
The Use of Cefiderocol as Salvage Therapy in an Infant Receiving ECMO and Continuous Renal Replacement Therapy
 ,
,  , ,
, ,
Abstract
:1. Introduction
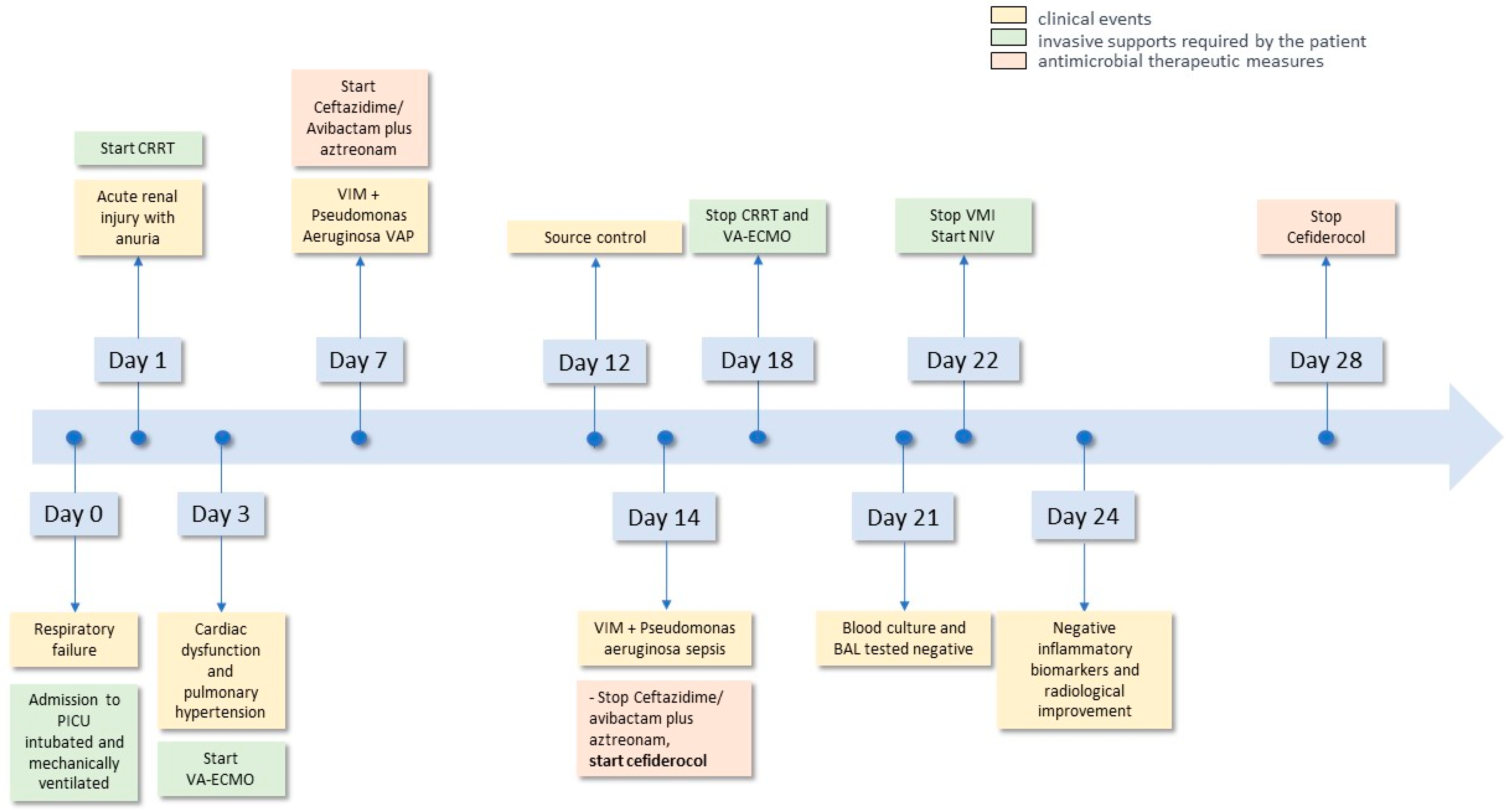
2. Case Report
3. Discussion
4. Materials and Methods
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Canton, R.; Doi, Y.; Simner, P.J. Treatment of carbapenem-resistant Pseudomonas aeruginosa infections: A case for cefiderocol. Expert Rev. Anti-Infect. Ther. 2022, 20, 1077–1094. [Google Scholar] [CrossRef] [PubMed]
- Livermore, D.M. Multiple mechanisms of antimicrobial resistance in Pseudomonas aeruginosa: Our worstnightmare? Clin. Infect. Dis. 2002, 34, 634–640. [Google Scholar] [CrossRef] [PubMed]
- Simner, P.J.; Opene, B.N.A.; Chambers, K.K.; Naumann, M.E.; Carroll, K.C.; Tamma, P.D. Carbapenemase detection among carbapenem-resistant glucose-nonfermenting gram-negative bacilli. J. Clin. Microbiol. 2017, 55, 2858–2864. [Google Scholar] [CrossRef] [PubMed]
- Kanj, S.S.; Bassetti, M.; Kiratisin, P.; Rodrigues, C.; Villegas, M.V.; Yu, Y.; van Duin, D. Clinical data from studies involving novel antibiotics to treat multidrug-resistant Gram-negative bacterial infections. Int. J. Antimicrob. Agents 2022, 60, 106633. [Google Scholar] [CrossRef]
- Satlin, M.J.; Simner, P.J.; Slover, C.M.; Yamano, Y.; Nagata, T.D.; Portsmouth, S. Cefiderocol Treatment for Patients with Multidrug- and Carbapenem-Resistant Pseudomonas aeruginosa Infections in the Compassionate Use Program. Antimicrob. Agents Chemother. 2023, 67, e0019423. [Google Scholar] [CrossRef]
- Vardakas, K.Z.; Voulgaris, G.L.; Maliaros, A.; Samonis, G.; Falagas, M.E. Prolonged versus short-term intravenous infusion of antipseudomonal β-lactams for patients with sepsis: A systematic review and meta-analysis of randomised trials. Lancet Infect. Dis. 2018, 18, 108–120. [Google Scholar] [CrossRef]
