A Prediction Tool for the Presence of Ceftriaxone-Resistant Uropathogens upon Hospital Admission

 , and
, and
Abstract
1. Introduction
2. Results
2.1. Study Population and Patient Characteristics
2.2. Distribution of the Types of UTIs and Initial Prescribed Antibiotics for UTI
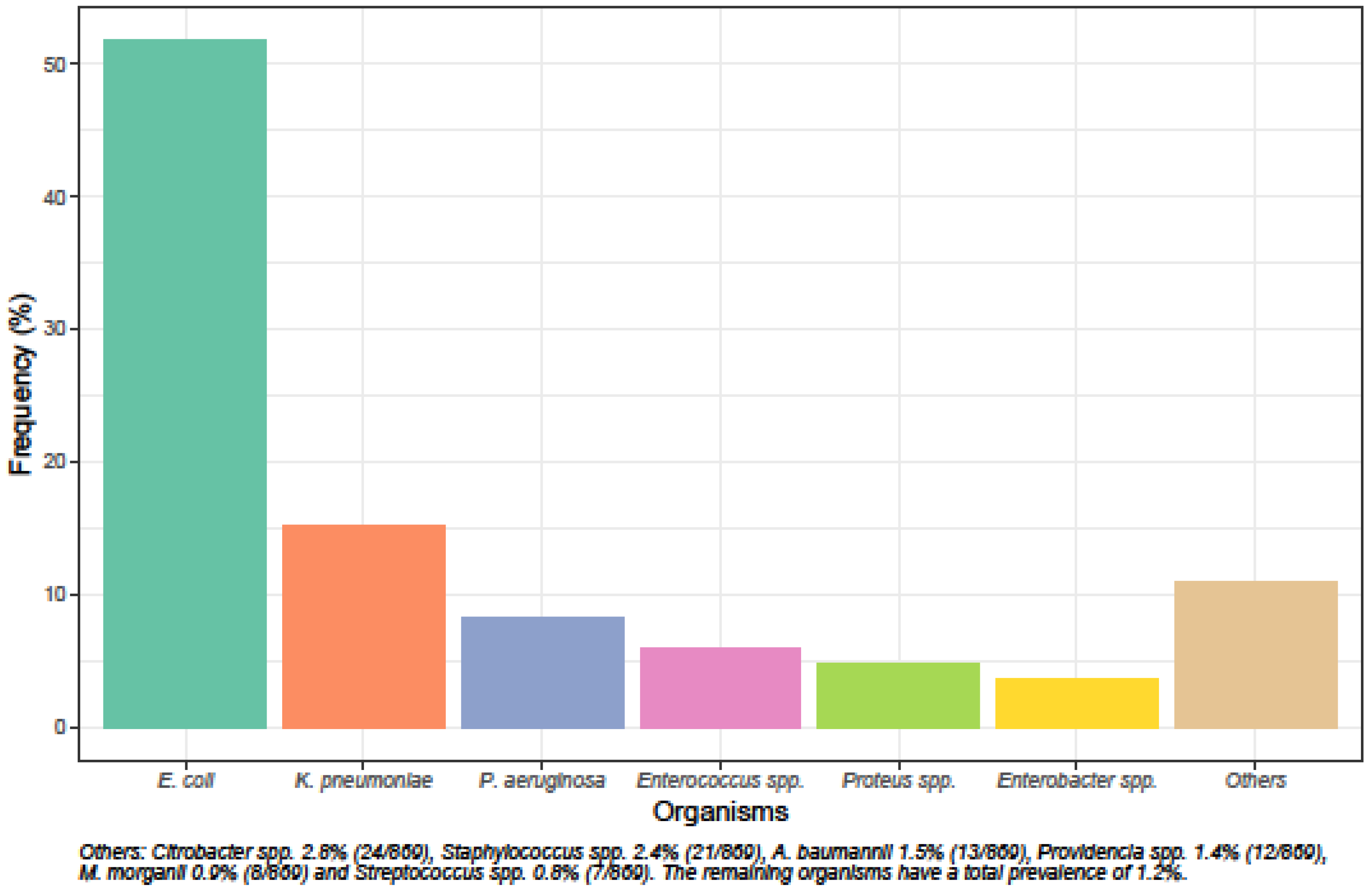
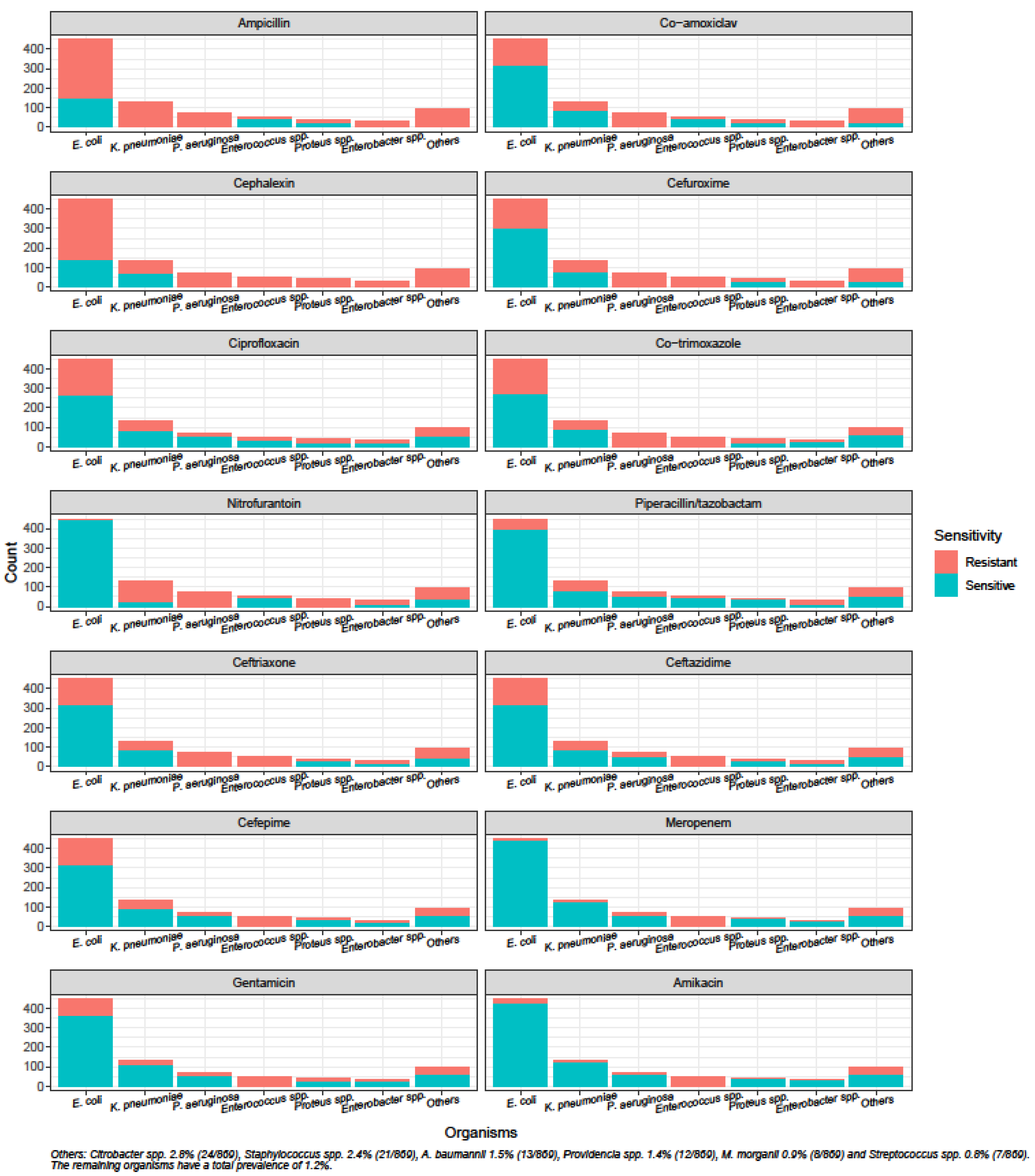
2.3. Species Distribution of Uropathogens and Susceptibility of Uropathogens to Common Antibiotics
2.4. Risk Factors for the Presence of CrP and CrGNR
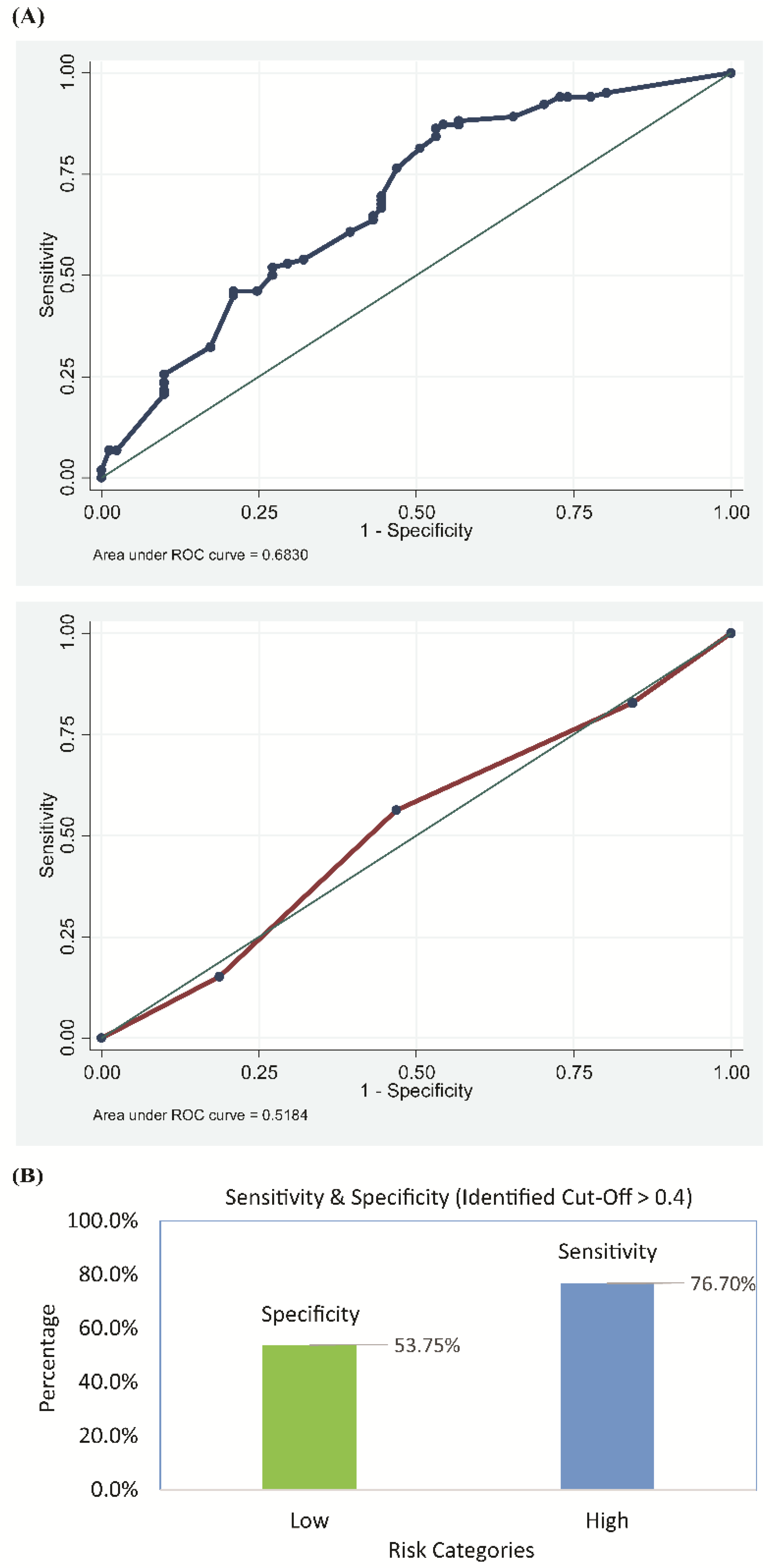
2.5. External Validity of the Risk-Scoring Model
3. Discussion
4. Materials and Methods
4.1. Patient Population, Study Design and Data
4.2. Data Analysis
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| UTI | Urinary tract infection |
| ASB | asymptomatic bacteriuria |
| CrP | ceftriaxone-resistant uropathogens |
| CrGNR | ceftriaxone-resistant Gram-negative uropathogens |
| NUH | National University Hospital |
| CAP | College of American Pathologists |
| EUCAST | European Committee for Antimicrobial Susceptibility Testing |
| CHAID | chi-square automated interactions detector |
| gSEM | generalized structural equation modeling |
| AOR | adjusted odds ratios |
| ROC | receiver operating characteristic |
| SMART | Study for Monitoring Antimicrobial Resistance Trends |
| SD | standard deviation |
| C.I. | confidence interval |
| GNR | Gram-negative uropathogens |
References
