

Activity of β-Lactamase Inhibitor Combinations Against Enterobacterales Isolated from Patients with Intra-Abdominal Infection from United States Medical Centres (2019–2023)
 ,
,
Abstract
1. Introduction
2. Results
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Organism Collection
5.2. Susceptibility Testing
5.3. Βeta-Lactamase Screening
5.4. Characterization of Aztreonam-Avibactam Resistant Isolates
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bonomo, R.A.; Chow, A.W.; Edwards, M.S.; Humphries, R.; Tamma, P.D.; Abrahamian, F.M.; Bessesen, M.; Dellinger, E.P.; Goldstein, E.; Hayden, M.K.; et al. 2024 Clinical Practice Guideline Update by the Infectious Diseases Society of America on Complicated Intra-abdominal Infections: Risk Assessment, Diagnostic Imaging, and Microbiological Evaluation in Adults, Children, and Pregnant People. Clin. Infect. Dis. 2024, 79, S81–S87. [Google Scholar] [CrossRef] [PubMed]
- Huston, J.M.; Barie, P.S.; Dellinger, E.P.; Forrester, J.D.; Duane, T.M.; Tessier, J.M.; Sawyer, R.G.; Cainzos, M.A.; Rasa, K.; Chipman, J.G.; et al. The Surgical Infection Society Guidelines on the Management of Intra-Abdominal Infection: 2024 Update. Surg. Infect. 2024, 25, 419–435. [Google Scholar] [CrossRef] [PubMed]
- Paul, M.; Carrara, E.; Retamar, P.; Tängdén, T.; Bitterman, R.; Bonomo, R.A.; de Waele, J.; Daikos, G.L.; Akova, M.; Harbarth, S.; et al. European Society of Clinical Microbiology and Infectious Diseases (ESCMID) guidelines for the treatment of infections caused by multidrug-resistant Gram-negative bacilli (endorsed by European society of intensive care medicine). J. Clin. Microbiol. Infect. 2022, 28, 521–547. [Google Scholar] [CrossRef] [PubMed]
- Chong, Y.P.; Bae, I.G.; Lee, S.R.; Chung, J.W.; Jun, J.B.; Choo, E.J.; Moon, S.Y.; Lee, M.S.; Jeon, M.H.; Song, E.H.; et al. Clinical and economic consequences of failure of initial antibiotic therapy for patients with community-onset complicated intra-abdominal infections. PLoS ONE 2015, 10, e0119956. [Google Scholar] [CrossRef] [PubMed]
- Kong, W.; Deng, T.; Li, S.; Shu, Y.; Wu, Y. Efficacy, safety, and tolerability of antimicrobial agents for complicated intra-abdominal infection: A systematic review and network meta-analysis. BMC Infect. Dis. 2023, 23, 256. [Google Scholar] [CrossRef] [PubMed]
- De Pascale, G.; Carelli, S.; Vallecoccia, M.S.; Cutuli, S.L.; Taccheri, T.; Montini, L.; Bello, G.; Spanu, T.; Tumbarello, M.; Cicchetti, A.; et al. Risk factors for mortality and cost implications of complicated intra-abdominal infections in critically ill patients. J. Crit. Care 2019, 50, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Tamma, P.D.; Heil, E.L.; Justo, J.A.; Mathers, A.J.; Satlin, M.J.; Bonomo, R.A. Infectious Diseases Society of America 2024 Guidance on the Treatment of Antimicrobial-Resistant Gram-Negative Infections. Clin. Infect. Dis. 2024, ciae403. [Google Scholar] [CrossRef] [PubMed]
- Sader, H.; Kimbrough, J.H.; Doyle, T.; Winkler, M.L.; Castanheira, M. Frequency, Antimicrobial Susceptibility, and Molecular Characterization of Carbapenem-Resistant Enterobacterales Stratified by United States Census Divisions: Results From the INFORM Program (2018–2022). Open Forum Infect. Dis. 2025, 12, ofaf005. [Google Scholar] [CrossRef] [PubMed]
- Carmeli, Y.; Cisneros, J.M.; Paul, M.; Daikos, G.L.; Wang, M.; Torre-Cisneros, J.; Singer, G.; Titov, I.; Gumenchuk, I.; Zhao, Y.; et al. Aztreonam-avibactam versus meropenem for the treatment of serious infections caused by Gram-negative bacteria (REVISIT): A descriptive, multinational, open-label, phase 3, randomised trial. Lancet Infect. Dis. 2025, 25, 218–230. [Google Scholar] [CrossRef] [PubMed]
- CLSI M100Ed35; Performance Standards for Antimicrobial Susceptability Testing; 35 the Informational Supplement. Clinical and Laboratory Standards Institute: Berwyn, PA, USA, 2025; Volume 100.
