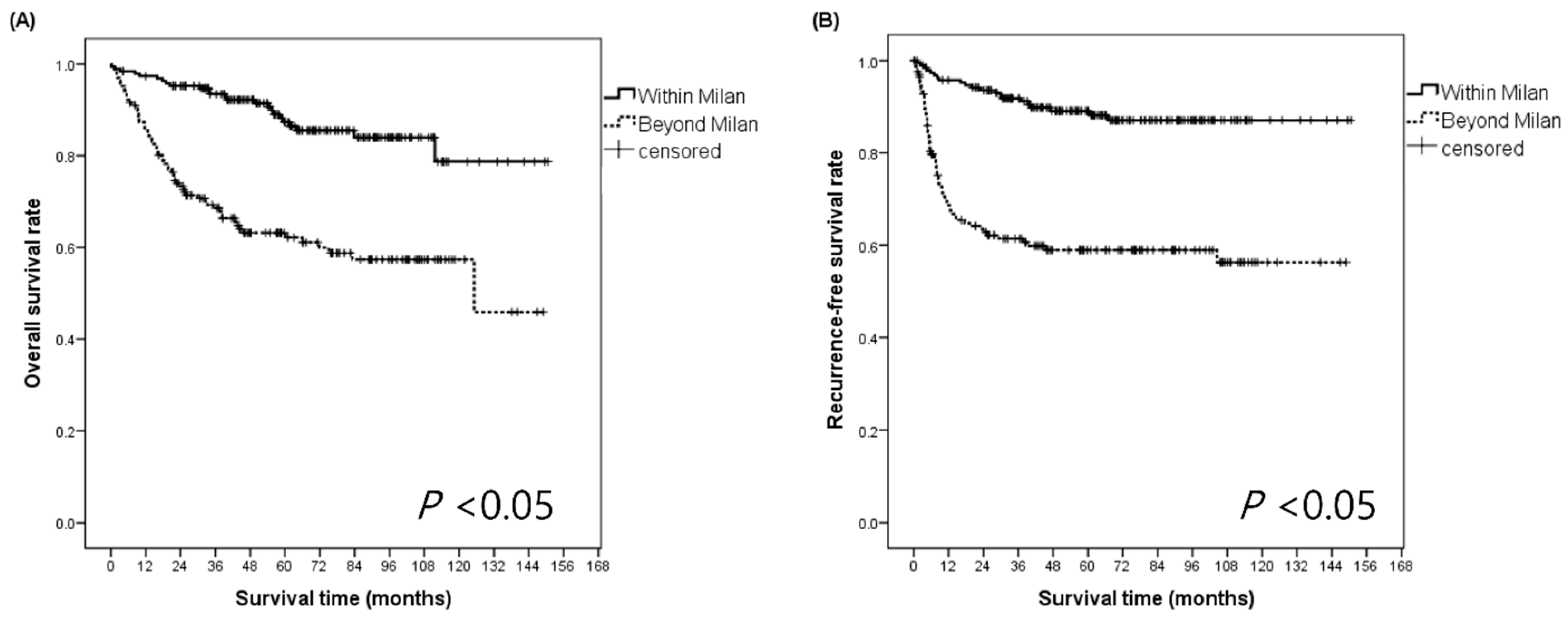
3.4. Survival Outcomes after LDLT for HCC
3.5. Prognostic Factors Related to OS and RFS
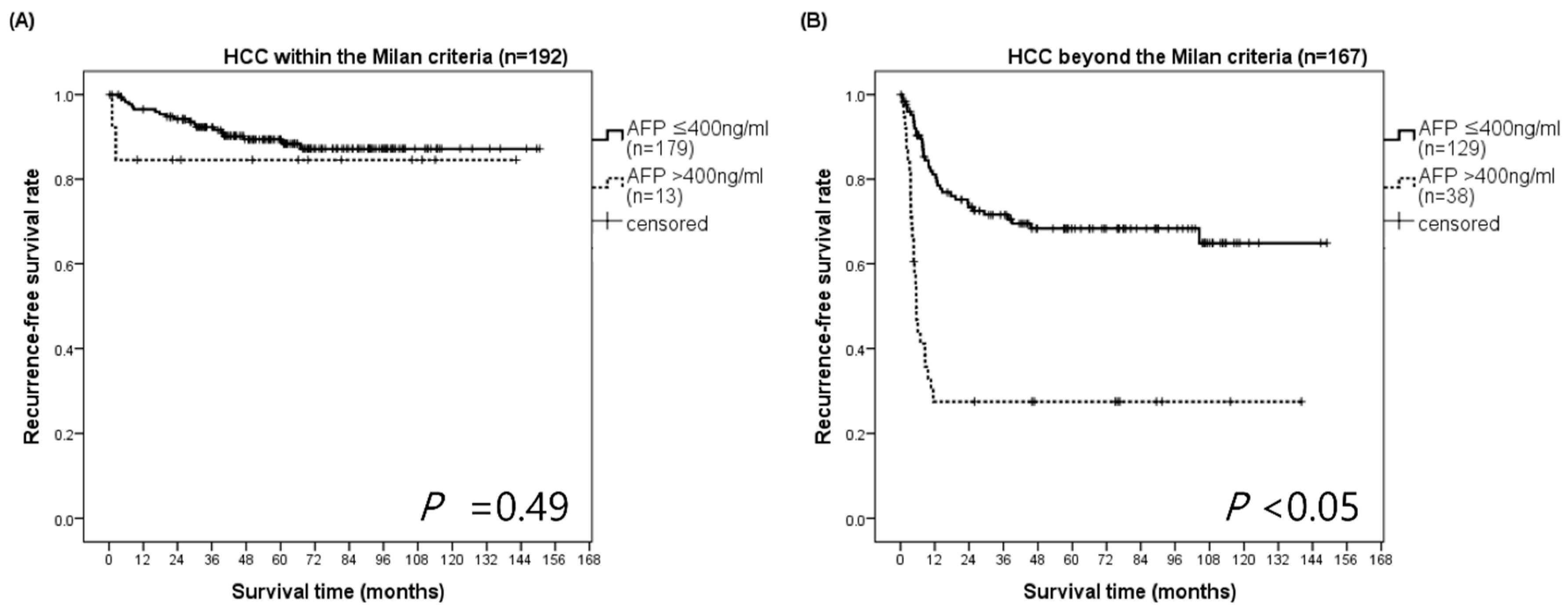
3.6. RFS Analysis According to AFP Stratified by the Milan Criteria
3.7. Preoperative Prognostic Factors Related to Recurrence within 5 Years
3.8. Preoperative Prognostic Factors for RFS in BM Patients with Very Large HCC (≥7 cm)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2014, 136, E359–E386. [Google Scholar] [CrossRef]
- Llovet, J.M.; Brú, C.; Bruix, J. Prognosis of Hepatocellular Carcinoma: The BCLC Staging Classification. Semin. Liver Dis. 1999, 19, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Mazzaferro, V.M.; Regalia, E.; Doci, R.; Andreola, S.; Pulvirenti, A.; Bozzetti, F.; Montalto, F.; Ammatuna, M.; Morabito, A.; Gennari, L. Liver Transplantation for the Treatment of Small Hepatocellular Carcinomas in Patients with Cirrhosis. N. Engl. J. Med. 1996, 334, 693–700. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Lee, E.C.; Park, S.J. Impact of preserved collateral veins on small-for-size grafts in living donor liver transplantation. Hepatol. Res. 2017, 48, 295–302. [Google Scholar] [CrossRef]
- Kim, S.H.; Kim, Y.K.; Lee, S.D.; Lee, E.C.; Park, S.J. The Impact of a Surgical Protocol for Enhanced Recovery on Living Donor Right Hepatectomy: A Single-Center Cohort Study. Medicine 2016, 95, e3227. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Kim, Y.K.; Lee, S.D.; Park, S.-J. Selection and outcomes of living donors with a remnant volume less than 30% after right hepatectomy. Liver Transpl. 2013, 19, 872–878. [Google Scholar] [CrossRef]
- Ciccarelli, O.; Lai, Q.; Goffette, P.; Finet, P.; De Reyck, C.; Roggen, F.; Sempoux, C.; Doffagne, E.; Reding, R.; Lerut, J. Liver transplantation for hepatocellular cancer: UCL ex-perience in 137 adult cirrhotic patients. Alpha-foetoprotein level and locoregional treatment as refined selection criteria. Transpl. Int. 2012, 25, 867–875. [Google Scholar] [CrossRef] [PubMed]
- Lai, Q.; Avolio, A.W.; Manzia, T.M.; Sorge, R.; Agnes, S.; Tisone, G.; Berloco, P.B.; Rossi, M. Combination of biological and morphological parameters for the selection of patients with hepatocellular carcinoma waiting for liver transplantation. Clin. Transplant. 2012, 26, E125–E131. [Google Scholar] [CrossRef]