- Gupta, K.; Hooton, T.M.; Naber, K.G. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin. Infect. Dis. 2011, 52, 103–120. [Google Scholar] [CrossRef] [PubMed]
- Zowawi, H.M.; Harris, P.N.; Roberts, M.J. The emerging threat of multidrug-resistant gram-negative bacteria in urology. Nat. Rev. Urol. 2015, 12, 570–584. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Antimicrobial Resistance: Global Report on Surveillance; World Health Organization: Geneva, Switzerland, 2014; Available online: https://www.who.int/drugresistance/documents/surveillancereport/en (accessed on 27 March 2018).
- Hsueh, P.R.; Hoban, D.J.; Carmeli, Y. Consensus review of the epidemiology and appropriate antimicrobial therapy of complicated urinary tract infections in Asia-Pacific region. J. Infect. 2011, 63, 114–123. [Google Scholar] [CrossRef] [PubMed]
- Choe, H.S.; Lee, S.J.; Cho, Y.H. Aspects of urinary tract infections and antimicrobial resistance in hospitalized urological patients in Asia: 10-year Results of the Global Prevalence Study of Infections in Urology (GPIU). J. Infect. Chemother. 2018, 24, 278–283. [Google Scholar] [CrossRef] [PubMed]
- Jean, S.-S.; Coombs, G.; Ling, T. Epidemiology and antimicrobial susceptibility profiles of pathogens causing urinary tract infections in the Asia-Pacific region: Results from the Study for Monitoring Antimicrobial Resistance Trends (SMART), 2010–2013. Int. J. Antimicrob. Agents 2016, 47, 328–334. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M. Strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. BMJ 2007, 335, 806–808. [Google Scholar] [CrossRef] [PubMed]
