Non-Tuberculous Mycobacteria in Respiratory Specimens of Patients with Obstructive Lung Diseases—Colonization or Disease?



Abstract
1. Introduction
2. Results
3. Discussion
4. Materials and Methods
Author Contributions
Funding
Conflicts of Interest
References
- Cowman, S.; van Ingen, J.; Griffith, D.E.; Loebinger, M.R. Non-Tuberculous mycobacterial pulmonary disease. Eur. Respir. J. 2019, 54, 1900250. [Google Scholar] [CrossRef] [PubMed]
- Haworth, C.S.; Banks, J.; Capstick, T.; Fisher, A.J.; Gorsuch, T.; Laurenson, I.F.; Leitch, A.; Loebinger, M.R.; Milburn, H.J.; Nightingale, M.; et al. British Thoracic Society guidelines for the management of non-tuberculous mycobacterial pulmonary disease (NTM-PD). Thorax 2017, 72 (Suppl. 2), ii1–ii64. [Google Scholar] [CrossRef] [PubMed]
- Donohue, M.J. Increasing nontuberculous mycobacteria reporting rates and species diversity identified in clinical laboratory reports. BMC Infect. Dis. 2018, 18, 163. [Google Scholar] [CrossRef] [PubMed]
- Shah, N.M.; Davidson, J.A.; Anderson, L.F.; Lalor, M.K.; Kim, J.; Thomas, H.L.; Lipman, M.; Abubakar, I. Pulmonary Mycobacterium avium-intracellulare is the main driver of the rise in non-tuberculous mycobacteria incidence in England, Wales and Northern Ireland 2007–2012. BMC Infect. Dis. 2016, 16, 195. [Google Scholar] [CrossRef] [PubMed]
- Van Ingen, J.; Hoefsloot, W.; Dekhuijzen, P.N.R.; Boeree, M.J.; van Soolingen, D. The changing pattern of clinical Mycobacterium avium isolation in Netherlands. Int. J. Tuberc. Lung Dis. 2010, 14, 1176–1180. [Google Scholar]
- Ringshausen, F.C.; Wagner, D.; de Roux, A.; Diel, R.; Hohmann, D.; Hickstein, L.; Welte, T.; Rademacher, J. Prevalence of non-tuberculous mycobacterial pulmonary disease, Germany 2009–2014. Emerg. Infect. Dis. 2016, 22, 1102–1105. [Google Scholar] [CrossRef]
- Prevots, D.R.; Loddenkemper, R.; Sotgiu, G.; Migliori, G.B. Nontuberculous mycobacterial pulmonary disease: An increasing burden with substantial costs. Eur. Respir. J. 2017, 49, 1700374. [Google Scholar] [CrossRef]
- Izumi, K.; Morimoto, K.; Hasegawa, N.; Uchimura, K.; Kawatsu, L.; Ato, M.; Mitarai, S. Epidemiology of adults and children treated for nontuberculous mycobacterial pulmonary disease in Japan. Ann. Am. Thorac. Soc. 2019, 16, 341–347. [Google Scholar] [CrossRef]
- Andrejak, C.; Nielsen, R.; Thomson, R.; Dahaut, P.; Sorensen, H.T.; Thomsen, R.W. Chronic respiratory disease, inhaled corticosteroids and risk of non-tuberculosis mycobacteriosis. Thorax 2013, 68, 256–262. [Google Scholar] [CrossRef]
- Griffith, D.E.; Aksamit, T.; Brown-Elliott, B.A.; Catanzaro, A.; Daley, C.; Gordin, F.; Holland, S.M.; Horsburgh, R.; Huitt, G.; Iademarco, M.F.; et al. An official ATS/IDSA statement: Diagnosis, treatment and prevention of nontuberculous mycobacterial diseases. Am. J. Respir. Crit. Care Med. 2007, 175, 367–416. [Google Scholar] [CrossRef]
- Gatheral, T.; Kumar, N.; Sansom, B.; Lai, D.; Nair, A.; Vlahos, I.; Baker, E. COPD-Related bronchiectasis; independent impact on disease course and outcomes. COPD 2014, 11, 605–614. [Google Scholar] [CrossRef]
