2. Results and Discussion
Of the 1524 drugs in the clinical drug library tested, six compounds (tosufloxacin, clinafloxacin, sarafloxacin, doxycycline, thiostrepton, and chlorosalicylanilide) produced no colonies on LB plates. Based on the results of the primary screen, we selected these drug candidates (50 μM) for rescreens using the same method as above to rank the relative activity of these drugs against
S. aureus persisters over time. The bacterial survival was monitored daily for 4 days in drug exposure assay by transferring the bacterial suspension onto TSB agar plates, respectively. Among them, tosufloxacin produced no colonies on TSB plates after 1 day drug exposure; clinafloxacin and thiostrepton produced no colonies on TSB plates after 2 days drug exposure; doxycycline and chlorosalicylanilide produced no colonies on TSB plates after 3 days drug exposure. Sarafloxacin produced no colonies on TSB plates after 4 days drug exposure (
Table 1). The MICs and MBCs of the six drug candidates are shown in
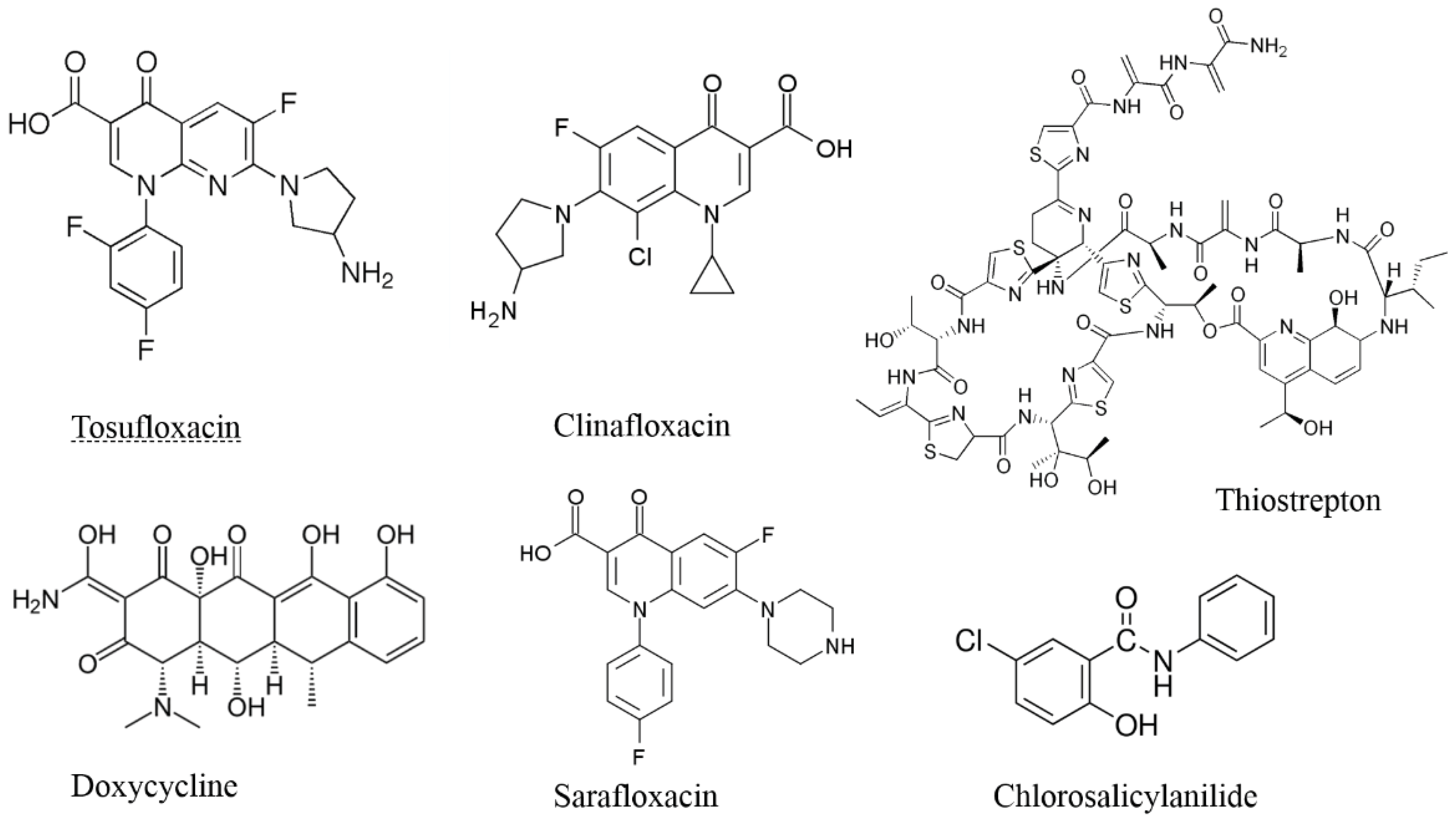
Table 1. The structures of the six drug candidates that showed anti-persister activity are shown in
Figure 1. Tosufloxacin, clinafloxacin and sarafloxacin are quinolone drugs, which exert their antibacterial effect by preventing bacterial DNA from unwinding and replicating [
7]. Doxycycline and thiostrepton interfere with bacterial protein synthesis by inhibiting prolongation of peptide chains when binding to 30S or 50S ribosomal subunits [
8,
9]. Chlorosalicylanilide is a brominated derivative of salicylanilide, and its antibacterial effect may be mediated by inhibiting cellular respiration and energy production.
