Implementation of the WHO Approved “Tailoring Antimicrobial Resistance Programs (TAP)” Reduces Patients’ Request for Antibiotics


 ,
,
Abstract
1. Introduction
2. Results
2.1. The Characteristics of the Study Subjects
2.2. Effect of TAP Intervention on Antibiotics Request among Study Subjects
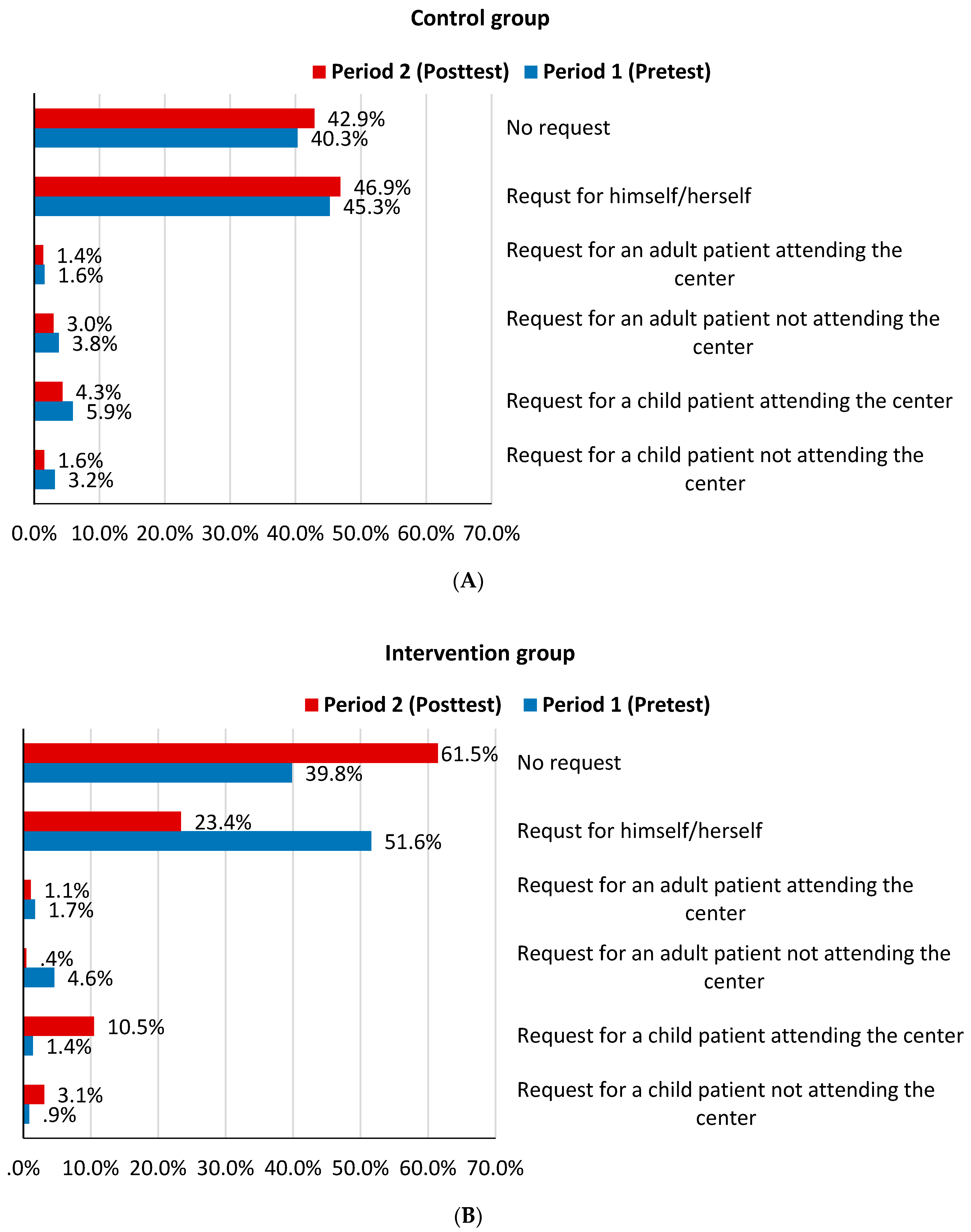
2.3. Pattern of Antibiotics Request
2.4. Reasons for Requesting Antibiotics
2.5. Type of Antibiotics Requested
2.6. Factors that Influence Antibiotics Request
3. Discussion
4. Materials and Methods
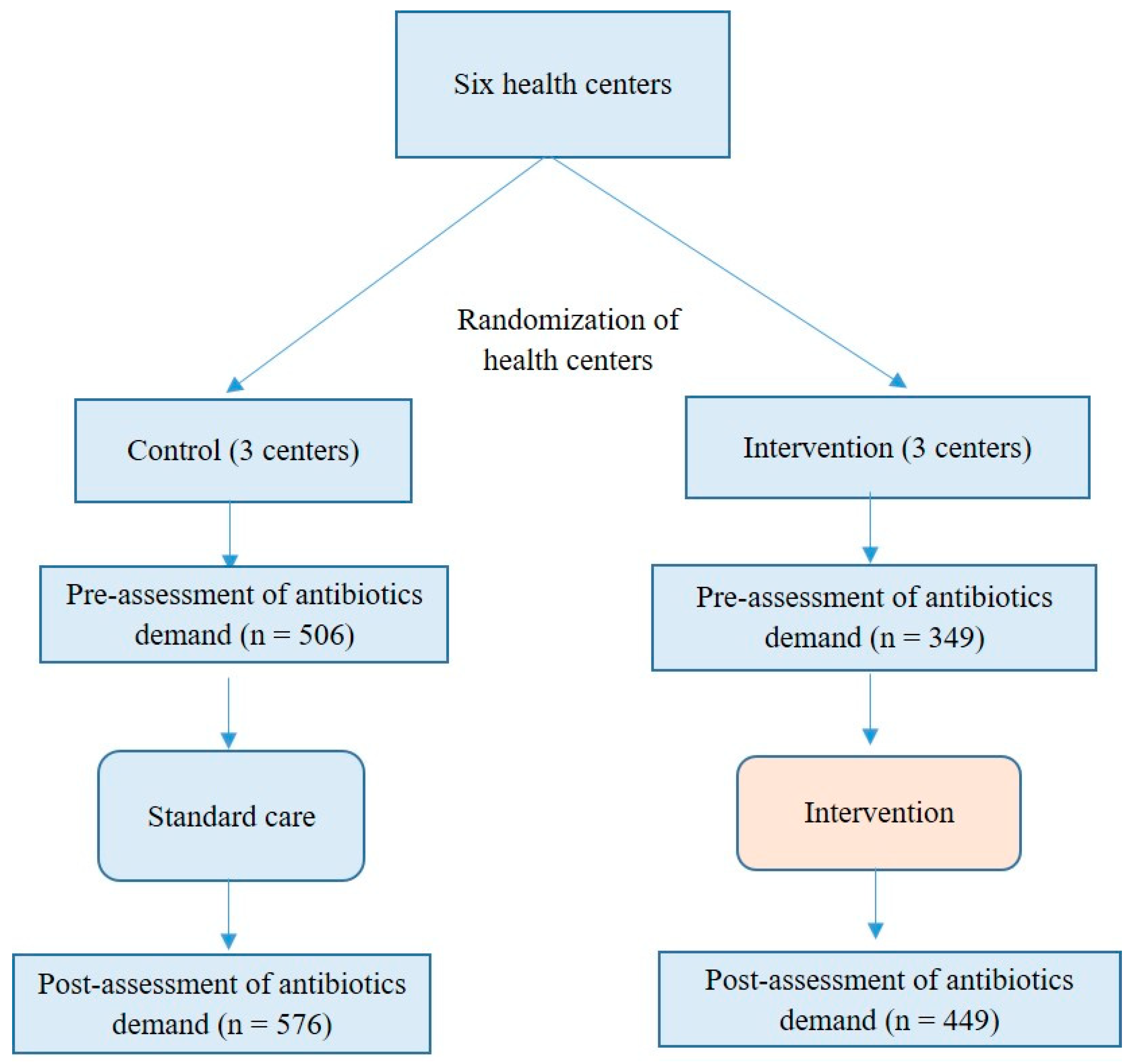
4.1. Study Design, Site Selection and Randomization
4.2. Patient Recruitment
4.3. Intervention
4.4. Sample Size
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| Abbreviation | Full Term |
| TAP | Tailoring Antimicrobial resistance Program |
| URTIs | Upper Respiratory Tract Infections |
| MENA | Middle East and North Africa |
| WHO | World Health Organization |
| EMRO | Eastern Mediterranean Regional Office |
| AMR | Antimicrobial resistance |
| SPSS | Statistical Package for the Social Sciences |
| OR | Odds Ratio |
| CME | Continuing Medical Education |
References
- Wise, R.; Hart, T.; Cars, O.; Streulens, M.; Helmuth, R.; Huovinen, P.; Sprenger, M. Antimicrobial Resistance: Is a major threat to public health. BMJ 1998, 317, 609–610. [Google Scholar] [CrossRef] [PubMed]
- Holmes, A.H.; Moore, L.S.; Sundsfjord, A.; Steinbakk, M.; Regmi, S.; Karkey, A.; Guerin, P.J.; Piddock, L.J. Understanding the mechanisms and drivers of antimicrobial resistance. Lancet 2016, 387, 176–187. [Google Scholar] [CrossRef]
- Laxminarayan, R.; Duse, A.; Wattal, C.; Zaidi, A.K.; Wertheim, H.F.; Sumpradit, N.; Vlieghe, E.; Hara, G.L.; Gould, I.M.; Goossens, H. Antibiotic resistance—the need for global solutions. Lancet Infect. Dis. 2013, 13, 1057–1098. [Google Scholar] [CrossRef]
- Levy, S.B.; Marshall, B. Antibacterial resistance worldwide: Causes, challenges and responses. Nat. Med. 2004, 10, S122–S129. [Google Scholar] [CrossRef] [PubMed]
- Atlanta, G. Antibiotic Resistance Threats in the United States; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2013.
- Harris, A.M.; Hicks, L.A.; Qaseem, A. Appropriate antibiotic use for acute respiratory tract infection in adults. Ann. Intern. Med. 2016, 164, 425–434. [Google Scholar] [CrossRef]