- Brode, S.K.; Campitelli, M.A.; Kwong, J.C.; Lu, H.; Marchand-Austin, A.; Gershon, A.S.; Jamieson, F.B.; Marras, T.K. The risk of mycobacterial infections associated with inhaled corticosteroid use. Eur. Respir. J. 2017, 50, 1700037. [Google Scholar] [CrossRef]
- Pyarali, F.F.; Schweitzer, M.; Bagley, V.; Salamo, O.; Guerrero, A.; Sharifi, A.; Campos, M.; Quartin, A.; Mirsaeidi, M. Increasing non-tuberculous mycobacteria infections in veterans with COPD and association with increased risk of mortality. Front. Med. 2018, 5, 311. [Google Scholar] [CrossRef] [PubMed]
- Liu, V.X.; Winthrop, K.L.; Lu, Y.; Sharifi, H.; Nasiri, H.U.; Ruoss, S.J. Association between inhaled corticosteroids use and pulmonary nontuberculous mycobacterial infection. Ann. Am. Thorac. Soc. 2018, 15, 1169–1176. [Google Scholar] [CrossRef] [PubMed]
- Burkes, R.; Donohue, J.F. An update on the Global Initiative for Chronic obstructive Lung Disease 2017 Guidelines with a focus on classification and management of stable COPD. Respir. Care 2018, 63, 749–758. [Google Scholar] [CrossRef]
- Huang, C.-T.; Tsai, Y.-J.; Wu, H.-D.; Wang, J.-Y.; Yu, C.-J.; Lee, L.-N.; Yang, P.-C. Impact of nontuberculous mycobacteria on pulmonary function decline in chronic obstructive pulmonary disease. Int. J. Tuberc. Lung Dis. 2012, 16, 539–545. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.A.; Kim, S.; Jo, K.-W.; Shim, T.S. Natural history of Mycobacterium avium complex lung disease in untreated patients with stable course. Eur. Respir. J. 2017, 49, 1600537. [Google Scholar] [CrossRef] [PubMed]
- Szturmowicz, M.; Siemion-Szcześniak, I.; Wyrostkiewicz, D.; Klatt, M.; Brzezińska, S.; Zabost, A.; Lewandowska, A.; Filipczak, D.; Oniszh, K.; Skoczylas, A.; et al. Factors predisposing to non-tuberculous mycobacterial lung disease in the patients with respiratory isolates of non-tuberculous mycobacteria. Adv. Respir. Med. 2018, 86, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Adzic-Vukicevic, T.; Barac, A.; Blanka-Protic, A.; Laban-Lazovic, M.; Lukovic, B.; Škodrić-Trifunović, V.; Rubino, S. Clinical features of infection caused by non-tuberculous mycobacteria: 7 years’ experience. Infection 2018, 46, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Bakula, Z.; Kościuch, J.; Safianowska, A.; Proboszcz, M.; Bielecki, J.; Van Ingen, J.; Krenke, R.; Jagielski, T. Clinical, radiological and molecular features of Mycobacterium kansasii pulmonary disease. Respir. Med. 2018, 139, 91–100. [Google Scholar] [CrossRef]
- Jones, M.; Winthrop, K.L.; Nelson, S.D.; Duvall, S.L.; Patterson, O.V.; Nechodom, K.E.; Findley, K.E.; Radonovich, L.J.; Samore, M.H.; Fennelly, K.P. Epidemiology of nontuberculous mycobacterial infections in the U.S. Veterans Health Administration. PLoS ONE 2018, 13, e0197976. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018; Available online: https://www.R-project.org/ (accessed on 24 April 2020).



