High Abundance of Proteobacteria in Ileo-Anal Pouch Anastomosis and Increased Abundance of Fusobacteria Associated with Increased Pouch Inflammation

 and
and
Abstract
1. Introduction
2. Results
2.1. Patients Characteristics
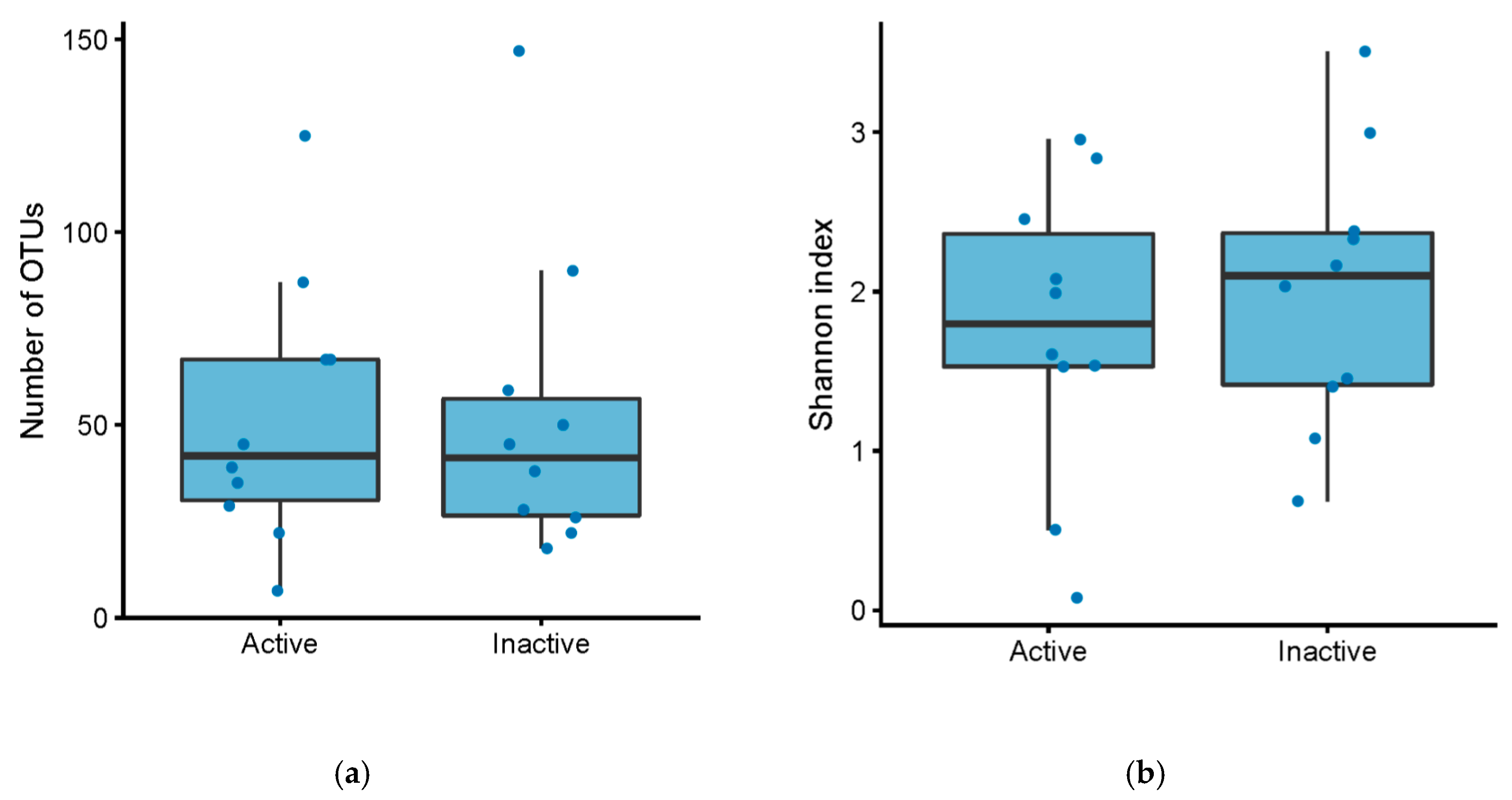
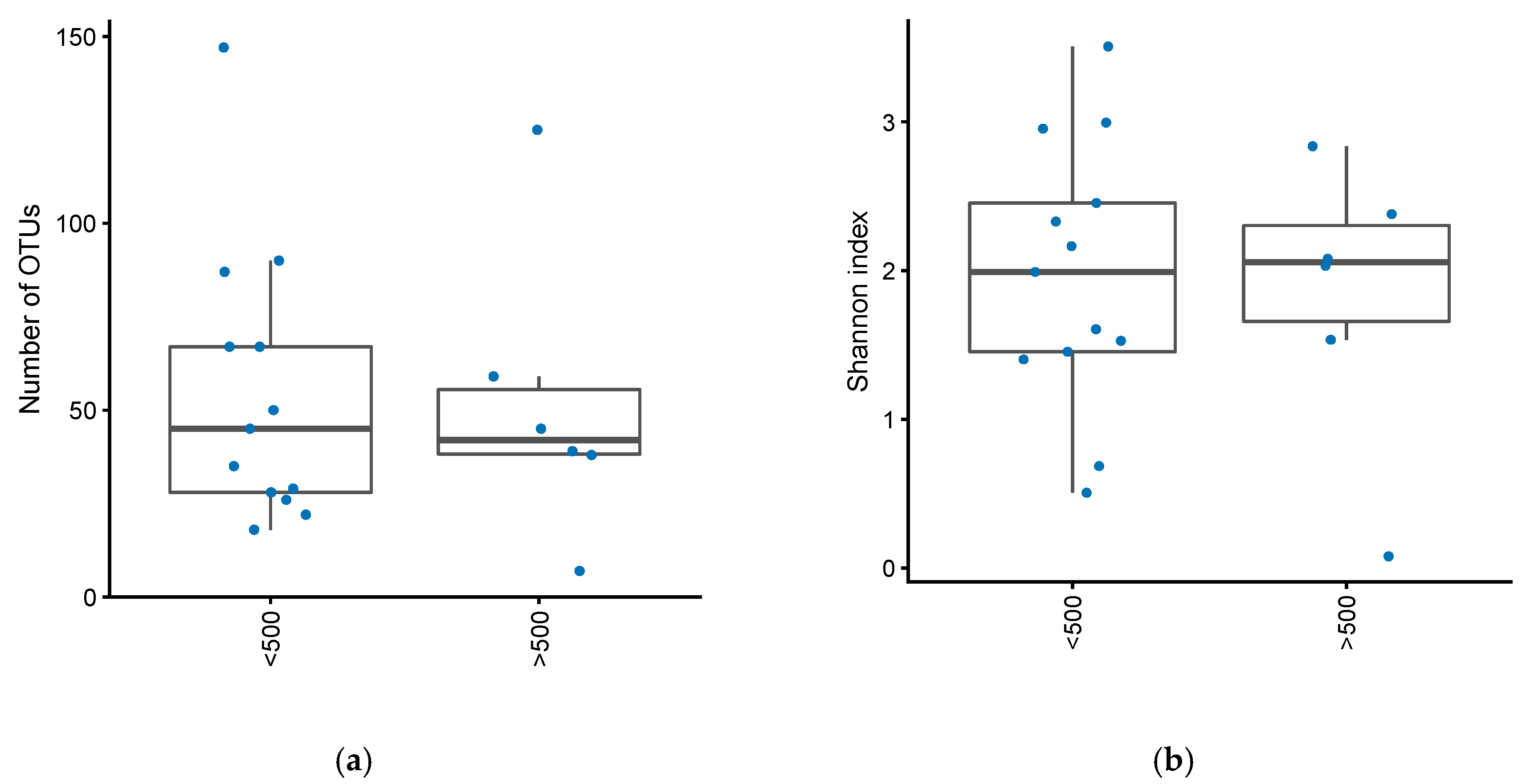
2.2. OTU and Shannon Index
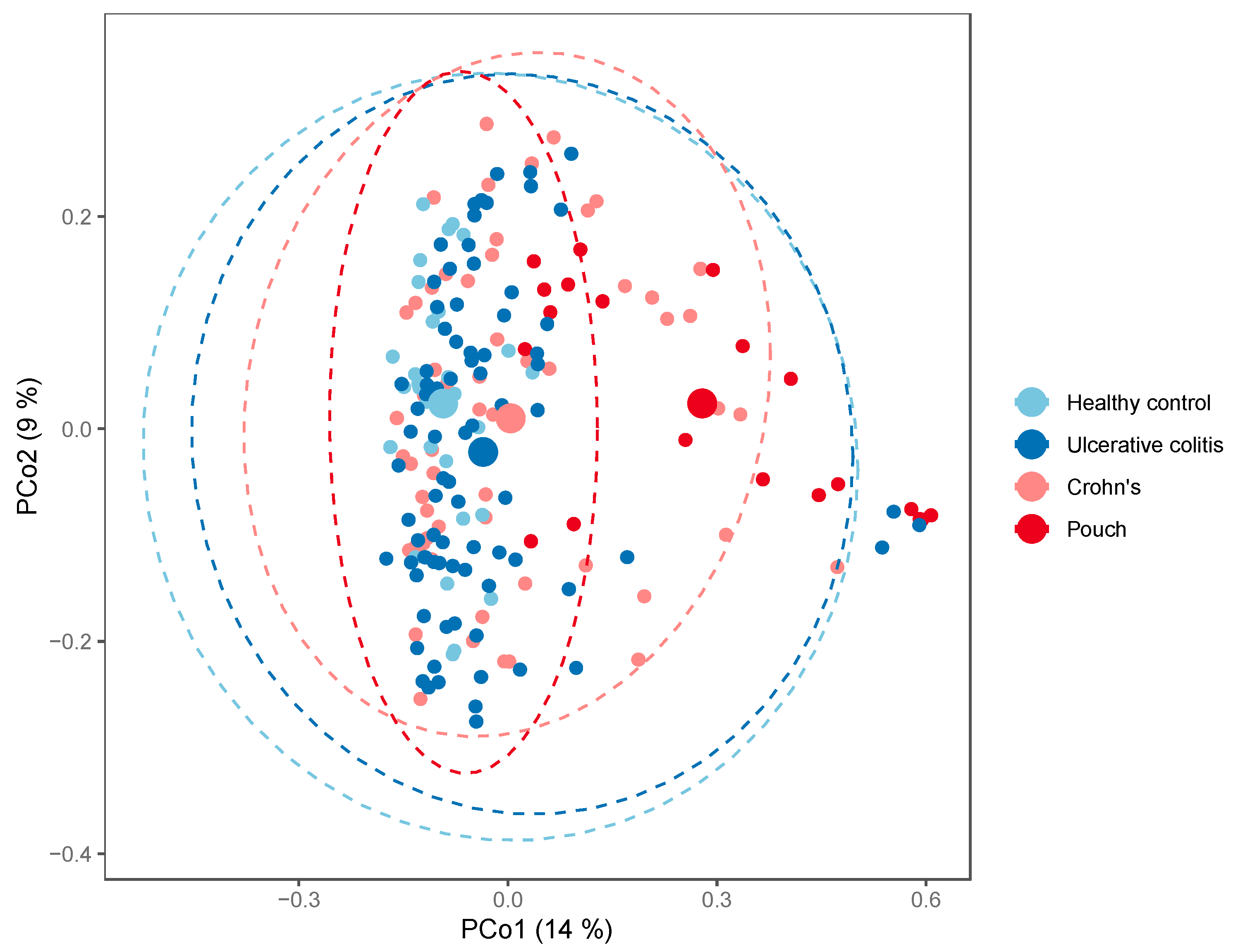
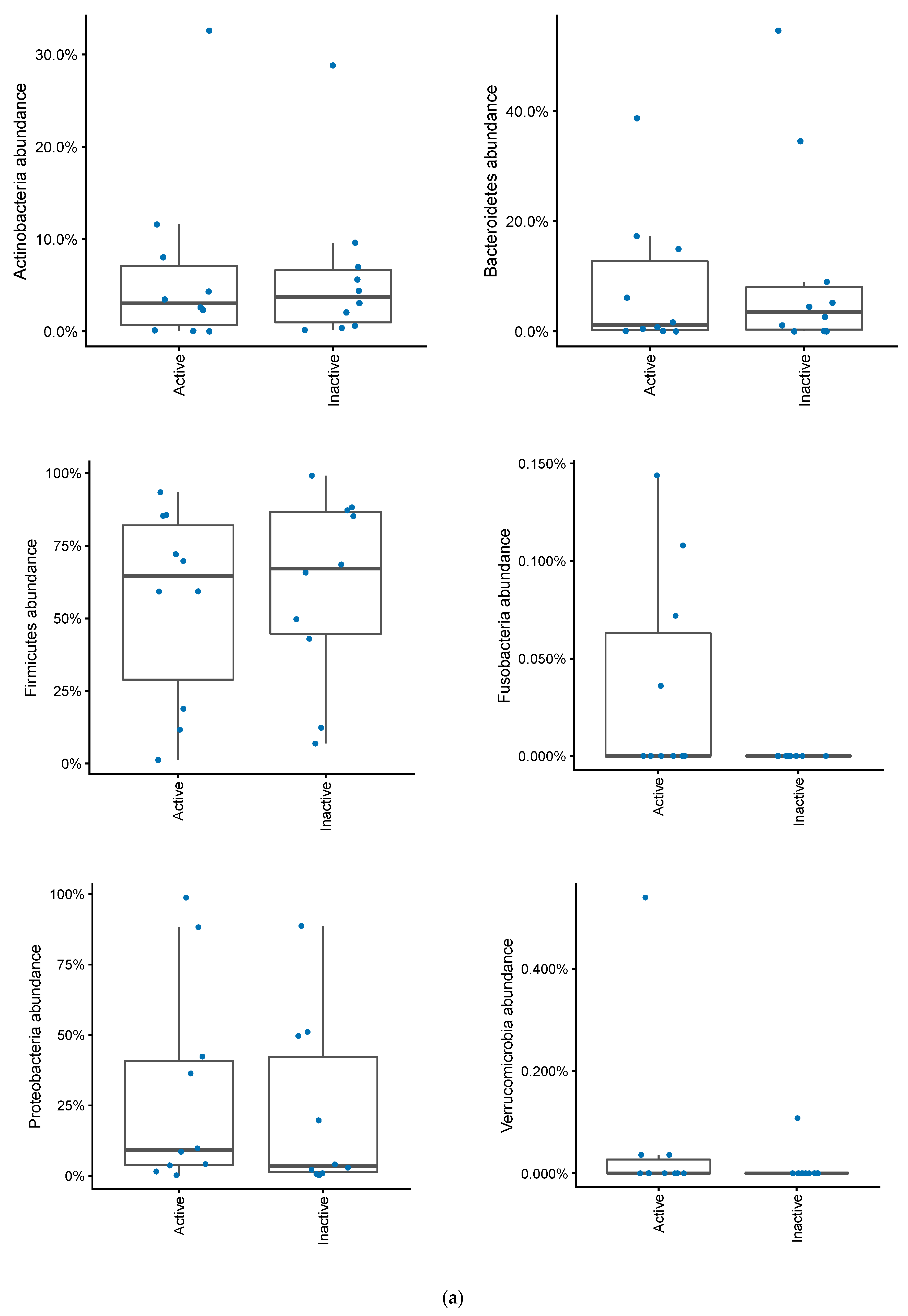
2.3. Bacterial Composition
2.4. E. coli Phylogenetic Groups
3. Discussion
4. Material and Methods
4.1. Population and Sample Collection
4.2. Disease Activity and Severity
4.3. Determination of Fecal Calprotectin
4.4. Isolation of E. coli from Fecal Samples
4.5. E. coli Phylogenetic Group Determination
4.6. DNA Extraction for Microbiota Analysis
4.7. Bioinformatical Analysis
4.8. Ethical Considerations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Feuerstein, J.D.; Cheifetz, A.S. Ulcerative colitis: Epidemiology, diagnosis, and management. Mayo Clin. Proc. 2014, 89, 1553–1563. [Google Scholar] [CrossRef] [PubMed]
- Hata, K.; Ishihara, S.; Nozawa, H.; Kawai, K.; Kiyomatsu, T.; Tanaka, T.; Kishikawa, J.; Anzai, H.; Watanabe, T. Pouchitis after ileal pouch-anal anastomosis in ulcerative colitis: Diagnosis, management, risk factors, and incidence. Dig. Endosc. 2017, 29, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Kartheuser, A.; Stangherlin, P.; Brandt, D.; Remue, C.; Sempoux, C. Restorative proctocolectomy and ileal pouch-anal anastomosis for familial adenomatous polyposis revisited. Fam. Cancer 2006, 5, 241–260. [Google Scholar] [CrossRef] [PubMed]
