
Zero-Fluoroscopy Cardiac Ablation: Technology Is Moving Forward in Complex Procedures—A Novel Workflow for Atrial Fibrillation

 ,
, 
 , and
, and {kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. State of the Art
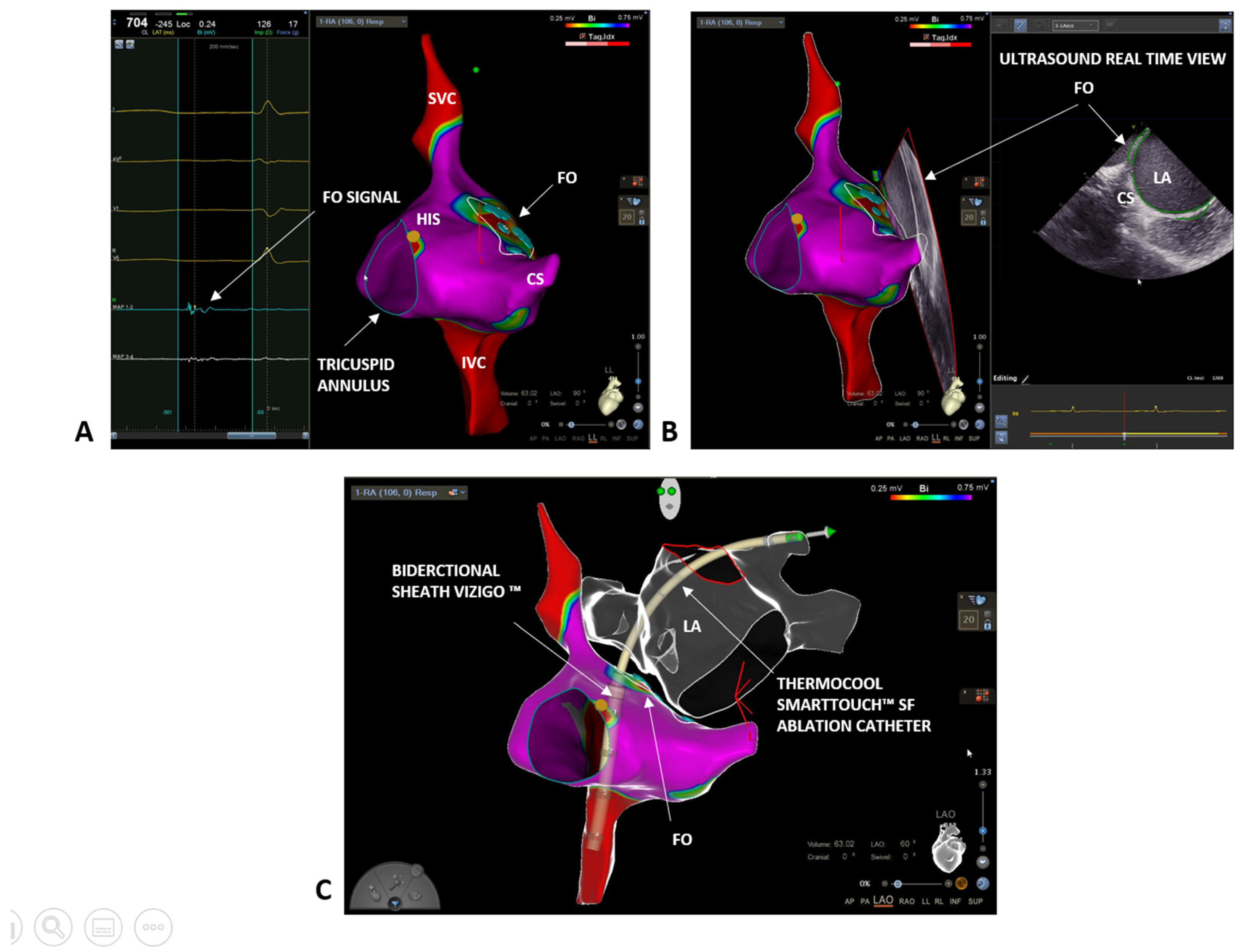
2. Case 1: Paroxysmal Atrial Fibrillation
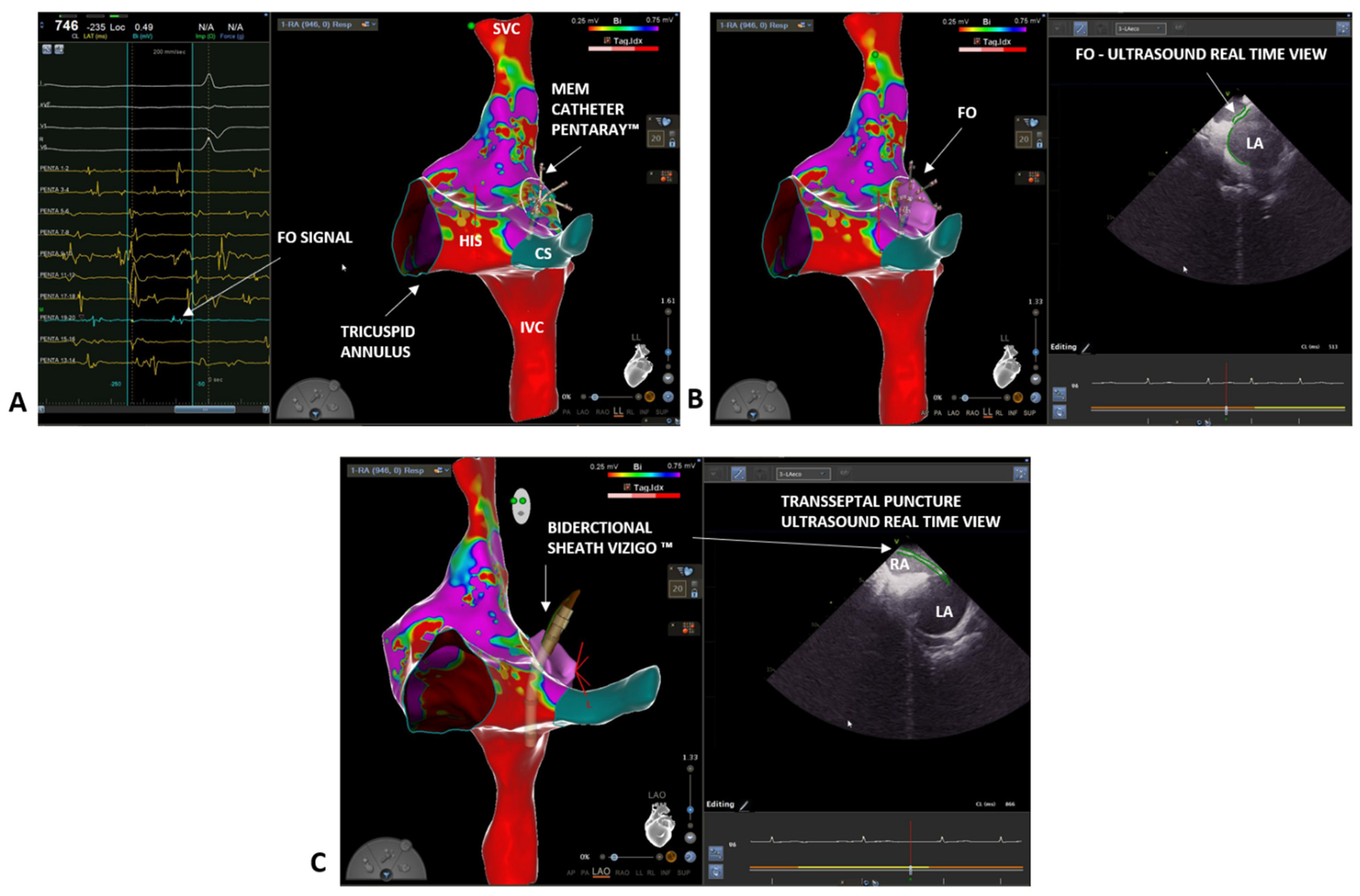
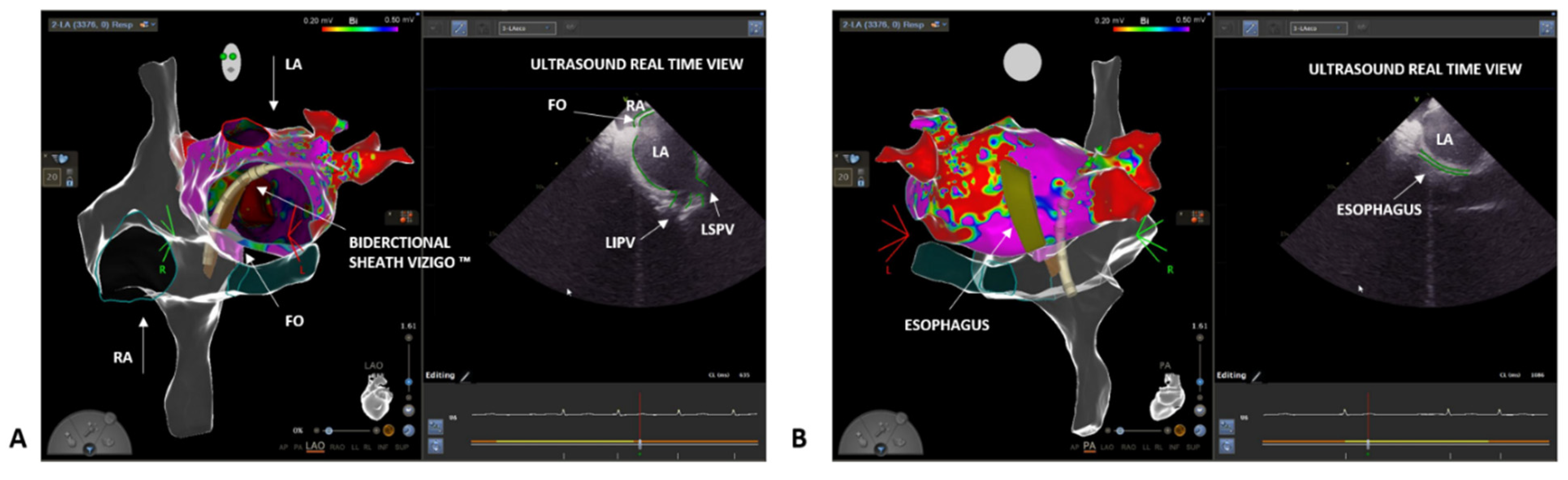
3. Case 2: Persistent Atrial Fibrillation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Heidbuchel, H.; Wittkampf, F.H.M.; Vano, E.; Ernst, S.; Schilling, R.; Picano, E.; Mont, L.; Jais, P.; de Bono, J.; Piorkowski, C.; et al. Practical Ways to Reduce Radiation Dose for Patients and Staff during Device Implantations and Electrophysiological Procedures. Europace 2014, 16, 946–964. [Google Scholar] [CrossRef] [PubMed]
- Gaita, F.; Guerra, P.G.; Battaglia, A.; Anselmino, M. The Dream of Near-Zero X-Rays Ablation Comes True. Eur. Heart J. 2016, 37, 2749–2755. [Google Scholar] [CrossRef] [PubMed]
- Limacher, M.C.; Douglas, P.S.; Germano, G.; Laskey, W.K.; Lindsay, B.D.; McKetty, M.H.; Moore, M.E.; Park, J.K.; Prigent, F.M.; Walsh, M.N. ACC Expert Consensus Document. Radiation Safety in the Practice of Cardiology. American College of Cardiology. J. Am. Coll. Cardiol. 1998, 31, 892–913. [Google Scholar] [CrossRef] [Green Version]
- Pani, A.; Giuseppina, B.; Bonanno, C.; Bongiorni, M.G.; Bottoni, N.; Brambilla, R.; de Ceglia, S.; Bella, P.D.; de Vito, G.; Malaspina, D.; et al. Predictors of Zero X-Ray Ablation for Supraventricular Tachycardias in a Nationwide Multicenter Experience. Circ. Arrhythmia Electrophysiol. 2018, 11, e005592. [Google Scholar] [CrossRef]
