
Intraperitoneal Chemotherapy for Peritoneal Metastases: Technical Innovations, Preclinical and Clinical Advances and Future Perspectives

 , , ,
, , ,  , and
, and
Abstract
Simple Summary
Abstract

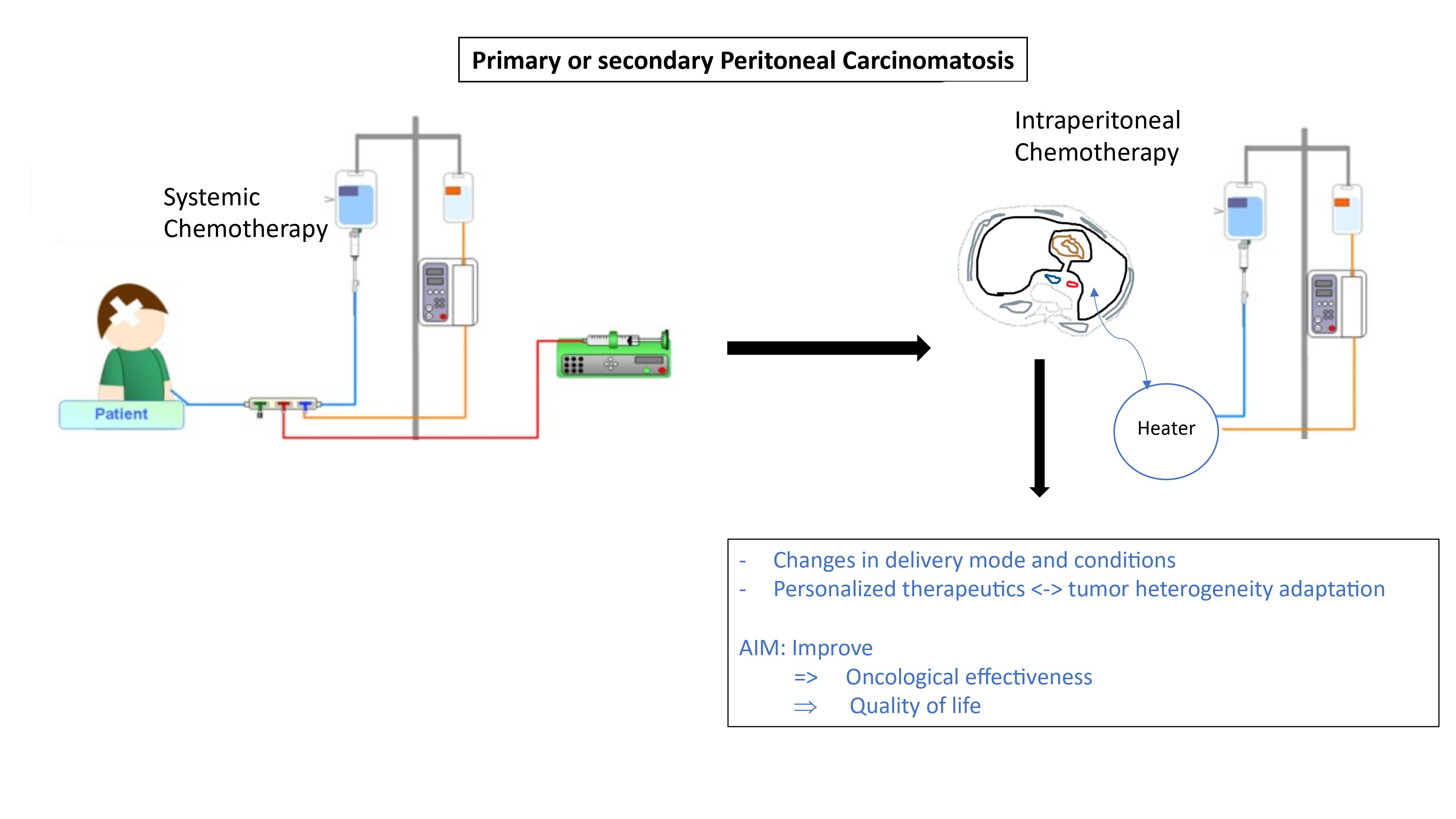
1. Introduction
2. Methods of Delivery
2.1. Delivery Conditions
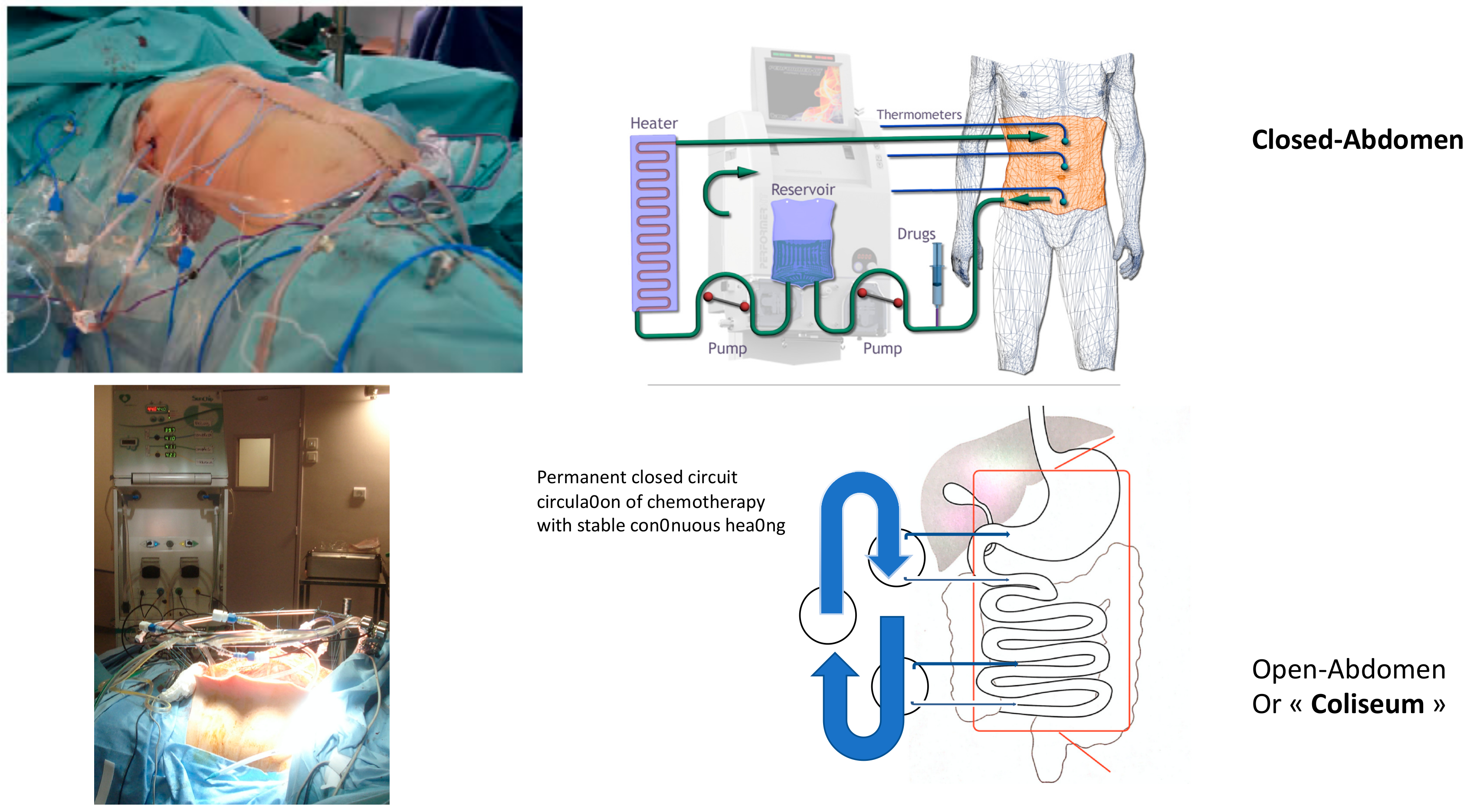
2.1.1. Hyperthermia = Intraoperative Chemoperfusion under Hyperthermic Conditions (HIPEC)
2.1.2. Pressurized Intraperitoneal Aerosol Chemotherapy (PIPAC)
2.1.3. Specific Delivery Conditions
Normothermia
Laparoscopic HIPEC
2.2. Delivery Modes
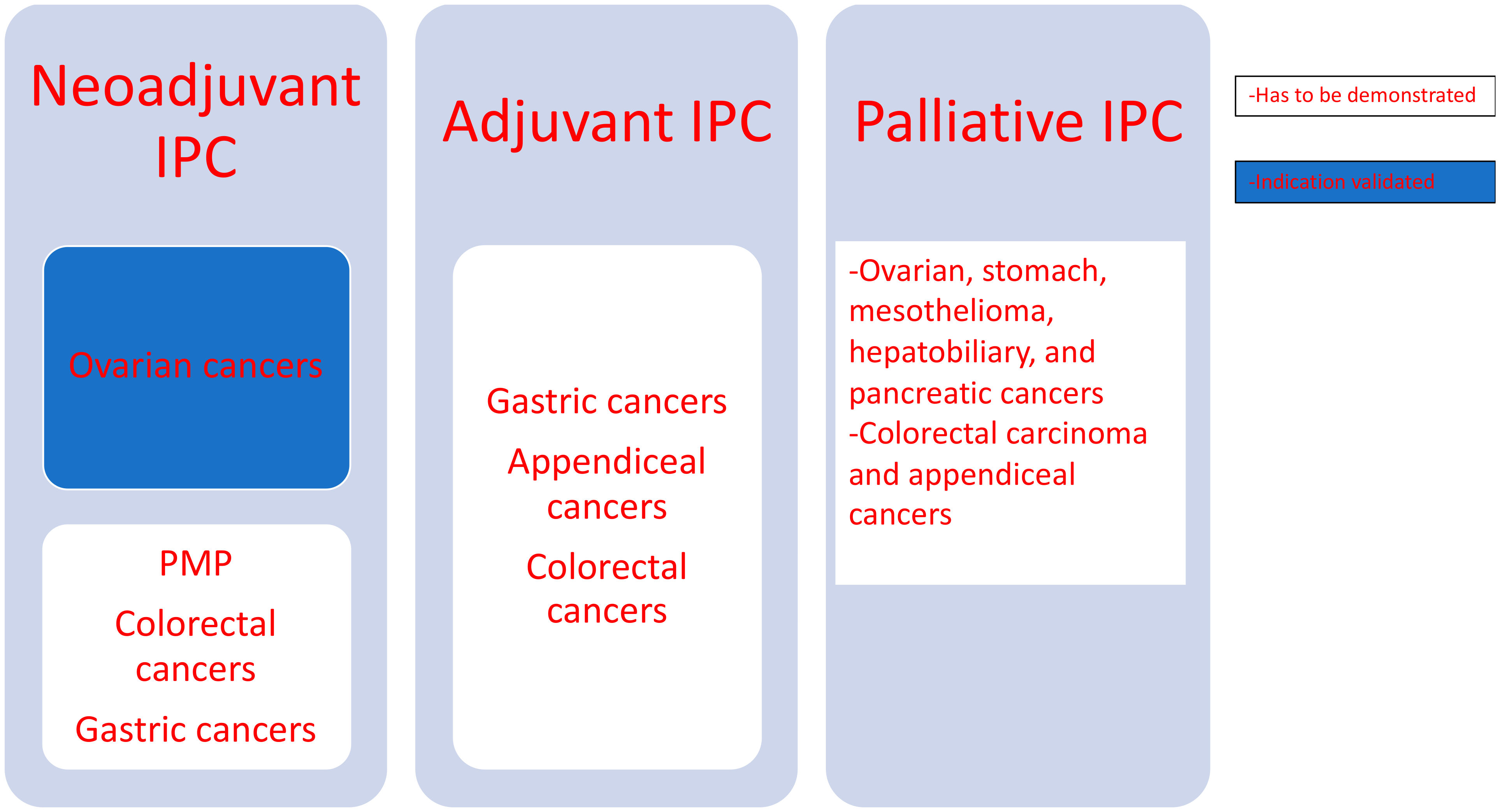
2.2.1. Delivery Mode of IPC: Time Factor
- a.
- Neoadjuvant IPC
- b.
- IPC, Extensive Intraoperative Peritoneal Lavage (EIPL), and HIPEC
- c.
- Early Postoperative Intraperitoneal Chemotherapy (EPIC)
2.2.2. Delivery Mode of IPC: Carrier Drug Factor
3. Evolution of the Drugs Used: From Unsophisticated Intra-Abdominal Chemotherapy to Complex Systems
3.1. A General Overview
3.2. Contribution of Current Basic Research—Perspectives
4. Evolution of the Clinical Indications of HIPEC
4.1. Recognized Indications
- Low-grade appendiceal mucinous neoplasm (LAMN).
- High-grade appendiceal mucinous neoplasm (HAMN).
- Mucinous adenocarcinoma.
- Poorly differentiated mucinous adenocarcinoma with signet ring cells.
- Signet ring carcinoma.
- Acellular mucin.
- Low-grade mucinous carcinoma peritonei or disseminated peritoneal adenomucinosis (DPAM).
- High-grade mucinous carcinoma peritonei or peritoneal mucinous carcinomatosis (PMCA).
- High-grade mucinous carcinoma peritonei with signet ring cells or peritoneal mucinous carcinomatosis with signet ring cells (PMCA-S).