- Singh, V.P.; Proctor, S.D.; Willing, B.P. Koch’s postulates, microbial dysbiosis and inflammatory bowel disease. Clin. Microbiol. Infect. 2016, 22, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Khan, K.J.; Ullman, T.A.; Ford, A.C.; Abreu, M.T.; Abadir, A.; Marshall, J.K.; Talley, N.J.; Moayyedi, P. Antibiotic therapy in inflammatory bowel disease: A systematic review and meta-analysis. Am. J. Gastroenterol. 2011, 106, 661–673. [Google Scholar] [CrossRef]
- Narula, N.; Kassam, Z.; Yuan, Y.; Colombel, J.F.; Ponsioen, C.; Reinisch, W.; Moayyedi, P. Systematic Review and Meta-analysis: Fecal Microbiota Transplantation for Treatment of Active Ulcerative Colitis. Inflamm. Bowel Dis. 2017, 23, 1702–1709. [Google Scholar] [CrossRef]
- Abraham, B.P.; Quigley, E.M.M. Probiotics in Inflammatory Bowel Disease. Gastroenterol. Clin. N. Am. 2017, 46, 769–782. [Google Scholar] [CrossRef]
- Goethel, A.; Croitoru, K.; Philpott, D.J. The interplay between microbes and the immune response in inflammatory bowel disease. J. Physiol. 2018, 596, 3869–3882. [Google Scholar] [CrossRef]
- Rizzatti, G.; Lopetuso, L.R.; Gibiino, G.; Binda, C.; Gasbarrini, A. Proteobacteria: A Common Factor in Human Diseases. Biomed Res. Int. 2017, 2017, 9351507. [Google Scholar] [CrossRef]
- Iebba, V.; Totino, V.; Gagliardi, A.; Santangelo, F.; Cacciotti, F.; Trancassini, M.; Mancini, C.; Cicerone, C.; Corazziari, E.; Pantanella, F. Eubiosis and dysbiosis: The two sides of the microbiota. New Microbiol. 2016, 39, 1–12. [Google Scholar]
- Shin, N.-R.; Whon, T.W.; Bae, J.-W. Proteobacteria: Microbial signature of dysbiosis in gut microbiota. Trends Biotechnol. 2015, 33, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Petersen, A.M.; Halkjær, S.I.; Gluud, L.L. Intestinal colonization with phylogenetic group B2 Escherichia coli related to inflammatory bowel disease: A systematic review and meta-analysis. Scand. J. Gastroenterol. 