- Clavien, P.A.; Lesurtel, M.; Bossuyt, P.M.; Gores, G.J.; Langer, B.; Perrier, A. Recommendations for liver transplantation for hepato-cellular carcinoma: An international consensus conference report. Lancet Oncol. 2012, 13, e11–e22. [Google Scholar] [CrossRef]
- Kim, S.H.; Kim, Y.-K. Improving outcomes of living-donor right hepatectomy. BJS 2013, 100, 528–534. [Google Scholar] [CrossRef]
- Ito, T.; Takada, Y.; Ueda, M.; Haga, H.; Maetani, Y.; Oike, F.; Ogawa, K.; Sakamoto, S.; Ogura, Y.; Egawa, H.; et al. Expansion of selection criteria for patients with hepatocellular carcinoma in living donor liver transplantation. Liver Transplant. 2007, 13, 1637–1644. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.G.; Hwang, S.; Moon, D.B.; Ahn, C.S.; Kim, K.H.; Sung, K.B.; Ko, G.Y.; Park, K.M.; Ha, T.Y.; Song, G.W. Expanded indication criteria of living donor liver transplan-tation for hepatocellular carcinoma at one large-volume center. Liver Transplant. 2008, 14, 935–945. [Google Scholar] [CrossRef]
- Yao, F.Y.; Ferrell, L.; Bass, N.M.; Watson, J.J.; Bacchetti, P.; Venook, A.; Ascher, N.L.; Roberts, J.P. Liver transplantation for hepatocellular carcinoma: Ex-pansion of the tumor size limits does not adversely impact survival. Hepatology 2001, 33, 1394–1403. [Google Scholar] [CrossRef] [PubMed]
- Klintmalm, G.B. Liver transplantation for hepatocellular carcinoma: A registry report of the impact of tumor characteristics on outcome. Ann. Surg. 1998, 228, 479–490. [Google Scholar] [CrossRef] [PubMed]
- Mehta, N.; Heimbach, J.; Harnois, D.M.; Sapisochin, G.; Dodge, J.L.; Lee, D.; Burns, J.M.; Sanchez, W.; Greig, P.D.; Grant, D.R.; et al. Validation of a Risk Estimation of Tumor Recurrence After Transplant (RETREAT) Score for Hepatocellular Carcinoma Recurrence After Liver Transplant. JAMA Oncol. 2017, 3, 493–500. [Google Scholar] [CrossRef]
- Todo, S.; Furukawa, H. Living donor liver transplantation for adult patients with hepatocellular carcinoma: Experience in Japan. Ann. Surg. 2004, 240, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Shetty, K.; Timmins, K.; Brensinger, C.; Furth, E.E.; Rattan, S.; Sun, W.; Rosen, M.; Soulen, M.; Shaked, A.; Reddy, K.R.; et al. Liver transplantation for hepatocellular carcinoma val-idation of present selection criteria in predicting outcome. Liver Transplant. 2004, 10, 911–918. [Google Scholar] [CrossRef]
