1. Introduction
Psoriasis is a recurrent chronic inflammatory disease with scaly, raised and red patches that is autoimmune in nature and multifactorial in character. According to epidemiological statistics, this disease affects 2.5 percent of the world’s population. This chronic illness affects both men and women equally and can strike at any age. It has an annual incidence rate of 50 to 140 new cases per million persons [
1]. Psoriasis is thought to develop as a result of a complicated association between hereditary variables and environmental agents, including cigarette smoke, bacterial infection, oxidative stress, alcohol use and physical trauma. The treatment for psoriasis varies depending on the severity of the illness. Topical medicines are the first-line active therapies for psoriasis, and they are usually adequate to treat mild-to-moderate psoriasis [
2]. Topical agents include coal tar [
3], dithranol [
4], vitamin D analogues, corticosteroids, retinoid, and keratolytic drugs such as salicylic acid [
5]. When the results of topical therapy are inadequate or when the severity of psoriasis prevents the use of topical medicines, phototherapy and systemic therapy may be explored [
6]. The current systemic treatments for psoriasis therapy include biological and non-biological treatment methods that are utilized as monotherapies or in combination regimens to treat mild-to-severe psoriasis [
2]. Since 1972, methotrexate (MTX) has been used as a systemic therapy for moderate-to-severe psoriasis. Psoriasis is conventionally treated orally and parenterally with methotrexate. Because of its cytotoxic, immune-suppressive, and anti-inflammatory properties, the medication appears to provide therapeutic benefits in psoriasis [
7,
8]. Methotrexate is also said to increase cellular adenosine levels, which is thought to be responsible for its anti-inflammatory effects and clinical efficacy in psoriasis treatment.
About 30–90% of methotrexate patients experience side effects, which can range from moderate nausea to severe life-threatening pancytopenia, necessitating a dosage reduction or even the cessation of therapy. Methotrexate toxicity has been observed in the liver, bone marrow, and renal and pulmonary systems [
9]. For the safe use of this medication in psoriasis, the FDA has issued a number of recommendations. Vital functions must be evaluated before commencing methotrexate medication, and monitoring must be performed at regular intervals during treatment, according to these guidelines.
There is a dire need for an efficient topical methotrexate administration method that will decrease systemic side effects associated with the drug. Easy and direct administration to localized psoriatic lesions, the absence of systemic adverse medication responses, application practicality, and non-invasiveness all contribute to the topical therapy being more convenient, resulting in increased patient compliance. As a result, efforts are being made to enhance methotrexate’s topical administration in order to decrease the drug’s systemic adverse effects in psoriasis. Although methotrexate is lipophilic, it is hydro soluble mainly at physiological pH and has a limited potential for passive diffusion through the skin; attempts to administer it topically have failed [
10]. A transdermal matrix film of methotrexate was fabricated utilizing the solvent evaporation method and a blend of hydrophilic (HPMC) and hydrophobic polymer (EC) [
11]. The transdermal flux does not reach the desired value in this case, and experimental data using the psoriatic model are unavailable. The transdermal iontophoretic administration of methotrexate was developed to improve its topical distribution [
12].
To improve skin permeability, oleic-acid-loaded methotrexate deformable liposomes were developed [
13]. It was reported that methotrexate-based nanostructured lipid carriers in conjunction with calcipotriol improve stratum corneum permeability [
14]. However, all of these investigations are restricted to in vitro data, with no consideration given to the impact of these systems on genuine in vivo psoriatic models. Chitosan-decorated niosomal methotrexate gel was developed and tested in psoriatic patients. Because the reduction in the psoriatic area severity index (PASI) obtained was less than 75%, the method cannot be considered clinically effective [
15]. As a result of the current literature, a novel carrier system for the effective topical administration of methotrexate in psoriasis is urgently needed. To achieve therapeutic efficacy without causing systemic toxicity, an optimal topical formulation of methotrexate should be able to offer appropriate skin penetration, as well as efficient drug localization to deep skin layers [
16].
Nanodermatology is without a doubt a growing field of interest and significance, as well as promising a new era in the treatment and management of psoriasis [
17]. The advent of nanoscale techniques allows for a prolonged drug release, while also protecting it against degradation. This is helpful because it maximizes therapeutic efficacy while reducing drug-related toxicities caused by clearance and overdosing. Furthermore, such therapeutical techniques minimize the frequency of medication administration, resulting in greater patient compliance [
18,
19].