- Rhodes, N.J.; Liu, J.; O’donnell, J.N.; Dulhunty, J.M.; Abdul-Aziz, M.H.; Berko, P.Y.; Nadler, B.; Lipman, J.; Roberts, J.A. Prolonged infusion piperacillin-tazobactam decreases mortality and improves outcomes in severely ill patients: Results of a systematic review and meta-analysis. Crit. Care Med. 2018, 46, 236–243. [Google Scholar] [CrossRef]
- Kondo, Y.; Ota, K.; Imura, H.; Hara, N.; Shime, N. Prolonged versus intermittent b-lactam antibiotics intravenous infusion strategy in sepsis or septic shock patients: A systematic review with meta-analysis and trial sequential analysis of randomized trials. J. Intensive Care 2020, 8, 77. [Google Scholar] [CrossRef]
- ClinicalTrials.gov. A Study to Assess the Safety, Tolerability, and Pharmacokinetics of Single and Multiple Doses of Cefiderocol in Hospitalized Pediatric Participants. 2020; ClinicalTrials.gov Identifier: NCT04335539. Available online: https://clinicaltrials.gov/ct2/show/NCT04335539 (accessed on 10 May 2023).
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 13.1. 2023. Available online: http://www.eucast.org (accessed on 10 May 2023).
- Monari, C.; Spagnuolo, F.; Pisaturo, M.; Ascione, S.; Donnarumma, G.; Calò, F.; Caredda, E.; Montella, F.; Maietta, A.; Montaldo, P.; et al. Bloodstream Infection Due to a VIM-Metallo-β-Lactamase-Producing Klebsiella pneumoniae Treated with Cefiderocol in a Preterm Newborn. Infect. Dis. Ther. 2023, 12, 727–734. [Google Scholar] [CrossRef]
- ClinicalTrial.gov. A Study to Assess the Safety, Tolerability, and Pharmacokinetics of Cefiderocol in Hospitalized Pediatric Participants. ClinicalTrials.gov Identifier: NCT04215991. Available online: https://clinicaltrials.gov/ct2/show/NCT04215991?term=cefiderocol&draw=2&rank=10 (accessed on 10 May 2023).