- EUCAST. Breakpoint Tables for Interpretation of MICs and Zone Diameters Version 15.0; European Committee on Antimicro-Bial Susceptibility Testing: Vaxjo, Sweden, 2025. [Google Scholar]
- Sader, H.S.; Castanheira, M.; Flamm, R.K.; Huband, M.D.; Jones, R.N. Ceftazidime-Avibactam Activity against Aerobic Gram Negative Organisms Isolated from Intra-Abdominal Infections in United States Hospitals, 2012–2014. Surg. Infect. 2016, 17, 473–478. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, J.N.; Lodise, T.P. New Perspectives on Antimicrobial Agents: Imipenem-Relebactam. Antimicrob. Agents Chemother. 2022, 66, e0025622. [Google Scholar] [CrossRef] [PubMed]
- Castanheira, M.; Simner, P.J.; Bradford, P.A. Extended-spectrum β-lactamases: An update on their characteristics, epidemiology and detection. JAC Antimicrob. Resist. 2021, 3, dlab092. [Google Scholar] [CrossRef] [PubMed]
- Castanheira, M.; Kimbrough, J.H.; DeVries, S.; Mendes, R.E.; Sader, H.S. Trends of beta-lactamase occurrence among Escherichia coli and Klebsiella pneumoniae in United States hospitals during a 5-year period and activity of antimicrobial agents against isolates stratified by beta-lactamase type. Open Forum Infect. Dis. 2023, 10, ofad038. [Google Scholar] [CrossRef] [PubMed]
- CLSI M07Ed12; Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria that Grow Aerobically. Clinical and Laboratory Standards Institute: Berwyn, PA, USA, 2024; Volume 7.
- Bankevich, A.; Nurk, S.; Antipov, D.; Gurevich, A.A.; Dvorkin, M.; Kulikov, A.S.; Lesin, V.M.; Nikolenko, S.I.; Pham, S.; Prjibelski, A.D.; et al. SPAdes: A new genome assembly algorithm and its applications to single-cell sequencing. J. Comput. Biol. 2012, 19, 455–477. [Google Scholar] [CrossRef] [PubMed]
- Mendes, R.E.; Jones, R.N.; Woosley, L.N.; Cattoir, V.; Castanheira, M. Application of next-generation sequencing for characterization of surveillance and clinical trial isolates: Analysis of the distribution of beta-lactamase resistance genes and lineage background in the United States. Open Forum Infect. Dis. 2019, 6, S69–S78. [Google Scholar] [CrossRef] [PubMed]
