
Digital versus Traditional Workflow for Immediate Loading in Single-Implant Restoration: A Randomized Clinical Trial

 ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients Selection
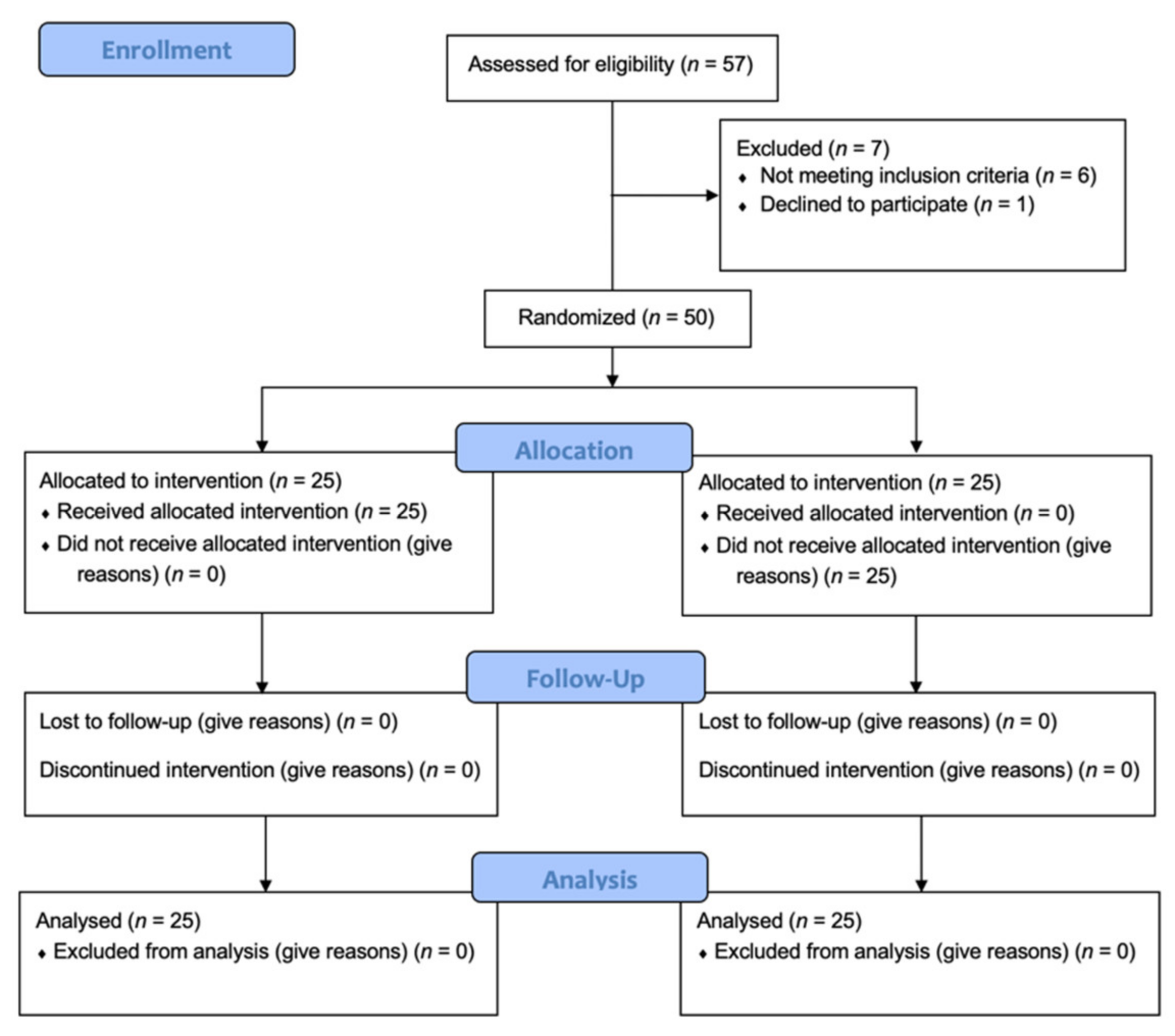
2.2. Sample Size and Randomization of Participants
2.3. Preoperative Evaluation
2.4. Pretreatment
2.5. Post-Extraction Surgical Protocol
2.6. Provisional Restoration
2.7. Post-Surgical Instruction
- -
- 1 g of Amoxicillin 875 mg + Clavulanic acid 125 mg (Augmentin, Glaxo Smith Kline, Brentford, UK) twice a day for a period of five days after the procedure;
- -
- 0.20% chlorhexidine mouthwash (Corsodyl, GlaxoSmithKline, Rixensart, Belgium) rinse two times a day for around one minute for the next 15 days;
- -
- Soft diet for the two months after the surgical;
- -
- The light smokers were remembered to limit and possibly to refrain from smoking.