- Foxman, B. Epidemiology of urinary tract infections: Incidence, morbidity, and economic costs. Am. J. Med. 2002, 113, 5–13. [Google Scholar] [CrossRef]
- Walker, E.; Lyman, A.; Gupta, K.; Mahoney, M.V.; Snyder, G.M.; Hirsch, E.B. Clinical management of an increasing threat: Outpatient urinary tract infections due to multidrug-resistant uropathogens. Clin. Infect. Dis. 2016, 63, 960–965. [Google Scholar] [CrossRef] [PubMed]
- Wright, S.W.; Wrenn, K.D.; Haynes, M.; Haas, D.W. Prevalence and risk factors for multidrug resistant uropathogens in ED patients. Am. J. Emerg. Med. 2000, 18, 143–146. [Google Scholar] [CrossRef]
- Kass, G. An exploratory technique for investigating large quantities of categorical data. Appl. Stat. 1980, 29, 119–127. [Google Scholar] [CrossRef]
- Rabe-Hesketh, S.; Skrondal, A.; Pickels, A. Generalized multilevel structural equation modelling. Psychometrika 2004, 69, 167–190. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | |
|---|---|
| Patient-Level Data | n = 686 |
| Age in years (mean ± SD) | 69.0 ± 18.7 |
| Race, n (%) | |
| Chinese | 443 (64.6) |
| Malay | 136 (19.8) |
| Indian | 74 (10.8) |
| Others | 33 (4.8) |
| Gender, n (%) | |
| Female | 416 (60.6) |
| Male | 270 (39.4) |
| Diabetes mellitus, n (%) | 276 (40.2) |
| Chronic Kidney Disease, n (%) | 181 (26.4) |
| Renal transplant, n (%) | 12 (1.7) |
| Hemodialysis within the past 30 days, n (%) | 8 (1.2) |
