Abstract
We investigated the effect of combination aminoglycoside and vancomycin local antibiotic treatment compared to aminoglycoside alone in the surgical management of bone infection. Data including patient demographics, type of surgery, microbiological characteristics, BACH score, duration of antibiotic treatment and clinical outcomes were collected. Failure of therapy was a composite of recurrence of infection, continued or new antimicrobial therapy, or reoperation with suspected or confirmed infection at one year after index surgery. A total of 266 patients met the inclusion criteria. 252 patients reached the final follow-up and were included in the final analysis. 113 patients had treatment with aminoglycoside alone and 139 patients had combination aminoglycoside and vancomycin. There was no difference in the failure rate between groups; 10/113 (8.8%) in the aminoglycoside alone and 12/139 (8.6%) in the combination group, p = 0.934. Multivariate analysis showed that there was no added benefit of combination therapy (OR 1.54: 95% CI 0.59–4.04, p = 0.38). BACH score and low BMI were associated with increased risk of failure (BACH OR 3.49: 95% CI 1.13–10.76, p = 0.03; Low BMI OR 0.91: 95% CI 0.84–0.99, p = 0.037). The form of the carrier material (pellets or injectable paste) had no effect on failure rate (p = 0.163). The presence of aminoglycoside resistance had no effect on failure rate (OR 0.39: 95% CI 0.05–3.01, p = 0.37). Clinical outcome was not improved by the addition of vancomycin to aminoglycoside alone as local therapy for the management of bone infection.
1. Introduction
Osteomyelitis and fracture-related infection (FRI) cause significant morbidity, often requiring surgical debridement and medical therapy with a combination of local and systemic antibiotic therapy. Local antibiotics delivered directly to the site of infection at the time of surgery achieve high tissue concentrations with limited risk of systemic side effects [1,2,3].
Local implantation of aminoglycosides (gentamicin and tobramycin) provides levels well above the minimum inhibitory concentration (MIC) of typical infecting organisms and may be sufficient on its own [1,4,5]. Clinical use of local aminoglycosides began over 40 years ago, initially delivered with non-absorbable beads made of polymethylmethacrylate cement (PMMA) [2,6]. Walenkamp [7] popularized their use in the management of chronic osteomyelitis, but more recently, absorbable carriers (mainly inorganic salts and ceramics) have been used in clinical series managing osteomyelitis and fracture-related infections [8,9,10,11,12]. These studies have shown that local antibiotics can effectively fill dead spaces with high success rates. Rodham et al. [9] studied osteomyelitis after fracture and demonstrated that the recurrence rate was reduced from 17.6% to 9.8% with the use of local antibiotics (p = 0.01). Similarly, McNally et al., in a study of 433 FRIs, showed that treatment failed in 18.7% of those treated without local antimicrobials, but this reduced to 10% when local antibiotics (predominantly aminoglycoside alone) were used (hazard ratio 0.48; 95% confidence interval 0.29–0.81) [13].
Aminoglycosides, including gentamicin, display concentration-dependent killing, whilst vancomycin exhibits time-dependent killing [14,15]. Also, vancomycin is solely active against Gram-positive organisms, whereas aminoglycosides have a broader activity. These differences in mechanism of action may have important implications for the efficacy of these drugs when delivered locally, as a single implantation, into the infected bone. The relative efficacy of single-agent aminoglycoside versus combination local antibiotics has not previously been studied.
The rationale for this study was based on the principle that we should try to reduce unnecessary use of antimicrobials. No previous study has shown improved efficacy with the addition of glycopeptides to aminoglycoside alone in local therapy of bone and joint infection. In theory, adding vancomycin may increase the effectiveness against Gram-positive organisms which could be resistant to aminoglycoside. However, the very high levels of aminoglycoside achieved in local therapy may negate this potential advantage. In our previous study, local aminoglycoside alone was highly effective and laboratory-measured resistance to gentamicin did not affect outcome [12]. This retrospective study evaluated the effect of combination aminoglycoside and vancomycin local antibiotic treatment compared to aminoglycoside alone in the surgical management of bone infection.
2. Results
2.1. Patient Demographics
A total of 1145 patients with bone and joint infections were reviewed. Of these, 441 received local antibiotic therapy; 266 had osteomyelitis or fracture-related infection, with local antimicrobial therapy and were included for analysis. After surgery, nine patients died from non-infectious causes before the outcome endpoint at 12 months and were excluded. Five patients were lost to follow-up and were excluded from analysis. A total of 252 patients were included in the final analysis, with a minimum of 12 months follow-up.
In total, 113 patients had treatment with aminoglycoside alone (gentamicin 92; tobramycin 9, gentamicin and tobramycin 12), and 139 patients had a combination of aminoglycoside and vancomycin (vancomycin and gentamicin 109; vancomycin, gentamicin and tobramycin 30).
