
Sperm Selection by Magnetic-Activated Cell Sorting before Microinjection of Autologous Oocytes Increases Cumulative Live Birth Rates with Limited Clinical Impact: A Retrospective Study in Unselected Males

 , , , ,
, , , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. IVF Procedures
2.3. Database
2.4. Outcome Measures
2.5. Statistical Analysis
2.5.1. Descriptive Analysis
2.5.2. Univariate Analysis
2.5.3. Multivariate Adjusted Analysis
3. Results
3.1. Descriptive Variables
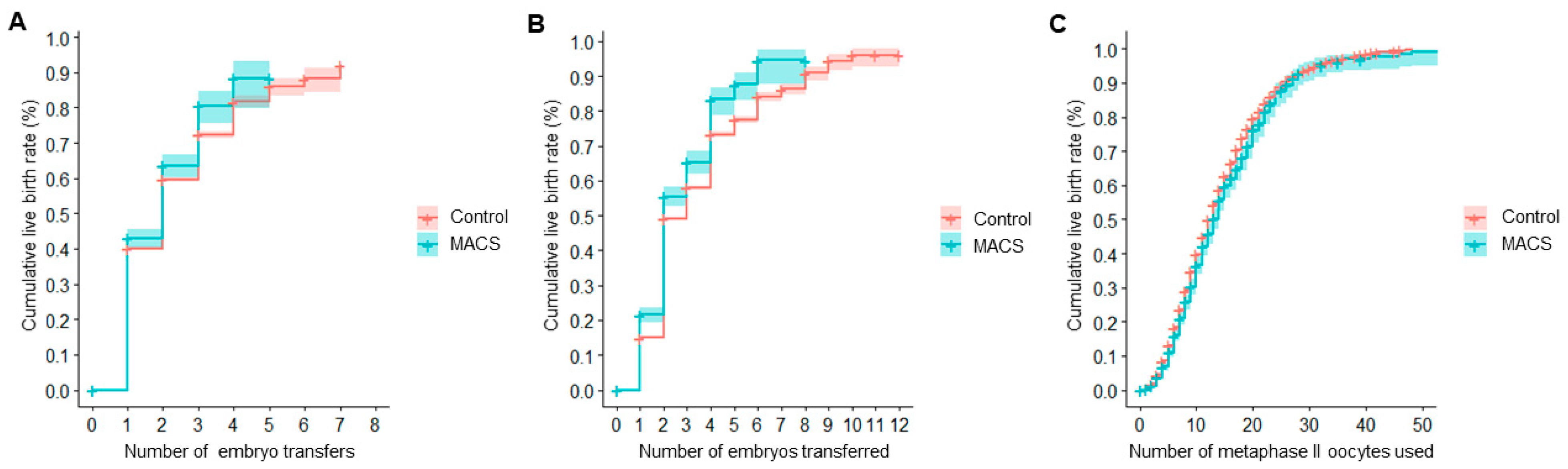
3.2. Main Outcomes: Cumulative Live Birth Rates
3.3. Secondary Outcomes: Gestational Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviation
| ART | assisted reproduction technologies |
| BMI | body-mass index |
| CLBR | cumulative live birth rate |
| DGC | density-gradient centrifugation |
| ET | embryo transfer |
| fDNA | DNA fragmentation |
| hCG | human chorionic gonadotropin |
| HR | hazard ratio |
| ICSI | intracytoplasmic sperm injection |
| LBR | live birth rate |
| MII | metaphase II |
| MACS | magnetic-activated cell sorting |
| OR | odds ratio |
| PGT-A | pre-implantation genetic testing for aneuploidies |
| RCT | randomized clinical trial |
| WHO | World Health Organization |
| 95% CI | 95% confidence interval |
References
- WHO. WHO Laboratory Manual for the Examination and Processing of Human Semen, 5th ed.; World Health Organization (WHO): Geneva, Switzerland, 2010. [Google Scholar]
- Said, T.M.; Land, J.A. Effects of advanced selection methods on sperm quality and ART outcome: A systematic review. Hum. Reprod. Update 2011, 17, 719–733. [Google Scholar] [CrossRef]
- Berteli, T.S.; Da Broi, M.G.; Martins, W.P.; Ferriani, R.A.; Navarro, P.A. Magnetic-activated cell sorting before density gradient centrifugation improves recovery of high-quality spermatozoa. Andrology 2017, 5, 776–782. [Google Scholar] [CrossRef]
- Grunewald, S.; Fitzl, G.; Springsguth, C. Induction of ultra-morphological features of apoptosis in mature and immature sperm. Asian J. Androl. 2017, 19, 533–537. [Google Scholar] [CrossRef] [PubMed]
- Said, T.M.; Gaglani, A.; Agarwal, A. Implication of apoptosis in sperm cryoinjury. Reprod. Biomed. Online 2010, 21, 456–462. [Google Scholar] [CrossRef]
- Mahfouz, R.Z.; Sharma, R.K.; Said, T.M.; Erenpreiss, J.; Agarwal, A. Association of sperm apoptosis and DNA ploidy with sperm chromatin quality in human spermatozoa. Fertil. Steril. 2009, 91, 1110–1118. [Google Scholar] [CrossRef] [PubMed]
- Weng, S.L.; Taylor, S.L.; Morshedi, M.; Schuffner, A.; Duran, E.H.; Beebe, S.; Oehninger, S. Caspase activity and apoptotic markers in ejaculated human sperm. Mol. Hum. Reprod. 2002, 8, 984–991. [Google Scholar] [CrossRef]
- Chen, Z.; Hauser, R.; Trbovich, A.M.; Shifren, J.L.; Dorer, D.J.; Godfrey-Bailey, L.; Singh, N.P. The relationship between human semen characteristics and sperm apoptosis: A pilot study. J. Androl. 2006, 27, 112–120. [Google Scholar] [CrossRef]
- Hichri, R.; Amor, H.; Khammari, M.; Harzallah, M.; El Fekih, S.; Saad, A.; Ajina, M.; Ben Ali, H. Apoptotic sperm biomarkers and the correlation between conventional sperm parameters and clinical characteristics. Andrologia 2018, 50. [Google Scholar] [CrossRef]