- Merani, S.; Majno, P.; Kneteman, N.M.; Berney, T.; Morel, P.; Mentha, G.; Toso, C. The impact of waiting list alpha-fetoprotein changes on the outcome of liver transplant for hepatocellular carcinoma. J. Hepatol. 2011, 55, 814–819. [Google Scholar] [CrossRef]
- Duvoux, C.; Roudot-Thoraval, F.; Decaens, T.; Pessione, F.; Badran, H.; Piardi, T.; Francoz, C.; Compagnon, P.; Vanlemmens, C.; Dumortier, J.; et al. Liver transplantation for hepatocellular car-cinoma: A model including alpha-fetoprotein improves the performance of Milan criteria. Gastroenterology 2012, 143, 986–994.e3. [Google Scholar] [CrossRef]
- Tamura, S.; Kato, T.; Berho, M.; Misiakos, E.P.; O’Brien, C.; Reddy, K.R.; Nery, J.R.; Burke, G.W.; Schiff, E.R.; Miller, J.; et al. Impact of histological grade of hepatocellular carcinoma on the outcome of liver transplantation. Arch. Surg. 2001, 136, 25–30, discussion 1. [Google Scholar] [CrossRef]
- Mazzaferro, V.; Llovet, J.M.; Miceli, R.; Bhoori, S.; Schiavo, M.; Mariani, L.; Camerini, T.; Roayaie, S.; Schwartz, M.E.; Grazi, G.L.; et al. Predicting survival after liver transplantation in patients with hepatocellular carcinoma beyond the Milan criteria: A retrospective, exploratory analysis. Lancet Oncol. 2009, 10, 35–43. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 359) | WM Patients (n = 192) | BM Patients (n = 167) | p | |
|---|---|---|---|---|
| Recipient | ||||
| Male (%) | 297 (82.7) | 150 (78.1) | 147 (88.0) | <0.05 |
| Age (yrs) | 54.2 ± 7.6 | 53.7 ± 7.6 | 54.7 ± 7.5 | 0.19 |
| BMI (kg/m2) | 23.6 (21.6–25.7) | 23.8 (21.9–26.4) | 23.5 (21.4–25.3) | 0.07 |
| Child-Pugh class | 0.05 | |||
| A | 195 (54.3) | 108 (56.3) | 87 (52.1) | |
| B | 98 (27.3) | 43 (22.4) | 55 (32.9) | |
| C | 66 (18.4) | 41 (21.3) | 25 (15.0) | |
| MELD score | 11 (6–51) | 11 (6–51) | 11 (6–47) | 0.38 |
| Ascites | ||||
| None | 205 (57.1%) | 111 (57.8%) | 94 (56.3%) | 0.37 |
| Mild to moderate | 110 (30.6%) | 54 (28.1%) | 56 (33.5%) | |
| Severe | 44 (12.3%) | 27 (14.1%) | 17 (10.2%) | |
| GRWR | 0.99 (0.42–1.93) | 1.01 (0.42–1.87) | 0.99 (0.45–1.93) | 0.47 |
| SFSS | 84 (23.4) | 42 (21.9) | 42 (25.2) | 0.46 |
| ABO incompatible | 34 (9.5) | 20 (10.4) | 14 (8.4) | 0.51 |
| Basal disease | 0.76 | |||
| Non-viral | 23 (6.4) | 13 (6.8) | 10 (6.0) | |