- Mendes, R.E.; Doyle, T.B.; Streit, J.M.; Arhin, F.F.; Sader, H.S.; Castanheira, M. Investigation of mechanisms responsible for decreased susceptibility of aztreonam/avibactam activity in clinical isolates of Enterobacterales collected in Europe, Asia and Latin America in 2019. J. Antimicrob. Chemother. 2021, 76, 2833–2838. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Antimicrobial Agent (No. of Isolates) | mg/L | CLSI a | EUCAST a | |||||
|---|---|---|---|---|---|---|---|---|
| MIC50 | MIC90 | %S | %I | %R | %S | %I | %R | |
| All Enterobacterales (2036) | ||||||||
| Aztreonam-avibactam | ≤0.03 | 0.12 | 99.9 b | 0.1 | <0.1 | 99.9 | 0.1 | |
| Ceftazidime-avibactam | 0.12 | 0.25 | 99.9 | 0.1 | 99.9 | 0.1 | ||
| Meropenem-vaborbactam | 0.03 | 0.06 | 99.9 | 0.0 | 0.1 | 99.9 | 0.1 | |
| Imipenem-relebactam c | 0.12 | 0.5 | 96.1 | 3.4 | 0.5 | 99.5 | 0.5 | |
| Ceftolozane-tazobactam | 0.25 | 1 | 93.0 | 1.3 | 5.7 | 93.0 | 7.0 | |
| Piperacillin-tazobactam | 2 | 16 | 87.2 | 2.9 d | 9.9 | 87.2 | 12.8 | |
| Ampicillin-sulbactam | 8 | 64 | 51.6 | 16.3 | 32.1 | |||
| Aztreonam | 0.12 | >16 | 84.6 | 2.1 | 13.3 | 82.3 | 2.3 | 15.4 |
| Ceftriaxone | ≤0.06 | >8 | 81.6 | 0.8 | 17.6 | 81.6 | 0.8 | 17.6 |
| Ceftazidime | 0.25 | 32 | 85.6 | 1.4 | 13.1 | 81.4 | 4.2 | 14.4 |
| Cefepime | 0.06 | 4 | 89.4 | 3.3 d | 7.3 | 87.4 | 3.7 | 8.8 |
| Meropenem | 0.03 | 0.06 | 99.2 | 0.1 | 0.7 | 99.3 | 0.3 | 0.3 |
| Imipenem | ≤0.12 | 1 | 93.9 | 4.6 | 1.5 | 98.5 | 0.9 | 0.6 |
| Levofloxacin | 0.06 | 8 | 82.7 | 1.9 | 15.3 | 82.7 | 1.9 | 15.3 |
| Gentamicin | 0.5 | 1 | 92.7 | 0.3 | 6.9 | 92.7 e | 7.3 | |
| Amikacin | 2 | 4 | 95.3 | 3.6 | 1.1 | 98.9 e | 1.1 | |
| Tigecycline | 0.25 | 1 | 97.2 b | 2.7 | <0.1 | 86.3 f | 13.7 | |
| Colistin | 0.25 | >8 | 87.0 | 13.0 | 87.0 | 13.0 | ||
| MDR (436) g | ||||||||
| Aztreonam-avibactam | 0.06 | 0.5 | 99.3 b | 0.5 | 0.2 | 99.3 | 0.7 | |
| Ceftazidime-avibactam | 0.25 | 1 | 99.3 | 0.7 | 99.3 | 0.7 | ||
| Meropenem-vaborbactam | 0.03 | 0.06 | 99.5 | 0.0 | 0.5 | 99.5 | 0.5 | |