- Engel, K.M.; Springsguth, C.H.; Grunewald, S. What happens to the unsuccessful spermatozoa? Andrology 2018, 6, 335–344. [Google Scholar] [CrossRef] [PubMed]
- Simopoulou, M.; Gkoles, L.; Bakas, P.; Giannelou, P.; Kalampokas, T.; Pantos, K.; Koutsilieris, M. Improving ICSI: A review from the spermatozoon perspective. Syst. Biol. Reprod. Med. 2016, 62, 359–371. [Google Scholar] [CrossRef]
- Sharma, R.; Kattoor, A.J.; Ghulmiyyah, J.; Agarwal, A. Effect of sperm storage and selection techniques on sperm parameters. Syst. Biol. Reprod. Med. 2015, 61, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Dirican, E.K.; Ozgun, O.D.; Akarsu, S.; Akin, K.O.; Ercan, O.; Ugurlu, M.; Camsari, C.; Kanyilmaz, O.; Kaya, A.; Unsal, A. Clinical outcome of magnetic activated cell sorting of non-apoptotic spermatozoa before density gradient centrifugation for assisted reproduction. J. Assist. Reprod. Genet. 2008, 25, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Delbes, G.; Herrero, M.B.; Troeung, E.T.; Chan, P.T. The use of complimentary assays to evaluate the enrichment of human sperm quality in asthenoteratozoospermic and teratozoospermic samples processed with Annexin-V magnetic activated cell sorting. Andrology 2013, 1, 698–706. [Google Scholar] [CrossRef]
- Bucar, S.; Goncalves, A.; Rocha, E.; Barros, A.; Sousa, M.; Sa, R. DNA fragmentation in human sperm after magnetic-activated cell sorting. J. Assist. Reprod. Genet. 2015, 32, 147–154. [Google Scholar] [CrossRef]
- Gonzalez-Martinez, M.; Sanchez-Martin, P.; Dorado-Silva, M.; Fernandez, J.L.; Girones, E.; Johnston, S.D.; Gosalvez, J. Magnetic-activated cell sorting is not completely effective at reducing sperm DNA fragmentation. J. Assist. Reprod. Genet. 2018, 35, 2215–2221. [Google Scholar] [CrossRef] [PubMed]
- Cakar, Z.; Cetinkaya, B.; Aras, D.; Koca, B.; Ozkavukcu, S.; Kaplanoglu, I.; Can, A.; Cinar, O. Does combining magnetic-activated cell sorting with density gradient or swim-up improve sperm selection? J. Assist. Reprod. Genet. 2016, 33, 1059–1065. [Google Scholar] [CrossRef]
- Gil, M.; Sar-Shalom, V.; Melendez Sivira, Y.; Carreras, R.; Checa, M.A. Sperm selection using magnetic activated cell sorting (MACS) in assisted reproduction: A systematic review and meta-analysis. J. Assist. Reprod. Genet. 2013, 30, 479–485. [Google Scholar] [CrossRef]
- Lepine, S.; McDowell, S.; Searle, L.M.; Kroon, B.; Glujovsky, D.; Yazdani, A. Advanced sperm selection techniques for assisted reproduction. Cochrane Database Syst. Rev. 2019, 7, CD010461. [Google Scholar] [CrossRef] [PubMed]
- Garrido, N.; Bellver, J.; Remohi, J.; Simon, C.; Pellicer, A. Cumulative live-birth rates per total number of embryos needed to reach newborn in consecutive in vitro fertilization (IVF) cycles: A new approach to measuring the likelihood of IVF success. Fertil. Steril. 2011, 96, 40–46. [Google Scholar] [CrossRef]
- Garrido, N.; Bellver, J.; Remohi, J.; Alama, P.; Pellicer, A. Cumulative newborn rates increase with the total number of transferred embryos according to an analysis of 15,792 ovum donation cycles. Fertil. Steril. 2012, 98, 341–346.e2. [Google Scholar] [CrossRef] [PubMed]