2015, 50, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- Magro, F.; Gionchetti, P.; Eliakim, R.; Ardizzone, S.; Armuzzi, A.; Barreiro-de Acosta, M.; Burisch, J.; Gecse, K.B.; Hart, A.L.; Hindryckx, P. Third European Evidence-based Consensus on Diagnosis and Management of Ulcerative Colitis. Part 1: Definitions, Diagnosis, Extra-intestinal Manifestations, Pregnancy, Cancer Surveillance, Surgery, and Ileo-anal Pouch Disorders. J. Crohn Colitis 2017, 11, 649–670. [Google Scholar] [CrossRef]
- Shen, B.; Achkar, J.-P.; Connor, J.T.; Ormsby, A.H.; Remzi, F.H.; Bevins, C.L.; Brzezinski, A.; Bambrick, M.L.; Fazio, V.W.; Lashner, B.A. Modified pouchitis disease activity index: A simplified approach to the diagnosis of pouchitis. Dis. Colon Rectum 2003, 46, 748–753. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Bittinger, K.; Charlson, E.S.; Hoffmann, C.; Lewis, J.; Wu, G.D.; Collman Ronald, G.; Bushman Frederic, D.; Li, H. Associating microbiome composition with environmental covariates using generalized UniFrac distances. Bioinformatics 2012, 28, 2106–2113. [Google Scholar] [CrossRef] [PubMed]
- Williams Turpin, O.K.; Borowski, K.; Boland, K.; Tyler, A.; Cohen, Z.; Croitoru, K.; Silverberg, M.S. Mucosa-Associated Microbiota in Ileoanal Pouches May Contribute to Clinical Symptoms, Particularly Stool Frequency, Independent of Endoscopic Disease Activity. Clin. Transl. Gastroenterol. 2019, 10, 1–7. [Google Scholar] [CrossRef]
- Segal, J.P.; Oke, S.; Hold, G.L.; Clark, S.K.; Faiz, O.D.; Hart, A.L. Systematic review: Ileoanal pouch microbiota in health and disease. Aliment. Pharmacol. Ther. 2018, 47, 466–477. [Google Scholar] [CrossRef]