- Abasaeed, A.; Vlcek, J.; Abuelkhair, M.; Kubena, A. Self-medication with antibiotics by the community of Abu Dhabi Emirate, United Arab Emirates. J. Infect. Dev. Ctries. 2009, 3, 491–497. [Google Scholar] [CrossRef]
- Al-Azzam, S.; Al-Husein, B.; Alzoubi, F.; Masadeh, M.; Ali, M. Self-medication with antibiotics in Jordanian population. Int. J. Occup. Med. Environ. Health 2007, 20, 373–380. [Google Scholar] [CrossRef]
- Awad, A.I.; Aboud, E.A. Knowledge, attitude and practice towards antibiotic use among the public in Kuwait. PLoS ONE 2015, 10, e0117910. [Google Scholar] [CrossRef]
- Sabry, N.A.; Farid, S.F.; Dawoud, D.M. Antibiotic dispensing in Egyptian community pharmacies: An observational study. Res. Soc. Adm. Pharm. 2014, 10, 168–184. [Google Scholar] [CrossRef]
- Jamhour, A.; El-Kheir, A.; Salameh, P.; Hanna, P.A.; Mansour, H. Antibiotic knowledge and self-medication practices in a developing country: A cross-sectional study. Am. J. Infect. Control 2017, 45, 384–388. [Google Scholar] [CrossRef]
- Barah, F.; Gonçalves, V. Antibiotic use and knowledge in the community in Kalamoon, Syrian Arab Republic: A cross-sectional study. EMHJ-East. Mediterr. Health J. 2010, 16, 516–521. [Google Scholar] [CrossRef]
- Mouhieddine, T.H.; Olleik, Z.; Itani, M.M.; Kawtharani, S.; Nassar, H.; Hassoun, R.; Houmani, Z.; El Zein, Z.; Fakih, R.; Mortada, I.K. Assessing the Lebanese population for their knowledge, attitudes and practices of antibiotic usage. J. Infect. Public Health 2015, 8, 20–31. [Google Scholar] [CrossRef] [PubMed]
- Darwish, D.A.; Abdelmalek, S.; Dayyih, W.A.; Hamadi, S. Awareness of antibiotic use and antimicrobial resistance in the Iraqi community in Jordan. J. Infect. Dev. Ctries. 2014, 8, 616–623. [Google Scholar] [CrossRef] [PubMed]
- El Zowalaty, M.E.; Belkina, T.; Bahashwan, S.A.; El Zowalaty, A.E.; Tebbens, J.D.; Abdel-Salam, H.A.; Khalil, A.I.; Daghriry, S.I.; Gahtani, M.A.; Madkhaly, F.M. Knowledge, awareness, and attitudes toward antibiotic use and antimicrobial resistance among Saudi population. Int. J. Clin. Pharm. 2016, 38, 1261–1268. [Google Scholar] [CrossRef] [PubMed]
- Taufiq, M.; Zuberi, R.W. Overuse of antibiotics in children for upper respiratory infections (URIs): A Dilemma. J. Coll. Physicians Surg. Pak. 2011, 21, 59–60. [Google Scholar]
- Albsoul-Younes, A.; Wazaify, M.; Yousef, A.-M.; Tahaineh, L. Abuse and misuse of prescription and nonprescription drugs sold in community pharmacies in Jordan. Subst. Use Misuse 2010, 45, 1319–1329. [Google Scholar] [CrossRef]
