
Prevalence of Non-Toxigenic Clostridioides difficile in Diarrhoea Patients and Their Clinical Characteristics

Abstract
:1. Introduction
2. Results
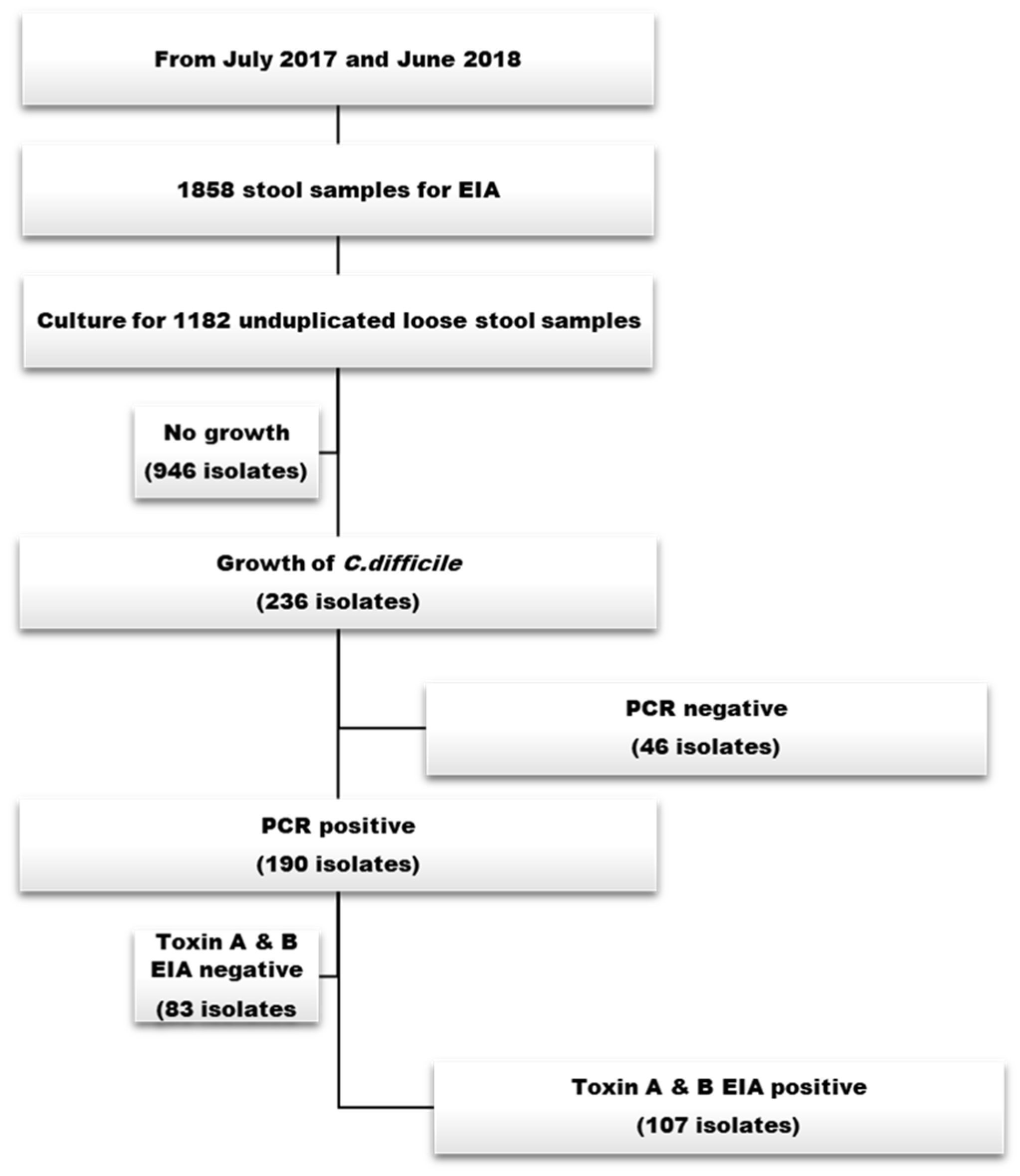
2.1. Characteristics of C. difficile Strains
2.2. Comparison of Clinical Features between Non-Toxigenic and Toxigenic C. difficile
2.3. Predictors of NTCD Strains in Patients with Diarrhoea
2.4. Comparison of Clinical Signs and Subsequent CDI Episodes between Non-Toxigenic and Toxigenic C. difficile
3. Discussion
4. Materials and Methods
- Study Design and Population
- Laboratory Testing
- Clinical Data Collection
- Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ananthakrishnan, A.N. Clostridium difficile infection: Epidemiology, risk factors and 322 management. Nat. Rev. Gastroenterol. Hepatol. 2011, 8, 17–26. [Google Scholar] [CrossRef]
- Magill, S.S.; Edwards, J.R.; Bamberg, W.; Beldavs, Z.G.; Dumyati, G.; Kainer, M.A.; Lynfield, R.; Maloney, M.; McAllister-Hollod, L.; Nadle, J.; et al. Emerging Infections Program Healthcare-Associated Infections and Antimicrobial Use Prevalence Survey Team. Multistate point-prevalence survey of health care-associated infections. N. Engl. J. Med. 2014, 370, 1198–1208. [Google Scholar] [CrossRef]
- Kato, H.; Kato, N.; Watanabe, K.; Iwai, N.; Nakamura, H.; Yamamoto, T.; Suzuki, K.; Kim, S.M.; Chong, Y.; Wasito, E.B. Identification of toxin A-negative, toxin B-positive Clostridium difficile by PCR. J. Clin. Microbiol. 1998, 36, 2178–2182. [Google Scholar] [CrossRef] [PubMed]
- Collins, D.A.; Hawkey, P.M.; Riley, T.V. Epidemiology of Clostridium difficile infection in Asia. Antimicrob. Resist. Infect. Control 2013, 2, 21. [Google Scholar] [CrossRef]
- Seo, M.R.; Kim, J.; Lee, Y.; Lim, D.G.; Pai, H. Prevalence, genetic relatedness and antibiotic resistance of hospital-acquired Clostridium difficile PCR ribotype 018 strains. Int. J. Antimicrob. Agents 2018, 51, 762–767. [Google Scholar] [CrossRef]
- Crobach, M.J.; Planche, T.; Eckert, C.; Barbut, F.; Terveer, E.; Dekkers, O.; Wilcox, M.; Kuijper, E. European Society of Clinical Microbiology and Infectious Diseases: Update of the diagnostic guidance document for Clostridium difficile infection. Clin. Microbiol. Infect. 2016, 22 (Suppl. 4), S63–S81. [Google Scholar] [CrossRef] [PubMed]