| Imipenem-relebactam c | 0.12 | 0.25 | 99.4 | 0.0 | 0.6 | 99.4 | 0.6 | |
| Ceftolozane-tazobactam | 0.5 | 16 | 67.9 | 5.7 | 26.4 | 67.9 | 32.1 | |
| Piperacillin-tazobactam | 8 | >128 | 50.2 | 8.3 d | 41.5 | 50.2 | 49.8 | |
| Ampicillin-sulbactam | 64 | >64 | 4.6 | 17.9 | 77.5 | |||
| Aztreonam | >16 | >16 | 35.3 | 6.4 | 58.3 | 30.5 | 4.8 | 64.7 |
| Ceftriaxone | >8 | >8 | 29.4 | 1.6 | 69.0 | 29.4 | 1.6 | 69.0 |
| Ceftazidime | 16 | >32 | 38.8 | 4.6 | 56.7 | 31.2 | 7.6 | 61.2 |
| Cefepime | 2 | >32 | 56.0 | 12.6 d | 31.4 | 47.9 | 14.9 | 37.2 |
| Meropenem | 0.03 | 0.12 | 96.1 | 0.7 | 3.2 | 96.8 | 1.6 | 1.6 |
| Levofloxacin | 1 | 32 | 46.9 | 4.6 | 48.5 | 46.9 | 4.6 | 48.5 |
| Gentamicin | 0.5 | >16 | 70.2 | 0.9 | 28.9 | 70.2 e | 29.8 | |
| Amikacin | 2 | 8 | 88.1 | 7.6 | 4.4 | 95.6 e | 4.4 | |
| Tigecycline | 0.25 | 1 | 95.9 b | 4.1 | 0.0 | 86.5 f | 13.5 | |
| Colistin | 0.25 | 0.5 | 93.8 | 6.2 | 93.8 | 6.2 | ||
| β-lactamase producers (207) h | ||||||||
| Aztreonam-avibactam | 0.06 | 0.25 | 99.0 b | 0.5 | 0.5 | 99.0 | 1.0 | |
| Ceftazidime-avibactam | 0.12 | 0.5 | 99.0 | 1.0 | 99.0 | 1.0 | ||
| Meropenem-vaborbactam | 0.03 | 0.03 | 99.0 | 0.0 | 1.0 | 99.0 | 1.0 | |
| Imipenem-relebactam c | 0.12 | 0.12 | 98.4 | 0.0 | 1.6 | 98.4 | 1.6 | |
| Ceftolozane-tazobactam | 0.5 | 16 | 82.0 | 2.4 | 15.5 | 82.0 | 18.0 | |
| Piperacillin-tazobactam | 4 | >128 | 70.0 | 8.2 d | 21.7 | 70.0 | 30.0 | |
| Ampicillin-sulbactam | 32 | >64 | 16.4 | 17.4 | 66.2 | |||
| Aztreonam | >16 | >16 | 9.7 | 14.0 | 76.3 | 0.5 | 9.2 | 90.3 |
| Ceftriaxone | >8 | >8 | 0.0 | 0.0 | 100.0 | 0.0 | 0.0 | 100.0 |
| Ceftazidime | 16 | >32 | 20.3 | 9.7 | 70.0 | 2.9 | 17.4 | 79.7 |
| Cefepime | 32 | >32 | 17.4 | 16.9 d | 65.7 | 13.0 | 12.1 | 74.9 |
| Meropenem | 0.03 | 0.06 | 94.2 | 0.5 | 5.3 | 94.7 | 1.9 | 3.4 |
| Levofloxacin | 8 | 32 | 32.9 | 4.8 | 62.3 | 32.9 | 4.8 | 62.3 |
| Gentamicin | 1 | >16 | 63.8 | 1.4 | 34.8 | 63.8 e | 36.2 | |
| Amikacin | 2 | 8 | 83.1 | 9.2 | 7.7 | 92.3 e | 7.7 | |
| Tigecycline | 0.25 | 1 | 96.6 b | 3.4 | 0.0 | 89.9 f | 10.1 | |