| Viral | 336 (93.6) | 179 (93.2) | 157 (94.0) | |
| Viral hepatitis type | 0.11 | |||
| B | 311 (86.6) | 170 (88.5) | 141 (84.4) | |
| C | 17 (4.7) | 6 (3.1) | 11 (6.6) | |
| B, C | 6 (1.7) | 1 (0.5) | 5 (3.0) | |
| NBNC | 25 (7.0) | 15 (7.8) | 10 (6.0) | |
| EBL (mL) | 1500 (200–90,000) | 1500 (300–400,000) | 1500 (200–900,000) | 0.33 |
| CIT (min) | 83.0 (20.0–255.0) | 82.0 (20.0–255.0) | 83.0 (23.0–212.0) | 0.75 |
| WIT (min) | 25.0 (5.0–255.0) | 26.0 (5.0–115.0) | 25.0 (7.0–55.0) | 0.23 |
| Plt count (×103/μL) | 79.0 (15.0–399.0) | 73.5 (15.0–399.0) | 84.0 (20.0–286.0) | 0.37 |
| AFP (ng/mL) | <0.05 | |||
| ≤400 | 308 (85.8) | 179 (93.2) | 129 (77.3) | |
| >400 | 51 (14.2) | 13 (6.8) | 38 (22.7) | |
| Locoregional treatment | ||||
| Resection | 59 (16.4) | 29 (15.1) | 30 (18.0) | 0.46 |
| TACE | 225 (62.7) | 107 (55.7) | 118 (70.7) | <0.05 |
| RFA | 27 (7.5) | 14 (7.3) | 13 (7.8) | 0.86 |
| PEI | 7 (2.0) | 5 (2.6) | 2 (1.2) | 0.45 |
| Donor | ||||
| Male | 229 (63.8) | 125 (65.1) | 104 (62.3) | 0.57 |
| Age (yrs) | 31 (16–75) | 30 (16–75) | 31 (16–62) | 0.76 |
| Graft type | 0.48 | |||
| Right liver | 351 (97.8) | 189 (98.4) | 162 (97.0) | |
| Extended right liver | 8 (2.2) | 3 (1.6) | 5 (3.0) |
| Total (n = 359) | WM Patients (n = 192) | BM Patients (n = 167) | p | |
|---|---|---|---|---|
| Number (n) | <0.05 | |||
| Solitary tumor | 152 (42.3) | 117 (60.9) | 35 (21.0) | |
| 2–3 tumors | 97 (27.0) | 75 (39.1) | 22 (13.2) | |
| >3 tumors | 110 (30.6) | 0 (0.0) | 110 (65.8) | |
| Maximum tumor size (cm) | 3.04 ± 2.48 | 1.97 ± 0.85 | 4.26 ± 3.09 | <0.05 |
| E–S grade III–IV | 105 (29.3) | 44 (22.9) | 61 (36.5) | <0.05 |
| Microvascular invasion | 136 (37.9) | 45 (23.4) | 91 (54.5) | <0.05 |
| Bile duct invasion | 12 (3.3) | 4 (2.1) | 8 (4.8) | 0.15 |
| Serosa invasion | 77 (21.5) | 23 (12.0) | 54 (32.3) | <0.05 |
| Intrahepatic metastasis | 144 (40.1) | 38 (19.8) | 106 (63.5) | <0.05 |
| Liver cirrhosis | 334 (93.0) | 181 (94.3) | 153 (91.6) | 0.32 |
| Dysplasia | 109 (30.4) | 50 (26.0) | 59 (35.3) | 0.05 |
| Total (n = 359) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Overall Survival | Recurrence-Free Survival | |||||||
| Univariate | Multivariate | Univariate | Multivariate | |||||
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | |
| Recipient | ||||||||
| Male | 1.92 (0.96–3.83) | 0.06 | 1.85 (0.96–3.57) | 0.06 | ||||