Overall, the study cohort was a middle-aged population (median age of the aminoglycoside alone cohort was 57 years (interquartile range: 40–66) and in the combination aminoglycoside and vancomycin cohort was 52 years (interquartile range: 37–62)) with excision of osteomyelitis being the most common surgical intervention. Infection was present in 255 bones in 252 patients (98 tibia, 65 femur, 23 humerus, 17 fibula, 14 calcanei, 8 ulnae, 6 metatarsals, 5 radii, 5 ankle fusions, 4 pelvic bones, 3 wrists, 2 patellae, 2 hips, one each of phalanx, scapula and metacarpal). The most frequently isolated organism was Staphylococcus aureus, followed by non-pseudomonas Gram-negative organisms. Rates of confirmed gentamicin resistance and polymicrobial infection were similar between the two groups. The characteristics are presented in Table 1.

Table 1.
Patient Demographics.
2.2. Patient Outcomes
There was no difference in the rate of the primary outcome (failure to eradicate infection) between the two groups: 10/113 (8.8%) in the aminoglycoside alone and 12/139 (8.6%) in the combination group, p = 0.934 (Figure 1). There was no difference for reoperation, ongoing suppressive antibiotic use, or clinical suspicion of infection.
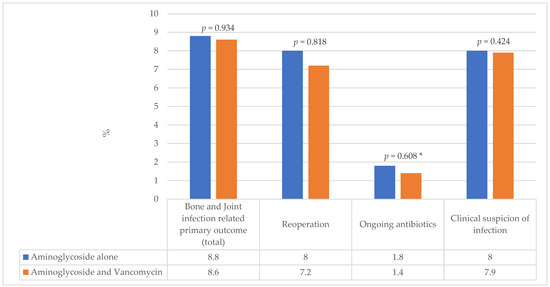
Figure 1.
Percentage of cases identified with the Primary Outcome. * Fisher’s exact test used for cells with a count <5.
2.3. Multivariate Analysis
Bone Involvement, Anti-microbial options, Coverage of the soft tissues, Host status (BACH) score [16] showed similar rates of complex cases in both groups (68.8% amino only vs. 69% combined therapy), but the aminoglycoside only group had fewer uncomplicated cases (27.7% vs. 40%) and a small number of severely affected cases with limited treatment options (3.6% vs. 0%). The univariate associations between potential confounding variables and the primary outcome are presented in Table 2. Laboratory-confirmed aminoglycoside resistance was similar in both groups (10.6% vs. 10.1%), but presumed aminoglycoside resistance was more frequent in the aminoglycoside only group (23.9% vs. 15.8%). However, the presence of aminoglycoside resistance had no effect on failure rate (Odds ratio (OR) 0.39: 95% Confidence Interval (CI) 0.05–3.01, p = 0.37).
Table 2.
Univariate analysis of association with the primary outcome.
Multivariate analysis demonstrated that there was no added benefit of combination therapy (OR 1.54: 95% CI 0.59–4.04, p = 0.38). Higher BACH score and low BMI were associated with increased risk of failure (BACH OR 3.49: 95% CI 1.13–10.76, p = 0.03; BMI (per 1 unit increase) OR 0.91: 95% CI 0.84–0.99, p = 0.037). The presence of Gram-negative pathogens showed a trend towards an increased risk of failure (OR 2.35: 95% CI 0.96–5.71, p = 0.06).
2.4. Subgroup Analysis of Carrier Material Type
There were 229 patients who had CERAMENT as the sole carrier for local antibiotics or in combination with other bioabsorbable carriers (90 with aminoglycoside alone and 135 with aminoglycoside and vancomycin). There was no difference in the number of cases who met the primary outcome at 12 months; 9/90 (10.0%) with aminoglycoside alone versus 12/135 (8.89%) with combination therapy; p = 0.938.
Carriers can be implanted as injectable paste or pellets/beads or both. In this cohort, 148/252 (58.7%) patients had injectable paste only, of which 9/68 (13.2%) in the aminoglycoside alone group and 7/80 (8.75%) in the combination group met the primary outcome; p = 0.381. In addition, 45/113 (39.8%) aminoglycoside only and 59/139 (42.4%) aminoglycoside plus vancomycin patients had pellets or beads inserted; p = 0.674. 1/45 (2.2%) of the aminoglycoside only group and 5/59 (8.5%) of the combination group met the primary outcome at 12 months; p = 0.175.
Comparing the form of the carrier material (injectable only versus injectable with pellets), there was no difference in the rate of the primary outcome (16/148; 10.8% injectable only vs. 6/104; 5.8% injectable plus pellets: p = 0.163).
3. Discussion
Local antibiotic delivery into an infected bone defect in osteomyelitis has become increasingly common in the treatment of bone and joint infection [11,12]. It results in high local concentration of antimicrobials and reduces concerns regarding patient compliance and systemic toxicity [17]. However, the choice of which empiric local antibiotic to insert into bone cement or void filler has not been investigated. In the past, gentamicin was the preferred antibiotic and was advocated in non-absorbable beads made from polymethylmethacrylate (PMMA) [2,18]. More recently, concerns about methicillin-resistant Staphylococcus aureus (MRSA) and reported increase in resistance to systemically administered aminoglycosides have prompted interest in additional local antimicrobials. However, it is important to limit the use of multiple antimicrobials without good evidence for additional efficacy, as part of good antibiotic stewardship. In particular, vancomycin is a valuable antibiotic for major Gram-positive infections and should be protected.