- Jan, M.; Žižek, D.; Kalinšek, T.P.; Kuhelj, D.; Trunk, P.; Kolar, T.; Kšela, J.; Rauber, M.; Yazici, M. Minimising Radiation Exposure in Catheter Ablation of Ventricular Arrhythmias. BMC Cardiovasc. Disord. 2021, 21, 306. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]
- Romero, J.; Patel, K.; Briceno, D.; Alviz, I.; Tarantino, N.; Rocca, D.G.D.; Natale, V.; Zhang, X.-D.; di Biase, L. Fluoroless Atrial Fibrillation Catheter Ablation: Technique and Clinical Outcomes. Card. Electrophysiol. Clin. 2020, 12, 233–245. [Google Scholar] [CrossRef]
- Malagù, M.; Vitali, F.; Marchini, F.; Fiorio, A.; Sirugo, P.; Mele, D.; Brieda, A.; Balla, C.; Bertini, M. Ablation of Atrioventricular Nodal Re-Entrant Tachycardia Combining Irrigated Flexible-Tip Catheters and Three-Dimensional Electroanatomic Mapping: Long-Term Outcomes. J. Cardiovasc. Dev. Dis. 2021, 8, 61. [Google Scholar] [CrossRef]
- Scaglione, M.; Ebrille, E.; di Clemente, F.; Gaita, F.; Bradfield, J.S. Catheter Ablation of Atrial Fibrillation without Radiation Exposure Using A 3D Mapping System. J. Atr. Fibrillation 2015, 7, 56–62. [Google Scholar] [CrossRef]
- Falasconi, G.; Penela, D.; Soto-Iglesias, D.; Jáuregui, B.; Chauca, A.; Antonio, R.S.; Ordoñez, A.; Teres, C.; Carreño, J.M.; Scherer, C.; et al. A standardized stepwise zero-fluoroscopy approach with transesophageal echocardiography guidance for atrial fibrillation ablation. J. Interv. Card. Electrophysiol. 2021. epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Tahin, T.; Riba, A.; Nemeth, B.; Arvai, F.; Lupkovics, G.; Szeplaki, G.; Geller, L. Implementation of a zero fluoroscopic workflow using a simplified intracardiac echocardiography guided method for catheter ablation of atrial fibrillation, including repeat procedures. BMC Cardiovasc. Disord. 2021, 21, 407. [Google Scholar] [CrossRef] [PubMed]