- Maharshak, N.; Cohen, N.A.; Reshef, L.; Tulchinsky, H.; Gophna, U.; Dotan, I. Alterations of Enteric Microbiota in Patients with a Normal Ileal Pouch Are Predictive of Pouchitis. J. Crohn Colitis 2017, 11, 314–320. [Google Scholar] [CrossRef]
- Komanduri, S.; Gillevet, P.M.; Sikaroodi, M.; Mutlu, E.; Keshavarzian, A. Dysbiosis in Pouchitis: Evidence of Unique Microfloral Patterns in Pouch Inflammation. Clin. Gastroenterol. Hepatol. 2007, 5, 352–360. [Google Scholar] [CrossRef]
- Benlice, C.; Shen, B.; Steele, S.R. Prevention and Medical Treatment of Pouchitis in Ulcerative Colitis. Curr. Drug Targets 2019, 20, 1399–1408. [Google Scholar] [CrossRef]
- Bashir, A.; Miskeen, A.Y.; Hazari, Y.M.; Asrafuzzaman, S.; Fazili, K.M. Fusobacterium nucleatum, inflammation, and immunity: The fire within human gut. Tumor Biol. 2016, 37, 2805–2810. [Google Scholar] [CrossRef]
- Spangler, S.K.; Jacobs, M.R.; Appelbaum, P.C. Activity of WY-49605 compared with those of amoxicillin, amoxicillin-clavulanate, imipenem, ciprofloxacin, cefaclor, cefpodoxime, cefuroxime, clindamycin, and metronidazole against 384 anaerobic bacteria. Antimicrob. Agents Chemother. 1994, 38, 2599–2604. [Google Scholar] [CrossRef]
- Chilton, C.H.; Pickering, D.S.; Freeman, J. Microbiologic factors affecting Clostridium difficile recurrence. Clin. Microbiol. Infect. 2018, 24, 476–482. [Google Scholar] [CrossRef]
- Ben-Bassat, O.; Tyler, A.D.; Xu, W.; Kirsch, R.; Schaeffer, D.F.; Walsh, J.; Steinhart, A.H.; Greenberg, G.R.; Cohen, Z.; Silverberg, M.S. Ileal pouch symptoms do not correlate with inflammation of the pouch. Clin. Gastroenterol. Hepatol. 2014, 12, 831–837. [Google Scholar] [CrossRef]
- Yamamoto, T.; Shimoyama, T.; Bamba, T.; Matsumoto, K. Consecutive Monitoring of Fecal Calprotectin and Lactoferrin for the Early Diagnosis and Prediction of Pouchitis after Restorative Proctocolectomy for Ulcerative Colitis. Am. J. Gastroenterol. 2015, 110, 881–887. [Google Scholar] [CrossRef]
