Abstract
Acute pancreatitis (AP) is a common but often self-limiting disease in the majority of patients. However, in the minority, who may progress to moderately severe or severe AP, high mortality risk has been reported. Infected pancreatitis necrosis (IPN) in necrotising pancreatitis has been shown to result in more than twice the mortality rate compared with in sterile pancreatic necrosis. This raises the question on whether prophylactic antibiotics (PABs) should be given in subgroups of AP to prevent superimposed infection to improve survival outcomes. Despite numerous randomised controlled trials (RCTs), meta-analyses, and guidelines on the management of AP, there is a lack of strong evidence to suggest the use of PABs in AP. Additionally, use of PABs is associated with antimicrobial resistance. Considerable heterogeneity exists and limits the interpretation of results—subgroup of AP benefitting from PAB use, choice/class of PAB, and timing of administration from symptom onset and duration of PAB use. Only a minority of existing meta-analyses suggest mortality benefits and reduction in IPN. The majority of existing guidelines do not recommend the use of PABs in AP. More research is required to make more definitive conclusions. Currently, PAB should only be administered after multidisciplinary discussions led by pancreatology experts.
1. Introduction
Acute pancreatitis (AP) is a commonly encountered pathology in general surgery and hepatopancreatobiliary surgery, with an approximate incidence of 50–80 cases per 100,000 people [1]. In the majority (80%) of cases, AP presents as a mild and self-limiting disease with a low mortality risk of 1–2% [2,3]. In mild AP, supportive management is provided with patient monitoring for risk of progression to severe AP, symptomatic relief, work-up of underlying aetiology, and administration of measures to reduce risk of recurrent AP [4]. However, for patients with moderately severe to severe AP (SAP), mortality risk has been reported to range from 20 to 40% [5,6,7]. Several international guidelines have been crafted to guide the management of SAP, aiming to reduce morbidity and mortality [8,9,10,11,12,13,14,15]. One big domain of contention is the role of prophylactic antibiotics (PABs) in SAP.
Recently published meta-analyses show conflicting results on the use of PABs. For instance, Ukai et al. demonstrated lower mortality for patients with acute necrotising pancreatitis (ANP) with PABs (administered within 72 h from symptom onset) [16], while Guo et al. showed similar mortality with and without prophylactic carbapenem use in SAP [17]. Several considerations need to be made, such as the presence of concomitant cholangitis, patient comorbidity, local resources, and available expertise. Despite the lack of concrete evidence supporting the use of PABs in AP, there is a considerable proportion of surgeons worldwide who administer PABs in AP [18]. This is causing growing global concern, especially with the silent epidemic of antimicrobial resistance (AMR), with an estimated 4.95 million deaths in 2019 [19]. It is necessary to rationalise the use of antibiotics and enforce governance to reduce the morbidity and mortality associated with AMR, calling for a timely update on the available literature on PABs. This review aims to summarise evidence on the role of PABs in AP with an up-to-date review of the available literature.
2. Definitions
To begin, there is a need to standardise the various terminologies used in the current literature. The indications for antibiotics can be classified into prophylactic, empirical, or therapeutic. Prophylactic refers to the administration of antibiotics to prevent an infection. Empirical antibiotics refer to administration to treat possible, probable, or suspected infection without definitive evidence that an infection is present, because the benefits outweigh the risks. Therapeutic refers to starting antibiotics with definitive proof that an infection exists. In the context of SAP, PABs are used when there is no evidence of an infection (e.g., afebrile, stable inflammatory markers, normal procalcitonin levels) and is used to prevent an infection, as this group of patients may deteriorate rapidly. Empirical antibiotics are used when there is suspected infection in SAP, such as concerns for infected pancreatic necrosis (IPN) and/or extra-pancreatic infections.
AP can be classified based on (1) severity, (2) morphological features, (3) types of local complications (if any), and (4) aetiology. The various definitions are summarised in Table 1. To date, the most commonly used system to stratify the severity of AP is the 2012 modified Atlanta classification system, where AP is stratified into mild, moderately severe, and severe [20]. There are other classification systems used in AP—though less commonly used—such as one proposed by the Pancreatitis Across Nations Clinical Research and Education Alliance (PANCREA) [21], where a four-tiered classification system (mild, moderate, severe, and critical) is used instead. Differences between that and the modified Atlanta classification system include the use of (peri)pancreatic necrosis instead of local complications, and classifying whether infection is present. In the classification system suggested by PANCREA, presence of infected (peri)pancreatic necrosis would place patients to be of at least severe AP, and critical AP would include both the presence of infected (peri)pancreatic necrosis (IPN) and persistent organ failure. One reason why presence of infection was used as a stratifying criterion would be the associated mortality. A meta-analysis by Werge et al. (n = 71 studies, 6970 patients) showed that IPN was associated with significantly higher mortality compared to sterile pancreatic necrosis (odds ratio (OR) 2.57, 95% confidence interval (CI): 2.00–3.31) [22]. This further reinforces the need to discuss the risks versus benefits of PABs in patients with sterile (peri)pancreatic necrosis.

Table 1.
Summary of the various definitions used in acute pancreatitis.
It is also important to stratify AP based on morphological features and type of local complications due to the difference in prognosis and management [20]. Morphology of AP can be broadly classified into interstitial oedematous pancreatitis or necrotising pancreatitis. Pancreatic necrosis occurs because of impairment of pancreatic perfusion [20]. Local complications can be broadly classified into the following (diagnosed on imaging):
- Non-necrotic (sequelae of interstitial oedematous AP):
- Acute peripancreatic fluid collection (APFC)—less than 4 weeks;
- Pancreatic pseudocyst (absence of necrosis)—more than 4 weeks.
- Necrotic (sequelae of necrotising AP):
- Acute necrotic collection (ANC)—less than 4 weeks;
- Walled-off necrosis (WON)—more than 4 weeks.
In general, majority of patients with APFC are managed conservatively and these resolve without intervention [23]. While pancreatic pseudocysts are rare, these usually require some form of intervention, either endoscopically, surgically, or percutaneously [24]. In contrast, local complications of ANP are more worrisome, with risk of superimposed infection of ANC or WON—about 30% of patients with ANP develop IPN after the first week [25]. This is concerning, especially since the mortality of IPN is more than twice that of sterile necrosis [22].
3. Guidelines on AP
In view of the complexity of AP as well as the associated morbidity and mortality with SAP, numerous guidelines have been published over the past decades to guide clinicians on management. We have summarised the available guidelines on AP published since 2005 on their recommendations and quality of evidence regarding the role of PABs in AP without any infection (Table 2). Additionally, we also summarised the guidance on the use of biochemical markers and/or investigations to guide diagnosis of infection in AP, as well as the role and/or choice of antibiotics in AP with concomitant infection. Across all guidelines included in our review, none of them recommend PABs for all cases of AP regardless of severity. The majority also do not recommend PABs for SAP, except for the 2015 Japanese Guidelines, which state that PABs may improve prognosis in SAP if administered in the early phases of AP (<72 h from onset); however, this was a weak recommendation with a moderate level of evidence.
Table 2.
Summary of existing guidelines on the role of antibiotics in acute pancreatitis.