| Colistin | 0.25 | 0.25 | 99.0 | 1.0 | 99.0 | 1.0 | ||
| CRE (15) | ||||||||
| Aztreonam-avibactam | 0.5 | 8 | 86.7 b | 6.7 | 6.7 | 86.7 | 13.3 | |
| Ceftazidime-avibactam | 1 | 32 | 86.7 | 13.3 | 86.7 | 13.3 | ||
| Meropenem-vaborbactam | 0.5 | 32 | 86.7 | 0.0 | 13.3 | 86.7 | 13.3 | |
| Imipenem-relebactam | 0.12 | 4 | 86.7 d | 0.0 | 13.3 | 86.7 d | 13.3 | |
| Cefiderocol i | 2 | 4 | 93.3 | 0.0 | 6.7 | 80.0 | 20.0 | |
| Levofloxacin | 16 | 32 | 40.0 | 6.7 | 53.3 | 40.0 | 6.7 | 53.3 |
| Gentamicin | 1 | 16 | 80.0 | 6.7 | 13.3 | 80.0 | 20.0 | |
| Amikacin | 4 | 32 | 73.3 | 13.3 | 13.3 | 86.7 | 13.3 | |
| Tigecycline | 0.5 | 1 | 100.0 | 0.0 | 0.0 | 80.0 | 20.0 | |
| Organism/Group | % Susceptible a (MIC50/90 in mg/L) | |||||||
|---|---|---|---|---|---|---|---|---|
| (No. of Isolates) | ATM-AVI | CAZ-AVI | MEM-VAB | IMI-REL | TOL-TAZ | PIP-TAZ | AMP-SUL | Ceftriaxone |
| Enterobacterales (2036) | 99.9 (≤0.03/0.12) | 99.9 (0.12/0.25) | 99.9 (0.03/0.06) | 96.1 (0.12/0.5) | 93.0 (0.25/1) | 87.2 (2/16) | 51.6 (8/64) | 81.6 (≤0.06/>8) |
| MDR (436) | 99.3 (0.06/0.5) | 99.3 (0.25/1) | 99.5 (/0.030.06) | 99.2 (0.12/0.25) | 67.9 (0.5/16) | 50.2 (8/>128) | 4.6 (64/>64) | 29.4 (>8/>8) |
| PIP-TAZ-NS (260) | 98.8 (0.12/1) | 98.8 (0.5/1) | 99.2 (0.03/0.06) | 98.7 (0.12/0.25) | 46.2 (4/>16) | -- | 1.9 (>64/>64) | 28.1 (>8/>8) |
| β-Lactamase producers (207) b | 99.0 (0.06/0.25) | 99.0 (0.12/0.5) | 99.0 (0.03/0.03) | 98.4 (0.12/0.12) | 82.0 (0.5/16) | 70.0 (4/>128) | 16.4 (32/>64) | 0.0 (>8/>8) |
| CRE (15) | 86.7 (0.5/8) | 86.7 (1/32) | 86.7 (0.5/32) | 86.7 (0.12/4) | 0.0 (>16/>16) | 0.0 (>128/>128) | 0.0 (>64/>64) | 0.0 (>8/>8) |
| E. coli (958) | 99.8 (≤0.03/0.12) | 99.8 (0.12/0.25) | 99.8 (≤0.015/0.03) | 99.6 (0.12/0.12) | 97.9 (0.25/0.5) | 93.4 (2/8) | 54.2 (8/64) | 83.6 (≤0.06/>8) |
| K. pneumoniae (380) | 100.0 (≤0.03/0.12) | 100.0 (0.12/0.25) | 100.0 (0.03/0.03) | 100.0 (0.12/0.25) | 96.6 (0.25/1) | 86.8 (4/16) | 73.2 (8/64) | 87.4 (≤0.06/>8) |