- Selvig, D.; Piceno, Y.; Terdiman, J.; Zydek, M.; Umetsu, S.E.; Balitzer, D.; Fadrosh, D.; Lynch, K.; Lamere, B.; Leith, T. Fecal Microbiota Transplantation in Pouchitis: Clinical, Endoscopic, Histologic, and Microbiota Results from a Pilot Study. Dig. Dis. Sci. 2019, 65, 1099–1106. [Google Scholar] [CrossRef]
- Mimura, T.; Rizzello, F.; Helwig, U.; Poggioli, G.; Schreiber, S.; Talbot, I.C.; Nicholls, R.J.; Gionchetti, P.; Campieri, M.; Kamm, M.A. Once daily high dose probiotic therapy (VSL#3) for maintaining remission in recurrent or refractory pouchitis. Gut 2004, 53, 108–114. [Google Scholar] [CrossRef]
- Petersen, A.M.; Schou, C.; Mirsepasi, H.; Engberg, J.; Friis-Møller, A.; Nordgaard-Lassen, I.; Wildt, S.; Krogfelt, K.A. Seroreactivity to E. coli outer membrane protein C antibodies in active inflammatory bowel disease; diagnostic value and correlation with phylogroup B2 E. coli infection. Scand. J. Gastroenterol. 2012, 47, 155–161. [Google Scholar] [CrossRef]
- Vester-Andersen, M.K.; Prosberg, M.V.; Jess, T.; Andersson, M.; Bengtsson, B.G.; Blixt, T.; Munkholm, P.; Bendtsen, F.; Vind, I. Disease course and surgery rates in inflammatory bowel disease: A population-based, 7-year follow-up study in the era of immunomodulating therapy. Am. J. Gastroenterol. 2014, 109, 705–714. [Google Scholar] [CrossRef]
- Vester-Andersen, M.K.; Mirsepasi-Lauridsen, H.C.; Prosberg, M.V.; Mortensen, C.O.; Träger, C.; Skovsen, K.; Sørensen, N. Increased abundance of proteobacteria in aggressive Crohn’s disease seven years after diagnosis. Sci. Rep. 2019, 9, 13473. [Google Scholar] [CrossRef]