2.8. Definitive Restoration
2.9. Follow-Up and Measurement of Periodontal Clinical Parameters
- -
- Height of the keratinized mucosa (KM): measured at the exact middle of the vestibular face of the tooth, using a probe, from the mucogingival junction to the coronal margin of the free gingiva;
- -
- Modified plaque index: measured according to the following scale 0 = no plaque; 1 = presence of plaque; four surfaces (distal, mesial, buccal and lingual) were considered, and the average value for each implant was thus calculated.
- -
- Modified bleeding index (mBI): measured by assessing the amount of bleeding by gentle probing on four surfaces (distal, mesial, buccal, and lingual), according to the scale 0 = no bleeding; 1 = presence of bleeding; the average value for each implant was considered;
- -
- Probing depth (PD): the deepest site measured on the four surfaces of the implant (buccal, lingual, mesial, distal) was considered and approximated to the millimeter.
2.10. X-ray Evaluation
2.11. Esthetic Evaluation and Patient Satisfaction
- A.
- The presence/absence of interproximal papilla;
- B.
- The scallop of the gingival margin;
- C.
- The position of the marginal tissue;
- D.
- The color of the marginal tissue;
- E.
- The appearance of the peri-implant tissue.
2.12. Measurement of Key Clinical Study Variables
- -
- Prosthetic failure: prosthesis not positioned due to implant failure.
- -
- Implant failure: any implant removed because of lack of stability, infection or fractured beyond repair.
- -
- Complications or secondary effects of any type, biological and/or prosthetic
- -
- Peri-implant marginal bone level variations measured mesially and distally using the method described in the section “X-ray evaluation”.
- -
- Periodontal clinical parameters: height of the keratinized mucosa (KM), modified Bleeding Index (mBI), modified Plaque Index (mPI), Probing Depth (PD).
2.13. Statistics
3. Results
3.1. Clinical Parameter Evaluation
3.2. Radiographic Parameter Evaluation
3.3. Pes Evaluation
3.4. Patients Satisfaction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Buser, D.; Janner, S.F.M.; Wittneben, J.-G.; Brägger, U.; Ramseier, C.A.; Salvi, G.E. 10-Year Survival and Success Rates of 511 Titanium Implants with a Sandblasted and Acid-Etched Surface: A Retrospective Study in 303 Partially Edentulous Patients. Clin. Implant Dent. Relat. Res. 2012, 14, 839–851. [Google Scholar] [CrossRef] [PubMed]
- Degidi, M.; Nardi, D.; Piattelli, A. 10-Year Follow-Up of Immediately Loaded Implants with TiUnite Porous Anodized Surface. Clin. Implant Dent. Relat. Res. 2012, 14, 828–838. [Google Scholar] [CrossRef] [PubMed]
- Valzania, C.; Torbica, A.; Tarricone, R.; Leyva, F.; Boriani, G. Implant rates of cardiac implantable electrical devices in Europe: A systematic literature review. Health Policy 2016, 120, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Malahias, M.A.; Kostretzis, L.; Greenberg, A.; Nikolaou, V.S.; Atrey, A.; Sculco, P.K. Highly Porous Titanium Acetabular Components in Primary and Revision Total Hip Arthroplasty: A Systematic Review. J. Arthroplast. 2020, 35, 1737–1749. [Google Scholar] [CrossRef]