4.2. Indications in Evaluation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goodman, M.T.; Shvetsov, Y.B. Incidence of Ovarian, Peritoneal, and Fallopian Tube Carcinomas in the United States, 1995–2004. Cancer Epidemiol. Prev. Biomark. 2009, 18, 132–139. [Google Scholar] [CrossRef]
- Rodríguez, D.; Cheung, M.C.; Housri, N.; Koniaris, L.G. Malignant abdominal mesothelioma: Defining the role of surgery. J. Surg. Oncol. 2009, 99, 51–57. [Google Scholar] [CrossRef]
- Babaier, A.; Ghatage, P. Mucinous Cancer of the Ovary: Overview and Current Status. Diagnostics 2020, 10, 52. [Google Scholar] [CrossRef] [PubMed]
- Segelman, J.; Granath, F.; Holm, T.; Machado, M.; Mahteme, H.; Martling, A. Incidence, prevalence and risk factors for peritoneal carcinomatosis from colorectal cancer. Br. J. Surg. 2012, 99, 699–705. [Google Scholar] [CrossRef] [PubMed]
- Ikeguchi, M.; Oka, A.; Tsujitani, S.; Maeta, M.; Kaibara, N. Relationship between area of serosal invasion and intraperitoneal free cancer cells in patients with gastric cancer. Anticancer Res. 1994, 14, 2131–2134. [Google Scholar] [PubMed]
- Sadeghi, B.; Arvieux, C.; Glehen, O.; Beaujard, A.C.; Rivoire, M.; Baulieux, J.; Fontaumard, E.; Brachet, A.; Caillot, J.L.; Faure, J.L.; et al. Peritoneal carcinomatosis from non-gynecologic malignancies: Results of the EVOCAPE 1 multicentric prospective study. Cancer 2000, 88, 358–363. [Google Scholar] [CrossRef]
- van Baal, J.O.A.M.; van Noorden, C.J.F.; Nieuwland, R.; Van de Vijver, K.K.; Sturk, A.; van Driel, W.J.; Kenter, G.G.; Lok, C.A.R. Development of Peritoneal Carcinomatosis in Epithelial Ovarian Cancer: A Review. J. Histochem. Cytochem. 2018, 66, 67–83. [Google Scholar] [CrossRef]
- Kelly, K.J. Management of Appendix Cancer. Clin. Colon Rectal Surg. 2015, 28, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Kusamura, S. Pathophysiology and biology of peritoneal carcinomatosis. World J. Gastrointest. Oncol. 2010, 2, 12. [Google Scholar] [CrossRef]
- van Baal, J.O.A.M.; Van de Vijver, K.K.; Nieuwland, R.; van Noorden, C.J.F.; van Driel, W.J.; Sturk, A.; Kenter, G.G.; Rikkert, L.G.; Lok, C.A.R. The histophysiology and pathophysiology of the peritoneum. Tissue Cell 2017, 49, 95–105. [Google Scholar] [CrossRef]
- Shahid, S.; Iman, A.; Matti, U.; Rachid, K.; Assaf, A.; Eveno, C.; Marc, P.; Massoud, M. Fibrin Deposit on the Peritoneal Surface Serves as a Niche for Cancer Expansion in Carcinomatosis Patients. Neoplasia 2019, 21, 1091–1101. [Google Scholar] [CrossRef] [PubMed]
- Mikuła-Pietrasik, J.; Uruski, P.; Tykarski, A.; Książek, K. The peritoneal “soil” for a cancerous “seed”: A comprehensive review of the pathogenesis of intraperitoneal cancer metastases. Cell. Mol. Life Sci. 2018, 75, 509–525. [Google Scholar] [CrossRef] [PubMed]
- Falk, P.; Jonsson, A.; Swartling, T.; Asplund, D.; Ivarsson, M.-L. Role of matrix metalloproteinases in tumour invasion: Immunohistochemistry of peritoneum from peritoneal carcinomatosis. Med. Oncol. 2018, 35, 64. [Google Scholar] [CrossRef] [PubMed]
- Tang, M.K.S.; Yue, P.Y.K.; Ip, P.P.; Huang, R.-L.; Lai, H.-C.; Cheung, A.N.Y.; Tse, K.Y.; Ngan, H.Y.S.; Wong, A.S.T. Soluble E-cadherin promotes tumor angiogenesis and localizes to exosome surface. Nat. Commun. 2018, 9, 2270. [Google Scholar] [CrossRef] [PubMed]
- Sugarbaker, P.H. Intraperitoneal chemotherapy and cytoreductive surgery for the prevention and treatment of peritoneal carcinomatosis and sarcomatosis. Semin. Surg. Oncol. 1998, 14, 254–261. [Google Scholar] [CrossRef]
- Fagotti, A.; Ferrandina, G.; Fanfani, F.; Garganese, G.; Vizzielli, G.; Carone, V.; Salerno, M.G.; Scambia, G. Prospective validation of a laparoscopic predictive model for optimal cytoreduction in advanced ovarian carcinoma. Am. J. Obstet. Gynecol. 2008, 199, 642. [Google Scholar] [CrossRef] [PubMed]
- Alter, R.; Turaga, K.; Lengyel, E. Are We Ready for Hyperthermic Intraperitoneal Chemotherapy in the Upfront Treatment of Ovarian Cancer? JAMA Netw. Open 2020, 3, e2014184. [Google Scholar] [CrossRef]
- Lemoine, L.; Sugarbaker, P.; Van der Speeten, K. Drugs, doses, and durations of intraperitoneal chemotherapy: Standardising HIPEC and EPIC for colorectal, appendiceal, gastric, ovarian peritoneal surface malignancies and peritoneal mesothelioma. Int. J. Hyperth. 2017, 33, 582–592. [Google Scholar] [CrossRef] [PubMed]
- Jacquet, P.; Averbach, A.; Stuart, O.A.; Chang, D.; Sugarbaker, P.H. Hyperthermic intraperitoneal doxorubicin: Pharmacokinetics, metabolism, and tissue distribution in a rat model. Cancer Chemother. Pharmacol. 1998, 41, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Bree, E.D.; Katsougkri, D.; Polioudaki, H.; Tsangaridou, E.; Michelakis, D.; Zoras, O.; Theodoropoulos, P. Hyperthermia During Intraperitoneal Chemotherapy with Paclitaxel or Docetaxel for Ovarian Cancer: Is There Any Benefit? Anticancer Res. 2020, 40, 6769–6780. [Google Scholar] [CrossRef]
- de Lima Vazquez, V.; Stuart, O.A.; Mohamed, F.; Sugarbaker, P.H. Extent of parietal peritonectomy does not change intraperitoneal chemotherapy pharmacokinetics. Cancer Chemother. Pharmacol. 2003, 52, 108–112. [Google Scholar] [CrossRef] [PubMed]
- Rubin, J.; Jones, Q.; Planch, A.; Rushton, F.; Bower, J. The Importance of the Abdominal Viscera to Peritoneal Transport During Peritoneal Dialysis in the Dog. Am. J. Med. Sci. 1986, 292, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Flessner, M.; Henegar, J.; Bigler, S.; Genous, L. Is the peritoneum a significant transport barrier in peritoneal dialysis? Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2003, 23, 542–549. [Google Scholar] [CrossRef]
- Dedrick, R.L.; Myers, C.E.; Bungay, P.M.; DeVita, V.T. Pharmacokinetic rationale for peritoneal drug administration in the treatment of ovarian cancer. Cancer Treat. Rep. 1978, 62, 1–11. [Google Scholar]