Nanoemulsions are one of the techniques that is gaining a lot of interest for improving the skin penetration of hydrophobic drugs [
20]. Nanoemulsions are kinetically stable and isotropic emulsion systems in which a tiny layer of emulsifier stabilizes the oil droplets carrying the medication. Owing to their prolonged physical stability, along with the tiny nanoscale of the droplets, the system can remain distributed without flocculation or coalescence, while also providing better thermodynamic stability. Nanoemulsion formulations are being researched intensively for their potential use as multifunctional nanocarriers in the field of pain and illness [
21]. Nanoemulsions have been shown to improve the dissolution rates and bioavailability of medicines that are poorly water soluble, while reducing adverse effects. The system is suitable for topical administration due to its improved drug solubility, efficient drug loading capacity, superior thermodynamic stability, and permeation-enhancing activity without skin irritation [
22,
23]. However, because nanoemulsions have a low viscosity, they have a lower retentive capacity in the skin, which limits their usage in the pharmaceutical sector [
24]. To overcome this limitation and provide an appropriate topical application, the viscosity must be raised by adding gelling agents such as carbopol 940, xanthan gum, sodium alginate, and so on [
25]. This therapy inhibits the absorption of medication into the bloodstream and increases drug deposition in the skin, allowing for more effective action.
The goal of this study was to create a stable oil-in-water methotrexate-loaded nanoemulsion, which was then converted into a methotrexate nanogel using 1% sodium alginate for the relevant and effective dermal treatment of psoriasis with improved cutaneous methotrexate deposition and an enhanced local effect. Because the topical route of medication administration is less intrusive, simple, and pleasant, the effective use of a dermal preparation containing methotrexate improves patient compliance.
2. Materials and Methods
2.1. Materials
Methotrexate was generously gifted from Wilson Pharmaceuticals, Islamabad. Tween 80, PEG 400 and sodium alginate were purchased from Sigma Aldrich (St. Louis, MO, USA). Triethanolamine was purchased from Merck (Darmstadt, Germany). Olive oil was purchased commercially from the local market (Marhaba Industries, Lahore, Pakistan). All chemicals used in this study were of analytical grade and were used without further purification.
2.2. Animals
Male rabbits (2 ± 0.5 kg) were purchased from the local market to conduct in vitro skin permeation, as well as in vivo studies. Male Sprague Dawley rats (weighing 230 ± 20 g) were purchased from Peshawar University for in vivo antipsoriatic activity analysis. These two different animals were used in two different experiments, as mentioned. The animals were given free access to standard animal food, as well as water. All of the experimental procedures were approved by the Institutional Ethical Committee. Animals were kept apart during topical administration to prevent systemic drug entry by licking each other.
2.3. Preparation of Methotrexate O/W Nanoemulsion
The optimized formulation of methotrexate nanoemulsion (0.25%
w/
w) from our previous study was prepared by means of the high shear homogenization technique [
26]. The homogenizer speed was set at 10,000 rpm for 15 min. Briefly, an oily phase containing olive oil, PEG 400, and methotrexate was magnetically stirred at 700 rpm for 1 h at 70 °C. Similarly, the aqueous phase was generated by continuously stirring Tween 80 into distilled water at 70 °C for 1 h. To achieve the final formulation, the oil phase was introduced drop-by-drop into the aqueous phase. To confirm the phase separation of the produced nanoemulsion, the optimal formulation was sonicated for 15 min before being placed at room temperature to investigate the thermodynamic stability of the nanoemulsion formulation.