Table 1.
Activity of six drug candidates (50 μM) selected from the clinical drug library against stationary-phase S. aureus persisters.
Table 1.
Activity of six drug candidates (50 μM) selected from the clinical drug library against stationary-phase S. aureus persisters.
| Drugs (50 μM) | MIC (μM) | MBC (μM) | Bacterial survival at different times of drug exposure a |
|---|
| Day 1 | Day 2 | Day 3 | Day 4 |
|---|
| Tosufloxacin | <0.3 | 0.3 | – | – | – | – |
| Clinafloxacin | 0.3 | 0.3 | + | – | – | – |
| Thiostrepton | 2.5 | – | + | – | – | – |
| Doxycycline | <0.3 | 0.6 | + | + | – | – |
| Chlorosalicylanilide | >10 | – | + | + | – | – |
| Sarafloxacin | 0.3 | – | + | + | + | – |
| Drug-free Control | - | – | + | + | + | + |
Figure 1.
Structures of the six drug candidates with activity against S. aureus persisters.
Figure 1.
Structures of the six drug candidates with activity against S. aureus persisters.
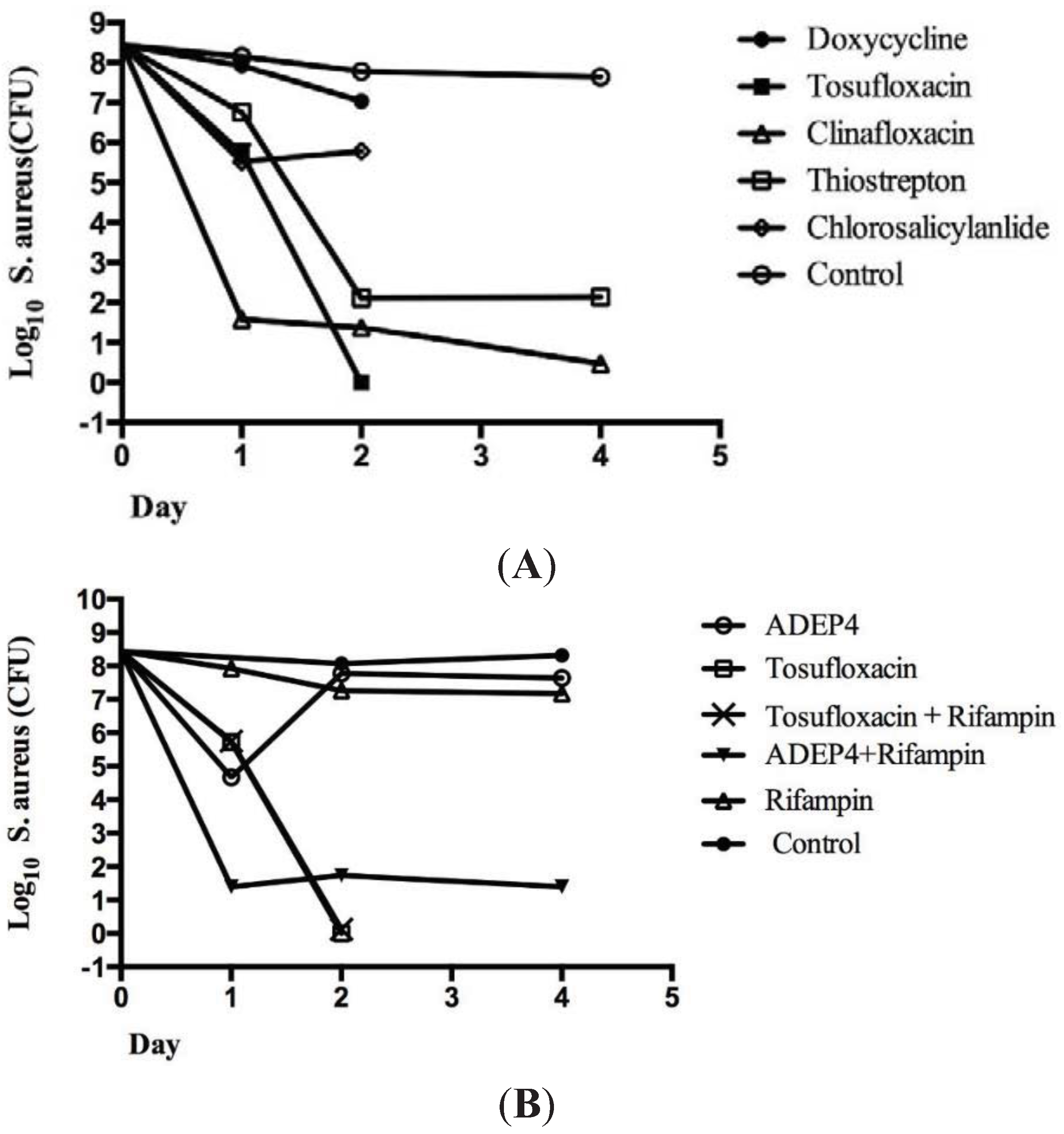
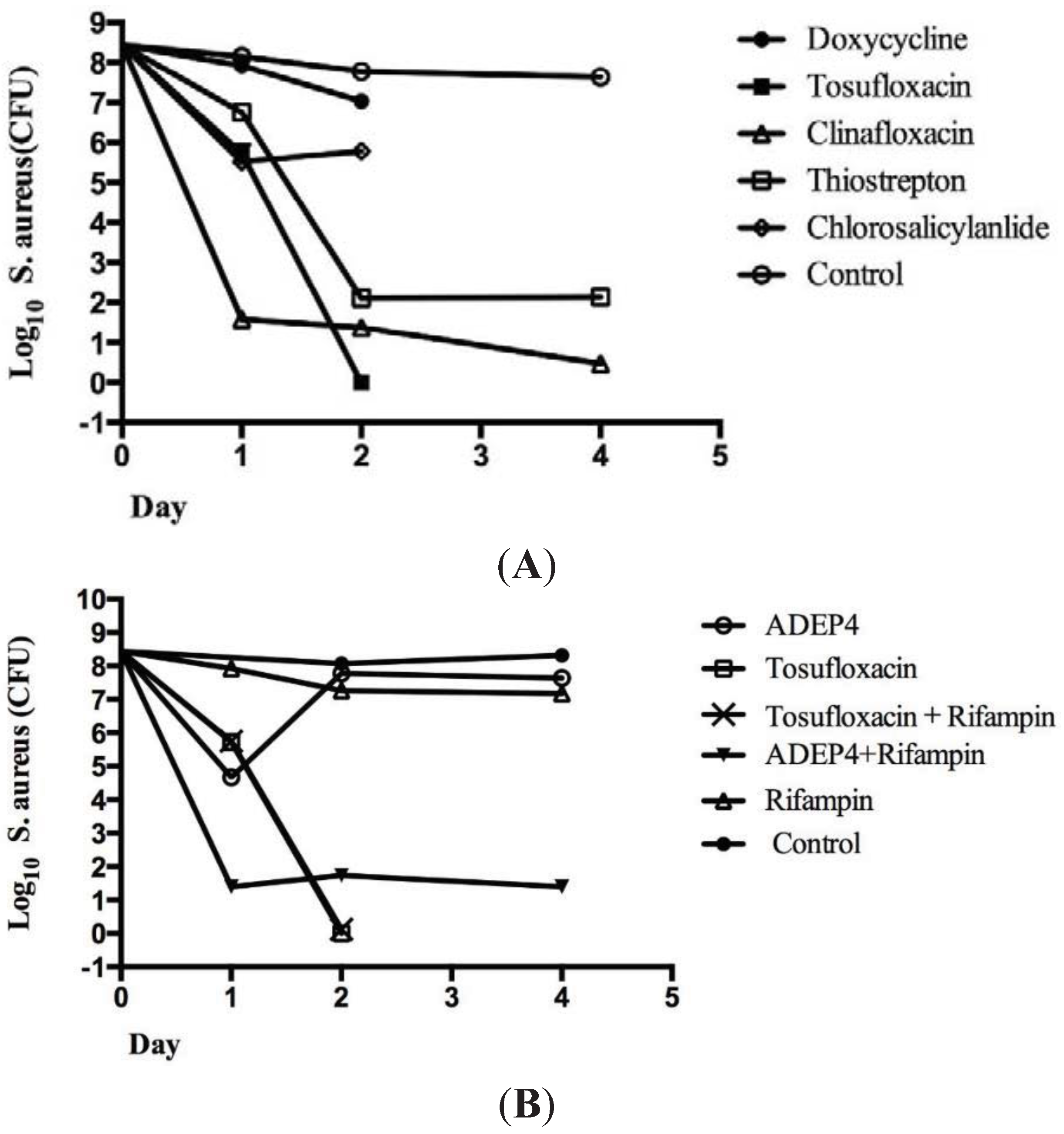
To more accurately rank the six effective drug candidates identified using the 96-well plate method, colony forming unit (CFU) count was also performed after 1 to 4 day drug exposure of persister bacteria in MOPS buffer in Eppendorf tubes. Tosufloxacin had the highest activity against
S. aureus persisters, eradicating all the persisters within 2 days (
Figure 2A). Clinafloxacin was the second highest active drug candidate followed by thiostrepton, decreasing the CFU of the
S. aureus persisters to 10 and 100 respectively after 4 day drug exposure. However, chlorosalicylanilide and doxycycline had limited activity against
S. aureus persisters and the persister level was still at more than 10
6 CFU/mL after drug exposure (
Figure 2A).