Nevertheless, despite the widespread availability of guidelines that do not recommend for PABs in AP, compliance is of concern. The MANCTRA-1 (coMpliAnce with evideNce-based cliniCal guidelines in the managemenT of acute biliaRy pancreAtitis) international audit from 2019 to 2020 showed that 83.4% and 53.4% of patients with severe acute biliary pancreatitis (ABP) and mild ABP, respectively, received PABs [27]. Other international surveys similarly supported this finding—163 of 1054 participants (15.5%) administered routine PABs for AP [18]. A plausible reason for the lack of compliance may be due to the clinicians’ fear of patient deterioration, especially in SAP where there is already organ dysfunction or lack of governance from stewardship teams. There is also a diagnostic dilemma on determining the presence of an infection in AP. The above reasons are drivers of AMR, which was described early on, such as in the 2006 guidelines by the American College of Gastroenterology [14]. However, subsequent guidelines do not cover the issue about the emergence of AMR and impact on outcomes, which highlights a concerning lack of awareness of the high mortality that ensues from AMR.
It is our view that pancreatologists are direct stakeholders of patient care and retain the stewardship of antimicrobial needs of their patients and work in tandem with institutional stakeholders to make joint decisions for individual patients. One needs to maintain a balance of antibiotic overuse, misuse, and abuse, and avoid that a deserving patient comes to harm from underuse, delayed use, or non-use. Frivolous use of antibiotics also results in wastage and environmental harm. Pancreatologists may also initiate somatostatin analogues to reduce pancreatic secretion. However, there is a role for multidisciplinary management of patients with AP given the clinical conundrums that exist; pancreatologists should work in tandem with other subspecialty experts—intensivists and radiologists. Patients with SAP have single- or multi-organ failure, which necessitates higher level acuity care, led by intensivists. Holistic management and supportive treatment of every organ system by intensivists are crucial. Referral to gastroenterologists for endoscopic retrograde cholangiopancreatogram (ERCP) should be considered when cholelithiasis or choledocholithiasis is the aetiology (which may also be iatrogenic from the use of somatostatin analogues) [28], but subject to the haemodynamic stability of the patient. Radiologists should be approached in the presence of intra-abdominal collections or suspicion of IPN. Confirmation of IPN requires culture confirmation by needle aspiration, which is invasive and has its risks. Hence, we will discuss the current literature on PABs in AP.
4. The Current Literature on the Role of Prophylactic Antibiotics in Acute Pancreatitis
Over the past decade, there have been several meta-analyses performed to try to pool results and identify whether PABs improve outcomes in AP. We have summarised the available meta-analyses (n = 8) in the literature published from 2010 to 2023 with the inclusion criteria (type of study, severity of AP), type and time of PAB administration, as well as a summary of effect size for each outcome variable obtained from the pooled studies in Table 3. Of these meta-analyses, there were six (75.0%) that included only RCTs [16,29,30,31,32,33], and six (75.0%) that included only SAP and/or ANP [16,17,31,32,33,34]. Table 4 summarises the number of meta-analyses which reported the outcomes of interest and have been stratified based on their study type and severity of AP.
Table 3.
Summary of existing meta-analyses on the use of prophylactic antibiotics in acute pancreatitis.
Table 4.
Summary of meta-analyses that reported the outcome variables of interest and stratified based on study type and inclusion criteria.
Of the three studies that reported on overall infection rates, two reported a significant reduction in overall infection with PABs use [17,29]. Only a minority of meta-analyses demonstrated a statistically significant reduction in mortality (n = 2/8) [16,34], IPN (n = 2/8) [16,32], or extrapancreatic infections (EPIs) (n = 1/7) [30]. No studies showed a significant reduction in incidence of pneumonia (n = 3), need for surgical intervention (n = 7), or organ failure (n = 2). Of the included meta-analyses, only the review by Villatoro et al. and Lim et al. collected data on AMR from the included original articles [33,34], of which, only two original articles reported data on AMR [35,36].
There are a few reasons for the heterogeneity in results, and considerations need to be made:
- Morphological features and severity of AP;
- Choice/class of PABs;
- Timing of administration of PABs from symptom onset;
- Duration of PABs use.
4.1. Morphological Features and Severity of AP
The inclusion criteria of the various meta-analyses differ; some included studies with AP of any severity, while some only included SAP and/or ANP. Both SAP and ANP are associated with mortality risks of up to 30% [26,37]. As described above, IPN is associated with more than twice the mortality rate compared with sterile necrosis [22]. Hence, results from studies on SAP and/or ANP alone are likely to be different compared to those that included any severity of AP. Only the reviews on severe AP and/or ANP showed a significant reduction in mortality and IPN with PABs use (Table 4). This reinforces the hypothesis that since patients with SAP and/or ANP are in a pro-inflammatory state with high risk of deterioration [38], PABs may help to reduce the risk of superimposed infection and resultant mortality. In patients with SAP and/or ANP, gastrointestinal mucosal hypoperfusion can disrupt the mucosal defence barrier and thus allow for portal venous access to the enteric microbial flora. This hypothesis is supported by Garret et al., who showed that presence of 1–2 system and ≥3 system organ failure was associated with 4.44 times and 28.67 times the odds of IPN respectively compared with no organ failure [39]. Hence, PABs may have some role in selected SAP and/or ANP patients to reduce risk of IPN and subsequent mortality.
4.2. Choice/Class of PABs
On top of the controversy behind the use of antibiotics, there is also a need to consider the class of antibiotics used, as the pharmacokinetics of each class of antibiotics differ. Not all classes of antibiotics are able to penetrate pancreatic parenchyma, hence appropriate class of antibiotics should be chosen [10]. The pathogens responsible for IPN are usually Gram-negative bacteria (e.g., Escherichia coli, Klebsiella pneumoniae, Proteus spp.) due to bacterial translocation from gastrointestinal flora [40]. However, Gram-positive bacteria such as Staphylococcus aureus, Streptococcus faecalis, and Enterococcus spp. are also not uncommon, with reported incidence of about 30% in those with positive fluid cultures [41]. Clinicians should ensure that PABs, if used, should cover both Gram-negative and Gram-positive bacteria.
The majority of the meta-analyses performed thus far did not limit their inclusion criteria on the choice of PABs used, except for the study by Guo et al. in 2022, which analysed seven studies (five RCTs and two retrospective studies) with 3846 patients who received prophylactic carbapenem for SAP within 48–120 h from the onset of symptoms [17]. They showed a reduction in incidence of overall infections and overall local and/or systemic complications, but no statistically significant differences were observed in mortality, IPN, or EPI (Table 3). Carbapenems are one of the broadest antimicrobials against Gram-negative organisms and Gram-positive organisms, except for methicillin-resistant Staphylococcus aureus (MRSA) and Enterococcus faecium. The World Society of Emergency Surgery (WSES) 2019 guidelines suggest the use of broad-spectrum antibiotics in order to penetrate pancreatic necrosis and cover against both Gram-negative and Gram-positive microbes (strong agreement, moderate quality of evidence) [10]. Similarly, the AGA clinical practice update on the management of pancreatic necrosis recommends the use of broad-spectrum antibiotics such as carbapenems, quinolones, and metronidazole [26]. However, these recommendations were for the use of empiric antibiotics against suspected/proven IPN, but not for the use of PABs to prevent IPN/other infective complications in AP.