- Henry, J.; Amoo, M.; Taylor, J.; O’Brien, D.P. Complications of Cranioplasty in Relation to Material: Systematic Review, Network Meta-Analysis and Meta-Regression. Neurosurgery 2021, 89, 383–394. [Google Scholar] [CrossRef]
- Bacci, C.; Zanon, E.; Berengo, M.; Favero, L. Safety of dental implant surgery in patients undergoing anticoagulation therapy: A prospective case-control study. Clin. Oral Implant. Res. 2010, 22, 151–156. [Google Scholar] [CrossRef]
- Gherlone, E.; Capparé, P.; Tecco, S.; Polizzi, E.; Pantaleo, G.; Gastaldi, G.; Grusovin, M.G. Implant Prosthetic Rehabilitation in Controlled HIV-Positive Patients: A Prospective Longitudinal Study with 1-Year Follow-Up. Clin. Implant. Dent. Relat. Res. 2015, 18, 725–734. [Google Scholar] [CrossRef]
- Quiles, J.; Souza, F.; Bassi, A.P.F.; Garcia, I.R., Jr.; França, M.; Carvalho, P. Survival rate of osseointegrated implants in atrophic maxillae grafted with calvarial bone: A retrospective study. Int. J. Oral Maxillofac. Surg. 2015, 44, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Sivolella, S.; Botticelli, D.; Prasad, S.; Ricci, S.; Bressan, E.; Prasad, H. Evaluation and comparison of histologic changes and implant survival in extraction sites immediately grafted with two different xenografts: A randomized clinical pilot study. Clin. Oral Implant. Res. 2020, 31, 825–835. [Google Scholar] [CrossRef]
- Becker, W.; Becker, E.B.; Israelson, H.; Lucchini, J.P.; Handelsman, M.; Ammons, W.; Rosenberg, E.; Rose, L.; Tucker, L.M.; Lekholm, U. One-step surgical placement of Brånemark implants: A prospective multicenter clinical study. Int. J. Oral Maxillofac. Implant. 1997, 12, 454–462. [Google Scholar]
- Aires, I.; Berger, J. Immediate Placement in Extraction Sites Followed by Immediate Loading: A Pilot Study and Case Presentation. Implant Dent. 2002, 11, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Pjetursson, B.E.; Tan, K.; Lang, N.P.; Bragger, U.; Egger, M.; Zwahlen, M. A systematic review of the survival and complication rates of fixed partial dentures (FPDs) after an observation period of at least 5 years. I. Implant-supported FPDs. Clin. Oral Implant. Res. 2004, 15, 625–642. [Google Scholar] [CrossRef] [PubMed]
- Shibly, O.; Kutkut, A.; Patel, N.; Albandar, J.M. Immediate Implants with Immediate Loading vs. Conventional Loading: 1-Year Randomized Clinical Trial. Clin. Implant. Dent. Relat. Res. 2010, 14, 663–671. [Google Scholar] [CrossRef] [PubMed]
- Del Fabbro, M.; Ceresoli, V.; Taschieri, S.; Ceci, C.; Testori, T. Immediate Loading of Postextraction Implants in the Esthetic Area: Systematic Review of the Literature. Clin. Implant. Dent. Relat. Res. 2013, 17, 52–70. [Google Scholar] [CrossRef] [PubMed]
- Donovan, E.T.; Chee, W. A review of contemporary impression materials and techniques. Dent. Clin. 2004, 48, 445–470. [Google Scholar] [CrossRef] [PubMed]
- Ferrini, F.; Sannino, G.; Chiola, C.; Capparé, P.; Gastaldi, G.; Gherlone, E.F. Influence of Intra-Oral Scanner (I.O.S.) on The Marginal Accuracy of CAD/CAM Single Crowns. Int. J. Environ. Res. Public Health 2019, 16, 544. [Google Scholar] [CrossRef] [Green Version]