- Sommer, P.; Bertagnolli, L.; Kircher, S.; Arya, A.; Bollmann, A.; Richter, S.; Rolf, S.; Hindricks, G. Safety profile of near-zero fluoroscopy atrial fibrillation ablation with non-fluoroscopic catheter visualization: Experience from 1000 consecutive procedures. EP Eur. 2018, 20, 1952–1958. [Google Scholar] [CrossRef]
- Troisi, F.; Quadrini, F.; di Monaco, A.; Vitulano, N.; Caruso, R.; Guida, P.; Langialonga, T.; Grimaldi, M. Electroanatomic Guidance versus Conventional Fluoroscopy during Transseptal Puncture for Atrial Fibrillation Ablation. J. Cardiovasc. Electrophysiol. 2020, 31, 2607–2613. [Google Scholar] [CrossRef]
- Phlips, T.; Taghji, P.; Haddad, M.E.; Wolf, M.; Knecht, S.; Vandekerckhove, Y.; Tavernier, R.; Duytschaever, M. Improving Procedural and One-Year Outcome after Contact Force-Guided Pulmonary Vein Isolation: The Role of Interlesion Distance, Ablation Index, and Contact Force Variability in the ‘CLOSE’-Protocol. EP Eur. 2018, 20, f419–f427. [Google Scholar] [CrossRef]
- Khongphatthanayothin, A.; Kosar, E.; Nademanee, K. Nonfluoroscopic Three-Dimensional Mapping for Arrhythmia Ablation: Tool or Toy? J. Cardiovasc. Electrophysiol. 2000, 11, 239–243. [Google Scholar] [CrossRef]
- Bertini, M.; Brieda, A.; Balla, C.; Pollastrelli, A.; Smarrazzo, V.; Francesco, V.; Malagù, M.; Ferrari, R. Efficacy and Safety of Catheter Ablation of Atrioventricular Nodal Re-Entrant Tachycardia by Means of Flexible-Tip Irrigated Catheters. J. Interv. Card. Electrophysiol. Int. J. Arrhythm. Pacing 2020, 58, 61–67. [Google Scholar] [CrossRef]