Figure 2.
Colony counts to determine the relative activity of the drug candidates and in comparison to known agents active against S. aureus persisters. The S. aureus stationary phase culture was treated with ofloxacin (10 μg/mL) for four hours to enrich persisters. Then, the surviving persisters from the treatment were subjected to drug exposure with different antibiotics (50 μM) as described in the text. The viability of the bacteria was determined by colony forming unit (CFU) count 1 to 4 days after drug exposure. (A) Tosufloxacin (50 μM) was the most active among the six drugs, and completely eliminated all persisters after 2 days; (B) acyldepsipeptide (ADEP4) + rifampin (RIF) could not completely eradicate S. aureus persisters even after 4 days. The final concentrations of ADEP4 and RIF were 5 μg/mL and 0.4 μg/mL, respectively.
Figure 2.
Colony counts to determine the relative activity of the drug candidates and in comparison to known agents active against S. aureus persisters. The S. aureus stationary phase culture was treated with ofloxacin (10 μg/mL) for four hours to enrich persisters. Then, the surviving persisters from the treatment were subjected to drug exposure with different antibiotics (50 μM) as described in the text. The viability of the bacteria was determined by colony forming unit (CFU) count 1 to 4 days after drug exposure. (A) Tosufloxacin (50 μM) was the most active among the six drugs, and completely eliminated all persisters after 2 days; (B) acyldepsipeptide (ADEP4) + rifampin (RIF) could not completely eradicate S. aureus persisters even after 4 days. The final concentrations of ADEP4 and RIF were 5 μg/mL and 0.4 μg/mL, respectively.