| Age | 1.00 (0.97–1.03) | 0.86 | 0.97 (0.94–1.00) | 0.05 | ||||
| MELD | 0.99 (0.96–1.02) | 0.69 | 0.94 (0.90–0.98) | <0.05 | 0.95 (0.91–1.00) | 0.08 | ||
| ABO incompatible | 1.48 (0.74–2.98) | 0.26 | 1.73 (0.94–3.19) | 0.07 | ||||
| EBL (mL) | 1.00 (1.00–1.00) | 0.92 | 1.00 (1.00–1.00) | 0.44 | ||||
| CIT (min) | 1.00 (0.99–1.01) | 0.13 | 0.99 (0.99–1.00) | 0.85 | ||||
| WIT (min) | 1.00 (0.98–1.01) | 0.85 | 0.99 (0.98–1.01) | 0.83 | ||||
| Platelet count | 1.00 (0.99–1.01) | 0.10 | 1.00 (0.99–1.01) | 0.13 | ||||
| AFP > 400 ng/mL | 4.25 (2.73–6.62) | <0.05 | 2.07 (1.28–3.36) | <0.05 | 4.62 (2.96–7.21) | <0.05 | 2.16 (1.34–3.49) | <0.05 |
| Locoregional treatment | 1.20 (0.76–1.89) | 0.42 | 1.56 (0.95–2.57) | 0.47 | ||||
| HCC beyond the Milan | 3.73 (2.33–5.97) | <0.05 | 2.61 (1.60–4.26) | <0.05 | 4.06 (2.55–6.49) | <0.05 | 3.01 (1.81–5.01) | <0.05 |
| Pathologic findings | ||||||||
| Number (n) | ||||||||
| Solitary tumor | - | - | ||||||
| 2–3 tumors | 0.76 (0.43–1.32) | 0.33 | 0.47 (0.26–0.87) | 0.01 | ||||
| >3 tumors | 1.25 (0.78–2.02) | 0.34 | 1.20 (0.76–1.88) | 0.42 | ||||
| Greatest tumor size (cm) | 1.22 (1.16–1.28) | <0.05 | 1.15 (1.07–1.23) | <0.05 | 1.31 (1.24–1.38) | <0.05 | 1.24 (1.16–1.33) | <0.05 |
| E-S grade III–IV | 3.25 (2.14–4.95) | <0.05 | 2.06 (1.34–3.18) | <0.05 | 3.76 (2.49–5.69) | <0.05 | 2.25 (1.45–3.49) | <0.05 |
| Microvascular invasion | 4.25 (2.72–6.64) | <0.05 | 2.39 (1.32–4.35) | <0.05 | 6.65 (4.14–10.69) | <0.05 | 2.15 (1.21–3.82) | <0.05 |
| Bile duct invasion | 4.02 (1.94–8.35) | <0.05 | 1.34 (0.60–3.01) | 0.47 | 3.59 (1.65–7.78) | <0.05 | 0.98 (0.43–2.26) | 0.97 |
| Serosa invasion | 3.84 (2.51–5.88) | <0.05 | 1.17 (0.67–2.04) | 0.57 | 4.88 (3.22–7.38) | <0.05 | 1.20 (0.70–2.04) | 0.49 |
| Intrahepatic metastasis | 3.04 (1.97–4.69) | <0.05 | 0.61 (0.31–1.20) | 0.15 | 4.52 (2.88–7.11) | <0.05 | 1.41 (0.71–2.79) | 0.31 |
| Total (n = 167) | No Recurrence (n = 103) | Recurrence (n = 64) | p | |
|---|---|---|---|---|
| Recipient | ||||
| Male (%) | 146 (87.4) | 90 (87.4) | 56 (87.5) | 0.99 |
| Age (yrs) | 54.8 ± 7.5 | 55.6 ± 6.7 | 53.5 ± 8.6 | 0.11 |
| Child-Pugh class | 0.65 | |||
| A | 87 (52.1) | 51 (49.5) | 36 (56.2) | |
| B | 55 (32.9) | 35 (34.0) | 20 (31.2) | |
| C | 25 (15.0) | 17 (16.5) | 8 (12.5) | |