In this study, we found no overall advantage from adding vancomycin to gentamicin. This may be due to the delivery of sufficiently high gentamicin concentrations to overcome moderate resistance [19]. This is in keeping with a previous prospective clinical study at our institution which demonstrated that gentamicin-resistant organisms on laboratory testing (European Committee on Antimicrobial Susceptibility Testing (EUCAST) breakpoints) were successfully treated with local gentamicin [12].
Local antimicrobial therapy was provided using injectable paste and preformed pellets. We performed a sub-analysis to confirm that the form of the local antibiotic carrier did not affect the delivery of antimicrobial agent or the clinical outcome.
Ten percent of our patients had gentamicin-resistant isolates (EUCAST breakpoints); however, breakpoint definitions refer to systemic administration of antimicrobials [20]. Local antibiotics are able to achieve a far higher concentration than systemic antibiotics [2,19,21], with minimal risk of systemic toxicity [22]. CERAMENT G delivers 100 times the MIC for gentamicin-susceptible Staphylococcus aureus and Pseudomonas species [23], so may be able to overcome intermediate level antibiotic resistance. In vitro testing of CERAMENT G elution against S. aureus, S. epidermidis, P. aeruginosa and E. cloacae at different MICs demonstrated a zone of inhibition to all organisms excepting only highly resistant S. aureus (gentamicin MIC > 1024 mg/L) [24]. In vitro, gentamicin-loaded ceramic fillers are also able to inhibit some gentamicin-resistant coagulase negative Staphylococci [25].
Whilst local antibiotic treatment is generally safe, concerns remain for the potential of local toxicity on bone healing at the site of infection in in vitro studies [26,27], but this has not been confirmed in clinical studies. High-dose vancomycin and tobramycin may decrease cellular proliferation, but at standard doses in rabbit and rat models this effect was not seen [27], suggesting the importance of choosing an appropriate dose and class of local antibiotic. The method of delivery may also be important with modern bioabsorbable carriers providing a gradual elution of antimicrobial over several weeks [17,19].
Limitations
This study is limited by its retrospective design with a relatively short follow-up period. Additionally, all patients received systemic antimicrobial therapy, and further studies into the effect of local antibiotic over and above standard systemic therapy are pending [28]. Depending on these results, a prospective study comparing gentamicin alone to combination gentamicin and vancomycin local therapy is required.
This study is not a randomized controlled trial, so the results must be carefully interpreted. The study group was not selected for this therapy but was a consecutive series of cases presenting with the conditions to our department over the study period. All surgery was performed by the same surgical team (three surgeons) using the same protocol, with identical diagnostic criteria and systemic antimicrobial therapy (empiric and definitive). The choice of local antimicrobial(s) was not based on any previous microbiological culture results. Surgeons were free to choose whatever local antimicrobial regime they thought appropriate. The two groups were well matched with regard to many of the parameters which affect outcome. The factors which were different (BACH score, percentage of presumed gentamicin-resistant organisms and presence of Gram-negative organisms) all favored a better outcome in the combined vancomycin and aminoglycoside group, but this was not found. Clearly, the lack of randomization could introduce a selection bias, but we believe we have minimized this by the study design and open reporting of the full characteristics of the two study groups.
4. Materials and Methods
This was a retrospective observational cohort study at the Oxford University Hospital Bone Infection Unit. This specialist Unit treats a wide range of adult patients, referred from all over the United Kingdom, with infections affecting the musculoskeletal system, including infection after fractures, prosthetic joint replacement and hematogenous infection of the bones, joints and spine.
4.1. Recruitment and Inclusion Criteria
The medical and surgical records and laboratory details of all patients who were referred between January 2019 and September 2022 were reviewed. We identified all consecutive patients treated with a diagnosis of hematogenous osteomyelitis and fracture-related infection. Patients who were under 18 years old at the time of treatment were excluded. Inclusion for outcome analysis required complete follow-up to a minimum of 12 months after surgery. Patients lost to follow-up or dying before 12 months were excluded from the analysis.
Infection was confirmed using the International FRI Consensus Definition [29]. Patients with infection of the spine, septic arthritis alone or infection following prosthetic joint replacement were excluded. Additionally, patients were only eligible for inclusion if five or more separate tissue samples were taken at surgery, for microbiological culture. If implants were removed at surgery, these could also be sent for culture of fluid after sonication [30], but this was not mandatory. The culture protocol has previously been reported [31]. Infection was confirmed with at least two positive cultures of a phenotypically identical organism. A single positive culture was accepted when there was also confirmatory evidence of infection on histopathology. Tissue samples for histology (usually 3 or more) were embedded in paraffin and 5 µm sections cut. Sections were stained with hematoxylin and eosin and Gram-stained. At least 10 high-power fields were examined per section (×400). Positive histology was defined as the presence of visible micro-organisms on Gram stain or an average of ≥5 polymorphonuclear neutrophils seen per high-power field on hematoxylin- and eosin-stained sections.