2.4. Preparation of Methotrexate Nanoemulsion Gel
The optimized nanoemulsion formulation was distributed in different gel bases to maximize the local skin accumulation of the medication with the least amount of penetration in the blood. For the optimal nanoemulsion gel formulation, various concentrations of sodium alginate (0.5, 1, 1.5, 2 and 2.5%), HPMC K4M (1, 2 and 3%), and HPMC K100 (1, 2 and 3%) were employed as gelling agents. The sodium alginate (1%) gel was chosen for the production of the methotrexate nanoemulsion gel (MTX NEG) based on the physical appearance of a plain gel. The methotrexate-loaded nanoemulsion was combined with a 1% (
w/
w) sodium alginate gel to make a skin-suitable formulation. Briefly, sodium alginate was progressively added to distilled water while agitating continuously at 700 rpm for 2–3 h until a transparent dispersion was formed. To thoroughly hydrate and swell the alginate dispersion, it was left at room temperature for 3 h. The methotrexate-loaded nanoemulsion was combined with slight stirring into the sodium alginate dispersion. Finally, to produce a transparent gel, the mix was neutralized to a pH of 7.0 ± 0.5 by adding triethanolamine (4–5 drops) drop-by-drop. To allow entrapped air to escape, the prepared gel formulation was stored overnight [
27,
28]. For the production of plain methotrexate gel, a similar procedure was used. However, instead of a methotrexate-loaded nanoemulsion, a methotrexate solution (MTX Sol) in PBS (pH 7.4) was mixed into the sodium alginate dispersion.
Table 1 shows the composition of the methotrexate-loaded nanoemulsion gel and the methotrexate plain gel.
2.5. Physico-Chemical and Rheological Characterization of Methotrexate Nanoemulsion Gel
The appearance, clarity, homogeneity, pH, drug content, and rheological properties of the developed methotrexate nanoemulsion gel and methotrexate plain gel were physicochemically analyzed. A visual inspection of gel compositions for clarity, appearance, and homogeneity was performed [
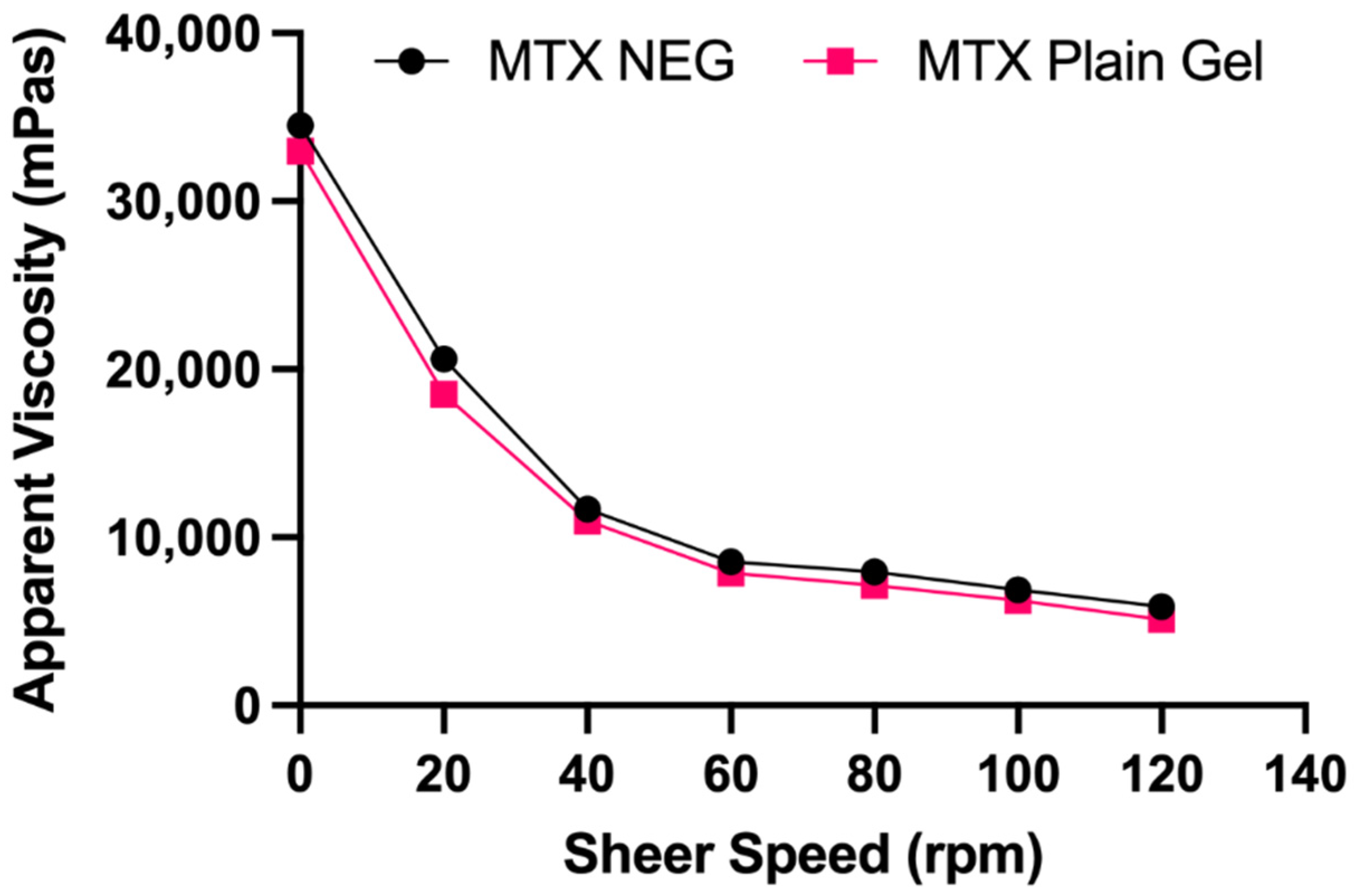
29]. After diluting 1 g of gel in 100 mL of PBS, the concentration of methotrexate in the gel formulations was measured at 303 nm using a UV-Visible spectrophotometer (UV-1601 SCHIMADZU, Japan). To determine the pH of the gel formulation, 1 g of gel was dissolved in 25 mL of distilled water, followed by a pH measurement using a pH meter (Accumet meter 21039, Denver Instruments, USA) at 25 ± 1 °C. For instrument calibration, buffer solutions with known pH (3, 7, and 9) were employed. At room temperature, rheological characteristics of gel formulations were evaluated using a Brookfield viscometer (RVTD, USA) fitted with a UL-adapter [