{kind=link}
{kind=link}
| Factor | Total Population No. 36 | NTM-LD No. 17 | Colonization No. 19 | p |
|---|---|---|---|---|
| Gender Males/Females | 15/21 | 7/10 | 8/11 | 0.95 |
| Age, mean (SD) | 65, 9 (11,6) | 65, 2 (11,1) | 66, 3 (12,2) | 0.85 |
| BMI, mean (SD) | 24, 5 (4,8) | 21, 9 (3,8) | 26, 8 (4,5) | 0.001 |
| ≤22.5 No (%) | 14 (39) | 10 (59) | 4 (21) | 0.04 |
| Smoking/pack-years median (range) | 20 (0–80) | 25 (0–50) | 20 (0–80) | 0.22 |
| Inhaled CS No. (%) | 25 (69) | 12 (71) | 13 (68) | 0.82 |
| Oral CS No. (%) | 5 (14) | 2 (12) | 3 (16) | 0.89 |
| Spirometry (median, range) | ||||
| FEV1%/FVC | 0.51 (0.3–0.86) | 0.45 (0.3–0.75) | 0.56 (0.41–0.86) | 0.09 |
| FEV1% pred. | 50 (22–123) | 45 (22–123) | 57 (34–110) | 0.41 |
| FVC% pred. | 77.5 (49–129) | (52–129) | (49–106) | 0.48 |
| Weight loss > 5% No (%) | 6 (17) | 4 (24) | 2 (11) | 0.38 |
| Elevated body temperature (>38 °C) No. (%) | 11 (31) | 9 (53) | 2 (11) | 0.02 |
| Dyspnea No. (%) | 26 (72) | 13 (77) | 13 (68) | 0.87 |
| Haemoptysis No. (%) | 8 (22) | 4 (24) | 4 (21) | 0.82 |
| Expectoration No. (%) | 17 (47) | 7 (41) | 10 (53) | 0.72 |
| Bronchiectasis No. (%) | 16 (44) | 7 (41) | 11 (58) | 0.5 |
| Hypothyreosis No. (%) | 7 (19) | 3 (18) | 4 (21) | 0.87 |
| Past neoplastic disease No. (%) | 6 (17) | 4 (24) | 2 (11) | 0.55 |
| Diabetes No. (%) | 6 (17) | 5 (29) | 1 (5) | 0.14 |