- Cobo, A.; Garrido, N.; Pellicer, A.; Remohi, J. Six years’ experience in ovum donation using vitrified oocytes: Report of cumulative outcomes, impact of storage time, and development of a predictive model for oocyte survival rate. Fertil. Steril. 2015, 104, 1426–1434.e8. [Google Scholar] [CrossRef]
- Rivera-Egea, R.; Garrido, N.; Sota, N.; Meseguer, M.; Remohi, J.; Dominguez, F. Sperm lipidic profiles differ significantly between ejaculates resulting in pregnancy or not following intracytoplasmic sperm injection. J. Assist. Reprod. Genet. 2018, 35, 1973–1985. [Google Scholar] [CrossRef] [PubMed]
- Esbert, M.; Pacheco, A.; Soares, S.R.; Amoros, D.; Florensa, M.; Ballesteros, A.; Meseguer, M. High sperm DNA fragmentation delays human embryo kinetics when oocytes from young and healthy donors are microinjected. Andrology 2018, 6, 697–706. [Google Scholar] [CrossRef]
- Romany, L.; Garrido, N.; Motato, Y.; Aparicio, B.; Remohi, J.; Meseguer, M. Removal of annexin V-positive sperm cells for intracytoplasmic sperm injection in ovum donation cycles does not improve reproductive outcome: A controlled and randomized trial in unselected males. Fertil. Steril. 2014, 102, 1567–1575.e1. [Google Scholar] [CrossRef]
- Esbert, M.; Godo, A.; Soares, S.R.; Florensa, M.; Amoros, D.; Ballesteros, A.; Vidal, F. Spermatozoa with numerical chromosomal abnormalities are more prone to be retained by Annexin V-MACS columns. Andrology 2017, 5, 807–813. [Google Scholar] [CrossRef]
- Cobo, A.; Garcia-Velasco, J.; Domingo, J.; Pellicer, A.; Remohi, J. Elective and Onco-fertility preservation: Factors related to IVF outcomes. Hum. Reprod. 2018, 33, 2222–2231. [Google Scholar] [CrossRef] [PubMed]
- Cobo, A.; Garcia-Velasco, J.A.; Coello, A.; Domingo, J.; Pellicer, A.; Remohi, J. Oocyte vitrification as an efficient option for elective fertility preservation. Fertil. Steril. 2016, 105, 755–764. [Google Scholar] [CrossRef] [PubMed]
- ASEBIR. Criterios ASEBIR de Valoración Morfológica de Oocitos, Embriones Tempranos y Blastocistos Humanos, 3rd ed.; Asociación para el Estudio de la Biología de la Reproducción (ASEBIR): Madrid, Spain, 2015. [Google Scholar]
- de Los Santos, M.J.; Diez Juan, A.; Mifsud, A.; Mercader, A.; Meseguer, M.; Rubio, C.; Pellicer, A. Variables associated with mitochondrial copy number in human blastocysts: What can we learn from trophectoderm biopsies? Fertil. Steril. 2018, 109, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Datta, A.K.; Campbell, S.; Deval, B.; Nargund, G. Add-ons in IVF programme—Hype or Hope? Facts Views Vis. Obgyn. 2015, 7, 241–250. [Google Scholar] [PubMed]
- van de Wiel, L.; Wilkinson, J.; Athanasiou, P.; Harper, J. The prevalence, promotion and pricing of three IVF add-ons on fertility clinic websites. Reprod. Biomed. Online 2020, 41, 801–806. [Google Scholar] [CrossRef]
- Rutherford, A.J. Should the HFEA be regulating the add-on treatments for IVF/ICSI in the UK?: FOR: Regulation of the fertility add-on treatments for IVF. BJOG 2017, 124, 1848. [Google Scholar] [CrossRef]
- Hendricks, S.; Pearson, S.D. A Proposed Framework for Strengthening Regulatory Review of Innovative Reproductive Techniques in the United States. Available online: https://www.fertstertdialog.com/posts/38973-hendriks-consider-this (accessed on 31 April 2021).