- Wazaify, M.; Abood, E.; Tahaineh, L.; Albsoul-Younes, A. Jordanian community pharmacists’ experience regarding prescription and nonprescription drug abuse and misuse in Jordan–An update. J. Subst. Use 2017, 22, 463–468. [Google Scholar] [CrossRef]
- Charani, E.; Edwards, R.; Sevdalis, N.; Alexandrou, B.; Sibley, E.; Mullett, D.; Franklin, B.D.; Holmes, A. Behavior change strategies to influence antimicrobial prescribing in acute care: A systematic review. Clin. Infect. Dis. 2011, 53, 651–662. [Google Scholar] [CrossRef]
- Charani, E.; Castro-Sanchez, E.; Sevdalis, N.; Kyratsis, Y.; Drumright, L.; Shah, N.; Holmes, A. Understanding the determinants of antimicrobial prescribing within hospitals: The role of “prescribing etiquette”. Clin. Infect. Dis. 2013, 57, 188–196. [Google Scholar] [CrossRef]
- Rawson, T.M.; Charani, E.; Moore, L.S.P.; Hernandez, B.; Castro-Sánchez, E.; Herrero, P.; Georgiou, P.; Holmes, A.H. Mapping the decision pathways of acute infection management in secondary care among UK medical physicians: A qualitative study. BMC Med. 2016, 14, 208. [Google Scholar] [CrossRef]
- Kandeel, A.; El-Shoubary, W.; Hicks, L.A.; Fattah, M.A.; Dooling, K.L.; Lohiniva, A.L.; Ragab, O.; Galal, R.; Talaat, M. Patient attitudes and beliefs and provider practices regarding antibiotic use for acute respiratory tract infections in Minya, Egypt. Antibiotics 2014, 3, 632–644. [Google Scholar] [CrossRef] [PubMed]
- Dooling, K.L.; Kandeel, A.; Hicks, L.A.; El-Shoubary, W.; Fawzi, K.; Kandeel, Y.; Etman, A.; Lohiniva, A.L.; Talaat, M. Understanding antibiotic use in Minya District, Egypt: Physician and pharmacist prescribing and the factors influencing their practices. Antibiotics 2014, 3, 233–243. [Google Scholar] [CrossRef] [PubMed]
- Joseph, H.A.; Agboatwalla, M.; Hurd, J.; Jacobs-Slifka, K.; Pitz, A.; Bowen, A. What Happens When “Germs Don’t Get Killed and They Attack Again and Again”: Perceptions of Antimicrobial Resistance in the Context of Diarrheal Disease Treatment Among Laypersons and Health-Care Providers in Karachi, Pakistan. Am. J. Trop. Med. Hyg. 2016, 95, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Shahid, A.; Iftikhar, F.; Arshad, M.K.; Javed, Z.; Sufyan, M.; Ghuman, R.S.; Tarar, Z. Knowledge and attitude of physicians about antimicrobial resistance and their prescribing practices in Services Hospital, Lahore, Pakistan. JPMA J. Pak. Med Assoc. 2017, 67, 968. [Google Scholar] [PubMed]