- Hirshfeld, J.W.; Baiter, S.; Brinker, J.A.; Kern, M.J.; Klein, L.W.; Lindsay, B.D.; Tommaso, C.L.; Tracy, C.M.; Wagner, L.K.; Creager, M.A.; et al. ACCF/AHA/HRS/SCAI Clinical Competence Statement on Physician Knowledge to Optimize Patient Safety and Image Quality in Fluoroscopically Guided Invasive Cardiovascular Procedures: A Report of the American College of Cardiology Foundation/American Heart Association/American College of Physicians Task Force on Clinical Competence and Training. Circulation 2005, 111, 511–532. [Google Scholar] [CrossRef]
- Ross, J.; Braunwald, E.; Morrow, A.G. Transseptal Left Atrial Puncture; New Technique for the Measurement of Left Atrial Pressure in Man. Am. J. Cardiol. 1959, 3, 653–655. [Google Scholar] [CrossRef]
- Ross, J.; Braunwald, E.; Morrow, A.G. Transseptal Left Heart Catheterization: A New Diagnostic Method. Prog. Cardiovasc. Dis. 1960, 2, 315–318. [Google Scholar] [CrossRef]
- Brockenbrough, E.C.; Braunwald, E.; Ross, J. Transseptal Left Heart Catheterization A Review of 450 Studies and Description of an Improved Technic. Circulation 1962, 25, 15–21. [Google Scholar] [CrossRef] [Green Version]
- Brockenbrough, E.G.; Braunwald, E. A New Technic for Left Ventricular Angiocardiography and Transseptal Left Heart Catheterization. Am. J. Cardiol. 1960, 6, 1062–1064. [Google Scholar] [CrossRef]
- Yu, R.; Liu, N.; Lu, J.; Zhao, X.; Hu, Y.; Zhang, J.; Xu, F.; Tang, R.; Bai, R.; Akar, J.G.; et al. 3-Dimensional Transseptal Puncture Based on Electrographic Characteristics of Fossa Ovalis: A Fluoroscopy-Free and Echocardiography-Free Method. JACC Cardiovasc. Interv. 2020, 13, 1223–1232. [Google Scholar] [CrossRef] [PubMed]