It has been reported that the combination of acyldepsipeptide (ADEP4) and rifampin produced complete eradication of
S. aureus biofilms
in vitro and
in vivo [
10]. ADEP4 when used alone had limited activity and that is the reason for the use of ADEP4 and RIF combination in this study for comparison with tosufloxacin. Therefore, we compared tosufloxacin identified from the clinical drug library with ADEP4 + RIF for their activities against
S. aureus persisters
in vitro. We found that while ADEP4+RIF had an initial rapid killing effect in Day 1 the combination failed to completely eradicate all
S. aureus persisters and there were still about 100 residual persisters left even after 4 day drug exposure (
Figure 2B). In contrast, despite a slow killing effect initially at Day 1, tosufloxacin completely eradicated all
S. aureus persisters in 2 days with no persisters surviving (
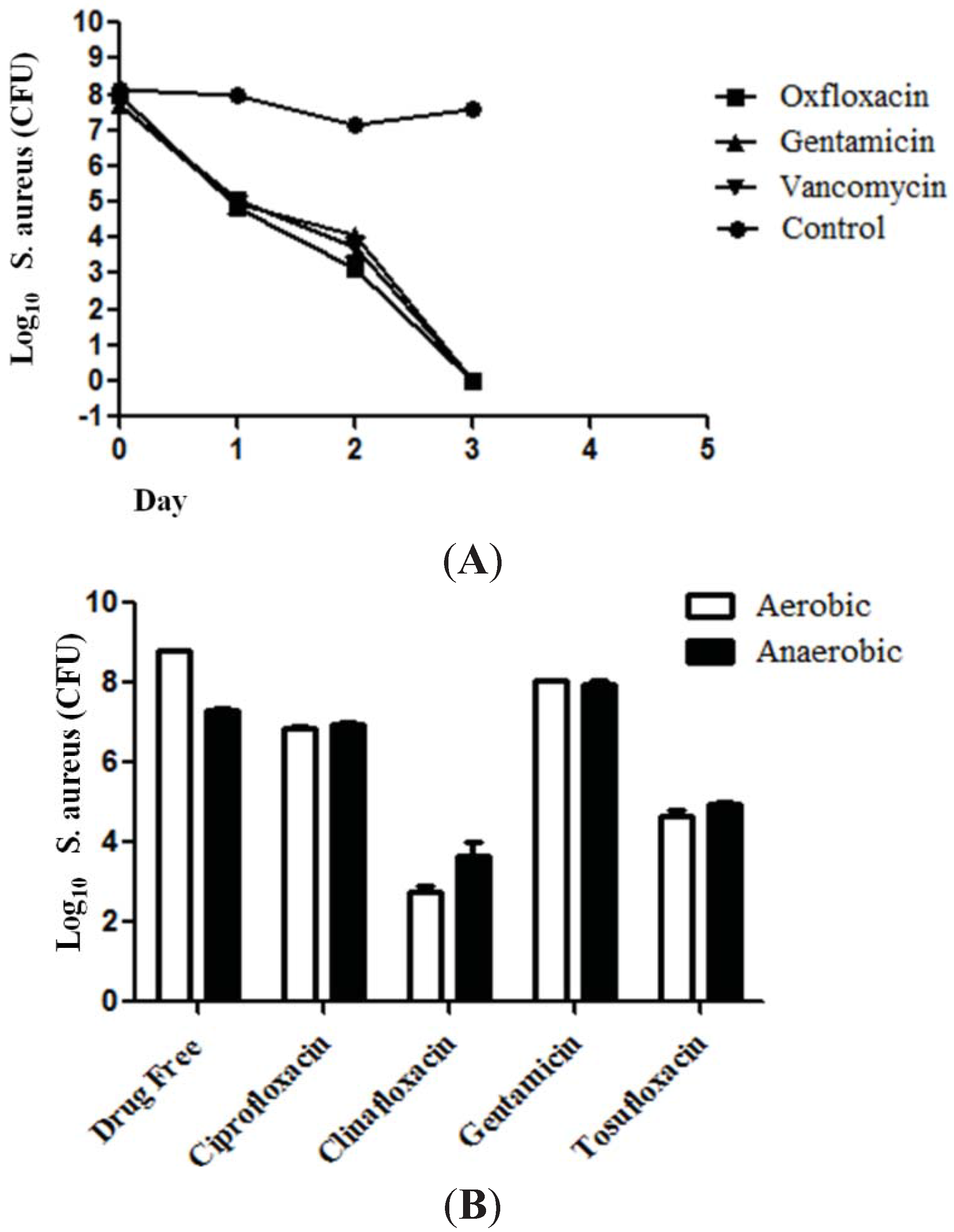
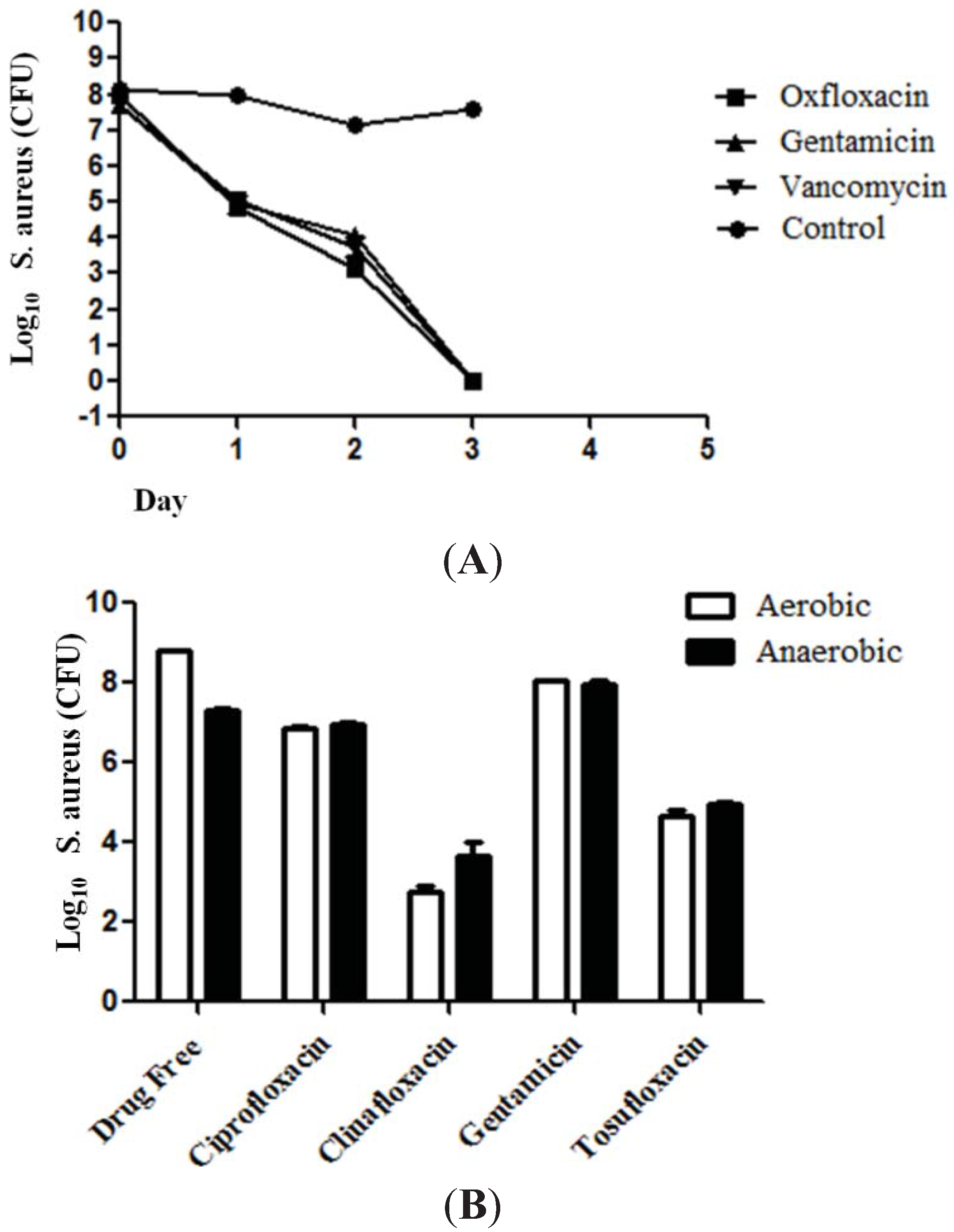
Figure 2B). We also found that
S. aureus persisters derived from other cidal antibiotics gentamicin and vancomycin could similarly be killed by tosufloxacin as those derived from ofloxacin pretreatment (
Figure 3A), and the activity of antibiotics against
S. aureus persisters was comparable in aerobic and anaerobic conditions (
Figure 3B).