Patients were only included if they had implantation of antibiotic carriers delivering aminoglycoside, with or without vancomycin, as part of their surgical management.
4.2. Surgical and Medical Treatment
All patients were treated with a single-stage protocol incorporating deep tissue sampling, excision of dead and compromised tissue, management of the excised dead space, bone stabilization (if required) and soft tissue closure, as previously described [32] (Figure 2a–e).
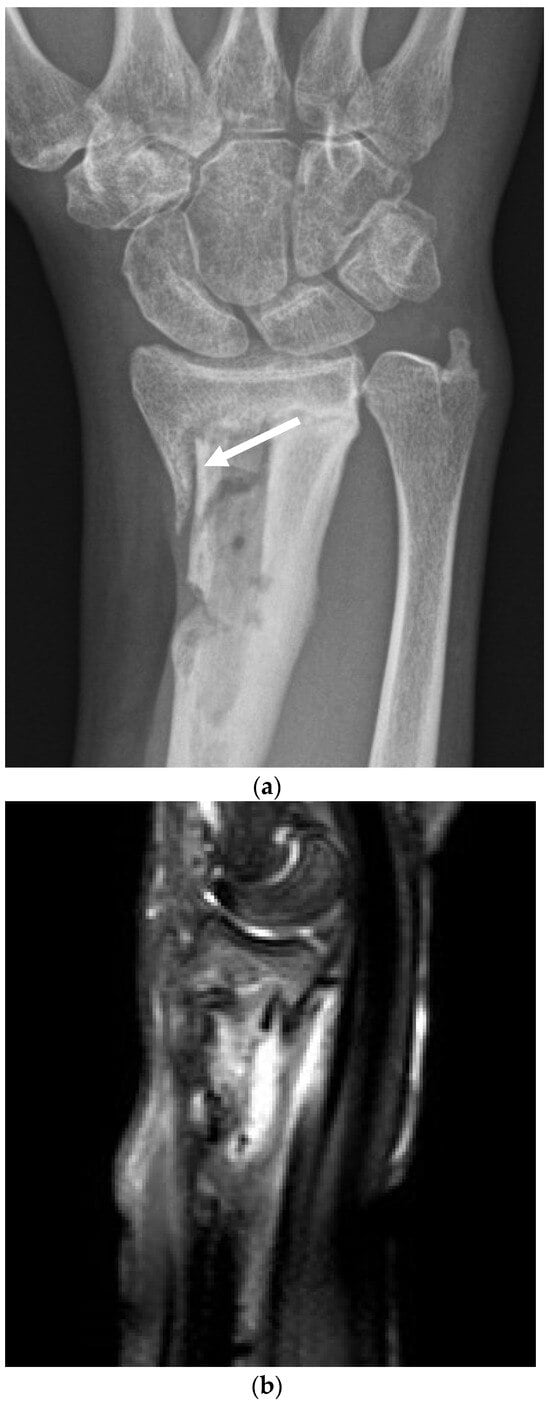
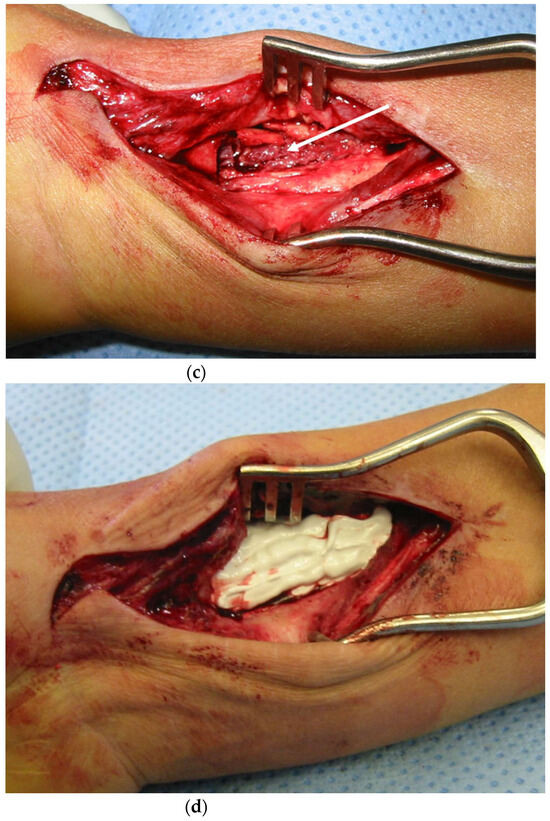

Figure 2.