| Immunodeficiency, n (%) | 44 (6.4) |
| Prior urological procedure, n (%) | 54 (7.9) |
| Antibiotic use within the past 3 months, n (%) | 231 (33.7) |
| Positive urine culture within the past 3 months, n (%) | 157 (22.9) |
| Structural/functional abnormality of urinary tract, n (%) | 294 (42.9) |
| Received chemotherapy infusion within past 30 days, n (%) | 8 (1.2) |
| Home wound care within past 30 days, n (%) | 45 (6.6) |
| Hospitalization for ≥2 days within the past 3 months, n (%) | 233 (34.0) |
| Hospitalization for ≥2 days within the past 30 days, n (%) | 149 (21.7) |
| Catheterization, n (%) | 162 (23.6) |
| Intermittent | 21 (3.1) |
| Suprapubic | 4 (0.6) |
| Indwelling | 137 (20.0) |
| Duration of catheterization, n (%) | |
| Short term (<30 days) | 24 (3.5) |
| Long term (≥30 days) | 138 (20.1) |
| Diagnosis | Prevalence (%) |
|---|---|
| Uncomplicated UTI | 132 (19.2) |
| Cystitis | 54 (7.9) |
| Pyelonephritis/Pyonephrosis ^ | 78 (11.4) |
| Complicated UTI * | 540 (78.7) |
| Pyelonephritis/Pyonephrosis ^ | 157 (22.9) |
| Prostatitis/Epididymo-orchitis | 5 (0.7) |
| Catheter associated UTI | 161 (23.5) |
| ASB (pregnancy) | 10 (1.5) |
| ASB (planning for invasive urological procedures) | 4 (0.6) |
| Risk Factor | Ceftriaxone-Resistant AOR (95% C.I.) | p-Value | Ceftriaxone-Resistant GNR AOR (95% C.I.) | p-Value |
|---|---|---|---|---|
| Hospitalization for ≥2 days within past 30 days | 3.05 (1.79 − 5.22) | <0.001 | NA | NA |