- Bush, K.; Courvalin, P.; Dantas, G.; Davies, J.; Eisenstein, B.; Huovinen, P.; Jacoby, G.A.; Kishony, R.; Kreiswirth, B.N.; Kutter, E. Tackling antibiotic resistance. Nat. Rev. Microbiol. 2011, 9, 894–896. [Google Scholar] [CrossRef] [PubMed]
- Monto, A.S. Epidemiology of viral respiratory infections. Am. J. Med. 2002, 112, 4–12. [Google Scholar] [CrossRef]
- Nyquist, A.-C.; Gonzales, R.; Steiner, J.F.; Sande, M.A. Antibiotic prescribing for children with colds, upper respiratory tract infections, and bronchitis. JAMA 1998, 279, 875–877. [Google Scholar] [CrossRef]
- Gonzales, R.; Steiner, J.F.; Sande, M.A. Antibiotic prescribing for adults with colds, upper respiratory tract infections, and bronchitis by ambulatory care physicians. JAMA 1997, 278, 901–904. [Google Scholar] [CrossRef]
- Fletcher-Lartey, S.; Yee, M.; Gaarslev, C.; Khan, R. Why do general practitioners prescribe antibiotics for upper respiratory tract infections to meet patient expectations: A mixed methods study. BMJ Open 2016, 6, e012244. [Google Scholar] [CrossRef]
- Hamm, R.M.; Hicks, R.J.; Bemben, D. Antibiotics and respiratory infections: Are patients more satisfied when expectations are met? J. Fam. Pract. 1996, 43, 56–62. [Google Scholar]
- Morgan, E.R.; Winter, R.J. Teaching communication skills: An essential part of residency training. Arch. Pediatrics Adolesc. Med. 1996, 150, 638–642. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Little, P.; Britten, N. Why do general practitioners prescribe antibiotics for sore throat? Grounded theory interview study. BMJ 2003, 326, 138. [Google Scholar] [PubMed]
- Biezen, R.; Brijnath, B.; Grando, D.; Mazza, D. Management of respiratory tract infections in young children—A qualitative study of primary care providers’ perspectives. NPJ Prim. Care Respir. Med. 2017, 27, 1–7. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Period 1 (Pretest) | Period 2 (Posttest) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Control Group | Intervention Group | p-value | Control Group | Intervention Group | p-value | ||||
| n | % | n | % | n | % | n | % | |||
| Gender | 0.666 | 0.488 | ||||||||
| Male | 297 | 58.7 | 210 | 60.2 | 369 | 64.1 | 297 | 66.1 | ||
| Female | 209 | 41.3 | 139 | 39.8 | 207 | 35.9 | 152 | 33.9 | ||
| Age | <0.001 | 0.320 | ||||||||