- Macklon, N.S.; Ahuja, K.K.; Fauser, B. Building an evidence base for IVF ‘add-ons’. Reprod. Biomed. Online 2019, 38, 853–856. [Google Scholar] [CrossRef] [PubMed]
- Pacheco, A.; Blanco, A.; Bronet, F.; Cruz, M.; García-Fernández, J.; García-Velasco, J.A. Magnetic-Activated Cell Sorting (MACS): A Useful Sperm-Selection Technique in Cases of High Levels of Sperm DNA Fragmentation. J. Clin. Med. 2020, 9, 3976. [Google Scholar] [CrossRef]
- Ziarati, N.; Tavalaee, M.; Bahadorani, M.; Nasr Esfahani, M.H. Clinical outcomes of magnetic activated sperm sorting in infertile men candidate for ICSI. Hum. Fertil. (Camb.) 2019, 22, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Troya, J.; Zorrilla, I. Annexin V-MACS in infertile couples as method for separation of sperm without DNA fragmentation. JBRA Assist. Reprod. 2015, 19, 66–69. [Google Scholar] [CrossRef] [PubMed]
- Stimpfel, M.; Verdenik, I.; Zorn, B.; Virant-Klun, I. Magnetic-activated cell sorting of non-apoptotic spermatozoa improves the quality of embryos according to female age: A prospective sibling oocyte study. J. Assist. Reprod. Genet. 2018, 35, 1665–1674. [Google Scholar] [CrossRef] [PubMed]
- Sheikhi, A.; Jalali, M.; Gholamian, M.; Jafarzadeh, A.; Jannati, S.; Mousavifar, N. Elimination of apoptotic spermatozoa by magnetic-activated cell sorting improves the fertilization rate of couples treated with ICSI procedure. Andrology 2013, 1, 845–849. [Google Scholar] [CrossRef]
- Sanchez-Martin, P.; Dorado-Silva, M.; Sanchez-Martin, F.; Gonzalez Martinez, M.; Johnston, S.D.; Gosalvez, J. Magnetic cell sorting of semen containing spermatozoa with high DNA fragmentation in ICSI cycles decreases miscarriage rate. Reprod. Biomed. Online 2017, 34, 506–512. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Reference | MACS |
|---|---|---|
| Patient’s age (years) | 37.03 (37.00, 37.06) | 36.76 (36.62, 36.91) |
| Patient’s BMI (kg/m2) | 23.22 (23.18, 23.25) | 23.05 (22.88, 23.21) |
| Semen age (years) | 38.88 (38.83, 38.92) | 38.77 (38.56, 38.97) |
| Duration of sterility (years) | 2.38 (2.36, 2.40) | 2.53 (2.46, 2.60) |
| Number of oocytes retrieved | 10.03 (9.97, 10.08) | 11.43 (11.16, 11.69) |
| Number of MII oocytes | 8.05 (8.01, 8.10) | 9.03 (8.81, 9.26) |
| Number of available embryos per cycle | 5.88 (5.85, 5.92) | 6.50 (6.33, 6.68) |
| Number of viable embryos per cycle | 2.37 (2.35, 2.39) | 2.35 (2.25, 2.45) |
| Number of non-viable embryos per cycle | 3.52 (3.49, 3.54) | 4.16 (4.01, 4.30) |
| Days of ovarian stimulation (days) | 10.66 (10.65, 10.68) | 10.77 (10.70, 10.84) |
| Dose of gonadotropins (IU) | 2247.82 (2240, 2256) | 2159.57 (2124, 2195) |
| Estrogen level at day of ovulation induction (pg/mL) | 1757.53 (1747, 1768) | 1327.38 (1990, 2093) |
| Progesterone level at day of ovulation induction (ng/mL) | 0.56 (0.44, 0.68) | 0.76 (0.21, 1.31) |
| Days of endometrial preparation (days) | 16.14 (16.11, 16.16) | 16.83 (16.74, 16.93) |
| Last recorded endometrial lining (mm) | 9.55 (9.54, 9.57) | 9.53 (9.47, 9.6) |
| Last recorded estrogen level (pg/mL) | 1438.09 (1428, 1448) | 1526.18 (1479, 1573) |
| Last recorded progesterone level (ng/mL) | 2.52 (2.09, 2.95) | 1.54 (1.01, 2.07) |