- Speyer, J.L.; Myers, C.E. The use of peritoneal dialysis for delivery of chemotherapy to intraperitoneal malignancies. In Cancer Chemo-and Immunopharmacology; Springer: Berlin/Heidelberg, Germany, 1980; pp. 264–269. [Google Scholar] [CrossRef]
- Tenckhoff, H.; Schechter, H. A bacteriologically safe peritoneal access device. Trans. Am. Soc. Artif. Int. Org. 1968, 14, 181–187. [Google Scholar]
- Sugarbaker, P.H. Technical Handbook for the Integration of Cytoreductive Surgery and Perioperative Intraperitoneal Chemotherapy into the Surgical Management of Gastrointestinal and Gynecologic Malignancy, 4th ed.; Laudann Company: Grand Rapids, MI, USA, 2005. [Google Scholar]
- Leiting, J.L.; Cloyd, J.M.; Ahmed, A.; Fournier, K.; Lee, A.J.; Dessureault, S.; Felder, S.; Veerapong, J.; Baumgartner, J.M.; Clarke, C.; et al. Comparison of open and closed hyperthermic intraperitoneal chemotherapy: Results from the United States hyperthermic intraperitoneal chemotherapy collaborative. World J. Gastrointest. Oncol. 2020, 12, 756–767. [Google Scholar] [CrossRef] [PubMed]
- Ceelen, W.P.; Flessner, M.F. Intraperitoneal therapy for peritoneal tumors: Biophysics and clinical evidence. Nat. Rev. Clin. Oncol. 2010, 7, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Overgaard, J. Effect of hyperthermia on malignant cells in vivo: A review and a hypothesis. Cancer 1977, 39, 2637–2646. [Google Scholar] [CrossRef]
- Sticca, R.P.; Dach, B.W. Rationale for hyperthermia with intraoperative intraperitoneal chemotherapy agents. Surg. Oncol. Clin. N. Am. 2003, 12, 689–701. [Google Scholar] [CrossRef]
- Shimizu, T.; Maeta, M.; Koga, S. Influence of local hyperthermia on the healing of small intestinal anastomoses in the rat. BJS Br. J. Surg. 1991, 78, 57–59. [Google Scholar] [CrossRef] [PubMed]
- Alyami, M.; Hübner, M.; Grass, F.; Bakrin, N.; Villeneuve, L.; Laplace, N.; Passot, G.; Glehen, O.; Kepenekian, V. Pressurised intraperitoneal aerosol chemotherapy: Rationale, evidence, and potential indications. Lancet Oncol. 2019, 20, e368–e377. [Google Scholar] [CrossRef]
- Jacquet, P.; Stuart, O.A.; Chang, D.; Sugarbaker, P.H. Effects of intra-abdominal pressure on pharmacokinetics and tissue distribution of doxorubicin after intraperitoneal administration. Anticancer. Drugs 1996, 7, 596–603. [Google Scholar] [CrossRef] [PubMed]
- Eveno, C.; Haidara, A.; Ali, I.; Pimpie, C.; Mirshahi, M.; Pocard, M. Experimental pharmacokinetics evaluation of chemotherapy delivery by PIPAC for colon cancer: First evidence for efficacy. Pleura Peritoneum 2017, 2, 103–109. [Google Scholar] [CrossRef]
- Solass, W.; Struller, F.; Horvath, P.; Königsrainer, A.; Sipos, B.; Weinreich, F.-J. Morphology of the peritoneal cavity and pathophysiological consequences. Pleura Peritoneum 2016, 1, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Solass, W.; Herbette, A.; Schwarz, T.; Hetzel, A.; Sun, J.-S.; Dutreix, M.; Reymond, M.A. Therapeutic approach of human peritoneal carcinomatosis with Dbait in combination with capnoperitoneum: Proof of concept. Surg. Endosc. 2012, 26, 847–852. [Google Scholar] [CrossRef] [PubMed]
- Tate, S.J.; Torkington, J. Pressurized intraperitoneal aerosol chemotherapy: A review of the introduction of a new surgical technology using the IDEAL framework. BJS Open 2020, 4, 206–215. [Google Scholar] [CrossRef]
- Solass, W.; Kerb, R.; Mürdter, T.; Giger-Pabst, U.; Strumberg, D.; Tempfer, C.; Zieren, J.; Schwab, M.; Reymond, M.A. Intraperitoneal Chemotherapy of Peritoneal Carcinomatosis Using Pressurized Aerosol as an Alternative to Liquid Solution: First Evidence for Efficacy. Ann. Surg. Oncol. 2014, 21, 553–559. [Google Scholar] [CrossRef]
- Solaß, W.; Giger-Pabst, U.; Zieren, J.; Reymond, M.A. Pressurized Intraperitoneal Aerosol Chemotherapy (PIPAC): Occupational Health and Safety Aspects. Ann. Surg. Oncol. 2013, 20, 3504–3511. [Google Scholar] [CrossRef]
- Blanco, A.; Giger-Pabst, U.; Solass, W.; Zieren, J.; Reymond, M.A. Renal and Hepatic Toxicities After Pressurized Intraperitoneal Aerosol Chemotherapy (PIPAC). Ann. Surg. Oncol. 2013, 20, 2311–2316. [Google Scholar] [CrossRef]
- Willaert, W.; Van de Sande, L.; Van Daele, E.; Van De Putte, D.; Van Nieuwenhove, Y.; Pattyn, P.; Ceelen, W. Safety and preliminary efficacy of electrostatic precipitation during pressurized intraperitoneal aerosol chemotherapy (PIPAC) for unresectable carcinomatosis. Eur. J. Surg. Oncol. 2019, 45, 2302–2309. [Google Scholar] [CrossRef]
- Lurvink, R.J.; Tajzai, R.; Rovers, K.P.; Wassenaar, E.C.E.; Moes, D.-J.A.R.; Pluimakers, G.; Boerma, D.; Burger, J.W.A.; Nienhuijs, S.W.; de Hingh, I.H.J.T.; et al. Systemic Pharmacokinetics of Oxaliplatin After Intraperitoneal Administration by Electrostatic Pressurized Intraperitoneal Aerosol Chemotherapy (ePIPAC) in Patients with Unresectable Colorectal Peritoneal Metastases in the CRC-PIPAC Trial. Ann. Surg. Oncol. 2020, 28, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Di Giorgio, A.; Abatini, C.; Attalla El Halabieh, M.; Vita, E.; Vizzielli, G.; Gallotta, V.; Pacelli, F.; Rotolo, S. From palliation to cure: PIPAC for peritoneal malignancies. Minerva Med. 2019, 110, 385–398. [Google Scholar] [CrossRef] [PubMed]
- Pressurized Intraperitoneal Aerosol Chemotherapy (PIPAC) Applied to Platinum-Resistant Recurrence of Ovarian Tumor—Full Text View—ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT02735928 (accessed on 23 February 2021).
- Park, S.Y.; Choi, G.-S.; Park, J.S.; Kim, H.J.; Yang, C.-S.; Kim, J.G.; Kang, B.W. Efficacy of Early Postoperative Intraperitoneal Chemotherapy After Complete Surgical Resection of Peritoneal Metastasis from Colorectal Cancer: A Case–Control Study from a Single Center. Ann. Surg. Oncol. 2016, 23, 2266–2273. [Google Scholar] [CrossRef] [PubMed]
- Intraperitoneal Cisplatin and Paclitaxel in Ovarian Cancer. Available online: https://www.nejm.org/doi/full/10.1056/nejmoa052985 (accessed on 18 October 2020).