(a). The surgical management with implantation of a gentamicin-loaded antibiotic carrier. This 32-year-old woman suffered a closed fracture of her distal radius in a fall. After fixation with a plate, the fracture became infected. The plate was removed, but she continued with a draining sinus and active infection. This preoperative radiograph shows the dead bone in the radial metaphysis (white arrow), but the fracture has healed. (b). The magnetic resonance scan demonstrates the area of high signal around the dead bone, with active infection. (c). At operation, the volar aspect of the wrist was opened and the infected bone exposed. Five deep tissue samples were taken for microbiology and three for histology. The central area of necrotic bone and infected tissue (white arrow) was excised back to healthy bleeding bone. (d). The excised dead space has been filled with CERAMENT G (with gentamicin), completely filling the bone defect. The material was compressed into the bone and the skin closed in layers. (e). The postoperative radiograph shows the antibiotic carrier in place, filling the defect.
Briefly, antibiotics were stopped at least two weeks before surgery when possible (stable patient without fever). Surgery was performed under tourniquet where possible. Sinus tracts and unstable skin were excised and discarded. Deep samples were taken by a validated protocol [33] involving harvest of at least 5 specimens of tissue, each taken with clean instruments and avoiding contact with the skin. Samples were transferred immediately to the microbiology laboratory for processing as described above. At least 3 specimens were also taken for histopathology [34].
All dead tissue was excised from the infected zone, preserving the peripheral living tissue. This was performed with gouges and chisels. Small spaces were excised with a saline-cooled bone burr, and screw holes were over-drilled. If the bone was unstable (unhealed fracture, non-union or very thin bone after resection), stabilization was performed, usually with the application of an external fixator.
In all cases, the dead space was filled with local antibiotics delivered in a carrier material. No patient had antibiotic powder implanted alone. The form of the carrier (injectable paste or beads or pellets) was chosen depending on the morphology of the space to allow good void filling. At the time of this study, there was no published evidence-based recommendation concerning the sole use of aminoglycoside or combined antibiotic use in local therapy for bone infection [27]. Multiple licensed commercial products were available (see Table 1) with various options for aminoglycoside or combined therapy. In this study, we defined two groups of patients by the type of antimicrobial(s) delivered locally into the bone. Group one had only an aminoglycoside antibiotic (gentamicin or tobramycin) delivered in a licensed carrier material. Group two also had aminoglycoside but in combination with vancomycin; both delivered in a licensed carrier material. Surgeons were free to choose their preferred material and antibiotic(s). This choice had no effect on any other aspect of the surgical or medical care. Antimicrobial choice was not based on any microbiological information obtained before surgery, as this was not regarded as relevant to local therapy.
After dead space filling, the soft tissues were closed during the same operation. No vacuum-assisted closure or delayed closure was employed. When the defect was too large for direct skin apposition, a local or free tissue transfer was performed to provide immediate skin coverage.
Empiric parenteral antibiotics were given after sampling and continued until microbial cultures were obtained. The regimen was chosen based on our previously published study of osteomyelitis and FRI [35]. The regimen was intravenous administration of 1–2 g of vancomycin (weight-dependent) and 500 mg of meropenem after sampling. Vancomycin was continued twice daily and meropenem 3 times daily for two days. If no Gram-negative organisms were cultured by the third day, meropenem was topped and vancomycin continued. When definitive microbiological cultures were obtained (usually within 5 days), the long-term antimicrobial therapy was decided. Patients were preferentially treated with oral therapy, when an oral option was available, based on the results of the OVIVA randomized trial [36]. The individual choice of drug was consistent with the recommendations of the FRI consensus guidelines [37] and continued for 6–12 weeks.
Patients were followed up for a minimum of one year or to death, if sooner. Patients visited a specialist combined clinic (with surgeons and infectious disease physicians), usually at 6, 12, 26 and 52 weeks after surgery. Patients with external fixators attended more frequently for review of fixator pin sites and stability. On each visit, the primary outcome was assessed with clinical assessment, radiology and blood tests when indicated.
4.3. Data Collection
Medical records were reviewed for inclusion and exclusion criteria, and data were extracted using a standardized template. Demographic information collected included age, gender, Body Mass Index (BMI) and American Society of Anesthesiology (ASA) score [38]. Clinical data collected included BACH classification [16,39], microbiological characteristics including antimicrobial susceptibility profile, type of local antibiotic carrier, duration of antibiotic therapy and outcome. Presumed gentamicin resistance was based on the Sanford Guide antibiogram [40].
4.4. Outcome
The primary outcome of failure of therapy was a composite of recurrence of infection, continued or new antimicrobial therapy, or reoperation with suspected or confirmed infection at one year after index surgery [28]. Any patient presenting with any one or more of the components of this composite, by one year of surgery, was regarded as having failed therapy. Subgroup analysis of the type and form of carrier material used was also performed.
