Antibiotic Prescribing in Primary Care and Antimicrobial Resistance in Patients Admitted to Hospital with Urinary Tract Infection: A Controlled Observational Pilot Study


Abstract
:1. Introduction
2. Results and Discussion

2.1. Practices and Participants

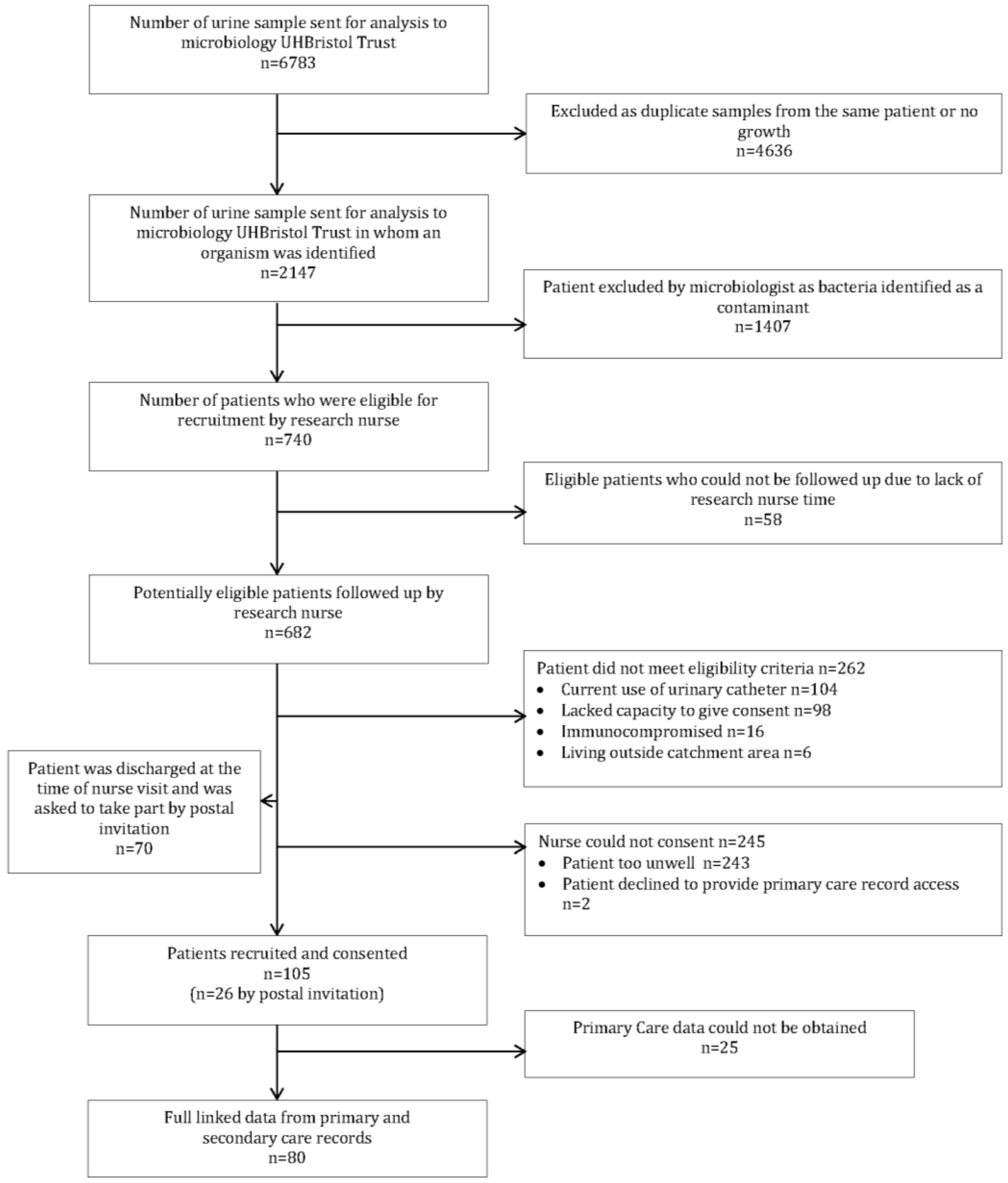{kind=link}
| Variable | n(%) n = 105 |
|---|---|
| Age (mean(SD)) | 63.4 (20.1) |
| Age category | - |
| 20–49 | 24(23) |
| 50–74 | 38(36) |
| 75–84 | 25(24) |
| 85+ | 18(17) |
| Female | 67(64) |
| Secondary care antibiotic use | 77(73) |
| Trimethoprim 1 | 63(82) |
| Co-amoxiclav 1 | 22(29) |
| Amoxicillin 1 | 66(86) |
| Nitrofurantoin 1 | 3(4) |
| Visited hospital in previous 12 months | 53(50) |
| Antibiotic use in previous 12 months | - |
| Yes | 21(20) |
| Unknown 2 | 79(75) |
| Co-morbidity | - |
| Asthma | 14(13) |
| Diabetes mellitus | 16(15) |
| COPD | 3(3) |
| History of smoking | 46(44) |
| Organism identified | n (%), n = 105 |
| Escherichia coli | 75 (71) |
| Proteus spp. | 10 (10) |
| Coliform | 20 (19) |
| Resistance (all urinary isolates) | n = 105 |
| Trimethoprim | 35 (33) |
| Amoxicillin | 25 (24) |
| Ciprofloxacin | 10 (10) |
| Antibiotic type | n (%) n = 154 a |
| Amoxicillin | 20 (13) |
| Co-amoxiclav | 16 (10) |
| Flucloxacillin | 13 (8) |
| Nitrofurantoin | 28 (18) |
| Trimethoprim | 31 (20) |
| Ciprofloxacin | 17 (11) |
| Erythromycin | 15 (10) |
| Clarithromycin | 4 (3) |
| Other | 10 (7) |
| Number of courses | n = 80 |
| 0 | 31 (39) |
| 1 | 22 (27) |
| 2 | 6 (8) |
| 3–5 | 12 (15) |
| 6+ | 9 (11) |
| Antibiotic prescribed n = 80 | Resistant n = 25 (31%) | Susceptible n = 55 (69%) | Crude OR 95% CI |
|---|---|---|---|
| Yes 49 (61) | 20 (80%) | 29 (53%) | 3.58 |
| No 31 (39) | 5 (20%) | 26 (47%) | 1.18 to 10.9 |
2.2. Discussion
2.3. Implications for Research and Clinical Practice
3. Experimental
3.1. Design, Setting and Participants
3.2. Identification of Bacteria
3.3. Microbiology Methods
3.4. Patient Recruitment and Consent
3.5. Primary Care Antibiotic Data
3.6. Outcome Measures
4. Conclusions
Acknowledgements
Authors’ Contributions
Conflicts of Interest
References
- Leung, E.; Weil, D.E.; Raviglione, M.; Nakatani, H. The WHO policy package to combat antimicrobial resistance. Bull. World Health Organ. 2011, 89, 390–392. [Google Scholar] [CrossRef]
- Infectious Diseases Society of America. Bad Bugs, no Drugs: As Antibiotic Discovery Stagnate and A Public Health Crisis Brews; Infectious Diseases Society of America: Alexandria, VA, USA, 2004. [Google Scholar]
- Standing Medical Advisory Committee. The Path of Least Resistance; Department of Health: London, UK, 1998. [Google Scholar]