- Tschudin-Sutter, S.; Kuijper, E.J.; Durovic, A.; Vehreschild, M.J.G.T.; Barbut, F.; Eckert, C.; Fitzpatrick, F.; Hell, M.; Norén, T.; O’Driscoll, J.; et al. Guidance document for prevention of Clostridium difficile infection in acute healthcare settings. Clin. Microbiol. Infect. 2018, 24, 1051–1054. [Google Scholar] [CrossRef] [PubMed]
- McDonald, L.C.; Gerding, D.N.; Johnson, S.; Bakken, J.S.; Carroll, K.C.; Coffin, S.E.; Dubberke, E.R.; Garey, K.W.; Gould, C.V.; Kelly, C.; et al. Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin. Infect. Dis. 2018, 66, e1–e48. [Google Scholar] [CrossRef]
- Kelly, C.R.; Fischer, M.; Allegretti, J.R.; LaPlante, K.; Stewart, D.B.; Limketkai, B.N.; Stollman, N.H. ACG clinical guidelines: Prevention, diagnosis, and treatment of Clostridioides difficile infections. Am. J. Gastroenterol. 2021, 116, 1124–1127. [Google Scholar] [CrossRef]
- Planche, T.D.; Davies, K.A.; Coen, P.G.; Finney, J.M.; Monahan, I.M.; Morris, K.A.; O’Connor, L.; Oakley, S.J.; Pope, C.F.; Wren, M.W.; et al. Differences in outcome according to Clostridium difficile testing method: A prospective multicentre diagnostic validation study of C. difficile infection. Lancet Infect. Dis. 2013, 13, 936–945. [Google Scholar] [CrossRef]
- Polage, C.R.; Gyorke, C.E.; Kennedy, M.A.; Leslie, J.L.; Chin, D.L.; Wang, S.; Nguyen, H.H.; Huang, B.; Tang, Y.-W.; Lee, L.W.; et al. Overdiagnosis of Clostridium difficile Infection in the Molecular Test Era. JAMA Intern. Med. 2015, 175, 1792–1801. [Google Scholar] [CrossRef]
- Wilcox, M.H. Overcoming barriers to effective recognition and diagnosis of Clostridium difficile infection. Clin. Microbiol. Infect. 2012, 18, 13–20. [Google Scholar] [CrossRef]
- Kelly, S.G.; Yarrington, M.; Zembower, T.R.; Sutton, S.H.; Silkaitis, C.; Postelnick, M.; Mikolajczak, A.; Bolon, M.K. Inappropriate Clostridium difficile testing and consequent overtreatment and inaccurate publicly reported metrics. Infect. Control Hosp. Epidemiol. 2016, 37, 1395–1400. [Google Scholar] [CrossRef]
- Saade, E.; Deshpande, A.; Kundrapu, S.; Sunkesula, V.C.; Guerrero, D.M.; Jury, L.A.; Donskey, C.J. Appropriateness of empiric therapy in patients with suspected Clostridium difficile infection. Curr. Med. Res. Opin. 2013, 29, 985–988. [Google Scholar] [CrossRef]
- Brouwer, M.S.; Allan, E.; Mullany, P.; Roberts, A.P. Draft Genome Sequence of the Nontoxigenic Clostridium difficile Strain CD37. J. Bacteriol. 2012, 194, 2125–2126. [Google Scholar] [CrossRef]