| MELD score | 11.0 (9.0–15.0) | 12.0 (9.0–16.0) | 10.0 (9.0–14.5) | 0.22 |
| Basal disease | 0.40 | |||
| Non-viral | 10 (6.0) | 6 (5.9) | 4 (6.2) | |
| Viral | 157 (94.0) | 97 (94.2) | 60 (93.8) | |
| Plt count (×103/μL) | 84.0 (51.5–123.5) | 79.0 (46.0–105.0) | 97.5 (68.5–134.5) | <0.05 |
| AFP (ng/mL) | <0.05 | |||
| ≤400 | 129 (77.2) | 92 (89.3) | 37 (57.8) | |
| >400 | 38 (22.8) | 11 (10.7) | 27 (42.2) | |
| Donor | ||||
| Male (%) | 104 (62.3) | 67 (65.0) | 37 (57.8) | 0.44 |
| Age (yrs) | 31 (25–39) | 31 (25–37) | 31 (23.5–42) | 0.74 |
| OR | 95% CI | p | |
|---|---|---|---|
| Plt count (×103/μL) | 1.01 | (1.00–1.02) | <0.05 |
| AFP > 400 ng/mL | 7.14 | (3.16–17.0) | <0.05 |
| Total (n = 359) | HCC < 7 cm (n = 332) | HCC ≥ 7 cm (n = 27) | p | |
|---|---|---|---|---|
| Number (n) | <0.05 | |||
| Solitary tumor | 152 (42.3) | 135 (40.7) | 17 (63.0) | |
| 2–3 tumors | 97 (27.0) | 95 (28.6) | 2 (7.4) | |
| >3 tumors | 110 (30.9) | 102 (30.7) | 8 (29.6) | |
| Maximum tumor size (cm) | 3.04 ± 2.48 | 2.49 ± 1.31 | 8.94 ± 1.99 | <0.05 |
| E–S grade III–IV | 105 (29.3) | 91 (27.4) | 14 (51.8) | <0.05 |
| Microvascular invasion | 136 (37.9) | 113 (34.0) | 23 (85.2) | <0.05 |
| Bile duct invasion | 12 (3.3) | 10 (3.0) | 2 (7.4) | 0.15 |
| Serosa invasion | 77 (21.5) | 57 (17.1) | 20 (74.1) | <0.05 |
| Intrahepatic metastasis | 144 (40.1) | 123 (37.0) | 21 (77.8) | <0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Na, B.-G.; Kim, S.-H.; Park, S.-J. Survival Analysis after Living Donor Liver Transplantation for Hepatocellular Carcinoma: A Single Center Cohort Study. Biology 2021, 10, 446. https://doi.org/10.3390/biology10050446
Na B-G, Kim S-H, Park S-J. Survival Analysis after Living Donor Liver Transplantation for Hepatocellular Carcinoma: A Single Center Cohort Study. Biology. 2021; 10(5):446. https://doi.org/10.3390/biology10050446
Chicago/Turabian StyleNa, Byung-Gon, Seong-Hoon Kim, and Sang-Jae Park. 2021. "Survival Analysis after Living Donor Liver Transplantation for Hepatocellular Carcinoma: A Single Center Cohort Study" Biology 10, no. 5: 446. https://doi.org/10.3390/biology10050446
APA StyleNa, B.-G., Kim, S.-H., & Park, S.-J. (2021). Survival Analysis after Living Donor Liver Transplantation for Hepatocellular Carcinoma: A Single Center Cohort Study. Biology, 10(5), 446. https://doi.org/10.3390/biology10050446