| Male factor (%) * | 15.03 (14.75, 15.32) | 18.65 (17.16, 20.14) |
| Transfer over day 5 (%) * | 36.74 (36.41, 37.07) | 48.62 (47.05, 50.19) |
| Per Transfer | Reference | MACS | OR | p-Value |
| Biochemical pregnancy rate (%) | 45.42 (45.04, 45.81) | 46.94 (45.15, 48.74) | 1.06 (0.99, 1.15) | 0.1085 |
| n = 63,128 | n = 2961 | |||
| Clinical pregnancy rate (%) | 38.48 (38.10, 38.86) | 39.68 (37.92, 41.44) | 1.05 (0.97, 1.13) | 0.1956 |
| n = 63,128 | n = 2961 | |||
| Ongoing pregnancy rate (%) | 31.80 (31.43, 32.16) | 32.41 (30.72, 34.11) | 1.03 (0.95, 1.11) | 0.4904 |
| n = 62,807 | n = 2931 | |||
| Live birth rate (%) | 29.20 (28.84, 29.56) | 29.30 (27.62, 30.99) | 1.01 (0.92, 1.09) | 0.9154 |
| n = 60,503 | n = 2802 | |||
| Clinical miscarriage rate (%) | 7.45 (7.22, 7.67) | 8.22 (7.11, 9.33) | 1.11 (0.95, 1.30) | 0.1715 |
| n = 52,218 | n = 2336 | |||
| Per Cycle | Reference | MACS | OR | p-Value |
| Live birth rate 1 (%) | 37.40 (36.96, 37.84) | 38.82 (36.74, 40.89) | 1.06 (0.97, 1.16) | 0.1907 |
| n = 47,235 | n = 2115 |
| Population | n | Adjusted OR | Standard Error | p-Value |
|---|---|---|---|---|
| All | 59,443 reference cycles | 1.018 (0.91, 1.14) | 0.059 | 0.767 |
| 2627 MACS cycles | ||||
| PGT-A | 18,710 reference cycles | 1.020 (084, 1.24) | 0.102 | 0.846 |
| 974 MACS cycles | ||||
| No PGT-A | 40,733 reference cycles | 1.017 (0.89, 1.17) | 0.070 | 0.810 |
| 1653 MACS cycles |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gil Juliá, M.; Hervás, I.; Navarro-Gómez Lechón, A.; Quintana, F.; Amorós, D.; Pacheco, A.; González-Ravina, C.; Rivera-Egea, R.; Garrido, N. Sperm Selection by Magnetic-Activated Cell Sorting before Microinjection of Autologous Oocytes Increases Cumulative Live Birth Rates with Limited Clinical Impact: A Retrospective Study in Unselected Males. Biology 2021, 10, 430. https://doi.org/10.3390/biology10050430
Gil Juliá M, Hervás I, Navarro-Gómez Lechón A, Quintana F, Amorós D, Pacheco A, González-Ravina C, Rivera-Egea R, Garrido N. Sperm Selection by Magnetic-Activated Cell Sorting before Microinjection of Autologous Oocytes Increases Cumulative Live Birth Rates with Limited Clinical Impact: A Retrospective Study in Unselected Males. Biology. 2021; 10(5):430. https://doi.org/10.3390/biology10050430
Chicago/Turabian StyleGil Juliá, María, Irene Hervás, Ana Navarro-Gómez Lechón, Fernando Quintana, David Amorós, Alberto Pacheco, Cristina González-Ravina, Rocío Rivera-Egea, and Nicolás Garrido. 2021. "Sperm Selection by Magnetic-Activated Cell Sorting before Microinjection of Autologous Oocytes Increases Cumulative Live Birth Rates with Limited Clinical Impact: A Retrospective Study in Unselected Males" Biology 10, no. 5: 430. https://doi.org/10.3390/biology10050430
APA StyleGil Juliá, M., Hervás, I., Navarro-Gómez Lechón, A., Quintana, F., Amorós, D., Pacheco, A., González-Ravina, C., Rivera-Egea, R., & Garrido, N. (2021). Sperm Selection by Magnetic-Activated Cell Sorting before Microinjection of Autologous Oocytes Increases Cumulative Live Birth Rates with Limited Clinical Impact: A Retrospective Study in Unselected Males. Biology, 10(5), 430. https://doi.org/10.3390/biology10050430