30]. With a #64 spindle, measurements were taken at a constant (40 rpm) as well as variable (10–120 rpm) shear speeds. The data were fitted to the appropriate rheological model based on the regression coefficient and rheograms of viscosity against shear rate were obtained [
31].
2.6. Determination of Particle Size, Zeta Potential and Polydispersity Index
The zeta sizer Nano ZS 90 was used to determine these three characteristics of formulations of the methotrexate nanoemulsion gel and plain gel (Malvern Instruments, Worcestershire, UK). It comes with software version 6.34 and a laser with a wavelength of 635 nm and a detection angle of 90°. To achieve a homogeneous dispersion, blends of methotrexate gel formulations and deionized water were vortexed for 2 min. At a temperature of 25 ± 0.1 °C, the diluted formulations were examined in triplicates. The final results were given as a mean ± SD [
32].
2.7. Morphology of the Methotrexate Nanoemulsion Gel Formulation
A scanning electron microscope (SEM, JSM 910, JEOL, Japan) was utilized to determine the shape and size of the methotrexate nanoemulsion gel formulation. The aqueous phase was removed from the produced formulation by centrifuging it at 10,000 rpm for 5 min. The sediment was combined with 3 drops of osmium tetra oxide (fixation medium) and maintained at 8 °C for 2 h. The material was diluted using a washing media that included 0.1 M phosphate buffer. The centrifugation and washing procedures were performed twice. Acetone was used to dehydrate the material. In the liquid sample cuvette, an aliquot of the formulation of the methotrexate nanogel was loaded on carbon film with 400 mesh copper grid. Then, at an accelerated voltage of 8.0 kV and a magnification of 10,000×, imaging of the specified sites was performed [
33].
2.8. In Vitro Drug Release Determination
The release behavior of the methotrexate nanogel, plain gel and solution were evaluated using a Franz diffusion cell, employing a Tuffryn membrane at skin pH (5.5). This 0.45-μm pore membrane served as a partitioning medium between the donor and receptor compartments of the Franz diffusion cell (Perme gear, Inc. No: 4G-01-00-15-12; Mumbai, India: diffusion area = 1.767 cm
2). About 7.0 mL of fresh phosphate buffer (pH 5.5), maintained at 32 ± 2 °C was filled into the receptor compartment to mimic skin fluid. At regular intervals, 1 mL samples were taken from the receptor compartment. The same amount of phosphate buffer was substituted to maintain the sink conditions. A UV-Vis spectrophotometer (UV-1601 SHIMADZU, Japan) was used to examine the samples. The mean ± SD of the triplicate results was displayed. The data were plotted as time versus concentration on a graph. The drug release data were analyzed using a power law kinetic model, as indicated in the equation below [
34].