Figure 3.
The effect of tosufloxacin against S. aureus persisters that survived from different cidal antibiotic treatments and comparison of the activity of antibiotics in aerobic and anaerobic environments. (A) S. aureus persisters enriched by ofloxacin, gentamycin or vancomycin were similarly killed by tosufloxacin (50 μM). The S. aureus stationary phase culture was treated with ofloxacin (10 μg/mL), gentamycin (10 μg/mL) or vancomycin (10 μg/mL) for four hours to enrich persisters. Then, the surviving persisters from the treatment were subjected to drug exposure with tosufloxacin (50 μM); (B) The activities of antibiotics were comparable in aerobic and anaerobic environments. The S. aureus stationary phase culture was exposed to 20 μM of the respective drugs and incubated for 3 days at 37 °C (aerobically and anaerobically) when the CFU was determined.
Figure 3.
The effect of tosufloxacin against S. aureus persisters that survived from different cidal antibiotic treatments and comparison of the activity of antibiotics in aerobic and anaerobic environments. (A) S. aureus persisters enriched by ofloxacin, gentamycin or vancomycin were similarly killed by tosufloxacin (50 μM). The S. aureus stationary phase culture was treated with ofloxacin (10 μg/mL), gentamycin (10 μg/mL) or vancomycin (10 μg/mL) for four hours to enrich persisters. Then, the surviving persisters from the treatment were subjected to drug exposure with tosufloxacin (50 μM); (B) The activities of antibiotics were comparable in aerobic and anaerobic environments. The S. aureus stationary phase culture was exposed to 20 μM of the respective drugs and incubated for 3 days at 37 °C (aerobically and anaerobically) when the CFU was determined.
The presence of persisters makes the treatment of many bacterial infections such as urinary tract infections, prosthetic biofilm infections very challenging. The ability to efficiently eradicate the infection without relapse will help reduce the spread of drug resistance. Since clinical drugs have relatively clear safety and pharmacokinetic profiles in humans, studies examining whether existing clinical drugs could effectively eliminate
S. aureus persisters represent a rapid and efficient approach to addressing this problem. In this study, we found that tosufloxacin had the best activity against
S. aureus persisters
in vitro among the six active drug candidates (
Table 1,