Yao et al. did not show a significant difference in mortality between PABs vs. no PABs in RCTs on ANP [32]; however, a subgroup analysis performed based on the class of antibiotics showed that prophylactic cephalosporins were associated with a significant reduction in mortality (RR: 0.71, 95% CI: 0.43–1.18), but not for beta-lactams in general (RR: 0.81, 95% CI: 0.47–1.38). One possible consideration is that beta-lactams include the use of broad-spectrum carbapenems; PABs with carbapenems raise concerns of increasing incidence of carbapenem-resistant bacteria, with a reported incidence of 33% accounting for EPI [42]. The use of carbapenems has also been postulated to result in a change in intestinal flora towards a higher incidence of Gram-positive bacteria [43], and may increase AMR. This is concerning, especially when 63% of patients with suspected/proven pancreatic infections had multi-drug-resistant (MDR) organisms [44]. Therefore, there is a need to balance the extent of antimicrobial coverage versus the risk of emerging AMR.
4.3. Timing of Administration of PABs from Symptom Onset, and Total Duration of PABs
In the management of sepsis, early antibiotic administration, during the “golden hour”, is prudent [45]. Reducing time to first antibiotics from more than 6 h to less than 1 h has been shown to reduce mortality by 9.5% [46]. Similarly, PABs for surgical procedures should be administered 30 to 60 min prior to surgical incision [47]. The evidence for this was based on antibiotic pharmacokinetics to achieve adequate plasma concentrations [48]. For PABs in AP, various timings have been used in the available literature, ranging from 48 to 120 h from symptom onset (Table 2). However, several of the included RCTs did not specify the timing of PABs administration [49,50]. The meta-analysis by Ukai et al. was the only one that had strict inclusion criteria of PABs administration within 72 h from symptom onset, or 48 h after admission; they showed lower mortality and IPN in the PABs group [16]. Lack of statistical significance in other meta-analyses may be due to the lack of standardisation of timing of antibiotics administration. However, it is apparent that several existing meta-analyses do not take into account the clinical significance of the timing of PABs administration, as this was not included in any subgroup analyses or their reported data [29,31,32,33].
Similarly, duration of PABs is another controversial issue. Antibiotic stewardship is an evolving concern due to over-prescription of antibiotics with risk of adverse events and AMR. Recommendations are made for a limit of 5–7 days in established intra-abdominal infection with no source control procedure [51]. Specific pathologies have been shown to require a protracted course of antibiotics, such as in cholecystitis and cholangitis complicated by bacteraemia [52], or pyogenic liver abscess (PLA). In the case of PLA, antibiotics are administered for a minimum of 2 weeks, with total duration of antibiotics guided by clinical and radiological response [53]. However, these are cases with a proven infective source. In the case of PAB use in AP, the duration of use varied from 5 to 21 days [35,36,54]. A protracted course of PABs may not necessarily be better at preventing infections, and vice versa. A 24 h course of PABs in elective plastic surgery has been shown to be as efficacious as a 5-day course in reducing surgical site infections [55]. Additionally, with such varied duration in PABs use, interpretation is difficult, and standardisation should be performed in subsequent studies. Additionally, we suggest that the duration of PABs be guided by clinical judgement and serologic biomarkers to avoid the risk of adverse events and AMR from a protracted course of antibiotics.
4.4. Antimicrobial Resistance
The emergence of AMR and its associated mortality are extremely concerning, especially in SAP, where mortality is already high. A global study using predictive statistical modelling also showed that in 2019 alone, E. coli and K. pneumoniae—common pathogens involved in gastrointestinal infections, including IPN—were each responsible for more than 250,000 deaths associated with AMR [19]. Lee et al. reported a high incidence (63%) of MDR organisms with suspected or proven pancreatic infections. Patients with MDR-associated infections had longer intensive care unit (ICU) stays (20 days vs. 2 days, p = 0.001) compared to those with non-MDR infections [44]. Although they showed that mortality was not statistically significant between MDR vs. non-MDR pancreatic infections (14% vs. 6%, p = 0.411), an absolute difference of 8% is clinically significant, and a lack of statistical significance may be due to lack of power.
Of the included reviews, only two original articles reported on AMR. Isenmann et al. reported a significant increase (p < 0.0001) in ciprofloxacin-resistant organisms in the PABs group (received ciprofloxacin) [35], and Dellinger et al. reported incidence of five bacterial isolates resistant to meropenem in each group [36]. However, the studies did not report which organisms were cultured. Ideally, studies evaluating the role of PABs should include microbiology results and culture sensitivities in patients who subsequently develop IPN or EPI to identify whether the use of PABs increases the incidence of MDR organisms. Subgroup analysis should also be performed to compare mortality of PABs vs. no PABs in patients with IPN and EPI. If sufficient well-designed studies demonstrate an increase in AMR without any reduction in mortality, IPN, EPI, and/or other improvements in study outcomes, this may call for the termination of further studies due to increased risks of harm to the PABs group.
4.5. Local Institutional Practice and Overall Management of Severe Acute Pancreatitis
Locally, in our institution, PABs are not routinely used for patients with SAP or ANP. If required, empirical antibiotics (and not prophylactic) are used for patients with AP and concomitant cholangitis or other EPIs (e.g., pneumonia or UTI). This is justified due to overlapping symptoms, clinical signs, and serologic biomarkers for both acute cholangitis and AP. The only distinction would be blood culture result, which takes 48–72 h, and a patient with suspected cholangitis should not be deprived of antibiotics. Thus, based on our local antibiogram, intravenous amoxicillin–clavulanate is used with a single dose of gentamicin for patients with suspected cholangitis.
For EPI, the choice of empiric antibiotics is based on its source—such as the use of piperacillin–tazobactam with a single dose of vancomycin to cover for hospital-acquired pneumonia. However, should the patient present with fever and/or haemodynamic instability with no localising source, it is up to the clinician to exercise clinical acumen to decide on an appropriate class of antibiotics. In this context, common choice of empiric antibiotics would be meropenem due to its broad-spectrum coverage. However, we also recommend multidisciplinary input. It is essential that the decision is led by clinical pancreatology experts who retain the direct oversight of clinical management. The choice and duration are based on local antibiogram and policies and allow for some subjectivity in clinical decision-making within the governance of local audits that form the local protocols. It is advocated that antibiotics are not a panacea to treat febrile episodes nor magic bullets to bring down elevated inflammatory markers. Lastly, a distinction is made in the ethos of prophylaxis versus therapy. A patient who has a documented infection rightfully deserves antibiotics to improve survival chances and should not be deprived of them. Often, it is witnessed that a patient does not have a documented infection, but the pancreatologist suspects infection based on their clinical wisdom, and this causes a dilemma on two fronts: (a) whether to observe or initiate antibiotics, and (b) if initiated, whether the antibiotic would be labelled as prophylactic or therapeutic. It remains our policy that when a pancreatologist suspects an infection, he/she retains the authority to initiate antibiotics, and such practice should not be claimed as prophylaxis due to its therapeutic intent. It is strongly encouraged to review the antibiotics with aggressive attempts for microbial isolation or consider withdrawal of antibiotics, again guided by the clinical course.