4.5. Data Management and Analysis
Analysis was performed using IBM SPSS v29. The difference in the rate of the primary outcome between the two groups was compared using logistic regression. Potential confounders considered for inclusion in the regression models were age, ASA, BMI, presence of gentamicin resistance, type of surgery, presence of polymicrobial infection, presence of Gram-negative organisms, BACH score, time from intravenous to oral antibiotic switch and duration of antibiotics. Each potential confounder was examined separately by univariate analysis to determine their association with the outcome variable. Confounders whose association with the outcome variable had a p-value < 0.2 were included in the multivariate model, except for age which was included regardless.
5. Conclusions
Clinical outcome was not improved by the addition of vancomycin to aminoglycoside alone as local therapy for the management of osteomyelitis and fracture-related infection. Additionally, laboratory-measured resistance, using currently accepted EUCAST breakpoints, may not be relevant in local therapy. This study should have an impact on the choice of empirical local antibiotic treatment used in the treatment of bone and joint infections.
Author Contributions
Conceptualization, M.M.; methodology, A.U., M.M., M.S. and B.Y.; formal analysis, A.U., M.M. and J.F.; investigation, A.U. and M.M.; data curation, A.U. and M.M.; writing—original draft preparation, A.U. and M.M.; writing—review and editing, A.U., M.M., J.F., M.S. and B.Y.; supervision, M.M., B.Y. and M.S. All authors have read and agreed to the published version of the manuscript.
Funding
AU received a Royal Australian College of Physicians Travel Grant to undertake a clinical fellowship at the Oxford Bone Infection Unit, Nuffield Orthopaedic Centre, Oxford, UK. No other funding was received for this study.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by our Institutional Governance Board as a Quality Improvement Project. No ethical committee review was required.
Informed Consent Statement
The patient described in Figure 2 gave written consent for the use of her images and clinical details. Her identity has been protected in the images.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author due to privacy reasons.
Acknowledgments
We would like to thank the staff of the Oxford Bone Infection Unit and The John Radcliffe Hospital Microbiology Laboratory for their dedication to the care of these patients.
Conflicts of Interest
M. McNally and J. Ferguson have performed consultancy work for Bonesupport AB, outside the scope of this paper. The other authors declare no conflicts of interest.
References
- Huang, J.; Sebastian, S.; Collin, M.; Tagil, M.; Lidgren, L.; Raina, D.B. A calcium sulphate/hydroxyapatite ceramic biomaterial carrier for the local delivery of tobramycin in bone infections: Analysis of rheology, drug release and antimicrobial efficacy. Ceram. Int. 2023, 49, 33725–33734. [Google Scholar] [CrossRef]
- Klemm, K.W. Antibiotic bead chains. Clin. Orthop. Relat. Res. 1993, 295, 63–76. [Google Scholar] [CrossRef]
- Pförringer, D.; Obermeier, A.; Kiokekli, M.; Büchner, H.; Vogt, S.; Stemberger, A.; Burgkart, R.; Lucke, M. Antimicrobial formulations of absorbable bone substitute materials as drug carriers based on calcium sulfate. Antimicrob. Agents Chemother. 2016, 60, 3897–3905. [Google Scholar] [CrossRef] [PubMed]
- Wassif, R.K.; Elkayal, M.; Shamma, R.N.; Elkheshen, S.A. Recent advances in the local antibiotics delivery systems for management of osteomyelitis. Drug Deliv. 2021, 28, 2392–2414. [Google Scholar] [CrossRef] [PubMed]
- Cobb, L.H.; McCabe, E.M.; Priddy, L.B. Therapeutics and delivery vehicles for local treatment of osteomyelitis. J. Orthop. Res. 2020, 38, 2091–2103. [Google Scholar] [CrossRef] [PubMed]