- Fagotti, A.; Petrillo, M.; Costantini, B.; Fanfani, F.; Gallotta, V.; Chiantera, V.; Turco, L.C.; Bottoni, C.; Scambia, G. Minimally invasive secondary cytoreduction plus HIPEC for recurrent ovarian cancer: A case series. Gynecol. Oncol. 2014, 132, 303–306. [Google Scholar] [CrossRef] [PubMed]
- Valle, M.; Van der Speeten, K.; Garofalo, A. Laparoscopic hyperthermic intraperitoneal peroperative chemotherapy (HIPEC) in the management of refractory malignant ascites: A multi-institutional retrospective analysis in 52 patients. J. Surg. Oncol. 2009, 100, 331–334. [Google Scholar] [CrossRef]
- Tuvin, D.; Berger, Y.; Aycart, S.N.; Shtilbans, T.; Hiotis, S.; Labow, D.M.; Sarpel, U. Prophylactic hyperthermic intraperitoneal chemotherapy in patients with epithelial appendiceal neoplasms. Int. J. Hyperth. Off. J. Eur. Soc. Hyperthermic 2016, 32, 311–315. [Google Scholar] [CrossRef]
- André, N.; Carré, M.; Pasquier, E. Metronomics: Towards personalized chemotherapy? Nat. Rev. Clin. Oncol. 2014, 11, 413–431. [Google Scholar] [CrossRef]
- Yonemura, Y.; Bandou, E.; Kinoshita, K.; Kawamura, T.; Takahashi, S.; Endou, Y.; Sasaki, T. Effective therapy for peritoneal dissemination in gastric cancer. Surg. Oncol. Clin. N. Am. 2003, 12, 635–648. [Google Scholar] [CrossRef]
- Ishigami, H.; Kitayama, J.; Kaisaki, S.; Hidemura, A.; Kato, M.; Otani, K.; Kamei, T.; Soma, D.; Miyato, H.; Yamashita, H.; et al. Phase II study of weekly intravenous and intraperitoneal paclitaxel combined with S-1 for advanced gastric cancer with peritoneal metastasis. Ann. Oncol. 2010, 21, 67–70. [Google Scholar] [CrossRef]
- Zylberberg, B.; Dormont, D.; Janklewicz, S.; Darai, E.; Bretel, J.J.; Poncelet, C.; Guillet, J.L.; Madelenat, P. Response to neo-adjuvant intraperitoneal and intravenous immunochemotherapy followed by interval secondary cytoreduction in stage IIIc ovarian cancer. Eur. J. Gynaecol. Oncol. 2001, 22, 40–45. [Google Scholar]
- Yonemura, Y.; Ishibashi, H.; Hirano, M.; Mizumoto, A.; Takeshita, K.; Noguchi, K.; Takao, N.; Ichinose, M.; Liu, Y.; Li, Y. Effects of Neoadjuvant Laparoscopic Hyperthermic Intraperitoneal Chemotherapy and Neoadjuvant Intraperitoneal/Systemic Chemotherapy on Peritoneal Metastases from Gastric Cancer. Ann. Surg. Oncol. 2017, 24, 478–485. [Google Scholar] [CrossRef]
- Fujiwara, Y.; Takiguchi, S.; Nakajima, K.; Miyata, H.; Yamasaki, M.; Kurokawa, Y.; Okada, K.; Mori, M.; Doki, Y. Neoadjuvant Intraperitoneal and Systemic Chemotherapy for Gastric Cancer Patients with Peritoneal Dissemination. Ann. Surg. Oncol. 2011, 18, 3726–3731. [Google Scholar] [CrossRef]
- Yonemura, Y.; Bandou, E.; Sawa, T.; Yoshimitsu, Y.; Endou, Y.; Sasaki, T.; Sugarbaker, P.H. Neoadjuvant treatment of gastric cancer with peritoneal dissemination. Eur. J. Surg. Oncol. 2006, 32, 661–665. [Google Scholar] [CrossRef]
- Muñoz-Casares, F.C.; Rufián, S.; Arjona-Sánchez, Á.; Rubio, M.J.; Díaz, R.; Casado, Á.; Naranjo, Á.; Díaz-Iglesias, C.J.; Ortega, R.; Muñoz-Villanueva, M.C.; et al. Neoadjuvant intraperitoneal chemotherapy with paclitaxel for the radical surgical treatment of peritoneal carcinomatosis in ovarian cancer: A prospective pilot study. Cancer Chemother. Pharmacol. 2011, 68, 267–274. [Google Scholar] [CrossRef][Green Version]
- Prabhu, A.; Brandl, A.; Wakama, S.; Sako, S.; Ishibashi, H.; Mizumoto, A.; Takao, N.; Noguchi, K.; Motoi, S.; Ichinose, M.; et al. Neoadjuvant Intraperitoneal Chemotherapy in Patients with Pseudomyxoma Peritonei-A Novel Treatment Approach. Cancers 2020, 12, 2212. [Google Scholar] [CrossRef] [PubMed]
- Yonemura, Y. A new bidirectional intraperitoneal and systemic induction chemotherapy (BISIC) for the peritoneal metastasis from gastric cancer in neoadjuvant setting. Integr. Cancer Sci. Ther. 2014, 1, 26–29. [Google Scholar] [CrossRef]
- Yonemura, Y.; Endou, Y.; Shinbo, M.; Sasaki, T.; Hirano, M.; Mizumoto, A.; Matsuda, T.; Takao, N.; Ichinose, M.; Mizuno, M.; et al. Safety and efficacy of bidirectional chemotherapy for treatment of patients with peritoneal dissemination from gastric cancer: Selection for cytoreductive surgery. J. Surg. Oncol. 2009, 100, 311–316. [Google Scholar] [CrossRef]
- Kuramoto, M.; Shimada, S.; Ikeshima, S.; Matsuo, A.; Yagi, Y.; Matsuda, M.; Yonemura, Y.; Baba, H. Extensive intraoperative peritoneal lavage as a standard prophylactic strategy for peritoneal recurrence in patients with gastric carcinoma. Ann. Surg. 2009, 250, 242–246. [Google Scholar] [CrossRef] [PubMed]
- Cui, H.-B.; Ge, H.-E.; Bai, X.-Y.; Zhang, W.; Zhang, Y.-Y.; Wang, J.; Li, X.; Xing, L.-P.; Guo, S.-H.; Wang, Z.-Y. Effect of neoadjuvant chemotherapy combined with hyperthermic intraperitoneal perfusion chemotherapy on advanced gastric cancer. Exp. Ther. Med. 2014, 7, 1083–1088. [Google Scholar] [CrossRef] [PubMed]
- Klaver, C.E.L.; Wisselink, D.D.; Punt, C.J.A.; Snaebjornsson, P.; Crezee, J.; Aalbers, A.G.J.; Brandt, A.; Bremers, A.J.A.; Burger, J.W.A.; Fabry, H.F.J.; et al. Adjuvant hyperthermic intraperitoneal chemotherapy in patients with locally advanced colon cancer (COLOPEC): A multicentre, open-label, randomised trial. Lancet Gastroenterol. Hepatol. 2019, 4, 761–770. [Google Scholar] [CrossRef]