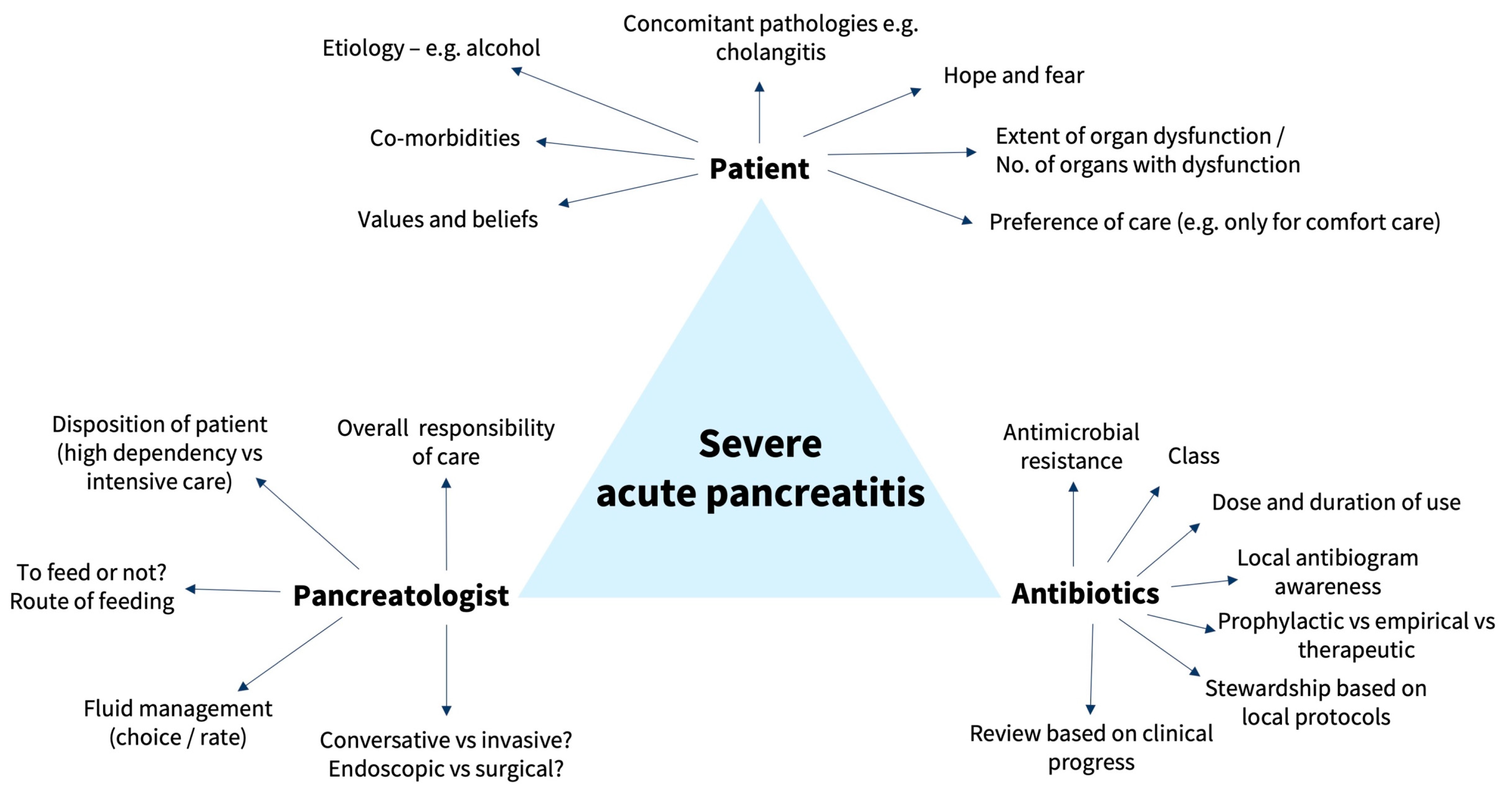
The management of SAP is complex. Chan et al. previously summarised the various controversies in the management of AP—extent of work-up for establishing aetiology of AP, comparison between various risk stratification scores, guidance on choice and amount of fluid resuscitation, indications for ICU admission, mode of nutrition, role of ERCP for gallstone pancreatitis, and indications for invasive interventions in SAP [4]. Fluid resuscitation is critical to restore microcirculation to the pancreas, which has been regarded as the most important pathophysiologic goal for ischemic AP [56]. However, caution is to be taken to avoid excessive fluid replacement, which can cause other complications such as dilutional coagulopathy and reperfusion-mediated injury [8]. Oral and/or enteral feeding should be used (if possible) to reduce the risk of intestinal mucosal atrophy, maintain the intestinal barrier, and prevent bacterial translocation from the gut into the pancreatic necrosis, which can result in IPN and sepsis [57,58]. However, in the event of IPN, drainage and/or debridement of pancreatic necrosis is indicated but should be attempted using a step-up approach via endoscopy or minimally invasive surgery [10,26]. Pancreatic debridement should be attempted at least 4 weeks from the initial diagnosis of SAP in view of the increased morbidity and mortality associated with pancreatic debridement in the acute period [26]. Delayed drainage in IPN was not inferior to immediate drainage; in addition, patients with delayed drainage had fewer invasive interventions compared with the immediate drainage group [59]. We have summarised the important triad and considerations to guide the management of SAP in Figure 1.
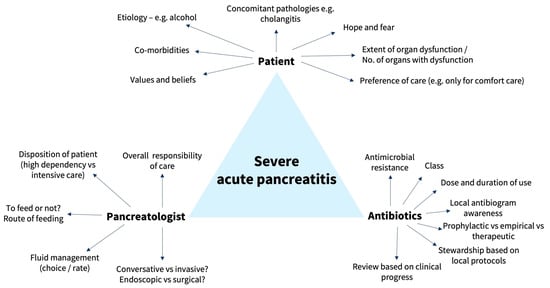
Figure 1.
Important triad and associated factors in the management of severe acute pancreatitis.
4.6. Should More Studies Be Conducted, or Is Existing Evidence Sufficient to Prove a Lack of Benefit?
Most meta-analyses have thus far failed to show a mortality benefit (only n = 2/8 meta-analysis showed reduction in mortality [16,34]) and reduction in IPN (only n = 2/8 showed reduction in IPN [16,32]). This raises the question on how many more studies are required before a conclusion can be definitively made on the use of PABs for AP. One flaw of meta-analyses is that repetitive testing of significance from pooling of results may lead to an overestimation of results when data are sparse, leading to false positives (type 1 error) or false negatives (type 2 error). Trial sequential analysis (TSA) allows for controlling for random errors [60]. Poropat et al. performed a meta-analysis in 2022 on 21 RCTs (PAB n = 703, no PAB n = 680) and concluded that PABs do not reduce mortality or IPN [29]; however, incidence of sepsis, UTI, and LOS were lower in the PAB group. The authors additionally performed TSA and showed that the Z-curve did not cross the constructed monitoring boundaries (i.e., insufficient sample size to conclude that there is indeed reduced sepsis and UTI), and also did not cross the futility boundaries (i.e., insufficient sample size to conclude that mortality is not affected by PABs). With an alpha of 5% and beta of 20%, and an estimated relative risk reduction of 30%, a total of 2714 patients were required (only 1076 patients were included) for mortality (estimated incidence of 10%), and 1383 patients were required (only 512 patients were included) for UTI (estimated incidence of 20%). Hence, further RCTs and subsequent TSA should be conducted to determine if there is indeed a lack of benefit of PABs in AP.