- Goya, M.; Frame, D.; Gache, L.; Ichishima, Y.; Tayar, D.O.; Goldstein, L.; Lee, S.H.Y. The Use of Intracardiac Echocardiography Catheters in Endocardial Ablation of Cardiac Arrhythmia: Meta-analysis of Efficiency, Effectiveness, and Safety Outcomes. J. Cardiovasc. Electrophysiol. 2020, 31, 664–673. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bertini, M.; Pompei, G.; Tolomeo, P.; Malagù, M.; Fiorio, A.; Balla, C.; Vitali, F.; Rapezzi, C. Zero-Fluoroscopy Cardiac Ablation: Technology Is Moving Forward in Complex Procedures—A Novel Workflow for Atrial Fibrillation. Biology 2021, 10, 1333. https://doi.org/10.3390/biology10121333
Bertini M, Pompei G, Tolomeo P, Malagù M, Fiorio A, Balla C, Vitali F, Rapezzi C. Zero-Fluoroscopy Cardiac Ablation: Technology Is Moving Forward in Complex Procedures—A Novel Workflow for Atrial Fibrillation. Biology. 2021; 10(12):1333. https://doi.org/10.3390/biology10121333
Chicago/Turabian StyleBertini, Matteo, Graziella Pompei, Paolo Tolomeo, Michele Malagù, Alessio Fiorio, Cristina Balla, Francesco Vitali, and Claudio Rapezzi. 2021. "Zero-Fluoroscopy Cardiac Ablation: Technology Is Moving Forward in Complex Procedures—A Novel Workflow for Atrial Fibrillation" Biology 10, no. 12: 1333. https://doi.org/10.3390/biology10121333
APA StyleBertini, M., Pompei, G., Tolomeo, P., Malagù, M., Fiorio, A., Balla, C., Vitali, F., & Rapezzi, C. (2021). Zero-Fluoroscopy Cardiac Ablation: Technology Is Moving Forward in Complex Procedures—A Novel Workflow for Atrial Fibrillation. Biology, 10(12), 1333. https://doi.org/10.3390/biology10121333