- Gatti, M.; Giannella, M.; Rinaldi, M.; Gaibani, P.; Viale, P.; Pea, F. Pharmacokinetic/Pharmacodynamic Analysis of Continuous-Infusion Fosfomycin in Combination with Extended-Infusion Cefiderocol or Continuous-Infusion Ceftazidime-Avibactam in a Case Series of Difficult-to-Treat Resistant Pseudomonas aeruginosa Bloodstream Infections and/or Hospital-Acquired Pneumonia. Antibiotics 2022, 11, 1739. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Antimicrobial Resistance in the EU/EEA (EARS-Net)—Annual Epidemiological Report 2022; ECDC: Stockholm, Sweden, 2023. [Google Scholar]
- Tenover, F.C.; Nicolau, D.P.; Gill, C.M. Carbapenemase-producing Pseudomonas aeruginosa—An emerging challenge. Emerg. Microbes Infect. 2022, 11, 811–814. [Google Scholar] [CrossRef] [PubMed]
- Zasowski, E.J.; Rybak, J.M.; Rybak, M.J. The β-Lactams Strike Back: Ceftazidime-Avibactam. Pharmacotherapy 2015, 35, 755–770. [Google Scholar] [CrossRef]
- Logan, L.K.; Bonomo, R.A. Metallo-β-Lactamase (MBL)-Producing Enterobacteriaceae in United States Children. Open Forum Infect. Dis. 2016, 3, ofw090. [Google Scholar] [CrossRef] [PubMed]
- Biagi, M.; Wu, T.; Lee, M.; Patel, S.; Butler, D.; Wenzler, E. Searching for the Optimal Treatment for Metallo- and Serine-β-Lactamase Producing Enterobacteriaceae: Aztreonam in Combination with Ceftazidime-avibactam or Meropenem-vaborbactam. Antimicrob. Agents Chemother. 2019, 63, AAC.01426-19. [Google Scholar] [CrossRef] [PubMed]
- Mularoni, A.; Mezzatesta, M.L.; Pilato, M.; Medaglia, A.A.; Cervo, A.; Bongiorno, D.; Aprile, A.; Luca, A.; Stefani, S.; Grossi, P. Combination of aztreonam, ceftazidime-avibactam and amikacin in the treatment of VIM-1 Pseudomonas aeruginosa ST235 osteomyelitis. Int. J. Infect. Dis. 2021, 108, 510–512. [Google Scholar] [CrossRef]
- Sempere, A.; Viñado, B.; Los-Arcos, I.; Campany, D.; Larrosa, N.; Fernández-Hidalgo, N.; Rodríguez-Pardo, D.; González-López, J.J.; Nuvials, X.; Almirante, B.; et al. Ceftazidime-Avibactam plus Aztreonam for the Treatment of Infections by VIM-Type-Producing Gram-Negative Bacteria. Antimicrob. Agents Chemother. 2022, 66, e0075122. [Google Scholar] [CrossRef]
- Lee, M.; Abbey, T.; Biagi, M.; Wenzler, E. Activity of aztreonam in combination with ceftazidime–avibactam against serine- and metallo-β-lactamase–producing Pseudomonas aeruginosa. Diagn. Microbiol. Infect. Dis. 2020, 99, 115227. [Google Scholar] [CrossRef]
- Summary of Product Characteristics: Zavicefta 2 g/0.5 g Powder for Concentrate for Solution for Infusion. Pfizer. Available online: https://www.ema.europa.eu/documents/product-information/zavicefta-epar-product-information_en.pdf (accessed on 10 May 2023).
- Shekar, K.; Fraser, J.F.; Smith, M.T.; Roberts, J.A. Pharmacokinetic changes in patients receiving extracorporeal membrane oxygenation. J. Crit. Care 2012, 27, 741.e9–741.e18. [Google Scholar] [CrossRef]
- Fresán, D.; Luque, S.; Sorlí, L.; Grau, S. Pharmacokinetics/pharmacodynamics and therapeutic drug monitoring of ceftazidime/avibactam administered by continuous infusion in patients with MDR Gram-negative bacterial infections—Authors’ response. J. Antimicrob. Chemother. 2023, 78, 2385–2386. [Google Scholar] [CrossRef]
- Tamma, P.D.; Doi, Y.; Bonomo, R.A.; Johnson, J.K.; Simner, P.J.; Antibacterial Resistance Leadership Group. A Primer on AmpC β-Lactamases: Necessary Knowledge for an Increasingly Multidrug-resistant World. Clin. Infect. Dis. 2019, 69, 1446–1455. [Google Scholar] [CrossRef]
- Ito, A.; Nishikawa, T.; Matsumoto, S.; Yoshizawa, H.; Sato, T.; Nakamura, R.; Tsuji, M.; Yamano, Y. Siderophore Cephalosporin Cefiderocol Utilizes Ferric Iron Transporter Systems for Antibacterial Activity against Pseudomonas aeruginosa. Antimicrob. Agents Chemother. 2016, 60, 7396–7401. [Google Scholar] [CrossRef] [PubMed]
- Berry, A.V.; Conelius, A.; Gluck, J.A.; Nicolau, D.P.; Kuti, J.L. Cefiderocol is Not Sequestered in an Ex Vivo Extracorporeal Membrane Oxygenation (ECMO) Circuit. Eur. J. Drug Metab. Pharmacokinet. 2023, 48, 437–441. [Google Scholar] [CrossRef] [PubMed]
- Wei, X.; Naseer, S.; Weinstein, E.A.; Iarikov, D.; Nambiar, S.; Reynolds, K.S.; Jang, S.H. Cefiderocol Dosing for Patients Receiving Continuous Renal Replacement Therapy. Clin. Pharmacol. Ther. 2022, 112, 1004–1007. [Google Scholar] [CrossRef] [PubMed]
- Wenzler, E.; Butler, D.; Tan, X.; Katsube, T.; Wajima, T. Pharmacokinetics, Pharmacodynamics, and Dose Optimization of Cefiderocol during Continuous Renal Replacement Therapy. Clin. Pharmacokinet. 2022, 61, 539–552. [Google Scholar] [CrossRef]
- FETROJA (Cefiderocol) for Injection, for Intravenous Use. Initial U.S. Approval: 2019. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/209445s004lbl.pdf (accessed on 10 May 2023).