- Yang, X.-J.; Huang, C.-Q.; Suo, T.; Mei, L.-J.; Yang, G.-L.; Cheng, F.-L.; Zhou, Y.-F.; Xiong, B.; Yonemura, Y.; Li, Y. Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy Improves Survival of Patients with Peritoneal Carcinomatosis from Gastric Cancer: Final Results of a Phase III Randomized Clinical Trial. Ann. Surg. Oncol. 2011, 18, 1575–1581. [Google Scholar] [CrossRef] [PubMed]
- Quenet, F.; Elias, D.; Roca, L.; Goéré, D.; Ghouti, L.; Pocard, M.; Facy, O.; Arvieux, C.; Lorimier, G.; Pezet, D.; et al. A UNICANCER phase III trial of Hyperthermic Intra-peritoneal Chemotherapy (HIPEC) for Colorectal Peritoneal Carcinomatosis. PRODIGE 7. Eur. J. Surg. Oncol. 2019, 45, e17. [Google Scholar] [CrossRef]
- Levine, E.A.; Stewart, J.H.; Shen, P.; Russell, G.B.; Loggie, B.L.; Votanopoulos, K.I. Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy for Peritoneal Surface Malignancy: Experience with 1000 Patients. J. Am. Coll. Surg. 2014, 218, 573–585. [Google Scholar] [CrossRef] [PubMed]
- Yan, T.D.; Welch, L.; Black, D.; Sugarbaker, P.H. A systematic review on the efficacy of cytoreductive surgery combined with perioperative intraperitoneal chemotherapy for diffuse malignancy peritoneal mesothelioma. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2007, 18, 827–834. [Google Scholar] [CrossRef] [PubMed]
- Gamboa, A.C.; Liu, Y.; Zaidi, M.Y.; Lee, R.M.; Russell, M.C.; Cardona, K.; Maithel, S.K. Duodenal neuroendocrine tumors: Somewhere between the pancreas and small bowel? J. Clin. Oncol. 2019, 37, 377. [Google Scholar] [CrossRef]
- Yang, Y.; Li, Y.; Du, X. Does Intraperitoneal Chemotherapy Increase the Incidence of Anastomotic Leakage after Colorectal Cancer Surgery: A Systematic Review and Meta-Analysis. Gastroenterol. Res. Pract. 2021, 2021, 1–5. [Google Scholar] [CrossRef]
- Soucisse, M.L.; Liauw, W.; Hicks, G.; Morris, D.L. Early postoperative intraperitoneal chemotherapy for lower gastrointestinal neoplasms with peritoneal metastasis: A systematic review and critical analysis. Pleura Peritoneum 2019, 4. [Google Scholar] [CrossRef] [PubMed]
- Yu, W.; Whang, I.; Chung, H.Y.; Averbach, A.; Sugarbaker, P.H. Indications for Early Postoperative Intraperitoneal Chemotherapy of Advanced Gastric Cancer: Results of a Prospective Randomized Trial. World J. Surg. 2001, 25, 985–990. [Google Scholar] [CrossRef]
- Yu, W.; Whang, I.; Averbach, A.; Chang, D.; Sugarbaker, P.H. Morbidity and mortality of early postoperative intraperitoneal chemotherapy as adjuvant therapy for gastric cancer. Am. Surg. 1998, 64, 1104–1108. [Google Scholar] [PubMed]
- Fan, R.; Tong, A.; Li, X.; Gao, X.; Mei, L.; Zhou, L.; Zhang, X.; You, C.; Guo, G. Enhanced antitumor effects by docetaxel/LL37-loaded thermosensitive hydrogel nanoparticles in peritoneal carcinomatosis of colorectal cancer. Int. J. Nanomed. 2015, 10, 7291–7305. [Google Scholar] [CrossRef]
- Langer, R. Drug delivery and targeting. Nature 1998, 392, 5–10. [Google Scholar] [PubMed]
- Khosrawipour, T.; Schubert, J.; Kulas, J.; Migdal, P.; Arafkas, M.; Bania, J.; Khosrawipour, V. Creating nanocrystallized chemotherapy: The differences in pressurized aerosol chemotherapy (PAC) via intracavitary (IAG) and extracavitary aerosol generation (EAG) regarding particle generation, morphology and structure. J. Cancer 2020, 11, 1308–1314. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.L.; Brady, M.F.; Wenzel, L.; Fleming, G.F.; Huang, H.Q.; DiSilvestro, P.A.; Fujiwara, K.; Alberts, D.S.; Zheng, W.; Tewari, K.S.; et al. Randomized Trial of Intravenous Versus Intraperitoneal Chemotherapy Plus Bevacizumab in Advanced Ovarian Carcinoma: An NRG Oncology/Gynecologic Oncology Group Study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2019, 37, 1380–1390. [Google Scholar] [CrossRef] [PubMed]
- Schubert, J.; Khosrawipour, T.; Reinhard, S.; Arafkas, M.; Martino, A.; Bania, J.; Pieczka, M.; Pigazzi, A.; Khosrawipour, V. The concept of foam as a drug carrier for intraperitoneal chemotherapy, feasibility, cytotoxicity and characteristics. Sci. Rep. 2020, 10, 10341. [Google Scholar] [CrossRef]
- de Bree, E.; Michelakis, D.; Stamatiou, D.; Romanos, J.; Zoras, O. Pharmacological principles of intraperitoneal and bidirectional chemotherapy. Pleura Peritoneum 2017, 2, 47–62. [Google Scholar] [CrossRef]
- Shannon, N.B.; Tan, J.W.-S.; Tan, H.L.; Wang, W.; Chen, Y.; Lim, H.J.; Tan, Q.X.; Hendrikson, J.; Ng, W.H.; Loo, L.Y.; et al. A set of molecular markers predicts chemosensitivity to Mitomycin-C following cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for colorectal peritoneal metastasis. Sci. Rep. 2019, 9, 10572. [Google Scholar] [CrossRef]
- Lei, Y.; Tang, L.; Hu, J.; Wang, S.; Liu, Y.; Yang, M.; Zhang, J.; Tang, B. Inhibition of MGMT-mediated autophagy suppression decreases cisplatin chemosensitivity in gastric cancer. Biomed. Pharmacother. 2020, 125, 109896. [Google Scholar] [CrossRef]