- Wahlig, H.; Dingeldein, E.; Bergmann, R.; Reuss, K. The release of gentamicin from polymethylmethacrylate beads. J. Bone Jt. Surg. 1978, 60-B, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Walenkamp, G.H. How I do it: Chronic osteomyelitis. Acta Orthop. Scand. 1997, 68, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Epstein, G.; Ferreira, N. Dead space management strategies in the treatment of chronic osteomyelitis. Eur. J. Orthop. Surg. Traumatol. 2023, 33, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Rodham, P.; Pantelli, M.; Qin, C.; Harwood, P.; Giannoudis, P.V. Long-term outcomes of lower limb post-traumatic osteomyelitis. Eur. J. Trauma Emerg. Surg. 2023, 49, 539–549. [Google Scholar] [CrossRef]
- Jiamton, C.; Apivatgaroon, A.; Aunaramwat, S.; Chawalitrujiwong, B.; Chuaychoosakoon, C.; Suwannaphisit, S.; Jeraveesal, C.; Iamsumang, C.; Kongmalai, P.; Sukvanich, P.; et al. Efficacy and Safety of Antibiotic Impregnated Microporous Nanohydroxyapatite Beads for Chronic Osteomyelitis Treatment: A Multicenter, Open-Label, Prospective Cohort Study. Antibiotics 2023, 12, 1049. [Google Scholar] [CrossRef]
- Ferguson, J.; Bourget-Murray, J.; Hotchen, A.J.; Stubbs, D.; McNally, M. A comparison of clinical and radiological outcomes between two different biodegradable local antibiotic carriers used in the single-stage surgical management of long bone osteomyelitis. Bone Jt. Res. 2023, 12, 412–422. [Google Scholar] [CrossRef] [PubMed]
- McNally, M.A.; Ferguson, J.Y.; Scarborough, M.; Ramsden, A.; Stubbs, D.A.; Atkins, B.L. Mid-to long-term results of single-stage surgery for patients with chronic osteomyelitis using a bioabsorbable gentamicin-loaded ceramic carrier. Bone Jt. J. 2022, 104, 1095–1100. [Google Scholar] [CrossRef] [PubMed]
- McNally, M.; Corrigan, R.; Sliepen, J.; Dudareva, M.; Rentenaar, R.; IJpma, F.; Atkins, B.L.; Wouthuyzen-Bakker, M.; Govaert, G. What factors affect outcome in the treatment of fracture-related infection? Antibiotics 2022, 11, 946. [Google Scholar] [CrossRef] [PubMed]
- Grayson, M.L.; Cosgrove, S.; Crowe, S.; Hope, W.; McCarthy, J.; Mills, J.; Mouton, J.W.; Paterson, D. (Eds.) Kucer’s the Use of Antibiotics; Taylor & Francis Group: Boca Raton, FL, USA, 2018. [Google Scholar]
- Rybak, M.J. The pharmacokinetic and pharmacodynamic properties of vancomycin. Clin. Infect. Dis. 2006, 42, S35–S39. [Google Scholar] [CrossRef] [PubMed]
- Hotchen, A.J.; Dudareva, M.; Ferguson, J.Y.; Sendi, P.; McNally, M.A. The BACH classification of long bone osteomyelitis. Bone Jt. Res. 2019, 8, 459–468. [Google Scholar] [CrossRef] [PubMed]
- Ene, R.; Nica, M.; Ene, D.; Cursaru, A.; Cirstoiu, C. Review of calcium-sulphate-based ceramics and synthetic bone substitutes used for antibiotic delivery in PJI and osteomyelitis treatment. EFORT Open Rev. 2021, 6, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Zalavras, C.G.; Patzakis, M.J.; Holtom, P. Local antibiotic therapy in the treatment of open fractures and osteomyelitis. Clin. Orthop. Relat. Res. 2004, 427, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Stravinskas, M.; Nilsson, M.; Horstmann, P.; Petersen, M.M.; Tarasevicius, S.; Lidgren, L. Antibiotic containing bone substitute in major hip surgery: A longterm gentamicin elution study. J. Bone Jt. Infect. 2018, 3, 68–72. [Google Scholar] [CrossRef][Green Version]
- Turnidge, J.; Paterson, D.L. Setting and revising antibacterial susceptibility breakpoints. Clin. Microbiol. Rev. 2007, 20, 391–408. [Google Scholar] [CrossRef]
- Salvati, E.A.; Callaghan, J.J.; Brause, B.D.; Klein, R.F.; Small, R.D. Reimplantation in Infection: Elution of Gentamicin from Cement and Beads. Clin. Orthop. Relat. Res. 1986, 207, 83–93. [Google Scholar] [CrossRef]
- Muir, R.; Birnie, C.; Hyder-Wilson, R.; Ferguson, J.; McNally, M.A. Does local implantation of gentamicin impair renal function in patients undergoing surgery for chronic bone infection. Int. J. Res. Orthop. 2021, 7, 438. [Google Scholar] [CrossRef]
- Bonesupport, N.a.l. Gentamicin Release In Vitro from Setting CERAMENT™|G Paste. Data on File Report S009/2012. Available online: https://www.stoecklimedical.ch/wp-content/uploads/2022/11/PR-01118-01-en-EU-Value-Guide.pdf (accessed on 1 June 2024).