- Cairoli, S.; Simeoli, R.; Tarchi, M.; Dionisi, M.; Vitale, A.; Perioli, L.; Dionisi-Vici, C.; Goffredo, B.M. A new HPLC–DAD method for contemporary quantification of 10 antibiotics for therapeutic drug monitoring of critically ill pediatric patients. Biomed. Chromatogr. 2020, 34, e4880. [Google Scholar] [CrossRef]

{kind=link}
| Day 1 | Day 7 | Day 14 | Day 28 | Reference Values | |
|---|---|---|---|---|---|
| Temperature (°C) | 37.4 | 38 | 38.3 | 36.8 | - |
| Hemoglobin (g/L) | 11.3 | 11.7 | 8.3 | 9.5 | 10.50–15.50 |
| Leukocytes /μL) | 8.57 | 31.03 | 22.26 | 11.88 | 6.00–17.00 |
| Neutrophils /μL) | 5.99 | 27.15 | 16.10 | 3.130 | 2.00–9.00 |
| Platelets /μL) | 92 | 494 | 72 | 260 | 150–450 |
| CRP (mg/dL) | 1.45 | 7.84 | 13.07 | 0.15 | <0.50 |
| Procalcitonin (ng/mL) | 0.39 | 3 | 8.13 | 0.1 | <0.5 |
| Creatinine (mg/dL) | 0.2 | 0.2 | 0.16 | 0.2 | 0.16–0.39 |
| BUN (mg/dL) | 22 | 8 | 6 | 8 | 4–19 |
| INR | 1.28 | 1.87 | 1.51 | 1.15 | 0.86–1.22 |
| D-dimers (µg/mL) | 3.50 | 3.43 | 0.73 | 0.5 | <0.50 |
| Blood cultures | - | negative | PA-VIM | negative | negative |
| BAL cultures | - | PA-VIM | PA-VIM | negative | negative |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mercadante, S.; Tripiciano, C.; Romani, L.; Di Nardo, M.; Bottari, G.; Goffredo, B.M.; Simeoli, R.; Guzzo, I.; Lancella, L.; Antachopoulos, C.; et al. The Use of Cefiderocol as Salvage Therapy in an Infant Receiving ECMO and Continuous Renal Replacement Therapy. Antibiotics 2024, 13, 37. https://doi.org/10.3390/antibiotics13010037
Mercadante S, Tripiciano C, Romani L, Di Nardo M, Bottari G, Goffredo BM, Simeoli R, Guzzo I, Lancella L, Antachopoulos C, et al. The Use of Cefiderocol as Salvage Therapy in an Infant Receiving ECMO and Continuous Renal Replacement Therapy. Antibiotics. 2024; 13(1):37. https://doi.org/10.3390/antibiotics13010037
Chicago/Turabian StyleMercadante, Stefania, Costanza Tripiciano, Lorenza Romani, Matteo Di Nardo, Gabriella Bottari, Bianca Maria Goffredo, Raffaele Simeoli, Isabella Guzzo, Laura Lancella, Charalampos Antachopoulos, and et al. 2024. "The Use of Cefiderocol as Salvage Therapy in an Infant Receiving ECMO and Continuous Renal Replacement Therapy" Antibiotics 13, no. 1: 37. https://doi.org/10.3390/antibiotics13010037
APA StyleMercadante, S., Tripiciano, C., Romani, L., Di Nardo, M., Bottari, G., Goffredo, B. M., Simeoli, R., Guzzo, I., Lancella, L., Antachopoulos, C., & De Luca, M. (2024). The Use of Cefiderocol as Salvage Therapy in an Infant Receiving ECMO and Continuous Renal Replacement Therapy. Antibiotics, 13(1), 37. https://doi.org/10.3390/antibiotics13010037