- Qian, X.; Li, X.; Lu, Z. Protein kinase activity of the glycolytic enzyme PGK1 regulates autophagy to promote tumorigenesis. Autophagy 2017, 13, 1246–1247. [Google Scholar] [CrossRef]
- Archid, R.; Zieker, D.; Weinreich, F.-J.; Hönes, F.; Königsrainer, A.; Quintanilla-Martínez, L.; Reymond, M.A.; Solass, W. shRNA-mediated inhibition of PhosphoGlycerate Kinase 1 (PGK1) enhances cytotoxicity of intraperitoneal chemotherapy in peritoneal metastasis of gastric origin. Eur. J. Surg. Oncol. 2020, 46, 613–619. [Google Scholar] [CrossRef]
- Gokare, P.; Finnberg, N.K.; Abbosh, P.H.; Dai, J.; Murphy, M.E.; El-Deiry, W.S. P53 represses pyrimidine catabolic gene dihydropyrimidine dehydrogenase (DPYD) expression in response to thymidylate synthase (TS) targeting. Sci. Rep. 2017, 7, 9711. [Google Scholar] [CrossRef]
- Zhang, R.; Pan, T.; Xiang, Y.; Zhang, M.; Feng, J.; Liu, S.; Duan, T.; Chen, P.; Zhai, B.; Chen, X.; et al. β-Elemene Reverses the Resistance of p53-Deficient Colorectal Cancer Cells to 5-Fluorouracil by Inducing Pro-death Autophagy and Cyclin D3-Dependent Cycle Arrest. Front. Bioeng. Biotechnol. 2020, 8, 378. [Google Scholar] [CrossRef] [PubMed]
- Ando, H.; Ishida, T. An RNAi therapeutic, DFP-10825, for intraperitoneal and intrapleural malignant cancers. Adv. Drug Deliv. Rev. 2020, 154–155, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Kanda, M.; Shimizu, D.; Tanaka, H.; Tanaka, C.; Kobayashi, D.; Hayashi, M.; Iwata, N.; Niwa, Y.; Yamada, S.; Fujii, T.; et al. Significance of SYT8 For the Detection, Prediction, and Treatment of Peritoneal Metastasis from Gastric Cancer. Ann. Surg. 2018, 267, 495–503. [Google Scholar] [CrossRef]
- Pardoll, D.M. The blockade of immune checkpoints in cancer immunotherapy. Nat. Rev. Cancer 2012, 12, 252–264. [Google Scholar] [CrossRef] [PubMed]
- Varghese, S.; Rabkin, S.D. Oncolytic herpes simplex virus vectors for cancer virotherapy. Cancer Gene Ther. 2002, 9, 967–978. [Google Scholar] [CrossRef]
- Katz, S.C.; Point, G.R.; Cunetta, M.; Thorn, M.; Guha, P.; Espat, N.J.; Boutros, C.; Hanna, N.; Junghans, R.P. Regional CAR-T cell infusions for peritoneal carcinomatosis are superior to systemic delivery. Cancer Gene Ther. 2016, 23, 142–148. [Google Scholar] [CrossRef]
- Kaufman, H.L.; Kohlhapp, F.J.; Zloza, A. Oncolytic viruses: A new class of immunotherapy drugs. Nat. Rev. Drug Discov. 2015, 14, 642–662. [Google Scholar] [CrossRef]
- Magge, D.; Guo, Z.S.; O’Malley, M.E.; Francis, L.; Ravindranathan, R.; Bartlett, D.L. Inhibitors of C5 complement enhance vaccinia virus oncolysis. Cancer Gene Ther. 2013, 20, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Auer, R.C.; Sivajohanathan, D.; Biagi, J.; Conner, J.; Kennedy, E.; May, T. Indications for hyperthermic intraperitoneal chemotherapy with cytoreductive surgery: A systematic review. Eur. J. Cancer 2020, 127, 76–95. [Google Scholar] [CrossRef]
- van Driel, W.J.; Koole, S.N.; Sikorska, K.; Schagen van Leeuwen, J.H.; Schreuder, H.W.R.; Hermans, R.H.M.; de Hingh, I.H.J.T.; van der Velden, J.; Arts, H.J.; Massuger, L.F.A.G.; et al. Hyperthermic Intraperitoneal Chemotherapy in Ovarian Cancer. N. Engl. J. Med. 2018, 378, 230–240. [Google Scholar] [CrossRef]
- Vergote, I.; Harter, P.; Chiva, L. Hyperthermic intraperitoneal chemotherapy does not improve survival in advanced ovarian cancer. Cancer 2019, 125 (Suppl. S24), 4594–4597. [Google Scholar] [CrossRef]
- Fagotti, A.; Costantini, B.; Petrillo, M.; Vizzielli, G.; Fanfani, F.; Margariti, P.A.; Turco, L.C.; Piovano, E.; Scambia, G. Cytoreductive surgery plus HIPEC in platinum-sensitive recurrent ovarian cancer patients: A case-control study on survival in patients with two year follow-up. Gynecol. Oncol. 2012, 127, 502–505. [Google Scholar] [CrossRef] [PubMed]
- Cianci, S.; Ronsini, C.; Vizzielli, G.; Tropea, A.; Biondi, A.; Scambia, G.; Fagotti, A. Cytoreductive surgery followed by HIPEC repetition for secondary ovarian cancer recurrence. Updat. Surg. 2019, 71, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Cianci, S.; Riemma, G.; Ronsini, C.; De Franciscis, P.; Torella, M.; Schiattarella, A.; La Verde, M.; Colacurci, N. Hyperthermic intraperitoneal chemotherapy (HIPEC) for ovarian cancer recurrence: Systematic review and meta-analysis. Gland Surg. 2020, 9, 1140–1148. [Google Scholar] [CrossRef]
- Paris, I.; Cianci, S.; Vizzielli, G.; Fagotti, A.; Ferrandina, G.; Gueli Alletti, S.; Costantini, B.; Cosentino, F.; Capoluongo, E.; Pasqualoni, M.; et al. Upfront HIPEC and bevacizumab-containing adjuvant chemotherapy in advanced epithelial ovarian cancer. Int. J. Hyperth. Off. J. Eur. Soc. Hyperthermic 2018, 35, 370–374. [Google Scholar] [CrossRef] [PubMed]
- Scambia, P.G. Surgery Plus Hyperthermic Intra-Peritoneal Chemotherapy (HIPEC) Versus Surgery Alone in Patients with Platinum-Sensitive First Recurrence of Ovarian Cancer: A Prospective Randomized Multicenter Trial. Report No.: NCT01539785. 2014. Available online: https://clinicaltrials.gov/ct2/show/NCT01539785 (accessed on 22 February 2021).