| E. cloacae complex (199) | 99.5 (0.06/1) | 99.5 (0.25/1) | 100.0 (0.03/0.06) | 100.0 (0.12/0.25) | 67.0 (0.5/16) | 61.3 (4/>128) | 12.6 (64/>64) | 57.3 (0.5/>8) |
| Morganellaceae (135) c | 100.0 (≤0.03/≤0.03) | 100.0 (0.06/0.06) | 100.0 (0.06/0.12) | 35.8 (2/2) | 99.3 (0.5/0.5) | 100.0 (0.25/1) | 59.3 (2/32) | 85.2 (≤0.06/8) |
| K. oxytoca (88) | 100.0 (≤0.03/0.06) | 100.0 (0.12/0.25) | 100.0 (0.03/0.03) | 100.0 (0.12/0.25) | 97.7 (0.25/0.5) | 94.3 (2/8) | 34.1 (16/32) | 90.9 (≤0.06/0.5) |
| C. freundii complex (79) | 100.0 (0.06/0.25) | 100.0 (0.12/0.5) | 100.0 (0.03/0.03) | 100.0 (0.12/0.12) | 75.6 (0.25/16) | 69.6 (4/128) | 57.0 (8/>64) | 72.2 (0.25/>8) |
| S. marcescens (65) | 100.0 (0.12/0.25) | 100.0 (0.25/0.5) | 100.0 (0.06/0.06) | 100.0 (0.5/1) | 96.9 (0.5/1) | 92.3 (2/8) | 7.7 (64/>64) | 89.2 (0.5/2) |
| Other species (132) d | 100.0 (0.06/0.25) | 100.0 (0.12/0.5) | 100.0 (0.03/0.06) | 100.0 (0.12/0.25) | 84.8 (0.25/8) | 72.7 (4/64) | 51.5 (8/64) | 78.8 (0.12/>8) |
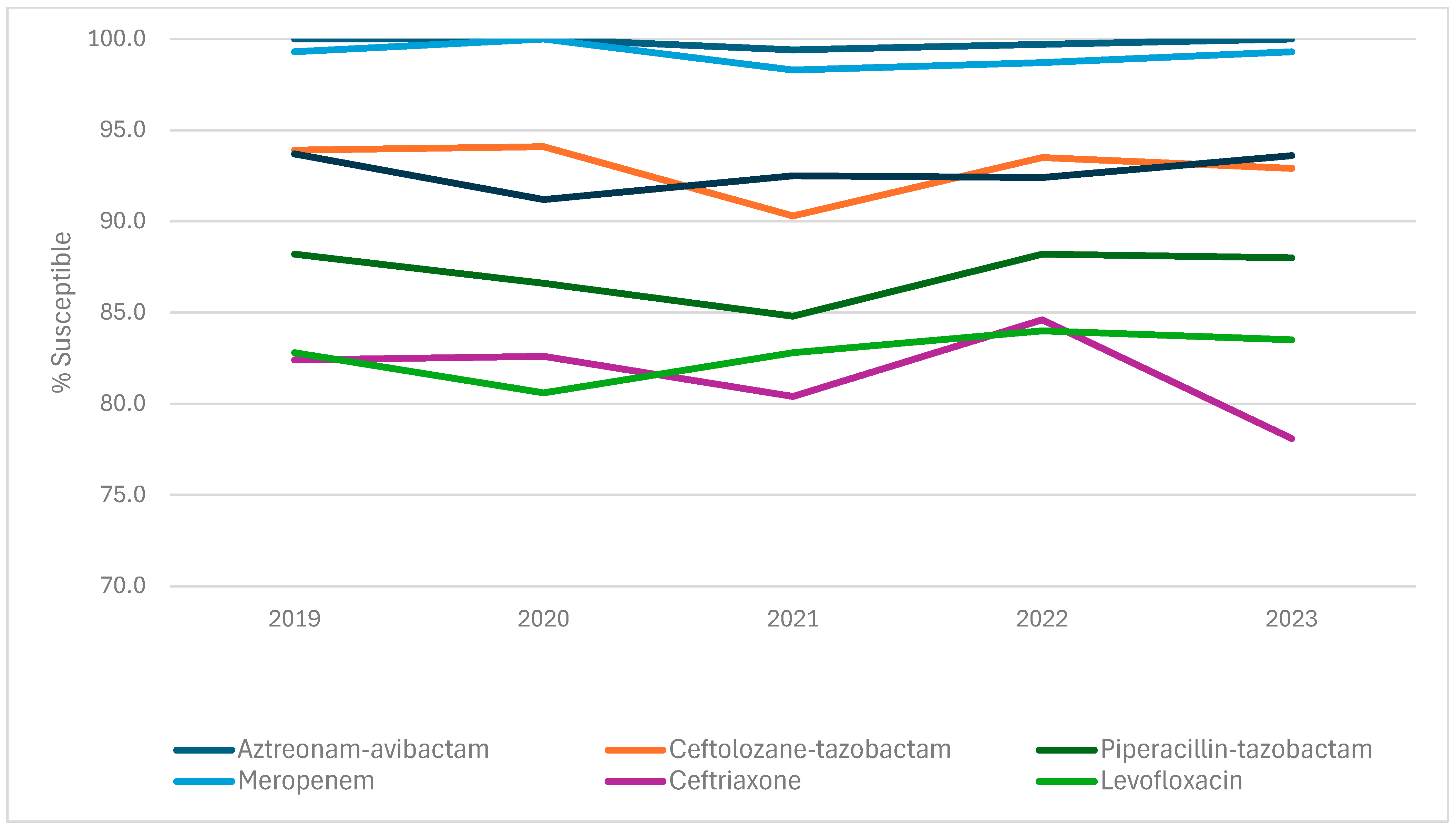
| Antimicrobial | % Susceptible (CLSI) by Year | ||||
|---|---|---|---|---|---|
| agent | 2019 | 2020 | 2021 | 2022 | 2023 |
| Aztreonam-avibactam | 100.0 | 100.0 | 99.4 | 99.7 | 100.0 |
| Ceftazidime-avibactam | 100.0 | 100.0 | 99.4 | 99.7 | 100.0 |
| Meropenem-vaborbactam | 100.0 | 100.0 | 99.7 | 99.7 | 100.0 |
| Imipenem-relebactam | - a | - a | 94.1 | 96.3 | 95.5 |
| Ceftolozane-tazobactam | 93.9 | 94.1 | 90.3 | 93.5 | 92.9 |
| Piperacillin-tazobactam | 88.2 | 86.6 | 84.8 | 88.2 | 88.0 |
| Meropenem | 99.3 | 100.0 | 98.3 | 98.7 | 99.3 |
| Ceftriaxone | 82.4 | 82.6 | 80.4 | 84.6 | 78.1 |
| Levofloxacin | 82.8 | 80.6 | 82.8 | 84.0 | 83.5 |
| Gentamicin | 93.7 | 91.2 | 92.5 | 92.4 | 93.6 |
| Organisms/β-Lactamase | No. of Isolates |
|---|---|
| Citrobacter freundii species complex | 1 |
| CMY-181 | 1 |
| Enterobacter cloacae species complex | 10 |
| CTX-M-15 | 1 |
| CTX-M-15, OXA-1/30 | 3 |
| SHV-12 | 5 |
| KPC-2 | 1 |
| Escherichia coli | 148 |
| CMY-2 | 16 |
| CMY-2, CTX-M-15 | 1 |
| CMY-42, CTX-M-15, OXA-1/30 | 1 |
| CMY-44-like, CTX-M-27 | 1 |
| CTX-M-1 | 1 |