| Children (<18 year) | 90 | 17.8 | 25 | 7.2 | 142 | 24.7 | 123 | 27.4 | ||
| Adults (≥18 year) | 416 | 82.2 | 324 | 92.8 | 434 | 75.3 | 326 | 72.6 | ||
| Nationality | ||||||||||
| Jordanian | 475 | 93.9 | 332 | 95.1 | 558 | 96.9 | 427 | 95.1 | ||
| Non-Jordanian | 31 | 6.1 | 17 | 4.9 | 18 | 3.1 | 22 | 4.9 | ||
| Education | <0.001 | <0.001 | ||||||||
| No formal education | 72 | 14.2 | 43 | 12.3 | 68 | 11.8 | 60 | 13.4 | ||
| Primary education | 84 | 16.6 | 98 | 28.1 | 106 | 18.4 | 141 | 31.4 | ||
| Secondary education | 155 | 30.6 | 114 | 32.7 | 161 | 28 | 151 | 33.6 | ||
| Professional training | 35 | 6.9 | 16 | 4.6 | 20 | 3.5 | 3 | 0.7 | ||
| College/University education | 160 | 31.6 | 78 | 22.3 | 221 | 38.4 | 94 | 20.9 | ||
| Marital status | <0.001 | 0.158 | ||||||||
| Married | 332 | 65.6 | 265 | 75.9 | 359 | 62.3 | 284 | 63.3 | ||
| Single | 60 | 11.9 | 30 | 8.6 | 43 | 7.5 | 29 | 6.5 | ||
| Divorced/Widow | 24 | 4.7 | 29 | 8.3 | 32 | 5.6 | 13 | 2.9 | ||
| Children | 90 | 17.8 | 25 | 7.2 | 142 | 24.7 | 123 | 27.4 | ||
| Patient’s type | <0.001 | 0.606 | ||||||||
| New | 283 | 55.9 | 115 | 33 | 298 | 51.7 | 225 | 50.1 | ||
| Regular | 223 | 44.1 | 234 | 67 | 278 | 48.3 | 224 | 49.9 | ||
| Complaint | Control | Intervention | ||||||
|---|---|---|---|---|---|---|---|---|
| Period 1 (Pretest) | Period 2 (Posttest) | Period 1 (Pretest) | Period 2 (Posttest) | |||||
| n | % | n | % | n | % | n | % | |
| Sore Throat | 104 | 34.4 | 118 | 35.9 | 103 | 49.0 | 56 | 32.4 |
| Flu | 67 | 22.2 | 64 | 19.5 | 33 | 15.7 | 32 | 18.5 |
| Cough | 84 | 27.8 | 119 | 36.2 | 34 | 16.2 | 42 | 24.3 |
| Pain on swallowing | 39 | 12.9 | 50 | 15.3 | 40 | 19.0 | 42 | 24.3 |
| Cold | 31 | 10.3 | 21 | 6.4 | 8 | 3.8 | 27 | 15.6 |
| Influenza | 61 | 20.2 | 62 | 18.8 | 27 | 12.9 | 40 | 23.1 |
| Fever | 58 | 19.2 | 50 | 15.2 | 16 | 7.6 | 49 | 28.3 |
| Nasal Congestion | 42 | 13.9 | 30 | 9.1 | 18 | 8.6 | 14 | 8.1 |
| Breathing Difficulties | 33 | 10.9 | 59 | 17.9 | 11 | 5.2 | 12 | 6.9 |
| Nasal secretion | 34 | 11.3 | 24 | 7.3 | 11 | 5.3 | 9 | 5.2 |
| Sneezing | 27 | 8.9 | 22 | 6.7 | 5 | 2.4 | 7 | 4.0 |
| Weakness | 16 | 5.3 | 14 | 4.3 | 14 | 6.7 | 8 | 4.6 |
| Variable | Control Group | Intervention Group | ||||||
|---|---|---|---|---|---|---|---|---|
| OR | 95% Confidence Interval | p-Value | OR | 95% Confidence Interval | p-Value | |||
| Time (post vs. pre) | 1.0 | 0.8 | 1.4 | 0.713 | 0.4 | 0.3 | 0.6 | <0.001 |