Power Law
where Mt/M
∞ represents a fraction of the drug released after time t, K is the rate constant, and n represents exponential release value.
When n = 0.5, then release occurs through the quasi–Fickian diffusion mechanism. When n > 0.5, then the release mechanism is anomalous, with non-Fickian diffusion, and n = 1 shows a zero-order release mechanism or case II transport.
2.9. In Vitro Skin Permeation of Methotrexate Gel Formulations
The technique outlined in our earlier work was used to accomplish in vitro skin penetration of methotrexate gel formulations [
26]. After being sacrificed via an intravenous injection of sodium phenobarbital ketamine, followed by cervical dislocation, the skin was meticulously removed from the abdomen region of male rabbits (2 ± 0.5 kg). The skin was rigorously cleaned of underlying lipids and connective tissues, then rinsed in saline, wrapped in aluminum foil, and kept at −20 °C until needed. Frozen skin was thawed at room temperature for 30 min before permeation tests.
A Franz diffusion cell (Perme gear, Inc. No: 4G-01-00-15-12; India) was used to conduct in vitro skin permeation investigations. It was equipped with vertical cells, heating circulation, magnetic stirring, as well as temperature control systems. The cell had an effective permeation area (1.77 cm
2) with a receptor cell volume of 7 mL. About 7 mL of PBS (pH 7.4) was added to the receptor compartment, which was constantly stirred at 500 rpm. Throughout the experiment, the temperature of the receptor compartment was kept constant at 37 ± 0.5 °C. Between the donor and receptor compartments of the diffusion cell, rabbit skin was affixed. Under an open hydration procedure and non-occlusive application, the donor compartment was filled with 500 mg of the gel formulation [
35,