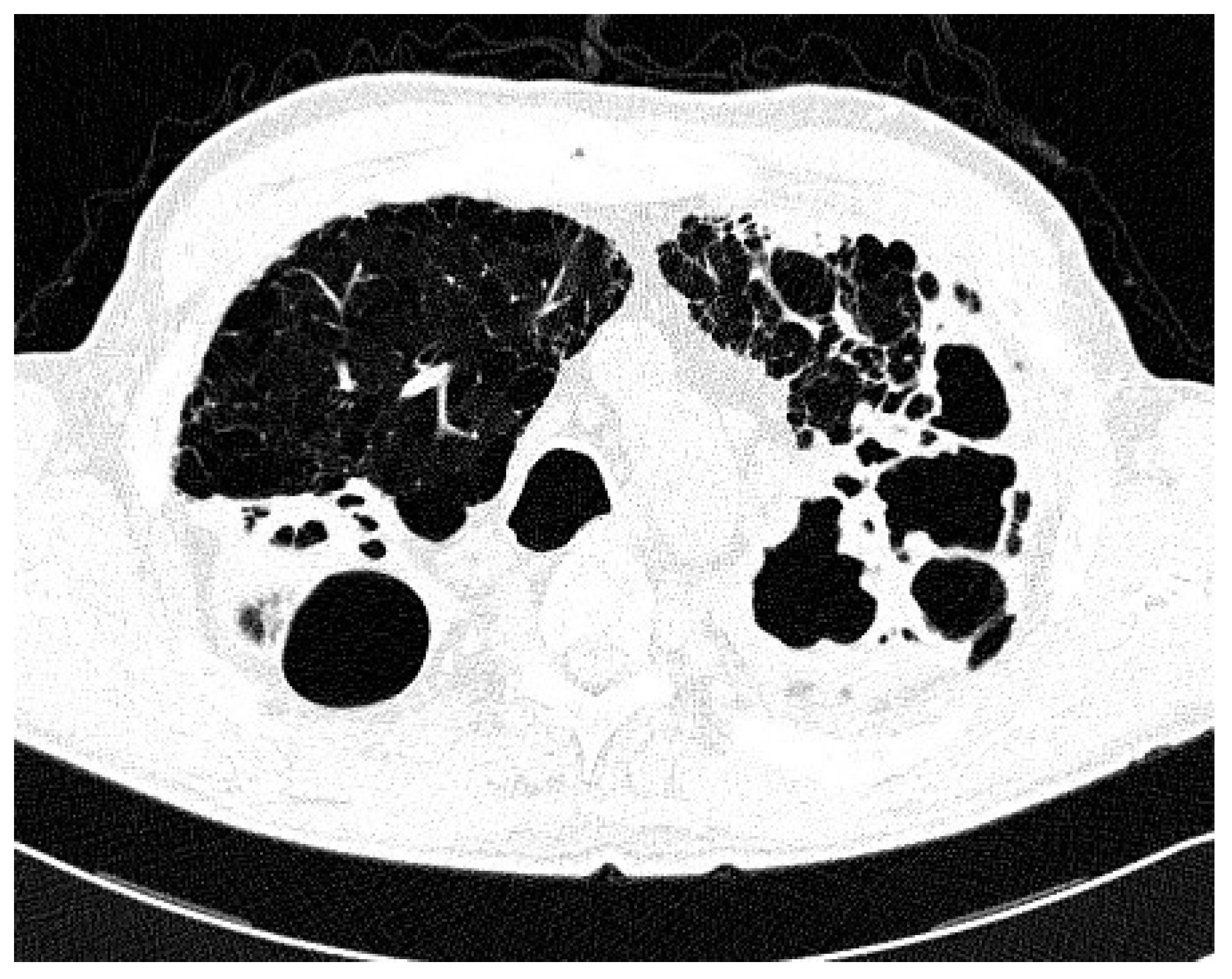
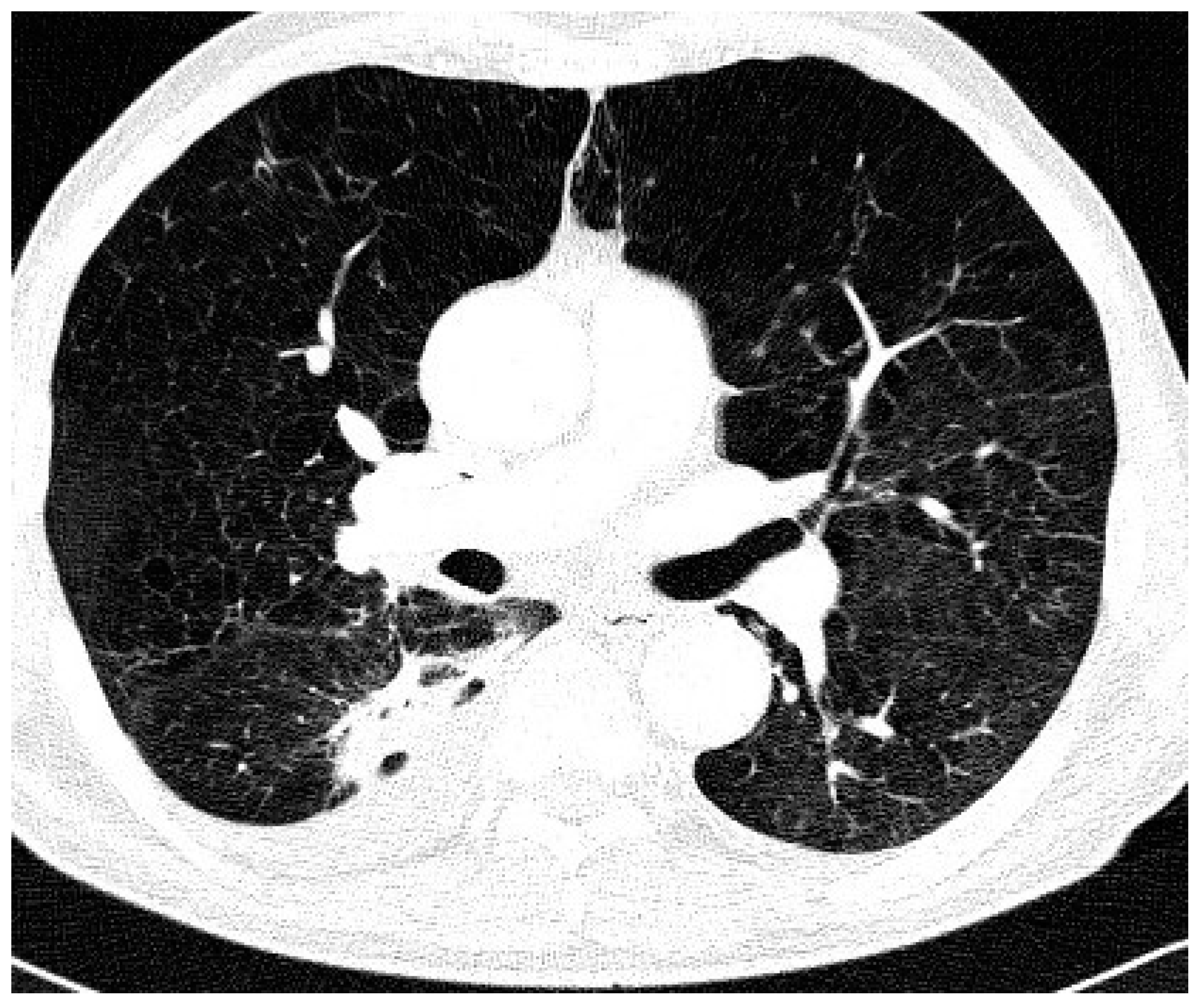
| Type of Chest CT Changes | Total Population No. 36 | NTM-LD No. 17 | Colonization No. 19 | p |
|---|---|---|---|---|
| Nodular/bronchiectasis No. (%) | 17 (47) | 8 (47) | 9 (47) | 0.03 |
| Infiltrations/cavities No. (%) | 6 (17) | 6 (35) | 0 (0) | |
| Non-specific No. (%) | 13 (36) | 3 (18) | 10 (57) | |
| Post tuberculous lesions No. (%) | 19 (53) | 10 (59) | 9 (47) | 0.72 |
| Species | Total Population No. 36 | NTM-LD No. 17 | Colonization No. 19 | p |
|---|---|---|---|---|
| M. avium | 14 (39) | 9 (60) | 5 (26) | M. gordonae versus remaining species 0.018 |
| M. gordonae | 7 (19) | 0 (0) | 7 (37) | |
| M. kansasii | 6 (17) | 3 (18) | 3 (16) | |
| M. xenopi | 6 (17) | 3 (18) | 3 (16) | |
| M. fortuitum | 2 (6) | 1 (6) | 1 (5) | |
| M. intracellulare | 1 (3) | 1 (3) | 0 (0) | |
| P. aeruginosa | 5 (14) | 1 (3) | 4 (21) | 0.4 |
| Other Gram (-) | 9 (25) | 4 (24) | 5 (26) | 0.85 |
| A. fumigatus | 6 (17) | 3 (18) | 3 (16) | 0.77 |
| Candida sp. | 9 (25) | 5 (29) | 4 (22) | 0.85 |
| Factor | HR | 95%CI | p |
|---|---|---|---|
| BMI | 3.55 | 2.84–4.12 | 0.001 |
| BMI < 22.5 | 2.45 | 1.16–3.85 | 0.002 |
| Elevated body temperature | 3.02 | 2.24–4.96 | 0.005 |
| CT infiltrative-cavitary type | 3.38 | 2.54–5.38 | 0.002 |