| Antibiotic use within the past 3 months | 2.56 (1.60 − 4.08) | <0.001 | NA | NA |
| Male gender | 2.66 (1.66 − 4.25) | <0.001 | 0.67 (0.41 − 1.11) | 0.124 |
| Catheterization | NA | NA | 1.58 (0.90 − 2.77) | 0.110 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, N.Y.; Poh, G.Q.; Teng, G.C.W.; Chen, H.H.; Chan, D.S.G.; Chan, S.-P.; Tambyah, P.A.; Bagdasarian, N.; Wu, J.E. A Prediction Tool for the Presence of Ceftriaxone-Resistant Uropathogens upon Hospital Admission. Antibiotics 2020, 9, 316. https://doi.org/10.3390/antibiotics9060316
Li NY, Poh GQ, Teng GCW, Chen HH, Chan DSG, Chan S-P, Tambyah PA, Bagdasarian N, Wu JE. A Prediction Tool for the Presence of Ceftriaxone-Resistant Uropathogens upon Hospital Admission. Antibiotics. 2020; 9(6):316. https://doi.org/10.3390/antibiotics9060316
Chicago/Turabian StyleLi, Nancy Yanzhe, Gang Quan Poh, Gladys Chung Wei Teng, Hui Hiong Chen, Douglas Su Gin Chan, Siew-Pang Chan, Paul Anantharajah Tambyah, Natasha Bagdasarian, and Jia En Wu. 2020. "A Prediction Tool for the Presence of Ceftriaxone-Resistant Uropathogens upon Hospital Admission" Antibiotics 9, no. 6: 316. https://doi.org/10.3390/antibiotics9060316
APA StyleLi, N. Y., Poh, G. Q., Teng, G. C. W., Chen, H. H., Chan, D. S. G., Chan, S.-P., Tambyah, P. A., Bagdasarian, N., & Wu, J. E. (2020). A Prediction Tool for the Presence of Ceftriaxone-Resistant Uropathogens upon Hospital Admission. Antibiotics, 9(6), 316. https://doi.org/10.3390/antibiotics9060316