- Goracci, C.; Franchi, L.; Vichi, A.; Ferrari, M. Accuracy, reliability, and efficiency of intraoral scanners for full-arch impressions: A systematic review of the clinical evidence. Eur. J. Orthod. 2015, 38, 422–428. [Google Scholar] [CrossRef]
- Ting-Shu, S.; Jian, S. Intraoral Digital Impression Technique: A Review. J. Prosthodont. 2014, 24, 313–321. [Google Scholar] [CrossRef]
- Cattoni, F.; Teté, G.; Calloni, A.M.; Manazza, F.; Gastaldi, G.; Capparè, P. Milled versus moulded mock-ups based on the superimposition of 3D meshes from digital oral impressions: A comparative in vitro study in the aesthetic area. BMC Oral Health 2019, 19, 230. [Google Scholar] [CrossRef]
- Yuzbasioglu, E.; Kurt, H.; Turunc, R.; Bilir, H. Comparison of digital and conventional impression techniques: Evaluation of pa-tients’ perception, treatment comfort, effectiveness and clinical outcomes. BMC Oral Health 2014, 14, 10. [Google Scholar] [CrossRef] [Green Version]
- Borgonovo, A.E.; Rigaldo, F.; Battaglia, D.; Re, D.; Giannì, A.B. Digital Device in Postextraction Implantology: A Clinical Case Presentation. Case Rep. Dent. 2014, 2014, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joda, T.; Brägger, U. Digital vs. conventional implant prosthetic workflows: A cost/time analysis. Clin. Oral Implant. Res. 2014, 26, 1430–1435. [Google Scholar] [CrossRef] [PubMed]
- Joda, T.; Brägger, U. Time-Efficiency Analysis Comparing Digital and Conventional Workflows for Implant Crowns: A Pro-spective Clinical Crossover Trial. Int. J. Oral Maxillofac. Implant. 2015, 30, 1047–1053. [Google Scholar] [CrossRef]
- Joda, T.; Zarone, F.; Ferrari, M. The complete digital workflow in fixed prosthodontics: A systematic review. BMC Oral Health 2017, 17, 124. [Google Scholar] [CrossRef] [PubMed]
- Brägger, U.; Joda, T. Complete digital workflow for the production of implant-supported single-unit monolithic crowns. Clin. Oral Implant. Res. 2014, 25, 1304–1306. [Google Scholar]
- Ramsey, C.D.; Ritter, R.G. Utilization of Digital Technologies for Fabrication of Definitive Implant-Supported Restorations. J. Esthet. Restor. Dent. 2011, 24, 299–308. [Google Scholar] [CrossRef]
- Gallardo, Y.R.; Bohner, L.; Tortamano, P.; Pigozzo, M.N.; Laganá, D.C.; Sesma, N. Patient outcomes and procedure working time for digital versus conventional impressions: A systematic review. J. Prosthet. Dent. 2018, 119, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Rattanapanich, P.; Aunmeungtong, W.; Chaijareenont, P.; Khongkhunthian, P. Comparative Study between an Immediate Loading Protocol Using the Digital Workflow and a Conventional Protocol for Dental Implant Treatment: A Randomized Clinical Trial. J. Clin. Med. 2019, 8, 622. [Google Scholar] [CrossRef] [Green Version]
- Polizzi, E.; Tetè, G.; Bova, F.; Capparè, P.; Gherlone, E. Antibacterial properties and side effects of chlorhexidinebased mouthwashes. A prospective, randomized clinical study. J. Osseointegration 2020, 12, 230. [Google Scholar]
- Gherlone, E.; Polizzi, E.; Tetè, G.; Capparè, P. Dentistry and Covid-19 pandemic: Operative indications post-lockdown. New Microbiol. 2020, 44, 1–11. [Google Scholar]
- Mombelli, A.; Lang, N.P. Clinical parameters for the evaluation of dental implants. Periodontology 2000 1994, 4, 81–86. [Google Scholar] [CrossRef]