| CTX-M-115 | 1 |
| CTX-M-14 | 11 |
| CTX-M-15 | 25 |
| CTX-M-15, CTX-M-33 | 1 |
| CTX-M-15, NDM-5, OXA-1/30 | 2 |
| CTX-M-15, OXA-1/30 | 38 |
| CTX-M-15, OXA-1/30, TEM-169 | 1 |
| CTX-M-24 | 2 |
| CTX-M-27 | 30 |
| CTX-M-55 | 13 |
| CTX-M-64 | 1 |
| DHA-1 | 1 |
| SHV-7 | 1 |
| KPC-3 | 1 |
| Klebsiella oxytoca | 1 |
| KPC-2 | 1 |
| Klebsiella pneumoniae | 47 |
| CMY-2 | 2 |
| CTX-M-15 | 14 |
| CTX-M-15, OXA-1/30 | 17 |
| CTX-M-15, OXA-1/30, SHV-7 | 1 |
| CTX-M-15, SHV-27 | 1 |
| CTX-M-27 | 1 |
| CTX-M-3 | 3 |
| KPC-2, SHV-12 | 1 |
| KPC-3 | 2 |
| KPC-3, SHV-12 | 1 |
| SHV-12, DHA-1 | 1 |
| SHV-27 | 1 |
| SHV-2-like | 1 |
| SHV-7 | 1 |
| Grand Total | 207 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sader, H.S.; Kimbrough, J.H.; Winkler, M.L.; Mendes, R.E.; Castanheira, M. Activity of β-Lactamase Inhibitor Combinations Against Enterobacterales Isolated from Patients with Intra-Abdominal Infection from United States Medical Centres (2019–2023). Antibiotics 2025, 14, 544. https://doi.org/10.3390/antibiotics14060544
Sader HS, Kimbrough JH, Winkler ML, Mendes RE, Castanheira M. Activity of β-Lactamase Inhibitor Combinations Against Enterobacterales Isolated from Patients with Intra-Abdominal Infection from United States Medical Centres (2019–2023). Antibiotics. 2025; 14(6):544. https://doi.org/10.3390/antibiotics14060544
Chicago/Turabian StyleSader, Helio S., John H. Kimbrough, Marisa L. Winkler, Rodrigo E. Mendes, and Mariana Castanheira. 2025. "Activity of β-Lactamase Inhibitor Combinations Against Enterobacterales Isolated from Patients with Intra-Abdominal Infection from United States Medical Centres (2019–2023)" Antibiotics 14, no. 6: 544. https://doi.org/10.3390/antibiotics14060544
APA StyleSader, H. S., Kimbrough, J. H., Winkler, M. L., Mendes, R. E., & Castanheira, M. (2025). Activity of β-Lactamase Inhibitor Combinations Against Enterobacterales Isolated from Patients with Intra-Abdominal Infection from United States Medical Centres (2019–2023). Antibiotics, 14(6), 544. https://doi.org/10.3390/antibiotics14060544