- Macfarlane, J.; Holmes, W.; Macfarlane, R.; Britten, N. Influence of patients’ expectations on antibiotic management of acute lower respiratory tract illness in general practice: Questionnaire study. BMJ 1997, 315, 1211–1214. [Google Scholar] [CrossRef]
- Simpson, S.A.; Wood, F.; Butler, C.C. General practitioners’ perceptions of antimicrobial resistance: A qualitative study. J. Antimicrob. Chemother. 2007, 59, 292–296. [Google Scholar] [CrossRef]
- Hay, A.D.; Thomas, M.; Montgomery, A.; Wetherell, M.; Lovering, A.; McNulty, C.; Lewis, D.; Carron, B.; Henderson, E.; MacGowan, A. The relationship between primary care antibiotic prescribing and bacterial resistance in adults in the community: A controlled observational study using individual patient data. J. Antimicrob. Chemother. 2005, 56, 146–153. [Google Scholar] [CrossRef]
- Malhotra-Kumar, S.; Lammens, C.; Coenen, S.; van Herck, K.; Goossens, H. Effect of azithromycin and clarithromycin therapy on pharyngeal carriage of macrolide-resistant streptococci in healthy volunteers: A randomised, double-blind, placebo-controlled study. Lancet 2007, 369, 482–490. [Google Scholar] [CrossRef]
- Costelloe, C.; Lovering, A.; Montgomery, A.; Lewis, D.; McNulty, C.; Hay, A.D. Effect of antibiotic prescribing in primary care on meticillin-resistant Staphylococcus aureus carriage in community-resident adults: A controlled observational study. Int. J. Antimicrob. Agents 2011, 39, 135–141. [Google Scholar]
- Chung, A.; Perera, R.; Brueggemann, A.B.; Elamin, A.E.; Harnden, A.; Mayon-White, R.; Smith, S.; Crook, D.W.; Mant, D. Effect of antibiotic prescribing on antibiotic resistance in individual children in primary care: Prospective cohort study. Br. Med. J. 2007, 335, 429–434. [Google Scholar] [CrossRef]
- Costelloe, C.; Metcalfe, C.; Lovering, A.; Mant, D.; Hay, A.D. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: Systematic review and meta-analysis. Br. Med. J. 2010, 340, c2096. [Google Scholar] [CrossRef]
- Lipsitch, M.; Samore, M.H. Antimicrobial use and antimicrobial resistance: A population perspective. Emerg. Infect. Dis. 2002, 8, 347–354. [Google Scholar] [CrossRef]
- Butler, C.C.; Rollnick, S.; Pill, R.; Maggs-Rapport, F.; Stott, N. Understanding the culture of prescribing: Qualitative study of general practitioners’ and patients’ perceptions of antibiotics for sore throats. Br. Med. J. 1998, 317, 637–642. [Google Scholar] [CrossRef]
- Brooks, L.; Shaw, A.; Sharp, D.; Hay, A.D. Towards a better understanding of patients’ perspectives of antibiotic resistance and MRSA: A qualitative study. Fam. Pract. 2008, 25, 341–348. [Google Scholar] [CrossRef]