- Johne, B.; Kronborg, O.; Tøn, H.I.; Kristinsson, J.; Fuglerud, P. A new fecal calprotectin test for colorectal neoplasia. Clinical results and comparison with previous method. Scand. J. Gastroenterol. 2001, 36, 291–296. [Google Scholar] [CrossRef]
- Clermont, O.; Bonacorsi, S.; Bingen, E. Rapid and simple determination of the Escherichia coli phylogenetic group. Appl. Environ. Microbiol. 2000, 66, 4555–4558. [Google Scholar] [CrossRef]
- Vejborg, R.M.; Hancock, V.; Petersen, A.M.; Krogfelt, K.; Klemm, P. Comparative genomics of Escherichia coli isolated from patients with inflammatory bowel disease. BMC Genom. 2011, 12, 316. [Google Scholar] [CrossRef]
- Petersen, A.M.; Nielsen, E.M.; Litrup, E.; Brynskov, J.; Mirsepasi, H.; Krogfelt, K. A phylogenetic group of Escherichia coli associated with active left-sided inflammatory bowel disease. BMC Microbiol. 2009, 9, 171. [Google Scholar] [CrossRef]
- Aagaard, K.; Petrosino, J.; Keitel, W.; Watson, M.; Katancik, J.; Garcia, N.; Patel, S.; Cutting, M.; Madden, T.; Hamilton, H. The Human Microbiome Project strategy for comprehensive sampling of the human microbiome and why it matters. FASEB J. 2013, 27, 1012–1022. [Google Scholar] [CrossRef]
- Weiss, S.; Amir, A.; Hyde, E.R.; Metcalf, J.L.; Song, S.J.; Knight, R. Tracking down the sources of experimental contamination in microbiome studies. Genome Biol. 2014, 15, 564. [Google Scholar] [CrossRef]
- Klindworth, A.; Pruesse, E.; Schweer, T.; Peplies, J.; Quast, C.; Horn, M.; Glöckner, F.O. Evaluation of general 16S ribosomal RNA gene PCR primers for classical and next-generation sequencing-based diversity studies. Nucleic Acids Res. 2013, 41, 1–11. [Google Scholar] [CrossRef]
- Edgar, R.C. UPARSE: Highly accurate OTU sequences from microbial amplicon reads. Nat. Methods 2013, 10, 996–998. [Google Scholar] [CrossRef]