5. Use of Serologic Biomarkers
As AP results in systemic inflammation and release of cytokines, it is therefore not surprising that inflammatory markers such as total white count (TWC) and C-reactive protein (CRP) are raised. Several scoring systems such as the Ranson score, Glasgow–Imrie score and APACHE II score use TWC as a surrogate marker of severity of inflammation i.e., severe AP [4]. Superimposed infection, which may be a sequelae of AP, similarly results in raised inflammatory markers, creating a conundrum on whether raised inflammatory markers are due to worsening inflammation versus a superimposed infection. In our opinion, trends of the markers when reviewed by pancreatology experts are paramount to informing clinical decision-making. We advocate pancreatology experts to retain autonomy to make decisions about antibiotics, as they follow the patients’ daily progress and are directly relevant by virtue of their ability to read and interpret computerised tomography scan images, distinct from non-pancreatology teams, who more often derive information by reading radiology reports or sporadically visit patients and provide episodic inputs.
Procalcitonin (PCT) is an increasingly used biomarker to differentiate between infective and non-infective causes of inflammation with higher specificity and sensitivity [61]. Studies have also been conducted to evaluate its use in severity stratification, such as in acute cholecystitis [62]. However, results have been inconclusive. The PROCAP trial, comparing the use of PCT-guided care vs. standard care, showed that serial trending of PCT was associated with reduced antibiotic use (45% vs. 63%, adjusted risk difference: −15.6%, p = 0.0071) without increasing the incidence of clinical infections or hospital-acquired infections in AP patients [63]. We suggest that PCT be used when faced with a conundrum on whether an infection is suspected, alongside the clinical progress and other clinical parameters of the patient.
Other biochemical markers that have been used to distinguish between IPN vs. sterile necrosis include phospholipase A2 (PLA2) [64], cortisol-binding globulin (CBG) [65], soluble triggering receptor expressed on myeloid cells (sTREM1) [66], and interleukin-6 (IL-6) [67]. However, these biochemical markers are not routinely measured clinically due to accessibility, affordability, availability, and lack of strong evidence to justify economics. Even if evidence does show that these biomarkers are able to predict risk of infection in AP, there is a need to improve their assay methods and lower costs for them to be valuable in clinical practice [68].
6. Role of Prophylactic Anti-Fungals in Acute Pancreatitis
Use of prophylactic anti-fungals is even more controversial in the management of AP. Translocation of gut bacteria has been postulated to be the pathogenesis of AP [40]. However, the gut microbiome also consists of fungi and it is therefore possible that both bacteria and fungi may translocate and colonise the pancreas, resulting in development of secondary infection [69]. Werge et al. and Rasch et al. reported that about 40% of patients with SAP and WON had fungal infection [70,71]. Rasch et al. also reported higher in-hospital mortality in patients with Candida spp.-positive fluid cultures compared to Candida spp.-negative fluid cultures (35.2% (n = 19/54) vs. 13.4% (n = 11/82), p = 0.003) [71].
Given the high incidence of fungal infections with associated increased mortality in AP, this raises the question as to whether prophylactic anti-fungals should be given to all patients, a select group of critically ill patients (e.g., SAP), or patients at risk of deterioration. For instance, female sex (OR: 3.13, 95% CI: 1.28–7.69) and post-ERCP pancreatitis (OR: 4.32, 95% CI: 1.01–18.36) were associated with increased risk of Candida-superimposed infections in ANP [71]. Additionally, broad-spectrum PABs may lead to the development of invasive pancreatic candidiasis due to stimulation of bacterial and Candida overgrowth [72,73]. However, to date, while there have been studies showing that prophylactic anti-fungals may reduce the risk of fungal infections in SAP, no RCTs have been performed to compare anti-fungal vs. control in preventing fungal infections in AP. The AGA clinical practice update also does not recommend the routine use of anti-fungals even when IPN is suspected [26]. Based on the above review, we believe that routine empirical anti-fungal prophylaxis should not be administered in AP and should only be administered in the presence of strongly suspected or documented fungal infection/fungaemia.
7. Conclusions
While SAP only occurs in a minority of patients, it bears high morbidity and mortality. Therapeutic antibiotics provide mortality benefit in patients with IPN, or AP with concomitant cholangitis. However, the role of PABs requires more studies to show a benefit. At present, a clinical conundrum exists; in view of the lack of evidence, choice of PABs should be guided by clinical progress, serologic biomarkers, and multidisciplinary discussions led by pancreatology experts who audit local protocols with organisational governance. Clinicians should also be cognizant of the emergence of AMR and need to rationalise antibiotic administration. On the contrary, there is no role for routine anti-fungal prophylaxis.
Author Contributions
Conceptualisation, K.S.C. and V.G.S.; Methodology, K.S.C.; Software, K.S.C.; Validation, K.S.C. and V.G.S.; Formal Analysis, K.S.C.; Investigation, K.S.C.; Resources, K.S.C.; Data Curation, K.S.C.; Writing—Original Draft Preparation, K.S.C.; Writing—Review and Editing, V.G.S.; Visualisation, V.G.S.; Supervision, V.G.S.; Project Administration, K.S.C. and V.G.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Clancy, T.E.; Benoit, E.P.; Ashley, S.W. Current management of acute pancreatitis. J. Gastrointest. Surg. 2005, 9, 440–452. [Google Scholar] [CrossRef]
- Triester, S.L.; Kowdley, K.V. Prognostic factors in acute pancreatitis. J. Clin. Gastroenterol. 2002, 34, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Popa, C.C.; Badiu, D.C.; Rusu, O.C.; Grigorean, V.T.; Neagu, S.I.; Strugaru, C.R. Mortality prognostic factors in acute pancreatitis. J. Med. Life 2016, 9, 413–418. [Google Scholar] [PubMed]