Figure 2). It is worth noting that we recently found that tosufloxacin also had high activity against
Escherichia coli persisters [
11]. Therefore, tosufloxacin may be a truly effective drug candidate against persisters of both Gram-positive and Gram-negative bacteria. Further studies are required to evaluate tosufloxacin and its combination with other antibiotics in animal models of persistent infections and to explain its unique activity against bacterial persisters.
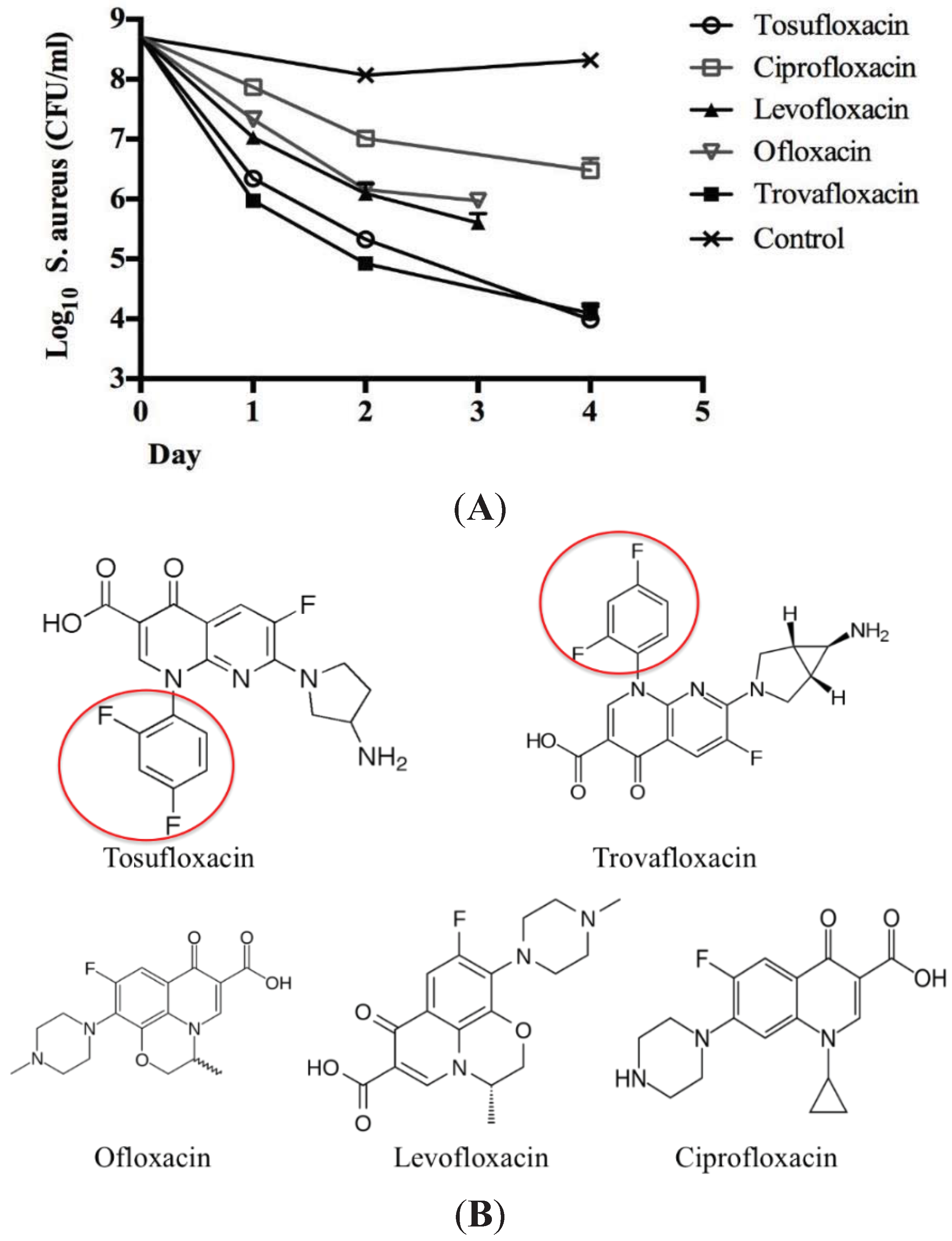
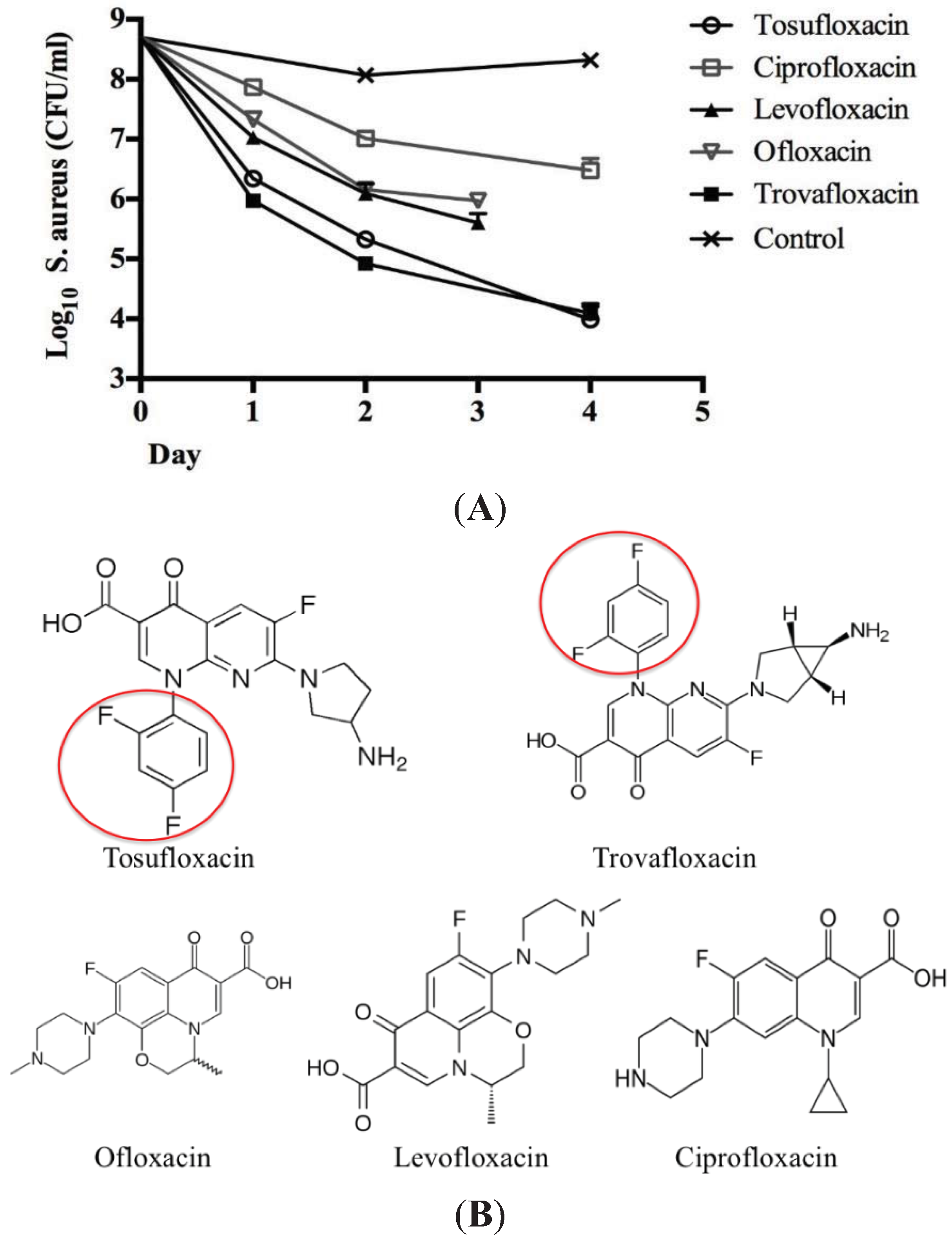
Tosufloxacin is a fluoroquinolone drug characterized by the 2,4-difluorophenyl and 3-amino-1-pyrrolidinyl groups at the quinolone nucleus. It has been reported that compounds with a 2,4-difluorophenyl group at the N-1 position in the quinolone nucleus exhibited good bactericidal activities [
12]. Here, we compared tosufloxacin and trovafloxacin which both contain the same 2,4-difluorophenyl group at the N-1 position with other quinolone drugs (ofloxacin, levofloxacin, ciprofloxacin) for their ability to kill
S. aureus persisters. We found that indeed both tosufloxacin and trovafloxacin showed higher anti-persister activity than other fluoroquinolones without the 2,4-difluorophenyl group at the N-1 position (
Figure 4A,B). Therefore, we speculate that the high activity of tosufloxacin and trovafloxacin against
S. aureus persisters may be due to the 2,4-difluorophenyl group at the N-1 position. Future structure activity studies are needed to test this possibility.
Figure 4.
Comparison of the structure and activity of tosufloxacin with the other quinolone drugs. (A) The activity of quinolone drugs (10 μM) against S. aureus persisters. S. aureus stationary phase culture was treated with ofloxacin (10 μg/mL) for 4 h to enrich persisters followed by treatment with different quinolone antibiotics. The bacterial viability was determined at different times by CFU count; (B) Structures of tosufloxacin and the other quinolone antibiotics. Tosufloxacin and trovafloxacin that have high activity against persisters both contain the 2,4-difluorophenyl group at the N-1 position, which is highlighted by the red circle and is absent in other less active quinolones.
Figure 4.