- Schloss, P.D.; Westcott, S.L.; Ryabin, T.; Hall, J.R.; Hartmann, M.; Hollister, E.B.; Lesniewski, R.A.; Oakley, B.B.; Parks, D.H.; Robinson, C.J. Introducing mothur: Open-source, platform-independent, community-supported software for describing and comparing microbial communities. Appl. Environ. Microbiol. 2009, 75, 7537–7541. [Google Scholar] [CrossRef]
- Edgar, R.C.; Haas, B.J.; Clemente, J.C.; Quince, C.; Knight, R. UCHIME improves sensitivity and speed of chimera detection. Bioinformatics 2011, 27, 2194–2200. [Google Scholar] [CrossRef]
- Wang, Q.; Garrity, G.M.; Tiedje, J.M.; Cole, J.R. Naïve Bayesian classifier for rapid assignment of rRNA sequences into the new bacterial taxonomy. Appl. Environ. Microbiol. 2007, 73, 5261–5267. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient ID. | Age | Sex | MPDAI | Calprotectin | E. coli Phylogroup | Abundance of Proteobacteria (%) | Shannon Index | Number of OTUs |
|---|---|---|---|---|---|---|---|---|
| P17 | 24 | F | 6 | 2009 | A | 3.71 | 1.53 | 39 |
| P20 | 38 | F | 4 | 62 | B1, A | 36.33 | 1.53 | 29 |
| P21 | 25 | M | 5 | 550 | B2, A | 8.53 | 2.08 | 45 |
| P25 | 47 | M | 4 | 80 | B1 | 1.51 | 1.61 | 67 |
| P47 | 32 | M | 3 | 111 | D | 88.17 | 0.51 | 22 |
| P68 | 42 | F | 5 | 1707 | A | 98.71 | 0.08 | 7 |
| P71 | 79 | F | 4 | <50 | no E. coli | 42.34 | 1.99 | 35 |
| P74 | 27 | M | 6 | 2309 | no E. coli | 4.1 | 2.84 | 125 |
| P80 | 60 | M | 3 | 296 | D | 9.75 | 2.95 | 87 |
| P121 | 62 | F | 6 | 111 | B2 | 0.18 | 2.46 | 67 |
| P1 | 40 | M | 0 | 71 | A | 19.68 | 3.51 | 147 |
| P58 | 41 | F | 1 | 163 | A | 49.64 | 1.40 | 26 |
| P62 | 50 | M | 0 | NA | no E. coli | 0.22 | 1.08 | 22 |
| P63 | 35 | M | 0 | <50 | D, B2 | 88.71 | 0.69 | 18 |