- Cohen, S.H.; Tang, Y.J.; Silva, J., Jr. Analysis of the pathogenicity locus in Clostridium difficile strains. J. Infect. Dis. 2000, 181, 659–663. [Google Scholar] [CrossRef]
- Fluit, A.C.; Wolfhagen, M.J.; Verdonk, G.P.; Jansze, M.; Torensma, R.; Verhoef, J. Nontoxigenic strains of Clostridium difficile lack the genes for both toxin A and toxin B. J. Clin. Microbiol. 1991, 29, 2666–2667. [Google Scholar] [CrossRef]
- Gerding, D.N.; Meyer, T.; Lee, C.; Cohen, S.H.; Murthy, U.K.; Poirier, A.; Van Schooneveld, T.C.; Pardi, D.S.; Ramos, A.; Barron, M.A.; et al. Administration of spores of nontoxigenic Clostridium difficile strain M3 for prevention of recurrent C. difficile infection: A randomized clinical trial. JAMA 2015, 313, 1719–1727. [Google Scholar] [CrossRef]
- Shim, J.K.; Johnson, S.; Samore, M.H.; Bliss, D.Z.; Gerding, D.N. Primary symptomless colonisation by Clostridium difficile and decreased risk of subsequent diarrhoea. Lancet 1998, 351, 633–636. [Google Scholar] [CrossRef]
- Riley, T.V.; Collins, D.A.; Karunakaran, R.; Kahar, M.A.; Adnan, A.; Hassan, S.A.; Zainul, N.H.; Rustam, F.R.M.; Wahab, Z.A.; Ramli, R.; et al. High Prevalence of Toxigenic and Nontoxigenic Clostridium difficile Strains in Malaysia. J. Clin. Microbiol. 2018, 56, e00170-18. [Google Scholar] [CrossRef]
- Collins, D.A.; Gasem, M.H.; Habibie, T.H.; Arinton, I.; Hendriyanto, P.; Hartana, A.; Riley, T. Prevalence and molecular epidemiology of Clostridium difficile infection in Indonesia. New Microbes New Infect. 2017, 18, 34–37. [Google Scholar] [CrossRef]
- Putsathit, P.; Maneerattanaporn, M.; Piewngam, P.; Kiratisin, P.; Riley, T.V. Prevalence and molecular epidemiology of Clostridium difficile infection in Thailand. New Microbes New Infect. 2017, 15, 27–32. [Google Scholar] [CrossRef]
- Collins, D.A.; Sohn, K.M.; Wu, Y.; Ouchi, K.; Ishii, Y.; Elliott, B.; Riley, T.V.; Tateda, K.; for the Clostridioides difficile Asia-Pacific Study Group. Clostridioides difficile infection in the Asia-Pacific region. Emerg. Microbes Infect. 2019, 9, 42–52. [Google Scholar] [CrossRef]
- Sambol, S.P.; Skinner, A.M.; Serna-Perez, F.; Owen, B.; Gerding, D.N.; Johnson, S. Effective Colonization by Nontoxigenic Clostridioides difficile REA Strain M3 (NTCD-M3) Spores following Treatment with Either Fidaxomicin or Vancomycin. Microbiol. Spectr. 2023, 11, e0051723. [Google Scholar] [CrossRef]