| Specialty of health care provider | ||||||||
| General practitioner | 1 | 1 | ||||||
| Family Medicine | 0.5 | 0.4 | 0.7 | <0.001 | 1.2 | 0.8 | 1.6 | 0.366 |
| Pediatrics | 1.1 | 0.8 | 1.7 | 0.519 | 1.0 | 0.6 | 1.6 | 0.927 |
| Internal Medicine | 0.9 | 0.5 | 1.7 | 0.792 | ||||
| Education | ||||||||
| No formal education | 2.9 | 1.9 | 4.5 | <0.001 | 1.0 | 0.6 | 1.7 | 0.968 |
| Primary education | 2.3 | 1.6 | 3.3 | <0.001 | 1.8 | 1.1 | 2.7 | 0.010 |
| Secondary education | 1.7 | 1.3 | 2.4 | 0.001 | 1.9 | 1.3 | 2.8 | 0.002 |
| Professional training | 5.7 | 2.8 | 11.6 | <0.001 | 0.8 | 0.3 | 2.3 | 0.74 |
| College/university education | 1 | |||||||
| Age of patient (adults vs. children) | 1.7 | 1.1 | 2.5 | 0.006 | 1.3 | 0.8 | 2.1 | 0.229 |
| Type of patient (regular vs. new) | 2.5 | 1.9 | 3.3 | <0.001 | 1.2 | 0.9 | 1.7 | 0.153 |
| Behavioral Barrier | Behavioral Domain | Intervention Function | Intervention | Activities | |||||
|---|---|---|---|---|---|---|---|---|---|
| Behavioral change strategies and activities for prescribers | |||||||||
| 1 | Limited communication skills to manage patient pressure of antibiotics for viral infections | Skills | Physical capability | To improve counselling and negotiation skills of doctor to better manage patient demand for antibiotics for viral infections | A training workshop for communication skills | ||||
| 2 | Limited knowledge of guidelines and alternative treatments for viral infections | Knowledge | Psychological capability | To increase doctors’ knowledge of guidelines and alternatives to antibiotics | A prescriber reference booklet including national guidelines for viral Upper Respiratory Tract Infections (URTIs) | ||||
| 3 | Social norms: patient culture of demanding antibiotics and expecting to best know the suitable treatment for self and family. | Social | Social opportunity | To emphasize the professional role of doctors as the best one to diagnose illness and prescribe antibiotics | A conversation/quiz with patients Commitment board | ||||
| 4 | Peer pressure to prescribe antibiotics for viral infections | Professional role | Reflective motivation | To strengthen the bonds between colleagues and managers as one entity that reduced unnecessary use of antibiotics | Peer to peer weekly coffee session | ||||
| Behavioral change strategies and activities for patients | |||||||||