36]. At predefined periods (0.5, 1, 2, 4, 8, 12, 16, 20, and 24 h), samples (0.5 mL) were removed from the diffusion cell’s sampling port, and an equivalent volume of new diffusion medium was kept at the same temperature and was immediately introduced to the receptor compartment. The MTX content of the obtained samples was determined using a UV–vis spectrophotometer (UV-1601 SHIMADZU, Hadano, Japan) set at 303 nm. A graph was constructed by plotting the cumulative amount of MTX permeated per unit area versus time period, and flux was determined using the slope of the curve. The magnitude of the formulation flux, as well as the initial MTX concentration in the donor compartment could be employed to calculate the permeability coefficient, whereas the enhancement ratio was generated via the division of the flux value of the MTX nanogel to that of the MTX solution.
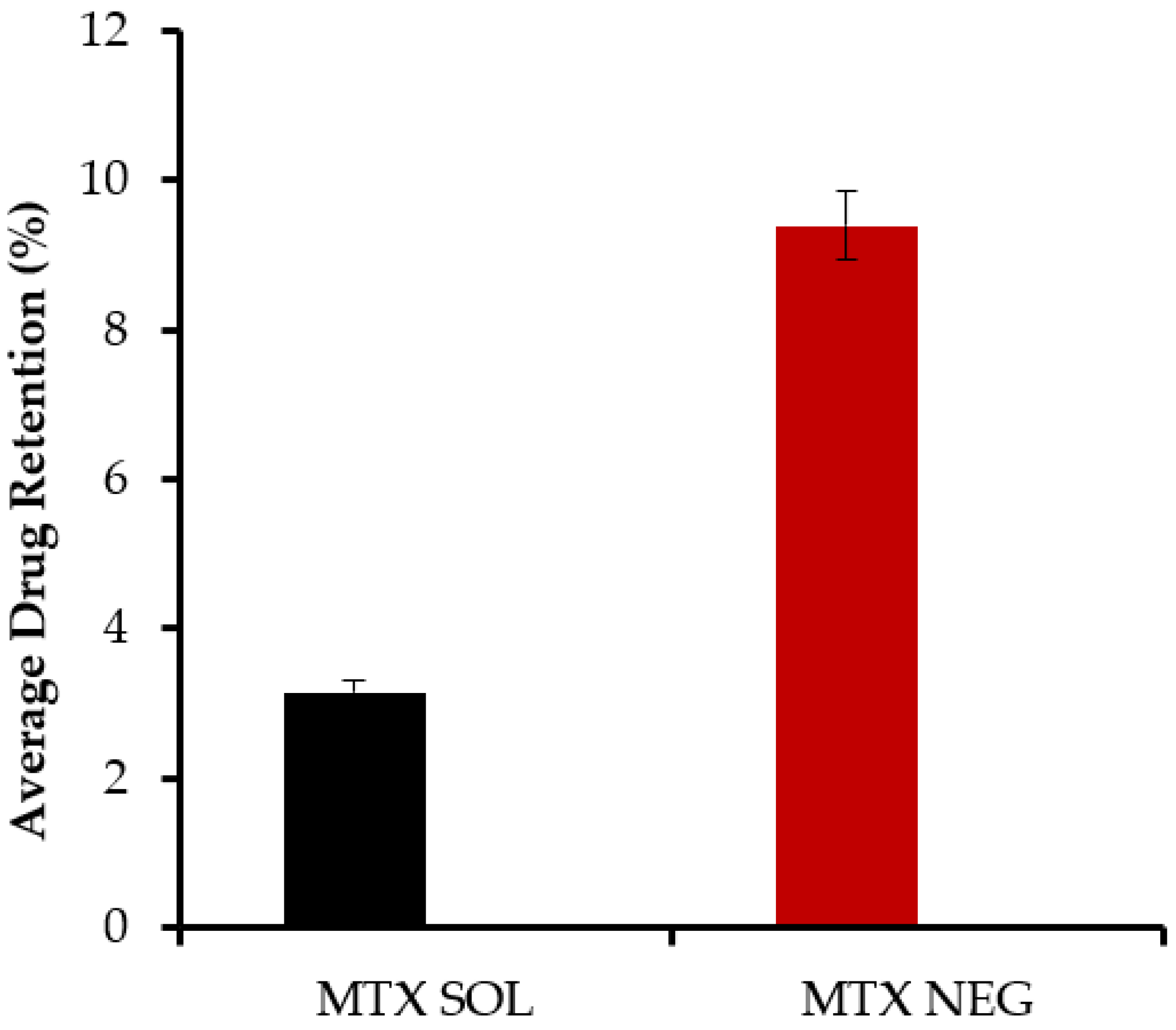
2.10. Skin Drug Retention Analysis
Upon completion of the permeation experiment, the skin mounted in the Franz diffusion cell was meticulously removed. To extract the drug retained, the skin was thoroughly cleaned with phosphate buffer solution. Before cutting it into small pieces (1 cm
2), the skin was tap dried with soft tissue paper and stirred in phosphate buffer solution of pH 7.4 overnight. The samples were then filtered through a 0.45 μm cellulose acetate filter and examined on a UV visible spectrophotometer at a 303 nm wavelength the next day [
37]. The experiment was repeated three times, with the results averaged.
2.11. Mechanism of Drug Retention
With the ultimate goal of increasing methotrexate skin drug accumulation, the skin drug retention mechanism of the improved formulation was investigated using ATR-FTIR on treated skin samples. Briefly, treated skin samples of the nanoemulsion gel, the gel base, as well as the nanoemulsion components, were exposed to vibrational spectroscopic examination by pressing the skin against a zinc selenide crystal to guarantee high sensitivity and intimate contact. Both the epidermis and the dermis were scanned at wave numbers ranging from 675 to 4000 cm−1. The typical peaks were reported. At least three replicates were performed, and the findings were averaged.