| NTM other than M. gordonae | 3.06 | 2.92–4.45 | 0.004 |
| Probability scoring | 5.75 | 4.19–6.64 | 0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szturmowicz, M.; Oniszh, K.; Wyrostkiewicz, D.; Radwan-Rohrenschef, P.; Filipczak, D.; Zabost, A. Non-Tuberculous Mycobacteria in Respiratory Specimens of Patients with Obstructive Lung Diseases—Colonization or Disease? Antibiotics 2020, 9, 424. https://doi.org/10.3390/antibiotics9070424
Szturmowicz M, Oniszh K, Wyrostkiewicz D, Radwan-Rohrenschef P, Filipczak D, Zabost A. Non-Tuberculous Mycobacteria in Respiratory Specimens of Patients with Obstructive Lung Diseases—Colonization or Disease? Antibiotics. 2020; 9(7):424. https://doi.org/10.3390/antibiotics9070424
Chicago/Turabian StyleSzturmowicz, Monika, Karina Oniszh, Dorota Wyrostkiewicz, Piotr Radwan-Rohrenschef, Dorota Filipczak, and Anna Zabost. 2020. "Non-Tuberculous Mycobacteria in Respiratory Specimens of Patients with Obstructive Lung Diseases—Colonization or Disease?" Antibiotics 9, no. 7: 424. https://doi.org/10.3390/antibiotics9070424
APA StyleSzturmowicz, M., Oniszh, K., Wyrostkiewicz, D., Radwan-Rohrenschef, P., Filipczak, D., & Zabost, A. (2020). Non-Tuberculous Mycobacteria in Respiratory Specimens of Patients with Obstructive Lung Diseases—Colonization or Disease? Antibiotics, 9(7), 424. https://doi.org/10.3390/antibiotics9070424