| P94 | 44 | F | 0 | 260 | no E. coli | 0.90 | 2.33 | 50 |
| P97 | 32 | M | 0 | <50 | no E. coli | 0.61 | 3.00 | 90 |
| P104 | 57 | M | 1 | <50 | B2, A, D | 4.06 | 2.16 | 45 |
| P130 | 40 | F | 0 | 119 | A | 51.08 | 1.45 | 28 |
| P150 | 37 | M | 1 | 1132 | B2, B1 | 2.19 | 2.38 | 59 |
| P200 | 36 | F | 2 | 1566 | no E. coli | 2.84 | 2.03 | 38 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petersen, A.M.; Mirsepasi-Lauridsen, H.C.; Vester-Andersen, M.K.; Sørensen, N.; Krogfelt, K.A.; Bendtsen, F. High Abundance of Proteobacteria in Ileo-Anal Pouch Anastomosis and Increased Abundance of Fusobacteria Associated with Increased Pouch Inflammation. Antibiotics 2020, 9, 237. https://doi.org/10.3390/antibiotics9050237
Petersen AM, Mirsepasi-Lauridsen HC, Vester-Andersen MK, Sørensen N, Krogfelt KA, Bendtsen F. High Abundance of Proteobacteria in Ileo-Anal Pouch Anastomosis and Increased Abundance of Fusobacteria Associated with Increased Pouch Inflammation. Antibiotics. 2020; 9(5):237. https://doi.org/10.3390/antibiotics9050237
Chicago/Turabian StylePetersen, Andreas Munk, Hengameh Chloé Mirsepasi-Lauridsen, Marianne K. Vester-Andersen, Nikolaj Sørensen, Karen Angeliki Krogfelt, and Flemming Bendtsen. 2020. "High Abundance of Proteobacteria in Ileo-Anal Pouch Anastomosis and Increased Abundance of Fusobacteria Associated with Increased Pouch Inflammation" Antibiotics 9, no. 5: 237. https://doi.org/10.3390/antibiotics9050237
APA StylePetersen, A. M., Mirsepasi-Lauridsen, H. C., Vester-Andersen, M. K., Sørensen, N., Krogfelt, K. A., & Bendtsen, F. (2020). High Abundance of Proteobacteria in Ileo-Anal Pouch Anastomosis and Increased Abundance of Fusobacteria Associated with Increased Pouch Inflammation. Antibiotics, 9(5), 237. https://doi.org/10.3390/antibiotics9050237