- Chan, K.S.; Shelat, V.G. Diagnosis, severity stratification and management of adult acute pancreatitis–current evidence and controversies. World J. Gastrointest. Surg. 2022, 14, 1179–1197. [Google Scholar] [CrossRef] [PubMed]
- Schepers, N.J.; Bakker, O.J.; Besselink, M.G.; Ahmed Ali, U.; Bollen, T.L.; Gooszen, H.G.; van Santvoort, H.C.; Bruno, M.J. Impact of characteristics of organ failure and infected necrosis on mortality in necrotising pancreatitis. Gut 2019, 68, 1044–1051. [Google Scholar] [CrossRef] [PubMed]
- van Santvoort, H.C.; Bakker, O.J.; Bollen, T.L.; Besselink, M.G.; Ahmed Ali, U.; Schrijver, A.M.; Boermeester, M.A.; van Goor, H.; Dejong, C.H.; van Eijck, C.H.; et al. A conservative and minimally invasive approach to necrotizing pancreatitis improves outcome. Gastroenterology 2011, 141, 1254–1263. [Google Scholar] [CrossRef] [PubMed]
- Bang, J.Y.; Wilcox, C.M.; Arnoletti, J.P.; Varadarajulu, S. Superiority of endoscopic interventions over minimally invasive surgery for infected necrotizing pancreatitis: Meta-analysis of randomized trials. Dig. Endosc. 2020, 32, 298–308. [Google Scholar] [CrossRef] [PubMed]
- Working Group IAP/APA Acute Pancreatitis Guidelines. IAP/APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology 2013, 13, e1–e15. [Google Scholar] [CrossRef]
- Lee, S.H.; Choe, J.W.; Cheon, Y.K.; Choi, M.; Jung, M.K.; Jang, D.K.; Jo, J.H.; Lee, J.M.; Kim, E.J.; Han, S.Y.; et al. Revised Clinical Practice Guidelines of the Korean Pancreatobiliary Association for Acute Pancreatitis. Gut Liver 2022, 17, 34–48. [Google Scholar] [CrossRef] [PubMed]
- Leppäniemi, A.; Tolonen, M.; Tarasconi, A.; Segovia-Lohse, H.; Gamberini, E.; Kirkpatrick, A.W.; Ball, C.G.; Parry, N.; Sartelli, M.; Wolbrink, D.; et al. 2019 WSES guidelines for the management of severe acute pancreatitis. World J. Emerg. Surg. 2019, 14, 27. [Google Scholar] [CrossRef] [PubMed]
- Crockett, S.D.; Wani, S.; Gardner, T.B.; Falck-Ytter, Y.; Barkun, A.N. American Gastroenterological Association Institute Guideline on Initial Management of Acute Pancreatitis. Gastroenterology 2018, 154, 1096–1101. [Google Scholar] [CrossRef] [PubMed]
- Yokoe, M.; Takada, T.; Mayumi, T.; Yoshida, M.; Isaji, S.; Wada, K.; Itoi, T.; Sata, N.; Gabata, T.; Igarashi, H.; et al. Japanese guidelines for the management of acute pancreatitis: Japanese Guidelines 2015. J. Hepatobiliary Pancreat. Sci. 2015, 22, 405–432. [Google Scholar] [CrossRef]
- Jaber, S.; Garnier, M.; Asehnoune, K.; Bounes, F.; Buscail, L.; Chevaux, J.B.; Dahyot-Fizelier, C.; Darrivere, L.; Jabaudon, M.; Joannes-Boyau, O.; et al. Guidelines for the management of patients with severe acute pancreatitis, 2021. Anaesth. Crit. Care Pain Med. 2022, 41, 101060. [Google Scholar] [CrossRef] [PubMed]
- Banks, P.A.; Freeman, M.L. Practice guidelines in acute pancreatitis. Am. J. Gastroenterol. 2006, 101, 2379–2400. [Google Scholar] [CrossRef] [PubMed]
- Working Party of the British Society of Gastroenterology; Association of Surgeons of Great Britain and Ireland; Pancreatic Society of Great Britain and Ireland; Association of Upper GI Surgeons of Great Britain and Ireland. UK guidelines for the management of acute pancreatitis. Gut 2005, 54 (Suppl. 3), iii1–iii9. [Google Scholar] [CrossRef] [PubMed]
- Ukai, T.; Shikata, S.; Inoue, M.; Noguchi, Y.; Igarashi, H.; Isaji, S.; Mayumi, T.; Yoshida, M.; Takemura, Y.C. Early prophylactic antibiotics administration for acute necrotizing pancreatitis: A meta-analysis of randomized controlled trials. J. Hepatobiliary Pancreat. Sci. 2015, 22, 316–321. [Google Scholar] [CrossRef]
- Guo, D.; Dai, W.; Shen, J.; Zhang, M.; Shi, Y.; Jiang, K.; Guo, L. Assessment of Prophylactic Carbapenem Antibiotics Administration for Severe Acute Pancreatitis: An Updated Systematic Review and Meta-Analysis. Digestion 2022, 103, 183–191. [Google Scholar] [CrossRef]
- Lluís, N.; Asbun, H.; Besselink, M.G.; Capurso, G.; Garg, P.K.; Gelrud, A.; Khannoussi, W.; Lee, H.S.; Leppäniemi, A.; Löhr, J.M.; et al. International multidisciplinary survey on the initial management of acute pancreatitis: Perspective of point-of-care specialists focused on daily practice. J. Hepatobiliary Pancreat. Sci. 2022, 30, 325–337. [Google Scholar] [CrossRef] [PubMed]
- Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef] [PubMed]
- Banks, P.A.; Bollen, T.L.; Dervenis, C.; Gooszen, H.G.; Johnson, C.D.; Sarr, M.G.; Tsiotos, G.G.; Vege, S.S. Classification of acute pancreatitis—2012: Revision of the Atlanta classification and definitions by international consensus. Gut 2013, 62, 102–111. [Google Scholar] [CrossRef]
- Dellinger, E.P.; Forsmark, C.E.; Layer, P.; Lévy, P.; Maraví-Poma, E.; Petrov, M.S.; Shimosegawa, T.; Siriwardena, A.K.; Uomo, G.; Whitcomb, D.C.; et al. Determinant-based classification of acute pancreatitis severity: An international multidisciplinary consultation. Ann. Surg. 2012, 256, 875–880. [Google Scholar] [CrossRef] [PubMed]
- Werge, M.; Novovic, S.; Schmidt, P.N.; Gluud, L.L. Infection increases mortality in necrotizing pancreatitis: A systematic review and meta-analysis. Pancreatology 2016, 16, 698–707. [Google Scholar] [CrossRef] [PubMed]
- Balthazar, E.J.; Robinson, D.L.; Megibow, A.J.; Ranson, J.H. Acute pancreatitis: Value of CT in establishing prognosis. Radiology 1990, 174, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Pan, G.; Wan, M.H.; Xie, K.L.; Li, W.; Hu, W.M.; Liu, X.B.; Tang, W.F.; Wu, H. Classification and Management of Pancreatic Pseudocysts. Medicine 2015, 94, e960. [Google Scholar] [CrossRef] [PubMed]
- van Santvoort, H.C.; Besselink, M.G.; Bakker, O.J.; Hofker, H.S.; Boermeester, M.A.; Dejong, C.H.; van Goor, H.; Schaapherder, A.F.; van Eijck, C.H.; Bollen, T.L.; et al. A step-up approach or open necrosectomy for necrotizing pancreatitis. N. Engl. J. Med. 2010, 362, 1491–1502. [Google Scholar] [CrossRef] [PubMed]
- Baron, T.H.; DiMaio, C.J.; Wang, A.Y.; Morgan, K.A. American Gastroenterological Association Clinical Practice Update: Management of Pancreatic Necrosis. Gastroenterology 2020, 158, 67–75.e61. [Google Scholar] [CrossRef] [PubMed]