- World Health Organisation. European Strategic Action Plan on Antibiotic Resistance; Copenhagen, Denmark, 2011. [Google Scholar]
- Alós, J.-I.; Serrano, M.G.; Gómez-Garcés, J.-L.; Perianes, J. Antibiotic resistance of Escherichia coli from community-acquired urinary tract infections in relation to demographic and clinical data. Clin. Microbiol. Infect. 2005, 11, 199–203. [Google Scholar] [CrossRef]
- Leflon-Guibout, V.; Ternat, G.; Heym, B.; Nicolas-Chanoine, M.H. Exposure to co-amoxiclav as a risk factor for co-amoxiclav-resistant Escherichia coli urinary tract infection. J. Antimicrob. Chemother. 2002, 49, 367–371. [Google Scholar] [CrossRef]
- Pallares, R.; Gudiol, F.; Linares, J.; Ariza, J.; Rufi, G.; Murgui, L.; Dorca, J.; Viladrich, P.F. Risk factors and response to antibiotic therapy in adults with bacteremic pneumonia caused by penicillin-resistant pneumococci. N. Engl. J. Med. 1987, 317, 18–22. [Google Scholar] [CrossRef]
- BSAC Microbiology Testing Guidelines. Available online: http://bsac.org.uk/wp-content/uploads/2012/02/version215-nov-2003-.pdf (accessed on 1 October 2010).
- Arain, M.; Campbell, M.J.; Cooper, C.L.; Lancaster, G.A. What is a pilot or feasibility study? A review of current practice and editorial policy. BMC Med. Res. Methodol. 2010, 10, e67. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Costelloe, C.; Williams, O.M.; Montgomery, A.A.; Dayan, C.; Hay, A.D. Antibiotic Prescribing in Primary Care and Antimicrobial Resistance in Patients Admitted to Hospital with Urinary Tract Infection: A Controlled Observational Pilot Study. Antibiotics 2014, 3, 29-38. https://doi.org/10.3390/antibiotics3010029
Costelloe C, Williams OM, Montgomery AA, Dayan C, Hay AD. Antibiotic Prescribing in Primary Care and Antimicrobial Resistance in Patients Admitted to Hospital with Urinary Tract Infection: A Controlled Observational Pilot Study. Antibiotics. 2014; 3(1):29-38. https://doi.org/10.3390/antibiotics3010029
Chicago/Turabian StyleCostelloe, Ceire, O. Martin Williams, Alan A. Montgomery, Colin Dayan, and Alastair D. Hay. 2014. "Antibiotic Prescribing in Primary Care and Antimicrobial Resistance in Patients Admitted to Hospital with Urinary Tract Infection: A Controlled Observational Pilot Study" Antibiotics 3, no. 1: 29-38. https://doi.org/10.3390/antibiotics3010029
APA StyleCostelloe, C., Williams, O. M., Montgomery, A. A., Dayan, C., & Hay, A. D. (2014). Antibiotic Prescribing in Primary Care and Antimicrobial Resistance in Patients Admitted to Hospital with Urinary Tract Infection: A Controlled Observational Pilot Study. Antibiotics, 3(1), 29-38. https://doi.org/10.3390/antibiotics3010029