- Verma, V.; Sleightholm, R.L.; Rusthoven, C.G.; Koshy, M.; Sher, D.J.; Grover, S.; Simone, C.B. Malignant Peritoneal Mesothelioma: National Practice Patterns, Outcomes, and Predictors of Survival. Ann. Surg. Oncol. 2018, 25, 2018–2026. [Google Scholar] [CrossRef] [PubMed]
- Carr, N.J.; Cecil, T.D.; Mohamed, F.; Sobin, L.H.; Sugarbaker, P.H.; González-Moreno, S.; Taflampas, P.; Chapman, S.; Moran, B.J. Peritoneal Surface Oncology Group International A Consensus for Classification and Pathologic Reporting of Pseudomyxoma Peritonei and Associated Appendiceal Neoplasia: The Results of the Peritoneal Surface Oncology Group International (PSOGI) Modified Delphi Process. Am. J. Surg. Pathol. 2016, 40, 14–26. [Google Scholar] [CrossRef] [PubMed]
- Di Leo, A.; Corvasce, A.; Weindelmayer, J.; Mason, E.J.; Casella, F.; de Manzoni, G. Cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) in pseudomyxoma peritonei of appendiceal origin: Result of a single centre study. Updat. Surg. 2020, 72, 1207–1212. [Google Scholar] [CrossRef]
- Grass, F.; Vuagniaux, A.; Teixeira-Farinha, H.; Lehmann, K.; Demartines, N.; Hübner, M. Systematic review of pressurized intraperitoneal aerosol chemotherapy for the treatment of advanced peritoneal carcinomatosis. Br. J. Surg. 2017, 104, 669–678. [Google Scholar] [CrossRef] [PubMed]
- Tempfer, C.B.; Winnekendonk, G.; Solass, W.; Horvat, R.; Giger-Pabst, U.; Zieren, J.; Rezniczek, G.A.; Reymond, M.-A. Pressurized intraperitoneal aerosol chemotherapy in women with recurrent ovarian cancer: A phase 2 study. Gynecol. Oncol. 2015, 137, 223–228. [Google Scholar] [CrossRef]
- Khomiakov, V.; Ryabov, A.; Bolotina, L.V.; Utkina, A.; Cheremisov, V.; Kolobaev, I.; Ivanov, A.; Chayka, A.; Sobolev, D. Bidirectional Chemotherapy in Gastric Cancer (GC) with Peritoneal Carcinomatosis (PC) Combining Intravenous Chemotherapy with Intraperitoneal Chemotherapy with Low-Dose Cisplatin and Doxorubicin Administered as a Pressurized Aerosol: An Open-Label, Phase II Study. Available online: https://ascopubs.org/doi/abs/10.1200/JCO.2017.35.15_suppl.e15532 (accessed on 20 October 2020).
- Sande, L.V.D.; Graversen, M.; Hubner, M.; Pocard, M.; Reymond, M.; Vaira, M.; Cosyns, S.; Willaert, W.; Ceelen, W. Intraperitoneal aerosolization of albumin-stabilized paclitaxel nanoparticles (AbraxaneTM) for peritoneal carcinomatosis—A phase I first-in-human study. Pleura Peritoneum 2018, 3. [Google Scholar] [CrossRef]
- Nowacki, M.; Alyami, M.; Villeneuve, L.; Mercier, F.; Hubner, M.; Willaert, W.; Ceelen, W.; Reymond, M.; Pezet, D.; Arvieux, C.; et al. Multicenter comprehensive methodological and technical analysis of 832 pressurized intraperitoneal aerosol chemotherapy (PIPAC) interventions performed in 349 patients for peritoneal carcinomatosis treatment: An international survey study. Eur. J. Surg. Oncol. 2018, 44, 991–996. [Google Scholar] [CrossRef] [PubMed]
- Sgarbura, O.; Gourgou, S.; Tosi, D.; Bakrin, N.; Bouazza, N.; Delaine, S.; De Forges, H.; Pocard, M.; Quénet, F. MESOTIP: Phase II multicenter randomized trial evaluating the association of PIPAC and systemic chemotherapy vs. systemic chemotherapy alone as 1st-line treatment of malignant peritoneal mesothelioma. Pleura Peritoneum 2019, 4, 20190010. [Google Scholar] [CrossRef] [PubMed]
- Eveno, C.; Jouvin, I.; Pocard, M. PIPAC EstoK 01: Pressurized IntraPeritoneal Aerosol Chemotherapy with cisplatin and doxorubicin (PIPAC C/D) in gastric peritoneal metastasis: A randomized and multicenter phase II study. Pleura Peritoneum 2018, 3, 20180116. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Drug Class | Subgroup | Drug | AUC (Area under the Curve) Ratio | Synergism with Heat | with Normothermia/with HIPEC | Indications |
|---|---|---|---|---|---|---|
| Alkylating agents | Platinum agents | Cisplatin | 7 | Yes | +/+ [17,18] | Ovarian cancers |
| Carboplatin | 18 | Bladder cancers | ||||
| Oxaliplatin | 16 | Colorectal cancers | ||||
| Gastric cancers | ||||||
| Topoisomerase inhibitors | Topoisomerase II inhibitors | Anthracyclines (Doxorubicin) | 230 | Yes | −/+ [19] | Gastric cancers |
| Mitoxantrone | 15.2 | |||||
| Antimetabolites | Pyrimidine antagonists | 5-Fluorouracil (5-FU) | 250 | Minimum | +/− [18] | Urothelial cell carcinoma, Colorectal cancer |
| Pancreatic cancer | ||||||
| Mitotic inhibitors | Taxanes | Docetaxel | 1000 | No | +/− [20] | Ovarian and gastric cancers |
| Paclitaxel | ||||||
| Antibiotic | Mitomycin C | 23.5 | Yes | −/+ [18] | Bladder carcinoma | |
| Colorectal cancers | ||||||
| Appendiceal mucocele |
| Recognized Indications | Indications under Evaluation |
|---|---|
| Stage III epithelial ovarian cancer | Peritoneal carcinomatosis (PC) from gastric cancers without extra-abdominal metastases |
| Peritoneal mesothelioma (PM) | Peritoneal carcinomatosis (PC) from colorectal cancers without extra-abdominal metastases |
| Pseudomyxoma peritonei (PMP) | |
| Peritoneal carcinomatosis (PC) from different cancerous origins, without extra-abdominal metastases: adenocarcinoma of the appendix, goblet cell carcinoma of the small bowel (SB) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Christou, N.; Auger, C.; Battu, S.; Lalloué, F.; Jauberteau-Marchan, M.-O.; Hervieu, C.; Verdier, M.; Mathonnet, M. Intraperitoneal Chemotherapy for Peritoneal Metastases: Technical Innovations, Preclinical and Clinical Advances and Future Perspectives. Biology 2021, 10, 225. https://doi.org/10.3390/biology10030225
Christou N, Auger C, Battu S, Lalloué F, Jauberteau-Marchan M-O, Hervieu C, Verdier M, Mathonnet M. Intraperitoneal Chemotherapy for Peritoneal Metastases: Technical Innovations, Preclinical and Clinical Advances and Future Perspectives. Biology. 2021; 10(3):225. https://doi.org/10.3390/biology10030225
Chicago/Turabian StyleChristou, Niki, Clément Auger, Serge Battu, Fabrice Lalloué, Marie-Odile Jauberteau-Marchan, Céline Hervieu, Mireille Verdier, and Muriel Mathonnet. 2021. "Intraperitoneal Chemotherapy for Peritoneal Metastases: Technical Innovations, Preclinical and Clinical Advances and Future Perspectives" Biology 10, no. 3: 225. https://doi.org/10.3390/biology10030225
APA StyleChristou, N., Auger, C., Battu, S., Lalloué, F., Jauberteau-Marchan, M.-O., Hervieu, C., Verdier, M., & Mathonnet, M. (2021). Intraperitoneal Chemotherapy for Peritoneal Metastases: Technical Innovations, Preclinical and Clinical Advances and Future Perspectives. Biology, 10(3), 225. https://doi.org/10.3390/biology10030225