- Podda, M.; Pacella, D.; Pellino, G.; Coccolini, F.; Giordano, A.; Di Saverio, S.; Pata, F.; Ielpo, B.; Virdis, F.; Damaskos, D.; et al. coMpliAnce with evideNce-based cliniCal guidelines in the managemenT of acute biliaRy pancreAtitis: The MANCTRA-1 international audit. Pancreatology 2022, 22, 902–916. [Google Scholar] [CrossRef] [PubMed]
- Calomino, N.; Poto, G.E.; Carbone, L.; Bagnacci, G.; Piccioni, S.; Andreucci, E.; Nenci, L.; Marano, L.; Verre, L.; Petrioli, R.; et al. Neuroendocrine tumors’ patients treated with somatostatin analogue could complicate with emergency cholecystectomy. Ann. Ital. Chir. 2023, 94, 518–522. [Google Scholar] [PubMed]
- Poropat, G.; Goričanec, K.; Lacković, A.; Kresović, A.; Lončarić, A.; Marušić, M. Systematic Review with Trial Sequential Analysis of Prophylactic Antibiotics for Acute Pancreatitis. Antibiotics 2022, 11, 1191. [Google Scholar] [CrossRef]
- Ding, N.; Sun, Y.H.; Wen, L.M.; Wang, J.H.; Yang, J.H.; Cheng, K.; Lin, H.; Chen, Q.L. Assessment of prophylactic antibiotics administration for acute pancreatitis: A meta-analysis of randomized controlled trials. Chin. Med. J. 2020, 133, 212–220. [Google Scholar] [CrossRef]
- Wittau, M.; Mayer, B.; Scheele, J.; Henne-Bruns, D.; Dellinger, E.P.; Isenmann, R. Systematic review and meta-analysis of antibiotic prophylaxis in severe acute pancreatitis. Scand. J. Gastroenterol. 2011, 46, 261–270. [Google Scholar] [CrossRef]
- Yao, L.; Huang, X.; Li, Y.; Shi, R.; Zhang, G. Prophylactic antibiotics reduce pancreatic necrosis in acute necrotizing pancreatitis: A meta-analysis of randomized trials. Dig. Surg. 2010, 27, 442–449. [Google Scholar] [CrossRef]
- Villatoro, E.; Mulla, M.; Larvin, M. Antibiotic therapy for prophylaxis against infection of pancreatic necrosis in acute pancreatitis. Cochrane Database Syst. Rev. 2010, 2010, Cd002941. [Google Scholar] [CrossRef] [PubMed]
- Lim, C.L.; Lee, W.; Liew, Y.X.; Tang, S.S.; Chlebicki, M.P.; Kwa, A.L. Role of antibiotic prophylaxis in necrotizing pancreatitis: A meta-analysis. J. Gastrointest. Surg. 2015, 19, 480–491. [Google Scholar] [CrossRef] [PubMed]
- Isenmann, R.; Rünzi, M.; Kron, M.; Kahl, S.; Kraus, D.; Jung, N.; Maier, L.; Malfertheiner, P.; Goebell, H.; Beger, H.G. Prophylactic antibiotic treatment in patients with predicted severe acute pancreatitis: A placebo-controlled, double-blind trial. Gastroenterology 2004, 126, 997–1004. [Google Scholar] [CrossRef] [PubMed]
- Dellinger, E.P.; Tellado, J.M.; Soto, N.E.; Ashley, S.W.; Barie, P.S.; Dugernier, T.; Imrie, C.W.; Johnson, C.D.; Knaebel, H.P.; Laterre, P.F.; et al. Early antibiotic treatment for severe acute necrotizing pancreatitis: A randomized, double-blind, placebo-controlled study. Ann. Surg. 2007, 245, 674–683. [Google Scholar] [CrossRef] [PubMed]
- Kiat, T.T.J.; Gunasekaran, S.K.; Junnarkar, S.P.; Low, J.K.; Woon, W.; Shelat, V.G. Are traditional scoring systems for severity stratification of acute pancreatitis sufficient? Ann. Hepato-Biliary-Pancreat. Surg. 2018, 22, 105–115. [Google Scholar] [CrossRef] [PubMed]
- Garg, P.K.; Singh, V.P. Organ Failure Due to Systemic Injury in Acute Pancreatitis. Gastroenterology 2019, 156, 2008–2023. [Google Scholar] [CrossRef] [PubMed]
- Garret, C.; Péron, M.; Reignier, J.; Le Thuaut, A.; Lascarrou, J.B.; Douane, F.; Lerhun, M.; Archambeaud, I.; Brulé, N.; Bretonnière, C.; et al. Risk factors and outcomes of infected pancreatic necrosis: Retrospective cohort of 148 patients admitted to the ICU for acute pancreatitis. United Eur. Gastroenterol. J. 2018, 6, 910–918. [Google Scholar] [CrossRef]
- Mourad, M.M.; Evans, R.; Kalidindi, V.; Navaratnam, R.; Dvorkin, L.; Bramhall, S.R. Prophylactic antibiotics in acute pancreatitis: Endless debate. Ann. R. Coll. Surg. Engl. 2017, 99, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Kryvoruchko, I.A.; Boyko, V.V.; Sartelli, M.; Ivanova, Y.V.; Yevtushenko, D.O.; Honcharov, A.S. Pancreatic Necrosis Infection as a Determinant of Multiple Organ Failure and Mortality in Acute Pancreatitis. Pathogens 2023, 12, 428. [Google Scholar] [CrossRef]
- Marstrand-Joergensen, M.R.; Bertilsson, S.; Kalaitzakis, E. Extrapancreatic infections are common in acute pancreatitis and they are related to organ failure: A population-based study. Eur. J. Gastroenterol. Hepatol. 2020, 32, 1293–1300. [Google Scholar] [CrossRef] [PubMed]
- Howard, T.J.; Temple, M.B. Prophylactic antibiotics alter the bacteriology of infected necrosis in severe acute pancreatitis. J. Am. Coll. Surg. 2002, 195, 759–767. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.S.; Lee, S.K.; Park, D.H.; Lee, S.S.; Seo, D.W.; Kim, M.H.; Chong, Y.P. Emergence of multidrug resistant infection in patients with severe acute pancreatitis. Pancreatology 2014, 14, 450–453. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Ferrer, R.; Martin-Loeches, I.; Phillips, G.; Osborn, T.M.; Townsend, S.; Dellinger, R.P.; Artigas, A.; Schorr, C.; Levy, M.M. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: Results from a guideline-based performance improvement program. Crit. Care Med. 2014, 42, 1749–1755. [Google Scholar] [CrossRef] [PubMed]
- Chung, W.T.G.; Shafi, H.; Seah, J.; Purnima, P.; Patun, T.; Kam, K.Q.; Seah, V.X.F.; Ong, R.Y.L.; Lin, L.; Choo, R.S.M.; et al. National surgical antibiotic prophylaxis guideline in Singapore. Ann. Acad. Med. Singap. 2022, 51, 695–711. [Google Scholar] [CrossRef] [PubMed]
- Zelenitsky, S.A. Effective Antimicrobial Prophylaxis in Surgery: The Relevance and Role of Pharmacokinetics-Pharmacodynamics. Antibiotics 2023, 12, 1738. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, M.; Isenmann, R.; Meyer, H.; Beger, H.G. Antibiotic use in necrotizing pancreatitis. Results of a controlled study. Dtsch. Med. Wochenschr. 1997, 122, 356–361. [Google Scholar] [CrossRef] [PubMed]
- Ho, H.S.; Frey, C.F. The role of antibiotic prophylaxis in severe acute pancreatitis. Arch. Surg. 1997, 132, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Mazuski, J.E.; Tessier, J.M.; May, A.K.; Sawyer, R.G.; Nadler, E.P.; Rosengart, M.R.; Chang, P.K.; O’Neill, P.J.; Mollen, K.P.; Huston, J.M.; et al. The Surgical Infection Society Revised Guidelines on the Management of Intra-Abdominal Infection. Surg. Infect. 2017, 18, 1–76. [Google Scholar] [CrossRef]