- Belser, U.C.; Grütter, L.; Vailati, F.; Bornstein, M.M.; Weber, H.-P.; Buser, D. Outcome Evaluation of Early Placed Maxillary Anterior Single-Tooth Implants Using Objective Esthetic Criteria: A Cross-Sectional, Retrospective Study in 45 Patients With a 2- to 4-Year Follow-Up Using Pink and White Esthetic Scores. J. Periodontol. 2009, 80, 140–151. [Google Scholar] [CrossRef] [PubMed]
- Pjetursson, B.E.; Karoussis, I.; Bürgin, W.; Brägger, U.; Lang, N.P. Patients’ satisfaction following implant therapy: A 10-year prospective cohort study. Clin. Oral Implant. Res. 2005, 16, 185–193. [Google Scholar] [CrossRef]
- Araújo, M.G.; Silva, C.; Souza, A.B.; Sukekava, F. Socket healing with and without immediate implant placement. Periodontol. 2000 2019, 79, 168–177. [Google Scholar] [CrossRef] [PubMed]
- Cappare’, P.; Teté, G.; Romanos, G.E.; Nagni, M.; Sannino, G.; Gherlone, E.F. The ’All-on-four’ protocol in HIV-positive patients: A prospective, longitudinal 7-year clinical study. Int. J. Oral. Implantol 2019, 12, 501–510. [Google Scholar]
- Montemezzi, P.; Ferrini, F.; Pantaleo, G.; Gherlone, E.; Capparè, P. Dental Implants with Different Neck Design: A Prospective Clinical Comparative Study with 2-Year Follow-Up. Materials 2020, 13, 1029. [Google Scholar] [CrossRef] [Green Version]
- Wenzel, A. Interproximal Papilla Levels Following Early Versus Delayed Placement of Single-Tooth Implants: A Controlled Clinical Trial. Int. J. Oral Maxillofac. Implant. 2005, 20, 753–761. [Google Scholar]
- Bozkaya, D.; Müftü, S. Mechanics of the tapered interference fit in dental implants. J. Biomech. 2003, 36, 1649–1658. [Google Scholar] [CrossRef] [Green Version]
- Krennmair, G.; Schmidinger, S.; Waldenberger, O. Single-tooth replacement with the Frialit-2 system: A retrospective clinical analysis of 146 implants. Int. J. Oral Maxillofac. Implant. 2002, 17, 78–85. [Google Scholar]
- Gherlone, E.F.; Capparè, P. Evaluation of resistance against bacterial microleakage of a new conical implant-Abutment con-nection versus conventional connections: An in vitro study. New Microbiol. 2016, 39, 59–66. [Google Scholar]
- Quirynen, M.; Bollen, C.M.L.; Eyssen, H.; Van Steenberghe, D. Microbial penetration along the implant components of the Brånemark system®. An in vitro study. Clin. Oral Implant. Res. 1994, 5, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Quirynen, M.; Van Steenberghe, D. Bacterial colonization of the internal part of two-stage implants. An in vivo study. Clin. Oral Implant. Res. 1993, 4, 158–161. [Google Scholar] [CrossRef] [PubMed]
- Dibart, S.; Warbington, M.; Su, M.F.; Skobe, Z. In vitro evaluation of the implant-abutment bacterial seal: The locking taper system. Int. J. Oral Maxillofac. Implant. 2005, 20, 732–737. [Google Scholar] [PubMed]
- Jung, R.E.; Jones, A.A.; Higginbottom, F.L.; Wilson, T.G.; Schoolfield, J.; Buser, D.; Hämmerle, C.H.; Cochran, D.L. The Influence of Non-Matching Implant and Abutment Diameters on Radiographic Crestal Bone Levels in Dogs. J. Periodontol. 2008, 79, 260–270. [Google Scholar] [CrossRef]