| 1 | Limited knowledge of proper use of antibiotics and Antimicrobial Resistance (AMR) | Knowledge | Psychological capability | To raise knowledge about antibiotics and AMR | A quiz during patient consultation | ||||
| 2 | Limited knowledge that antibiotics are not a solution for viral infections | Knowledge | To raise awareness about alternative therapies | A quiz during patient consultation | |||||
| 3 | Limited understanding of the consequences of improper use of antibiotics | Belief in consequences | Reflective motivation | To label families who do not consume antibiotics for viral infections as healthy and wealthy families | A quiz during patient consultation Poster | ||||
| 4 | Social norms linked with beliefs that people know which antibiotics work best for them | Social | Social environment | To emphasize doctors’ role as the best to diagnose patients following the Arabic proverb “give the bread to the baker”. | A quiz during patient consultation Poster: Never demand antibiotics from your doctor. Always consult your doctor before taking antibiotics | ||||
| 5 | No plans to change behavior | Intentions/goals | To encourage change in social norms by using people who do not use antibiotics as a reference group | Commitment board | |||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaplan, N.M.; Khader, Y.S.; Alfaqih, M.A.; Saadeh, R.; Al Sawalha, L. Implementation of the WHO Approved “Tailoring Antimicrobial Resistance Programs (TAP)” Reduces Patients’ Request for Antibiotics. Antibiotics 2020, 9, 507. https://doi.org/10.3390/antibiotics9080507
Kaplan NM, Khader YS, Alfaqih MA, Saadeh R, Al Sawalha L. Implementation of the WHO Approved “Tailoring Antimicrobial Resistance Programs (TAP)” Reduces Patients’ Request for Antibiotics. Antibiotics. 2020; 9(8):507. https://doi.org/10.3390/antibiotics9080507
Chicago/Turabian StyleKaplan, Nasser M., Yousef S. Khader, Mahmoud A. Alfaqih, Rami Saadeh, and Lora Al Sawalha. 2020. "Implementation of the WHO Approved “Tailoring Antimicrobial Resistance Programs (TAP)” Reduces Patients’ Request for Antibiotics" Antibiotics 9, no. 8: 507. https://doi.org/10.3390/antibiotics9080507
APA StyleKaplan, N. M., Khader, Y. S., Alfaqih, M. A., Saadeh, R., & Al Sawalha, L. (2020). Implementation of the WHO Approved “Tailoring Antimicrobial Resistance Programs (TAP)” Reduces Patients’ Request for Antibiotics. Antibiotics, 9(8), 507. https://doi.org/10.3390/antibiotics9080507