- Bezstarosti, H.; van Lieshout, E.M.M.; van den Hurt, M.J.B.; Kortram, K.; Oprel, P.; Kock, B.C.P.; Croughs, P.D.; Verhofstad, M.H.J. In vitro elution of gentamicin from CERAMENT G has an antimicrobial effect on bacterial with various levels of gentamicin resistance found in fracture-related infection. Clin. Orthop. Relat. Res. 2024, 482, 885–891. [Google Scholar] [CrossRef] [PubMed]
- Bidossi, A.; Bottagisio, M.; Logoluso, N.; De Vecchi, E. In vitro evaluation of gentamicin or vancomycin containing bone graft substitute in the prevention of orthopedic implant-related infections. Int. J. Mol. Sci. 2020, 21, 9250. [Google Scholar] [CrossRef] [PubMed]
- Antoci, V., Jr.; Adams, C.S.; Hickok, N.J.; Shapiro, I.M.; Parvizi, J. Antibiotics for local delivery systems cause skeletal cell toxicity in vitro. Clin. Orthop. Relat. Res. 2007, 462, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Metsemakers, W.-J.; Fragomen, A.T.; Moriarty, T.F.; Morgenstern, M.; Egol, K.A.; Zalavras, C.; Obremskey, W.T.; Raschke, M.; McNally, M.A. Evidence-based recommendations for local antimicrobial strategies and dead space management in fracture-related infection. J. Orthop. Trauma 2020, 34, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Dudareva, M.; Kümin, M.; Vach, W.; Kaier, K.; Ferguson, J.; McNally, M.; Scarborough, M. Short or Long Antibiotic Regimes in Orthopaedics (SOLARIO): A randomised controlled open-label non-inferiority trial of duration of systemic antibiotics in adults with orthopaedic infection treated operatively with local antibiotic therapy. Trials 2019, 20, 693. [Google Scholar] [CrossRef] [PubMed]
- Govaert, G.A.M.; Kuhl, R.; Atkins, B.L.; Trampuz, A.; Morgenstern, M.; Obremsky, W.T.; Verhofstad, M.H.J.; McNally, M.A.; Metsemakers, W.-J. Diagnosing Fracture-related infections: Current concepts and recommendations. J. Orthop. Trauma 2020, 34, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Sandbakken, E.T.; Witsø, E.; Sporsheim, B.; Egeberg, K.W.; Foss, O.A.; Hoang, L.; Bjerkan, G.; Løseth, K.; Bergh, K. Highly variable effect of sonication to dislodge biofilm-embedded taphylococcus epidermidis directly quantified by epifluorescence microscopy: An in vitro model study. J. Orthop. Surg. 2020, 15, 522. [Google Scholar] [CrossRef] [PubMed]
- Young, B.C.; Dudareva, M.; Vicentine, M.P.; Hotchen, A.J.; Ferguson, J.; McNally, M. Microbial Persistence, Replacement and Local Antimicrobial Therapy in Recurrent Bone and Joint Infection. Antibiotics 2023, 12, 708. [Google Scholar] [CrossRef]
- Wijendra, A.; Tsang, J.; Ferguson, J.; McNally, M.A. Managing fracture-related infection. Orthop. Trauma 2023, 37, 366–378. [Google Scholar] [CrossRef]
- Dudareva, M.; Barrett, L.; Oakley, S.; Jesuthasan, G.; Morgenstern, M.; Atkins, B.L.; Brent, A.J.; McNally, M.A. Providing an evidence base for tissue sampling and culture interpretation in suspected fracture-related infection. J. Bone Jt. Surg. 2021, 103, 977–983. [Google Scholar] [CrossRef] [PubMed]
- Sigmund, I.K.; Yeghiazaryan, L.; Luger, M.; Windhager, R.; Sulzbacher, I.; McNally, M.A. Three to six tissue specimens for histopathological analysis are most accurate for diagnosing periprosthetic joint infections. Bone Jt. J. 2023, 105-B, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Dudareva, M.; Hotchen, A.J.; Ferguson, J.; Hodgson, S.; Scarborough, M.; Atkins, B.L.; McNally, M.A. The microbiology of osteomyelitis: Changes over ten years. J. Infect. 2019, 79, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Li, H.-K.; Rombach, I.; Zambellas, R.; Walker, A.S.; McNally, M.A.; Atkins, B.L.; Lipsky, B.A.; Hughes, H.C.; Bose, D.; Kümin, M.; et al. Oral versus Intravenous Antibiotics for Bone and Joint Infection. N. Engl. J. Med. 2019, 380, 425–436. [Google Scholar] [CrossRef] [PubMed]
- Depypere, M.; Kuehl, R.; Metsemakers, W.J.; Senneville, E.; McNally, M.A.; Obremskey, W.T.; Zimmerli, W.; Atkins, B.L.; Trampuz, A. Recommendations for systemic antimicrobial therapy in fracture-related infection: A consensus from an international expert group. J. Orthop. Trauma 2020, 34, 30–41. [Google Scholar] [CrossRef]
- Michel, J.-P.; Klopfenstein, C.; Hoffmeyer, P.; Stern, R.; Grab, B. Hip fracture surgery: Is the pre-operative American Society of Anesthesiologists (ASA) score a predictor of functional outcome? Aging Clin. Exp. Res. 2002, 14, 389–394. [Google Scholar] [CrossRef]
- Hotchen, A.J.; Wismayer, M.G.; Robertson-Waters, E.; McDonnell, S.M.; Kendrick, B.; Taylor, A.; Alvand, A.; McNally, M. The Joint-Specific BACH classification: A predictor of outcome in prosthetic joint infection. eClinicalMedicine 2021, 42, 101192. [Google Scholar] [CrossRef]
- The Sanford Guide to Antimicrobial Therapy 2023; Antimicrobial Therapy, Inc.: Sperryville, VA, USA, 2023.




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).