- Cochran, D.L.; Bosshardt, D.D.; Grize, L.; Higginbottom, F.L.; Jones, A.A.; Jung, R.E.; Wieland, M.; Dard, M. Bone Response to Loaded Implants with Non-Matching Implant-Abutment Diameters in the Canine Mandible. J. Periodontol. 2009, 80, 609–617. [Google Scholar] [CrossRef] [PubMed]
- Luongo, R.; Traini, T.; Guidone, P.C.; Bianco, G.; Cocchetto, R.; Celletti, R. Hard and soft tissue responses to the platform-switching technique. Int. J. Periodontics Restor. Dent. 2008, 28, 551–557. [Google Scholar]
- Sabbah, A.; Hicks, J.; MacNeill, B.; Arbona, A.; Aguilera, A.; Liu, Q.; Gelfond, J.; Gardner, W. A retrospective analysis of dental implant survival in HIV patients. J. Clin. Periodontol. 2019, 46, 363–372. [Google Scholar] [CrossRef]
- D’Orto, B.; Tetè, G.; Polizzi, E. Osseointegrated dental implants supporting fixed prostheses in patients affected by Sjögren’s Sindrome: A narrative review. J. Biol. Regul. Homeost. Agents 2020, 34, 89–91. [Google Scholar]
- Conti, P.; Caraffa, A.; Tetè, G.; Gallenga, C.E.; Ross, R.; Kritas, S.K.; Frydas, I.; Younes, A.; Di Emidio, P.; Ronconi, G. Mast cells activated by SARS-CoV-2 release histamine which increases IL-1 levels causing cytokine storm and inflammatory reaction in COVID-19. J. Biol. Regul. Homeost. Agents 2020, 34, 1629–1632. [Google Scholar]
- Britain, S.K.; Arnold, R.M.; Lyford, R.H.; Oates, T.W. Clinical and radiographic evaluation of the papilla level adjacent to single-tooth dental implants: A retrospective study in the maxillary anterior region. Implant Dent. 2002, 11, 96. [Google Scholar] [CrossRef]
- Schepke, U.; Meijer, H.J.A.; Kerdijk, W.; Cune, M.S. Digital versus analog complete-arch impressions for single-unit premolar implant crowns: Operating time and patient preference. J. Prosthet. Dent. 2015, 114, 403–406.e1. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| 1. Man/woman | 1. Patients who were pregnant or breastfeeding |
| 2. Age > 18 years | 2. Radiation therapy on the head/neck or chemotherapy in the last five years |
| 3. Good oral hygiene | 3. Poor oral hygiene (Full Mouth Plaque Score (FMPS) and Full Mouth Bleeding Score (FMBS) >20%) and low motivation to maintain correct oral hygiene |
| 4. FMPS and FMBS < 20%; | 4. Chronic abuse of drugs or alcohol |
| 5. Non-smokers or smokers of less than 10 cigarettes/day | 5. Heavy smokers (>10 cigarettes per day) |
| 6. No contraindications to oral surgery (ASA-1/ASA-2) | 6. Compromised medical conditions (ASA score 3 or more) |
| 7. Bone volume and density that would allow for the insertion of an implant with a minimal diameter of 3.0 mm and a minimal length of 8.5 mm | 7. The need for bone increase/bone regeneration procedures for the positioning of an implant |
| 8. No active infections around the surgical site | 8. Limited mouth opening, functional limitations or temporomandibular problems |
| 9. Signing of an informed consent for the protocol | 9. Severe parafunctions (bruxism, clenching) |
| 10. Systemic medical conditions that would contraindicate implant surgery (e.g., uncontrolled diabetes, coagulation problems not adequately treated and psychiatric problems) | |
| 11. Use of oral and/or parenteral bisphosphonates for >3 years | |