Comparison of the structure and activity of tosufloxacin with the other quinolone drugs. (A) The activity of quinolone drugs (10 μM) against S. aureus persisters. S. aureus stationary phase culture was treated with ofloxacin (10 μg/mL) for 4 h to enrich persisters followed by treatment with different quinolone antibiotics. The bacterial viability was determined at different times by CFU count; (B) Structures of tosufloxacin and the other quinolone antibiotics. Tosufloxacin and trovafloxacin that have high activity against persisters both contain the 2,4-difluorophenyl group at the N-1 position, which is highlighted by the red circle and is absent in other less active quinolones.
3. Experimental Section
S. aureus Newman, a strain that was originally isolated from a patient suffering from osteomyelitis [
13], was cultured in Tryptic soy broth (TSB) medium overnight to stationary phase. Then, the overnight culture was treated with ofloxacin (10 μg/mL) for 4 h to kill growing bacteria and enrich persisters. Finally, the persisters that survived the ofloxacin treatment were washed twice and resuspended in 3-(
N-morpholino) propanesulfonic acid (MOPS) buffer and 100 μL bacterial suspension was transferred to 96-well microplates for drug screens. The clinical drug library consisting of 1524 pharmacologically active compounds, which were either FDA-approved drugs or drugs approved for use abroad, was prepared as 10 mM stock solutions and 1 mM working stock solution in dimethyl sulfoxide (DMSO) and was arrayed in a total of 24 96-well plates [
14], leaving the first and last columns in each plate for controls. To qualitatively determine the effect of clinical drugs on
S. aureus persisters, each compound from the working stock solution (5 μL) was added to the persister cell suspension to achieve a final drug concentration of 50 μM in the drug screen. The plates were sealed and placed in a 37 °C incubator for 5 days without shaking. After 5 days of drug exposure, a 96-pin replicator was used to transfer the bacterial suspension onto TSB agar plates, to monitor the bacterial survival after drug exposure.
To more quantitatively validate the active drug candidates, colony forming unit (CFU) count was performed. The surviving persisters from the ofloxacin treatment (10 μg/mL) were dispensed into 1.5 mL Eppendorf tubes in 1 mL MOPS buffer followed by addition of drugs at a final concentration of 50 μM. After 1 to 4 day drug exposure, 100 μL bacterial suspension was removed followed by washing in PBS. Serial dilutions were spotted onto TSB agar plates to get CFU count after incubation overnight at 37 °C.




{kind=link}
{kind=link}
{kind=link}
{kind=link}