- Gomi, H.; Solomkin, J.S.; Schlossberg, D.; Okamoto, K.; Takada, T.; Strasberg, S.M.; Ukai, T.; Endo, I.; Iwashita, Y.; Hibi, T.; et al. Tokyo Guidelines 2018: Antimicrobial therapy for acute cholangitis and cholecystitis. J. Hepato-Biliary-Pancreat. Sci. 2018, 25, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.S.; Shelat, V. Pyogenic Liver Abscess. In The IASGO Textbook of Multi-Disciplinary Management of Hepato-Pancreato-Biliary Diseases; Makuuchi, M., Kokudo, N., Popescu, I., Belghiti, J., Han, H.-S., Takaori, K., Duda, D.G., Eds.; Springer Nature Singapore: Singapore, 2022; pp. 509–519. [Google Scholar] [CrossRef]
- Røkke, O.; Harbitz, T.B.; Liljedal, J.; Pettersen, T.; Fetvedt, T.; Heen, L.; Skreden, K.; Viste, A. Early treatment of severe pancreatitis with imipenem: A prospective randomized clinical trial. Scand. J. Gastroenterol. 2007, 42, 771–776. [Google Scholar] [CrossRef] [PubMed]
- Toman, J.; Zachary Porterfield, J.; Randall, M.W.; Kumar, A.; Farrior, E.H. Efficacy of 24 hours versus 5 days of prophylactic antibiotics for the prevention of surgical site infection in outpatient elective facial plastic surgery. JPRAS Open 2024, 40, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Hackert, T.; Hartwig, W.; Fritz, S.; Schneider, L.; Strobel, O.; Werner, J. Ischemic acute pancreatitis: Clinical features of 11 patients and review of the literature. Am. J. Surg. 2009, 197, 450–454. [Google Scholar] [CrossRef] [PubMed]
- Dervenis, C.; Smailis, D.; Hatzitheoklitos, E. Bacterial translocation and its prevention in acute pancreatitis. J. Hepatobiliary Pancreat. Surg. 2003, 10, 415–418. [Google Scholar] [CrossRef] [PubMed]
- Schörghuber, M.; Fruhwald, S. Effects of enteral nutrition on gastrointestinal function in patients who are critically ill. Lancet Gastroenterol. Hepatol. 2018, 3, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Boxhoorn, L.; van Dijk, S.M.; van Grinsven, J.; Verdonk, R.C.; Boermeester, M.A.; Bollen, T.L.; Bouwense, S.A.W.; Bruno, M.J.; Cappendijk, V.C.; Dejong, C.H.C.; et al. Immediate versus Postponed Intervention for Infected Necrotizing Pancreatitis. N. Engl. J. Med. 2021, 385, 1372–1381. [Google Scholar] [CrossRef] [PubMed]
- Brok, J.; Thorlund, K.; Gluud, C.; Wetterslev, J. Trial sequential analysis reveals insufficient information size and potentially false positive results in many meta-analyses. J. Clin. Epidemiol. 2008, 61, 763–769. [Google Scholar] [CrossRef]
- Lee, C.C.; Chen, S.Y.; Tsai, C.L.; Wu, S.C.; Chiang, W.C.; Wang, J.L.; Sun, H.Y.; Chen, S.C.; Chen, W.J.; Hsueh, P.R. Prognostic value of mortality in emergency department sepsis score, procalcitonin, and C-reactive protein in patients with sepsis at the emergency department. Shock 2008, 29, 322–327. [Google Scholar] [CrossRef] [PubMed]
- Yaow, C.Y.L.; Chong, R.I.H.; Chan, K.S.; Chia, C.T.W.; Shelat, V.G. Should Procalcitonin Be Included in Acute Cholecystitis Guidelines? A Systematic Review. Medicina 2023, 59, 805. [Google Scholar] [CrossRef] [PubMed]
- Siriwardena, A.K.; Jegatheeswaran, S.; Mason, J.M. A procalcitonin-based algorithm to guide antibiotic use in patients with acute pancreatitis (PROCAP): A single-centre, patient-blinded, randomised controlled trial. Lancet Gastroenterol. Hepatol. 2022, 7, 913–921. [Google Scholar] [CrossRef]
- Mayer, J.; Rau, B.; Grewe, M.; Schoenberg, M.H.; Nevalainen, T.J.; Beger, H.G. Secretory phospholipase A2 in patients with infected pancreatic necroses in acute pancreatitis. Pancreas 1998, 17, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Muller, C.A.; Belyaev, O.; Vogeser, M.; Weyhe, D.; Gloor, B.; Strobel, O.; Werner, J.; Borgstrom, A.; Buchler, M.W.; Uhl, W. Corticosteroid-binding globulin: A possible early predictor of infection in acute necrotizing pancreatitis. Scand. J. Gastroenterol. 2007, 42, 1354–1361. [Google Scholar] [CrossRef] [PubMed]
- Lu, Z.; Liu, Y.; Dong, Y.H.; Zhan, X.B.; Du, Y.Q.; Gao, J.; Gong, Y.F.; Li, Z.S. Soluble triggering receptor expressed on myeloid cells in severe acute pancreatitis: A biological marker of infected necrosis. Intensive Care Med. 2012, 38, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Müller, C.A.; Uhl, W.; Printzen, G.; Gloor, B.; Bischofberger, H.; Tcholakov, O.; Büchler, M.W. Role of procalcitonin and granulocyte colony stimulating factor in the early prediction of infected necrosis in severe acute pancreatitis. Gut 2000, 46, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Petrovic, N.; Grove, C.; Langton, P.E.; Misso, N.L.; Thompson, P.J. A simple assay for a human serum phospholipase A2 that is associated with high-density lipoproteins. J. Lipid Res. 2001, 42, 1706–1713. [Google Scholar] [CrossRef] [PubMed]
- Otsuka, Y.; Kamata, K.; Minaga, K.; Watanabe, T.; Kudo, M. Pancreatic colonization of fungi in the development of severe acute pancreatitis. Front. Cell. Infect. Microbiol. 2022, 12, 940532. [Google Scholar] [CrossRef] [PubMed]
- Werge, M.; Roug, S.; Novovic, S.; Schmidt, P.N.; Hansen, E.F.; Knudsen, J.D. Fungal Infections in Patients With Walled-off Pancreatic Necrosis. Pancreas 2016, 45, 1447–1451. [Google Scholar] [CrossRef] [PubMed]
- Rasch, S.; Mayr, U.; Phillip, V.; Schmid, R.M.; Huber, W.; Algül, H.; Lahmer, T. Increased risk of candidemia in patients with necrotising pancreatitis infected with candida species. Pancreatology 2018, 18, 630–634. [Google Scholar] [CrossRef] [PubMed]
- Horibe, M.; Sanui, M.; Sasaki, M.; Honda, H.; Ogura, Y.; Namiki, S.; Sawano, H.; Goto, T.; Ikeura, T.; Takeda, T.; et al. Impact of Antimicrobial Prophylaxis for Severe Acute Pancreatitis on the Development of Invasive Candidiasis: A Large Retrospective Multicenter Cohort Study. Pancreas 2019, 48, 537–543. [Google Scholar] [CrossRef] [PubMed]
- Chakrabarti, A.; Rao, P.; Tarai, B.; Shivaprakash, M.R.; Wig, J. Candida in acute pancreatitis. Surg. Today 2007, 37, 207–211. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).