| 12. Immunosuppressant therapy |
| Questions |
|---|
| 1. Are you satisfied with the treatment? with 0 = very dissatisfied and 100 = very satisfied |
| 2. Are you pleased with the functional result? with 0 = not pleased and 100 = very much pleased |
| 3.Are you pleased with the final aesthetic result? with 0 = not pleased and 100 = very much pleased |
| 4. Did you experience discomfort during the impression-taking? with 0 = high discomfort and 100 = no discomfort |
| 5. Did you experience gag reflex/nausea during the impression-taking? with 0 = strong gag reflex/nausea, and 100 = no gag reflex/nausea |
| 6. How annoying was the impression procedure? with 0 = very annoying and 100 = not annoying |
| 7. Was the treatment time justified? with 0 = totally not justified and 100 = completely justified |
| 8. Has the dental implant treatment performed as expected? with 0 = absolutely not and 100 = yes |
| 9. Would you repeat this treatment again, if necessary? with 0 = absolutely not and 100 = yes, of course |
| 10. Would you encourage friends or family members to perform the same treatment? with 0 = absolutely not and 100 = Yes, obviously |
| Immediate Loading with Digital Workflow | Immediate Loading with Analogical Workflow | |
|---|---|---|
| Men | 14 | 5 |
| Women | 11 | 20 |
| Overall Patients | 25 | 25 |
| Mean Age | 49.21 ± 9.07 | 41.05 ± 15.73 |
| Inserted Implants | 25 | 25 |
| TG | CG | |||||||
|---|---|---|---|---|---|---|---|---|
| Parameter | Baseline | 3 Months | 6 Months | 12 Months | Baseline | 3 Months | 6 Months | 12 Months |
| mPI | 1.07 ± 0.90 | 0.75 ± 0.70 | 0.89 ± 0.68 | 1.03 ± 0.64 | 0.86 ± 0.93 | 0.46 ± 0.64 | 0.64 ± 0.68 | 0.82 ± 0.77 |
| mBI | 1.14 ± 0.93 | 0.64 ± 0.68 | 0.82 ± 0.81 | 0.96 ± 0.69 | 0.82 ± 1.09 | 0.36 ± 0.49 | 0.57 ± 0.63 | 0.78 ± 0.74 |
| PD (mm) | 2.10 ± 0.87 | 1.97 ± 0.75 | 2.21 ± 0.98 | 2.41 ± 0.89 | 2.23 ± 0.76 | 1.87 ± 0.73 | 2.60 ± 0.65 | 2.95 ± 1.00 |
| KM (MM) | 3.25 ± 1.32 | 2.96 ± 1.17 | 2.68 ± 1.02 | 2.57 ± 0.83 | 3.33 ± 0.69 | 3.07 ± 1.01 | 2.89 ± 0.99 | 3.03 ± 1.03 |
| Source | Dependent Variable | SUM OF Squares | Degrees of Freedom | Mean Square | F | Significance |
|---|---|---|---|---|---|---|
| Type of Technique | KM (mm) | 2.161 | 1 | 2.161 | 0.55 | 0.463 |
| mBI | 3.754 | 1 | 3.754 | 4.832 | 0.032 | |
| mPI | 3.254 | 1 | 3.254 | 2.881 | 0.095 | |
| PD (mm) | 3.135 | 1 | 3.135 | 1.92 | 0.17 | |
| Times | KM (mm) | 6.914 | 1 | 6.914 | 17.52 | <0.001 |
| mBI | 0.044 | 1 | 0.044 | 0.046 | 0.831 | |
| mPI | 0.008 | 1 | 0.008 | 0.014 | 0.906 | |
| PD (mm) | 11.401 | 1 | 11.401 | 20.32 | <0.001 | |
| Interaction Type of Technique by Time | KM (mm) | 1.575 | 1 | 1.575 | 3.99 | 0.05 |
| mBI | 0.151 | 1 | 0.151 | 0.158 | 0.693 | |
| mPI | 0.001 | 1 | 0.001 | 0.002 | 0.969 | |
| PD (mm) | 2.100 | 1 | 2.100 | 3.743 | 0.05 |
| Test Group | Control Group | |
|---|---|---|
| 3 months | 0.04 ± 0.51 mm | 0.32 ± 0.52 mm |
| 6 months | 0.24 ± 0.58 mm | 0.25 ± 0.59 mm |
| 12 months | 0.12 ± 0.66 mm | 0.15 ± 0.54 mm |
| Bone Loss | Mesial | Distal | Mean Bone Loss | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| <0.0 | 10 | 35.71% | 11 | 42.86% | 10 | 35.71% |
| 0.0 a 0.1 | 5 | 17.86% | 4 | 14.29% | 3 | 10.71% |