2.12. Anti-Psoriatic Activity Studies
We employed an imiquimod (IMQ)-generated psoriatic animal model to test anti-psoriatic effectiveness. A pilot study in our laboratory was used to standardize the model. Male Sprague Dawley rats were split into four groups, as illustrated in
Table 2. The animals were housed in pathogen-free environments and given unrestricted access to food and water. The hair on the animals’ backs was removed using an electric clipper, and the shaved region was treated with 62.5 mg of IMQ (5%) for 7 days to see if psoriatic-type skin lesions developed. Following the onset of psoriasis, IMQ was used occasionally (three days at a three-day interval) for another three weeks in order to maintain psoriasis. The formulations were applied daily to IMQ-treated regions to see if psoriasis improved to evaluate efficacy. The dosage of an oral methotrexate tablet given weekly (MTX tablet) was 5.143 mg/kg (mouse dose equal to 25 mg clinical dose for an average 60 kg human). For delivery, a commercially available tablet of 15 mg dissolved in 30 mL of PBS and delivered through oral gavage tubes in a volume capable of transferring the required dosage. The clinical psoriasis area and severity index (PASI) score measures were used to evaluate the extent of skin irritation and inflammation during the therapy period. The thickening, erythema and scaling of the animal’s skin were evaluated separately on a scale of 0 to 4 for the PASI score determination, where 0, none; 1, minor; 2, moderate; 3, noticeable; 4, severe. During the treatment period, scoring was done every 24 h, and the total PASI was computed [
38,
39]. The percentage reduction in PASI at the end of the trial was compared to PASI on the 7th day and the induction of psoriasis.
2.13. HPLC Analysis of Methotrexate
Methotrexate was quantified using a high-performance liquid chromatography system (Agilent 1269, Agilent Technologies, Santa Clara, CA, USA). A C18 column (4.6 1003.5 mm, Zorbax C18, Agilent, USA) was utilized in the experiment. The mobile phase was made up of a buffer (0.2 M Na2HPO4 and 0.2 M citric acid in a 2:1 ratio) at pH 6.0 and acetonitrile in a 90:10 (
v/
v) ratio. The mobile phase was maintained at a constant flow rate of 1 mL/min at 25 °C. By injecting 20 μL of each sample, all of the samples were examined. The wavelength of the UV detector was adjusted at 303 nm [
1].
2.14. In Vivo Analysis
Healthy male albino rabbits, used as test animals, were purchased from a local market. They were kept at room temperature (25 ± 2 °C) with a relative humidity of 55 ± 5% and were given normal access to food and drink for seven days while acclimating. All animal procedures followed the institution’s ethical norms, as well as international standards. A ketamine-xylazine injection was administered intramuscularly to anesthetize the rabbits. The back was shaved and cleaned with an ethanol swab in an area of around 2–3 cm2.
All of the animals were separated into two groups, each with six animals: group A and group B. Group A (the control group) was given aqueous methotrexate solution, whereas group B (the test group) was given an optimized nanogel formulation. At regular intervals, 0.5 mL of blood was taken and centrifuged to separate plasma. Adding methanol to plasma and vortexing for 10 min precipitated plasma proteins, which were then centrifuged for 30 min at 5000 rpm. The clear supernatant was subjected to filtration, followed by its dissolution in 0.5 mL of HPLC mobile phase (0.2 M Na2HPO4 and 0.2 M citric acid in a 2:1 ratio) at pH 6.0 and acetonitrile in 90:10 (v/v) and evaluated via HPLC for drug contents that were permeated.
An overdose IV injection of sodium pentobarbital was administered to sacrifice the rabbits when the permeation experiment was over. Skin excision into small pieces was performed meticulously, followed by saline washing and tap drying. The skin was swirled in distilled water overnight to remove methotrexate, then filtered and analyzed using HPLC to determine the residual drug concentration [
40].
2.15. Stability Studies
Nanoemulsion gels have the ability to improve the physical and chemical stability of drugs, so formulations of nanoemulsion gels have been subjected to stability testing. In order to determine the stability studies, the formulations were stored under various storage settings. For 90 days, the formulations were kept in the refrigerator (2–8 °C) by sealing in a glass container, at ambient temperature (25 ± 5 °C), and at accelerated temperature (40 °C and 65% RH). After 1, 2, and 3 months, the formulations were examined for any changes in color or clarity, particle size, phase separation, zeta potential, pH, polydispersity index, and drug content [
37].
2.16. Statistical Analysis
All of the tests were carried out in triplicate. The data were presented as mean ± SD. SPSS software version 18 was used to analyze the statistical data (SPSS Inc., Chicago, IL, USA). For statistical analysis, Student’s t-test or ANOVA were employed. A p-value < 0.05 was deemed significant.


 ,
, 









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}