| 0.1 a 0.5 | 6 | 21.43% | 5 | 17.86% | 6 | 28.57% |
| 0.6 a 1.0 | 3 | 14.29% | 3 | 17.86% | 5 | 21.43% |
| 1.1 a 2.0 | 1 | 10.71% | 2 | 7.14% | 1 | 3.57% |
| >2.0 | 0 | 0% | 0 | 0% | 0 | 0% |
| <0.0 | 12 | 42.86% | 9 | 35.71% | 11 | 39.28% |
| 0.0 a 0.1 | 2 | 7.14% | 3 | 14.29% | 2 | 7.14% |
| 0.1 a 0.5 | 8 | 35.71% | 8 | 32.14% | 6 | 28.57% |
| 0.6 a 1.0 | 0 | 0% | 2 | 7.14% | 4 | 17.86% |
| 1.1 a 2.0 | 3 | 14.29% | 3 | 10.71% | 2 | 7.14% |
| >2.0 | 0 | 0% | 0 | 0% | 0 | 0% |
| Mean Marginal Bone Increase | |
|---|---|
| Test Group | Control Group |
| 0.24 mm | 0.05 mm |
| 0.28 mm | 0.21 mm |
| 0.29 mm | 0.26 mm |
| 0.32 mm | 0.29 mm |
| 0.36 mm | 0.30 mm |
| 0.57 mm | 0.33 mm |
| 0.58 mm | 0.50 mm |
| 0.64 mm | 0.64 mm |
| 0.66 mm | 0.64 mm |
| 0.70 mm | 0.89 mm |
| 1.09 mm | |
| PES Value | Group | Mesial Papilla | Distal Papilla | Scallop of the Soft Tissue Margin | Level of Facial Mucosa | Soft Tissue Color and Texture |
|---|---|---|---|---|---|---|
| Maximum | TG | 2 | 2 | 2 | 2 | 2 |
| CG | 2 | 2 | 2 | 2 | 2 | |
| Minimum | TG | 1 | 1 | 1 | 1 | 0 |
| CG | 1 | 1 | 1 | 1 | 0 | |
| Mean ± SD | TG | 1.54 ± 0.51 | 1.25 ± 0.44 | 1.86 ± 0.36 | 1.86 ± 0.36 | 1.25 ± 0.52 |
| CG | 1.71 ± 0.46 | 1.39 ± 0.50 | 1.75 ± 0.44 | 1.57 ± 0.50 | 1.07 ± 0.60 |
| Questionnaires | Group | Mean + SD | t-Test p Value |
|---|---|---|---|
| Question 1 | TG | 94.32 ± 8.61 | 0.363 |
| CG | 92.02 ± 8.87 | ||
| Question 2 | TG | 93.2 ± 8.01 | 0.59 |
| CG | 92 ± 7.6 | ||
| Question 3 | TG | 95.05 ± 8.56 | 0.161 |
| CG | 91.97 ± 10.32 | ||
| Question 4 | TG | 96.8 ± 6.42 | 0.007 |
| CG | 72.8 ± 16.57 | ||
| Question 5 | TG | 94.76 ± 9.45 | 0.03 |
| CG | 86.34 ± 0.34 | ||
| Question 6 | TG | 97.6 ± 4.3 | 0.005 |
| CG | 69.2 ± 13.8 | ||
| Question 7 | TG | 97.2 ± 7.3 | 0.023 |
| CG | 81.2 ± 11.3 | ||
| Question 8 | TG | 94.99 ± 9.05 | 0.450 |
| CG | 93.11 ± 9.39 | ||
| Question 9 | TG | 91.2 ± 8.8 | 0.73 |
| CG | 90.4 ± 7.3 | ||
| Question 10 | TG | 92.8 ± 7.9 | 0.86 |
| CG | 92.4 ± 8.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Capparé, P.; Ferrini, F.; Ruscica, C.; Pantaleo, G.; Tetè, G.; Gherlone, E.F. Digital versus Traditional Workflow for Immediate Loading in Single-Implant Restoration: A Randomized Clinical Trial. Biology 2021, 10, 1281. https://doi.org/10.3390/biology10121281
Capparé P, Ferrini F, Ruscica C, Pantaleo G, Tetè G, Gherlone EF. Digital versus Traditional Workflow for Immediate Loading in Single-Implant Restoration: A Randomized Clinical Trial. Biology. 2021; 10(12):1281. https://doi.org/10.3390/biology10121281
Chicago/Turabian StyleCapparé, Paolo, Francesco Ferrini, Corrado Ruscica, Giuseppe Pantaleo, Giulia Tetè, and Enrico Felice Gherlone. 2021. "Digital versus Traditional Workflow for Immediate Loading in Single-Implant Restoration: A Randomized Clinical Trial" Biology 10, no. 12: 1281. https://doi.org/10.3390/biology10121281
APA StyleCapparé, P., Ferrini, F., Ruscica, C., Pantaleo, G., Tetè, G., & Gherlone, E. F. (2021). Digital versus Traditional Workflow for Immediate Loading in Single-Implant Restoration: A Randomized Clinical Trial. Biology, 10(12), 1281. https://doi.org/10.3390/biology10121281