- Guerrero, D.M.; Chou, C.; Jury, L.A.; Nerandzic, M.M.; Cadnum, J.C.; Donskey, C.J. Clinical and infection control implications of Clostridium difficile infection with negative enzyme immunoassay for toxin. Clin. Infect. Dis. 2011, 53, 287–290. [Google Scholar] [CrossRef]
- Alasmari, F.; Seiler, S.M.; Hink, T.; Burnham, C.A.; Dubberke, E.R. Prevalence and risk factors for asymptomatic Clostridium difficile carriage. Clin. Infect. Dis. 2014, 59, 216–222. [Google Scholar] [CrossRef]
- Polage, C.R.; Solnick, J.V.; Cohen, S.H. Nosocomial diarrhea: Evaluation and treatment of causes other than Clostridium difficile. Clin. Infect. Dis. 2012, 55, 982–989. [Google Scholar] [CrossRef]
- Wren, B.W.; Heard, S.R.; al-Saleh, A.I.; Tabaqchali, S. Characterisation of Clostridium difficile strains by polymerase chain reaction with toxin A- and B-specific primers. J. Med. Microbiol. 1993, 38, 109–113. [Google Scholar] [CrossRef]
- Mathis, J.N.; Pilkinton, L.; McMillin, D.E. Detection and transcription of toxin DNA in a nontoxigenic strain of Clostridium difficile. Curr. Microbiol. 1999, 38, 324–328. [Google Scholar] [CrossRef]
- Eliakim-Raz, N.; Fishman, G.; Yahav, D.; Goldberg, E.; Stein, G.Y.; Zvi, H.B.; Barsheshet, A.; Bishara, J. Predicting Clostridium difficile infection in diabetic patients and the effect of metformin therapy: A retrospective, case-control study. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 1201–1205. [Google Scholar] [CrossRef]
- Cao, F.; Chen, C.X.; Wang, M.; Liao, H.R.; Wang, M.X.; Hua, S.Z.; Huang, B.; Xiong, Y.; Zhang, J.Y.; Xu, Y.L. Updated meta-analysis of controlled observational studies: Proton-pump inhibitors and risk of Clostridium difficile infection. J. Hosp. Infect. 2018, 98, 4–13. [Google Scholar] [CrossRef]
- Walker, A.S.; Eyre, D.W.; Wyllie, D.H.; Dingle, K.E.; Harding, R.M.; O’Connor, L.; Griffiths, D.; Vaughan, A.; Finney, J.; Wilcox, M.H.; et al. Characterisation of Clostridium difficile hospital ward-based transmission using extensive epidemiological data and molecular typing. PLoS Med. 2012, 9, e1001172. [Google Scholar] [CrossRef]
- Eyre, D.W.; Cule, M.L.; Wilson, D.J.; Griffiths, D.; Vaughan, A.; O’Connor, L.; Ip, C.L.; Golubchik, T.; Batty, E.M.; Finney, J.M.; et al. Diverse sources of C. difficile infection identified on whole-genome sequencing. N. Engl. J. Med. 2013, 369, 1195–1205. [Google Scholar] [CrossRef]
- Park, K.S.; Ki, C.S.; Lee, N.Y. Isolation and Identification of Clostridium difficile Using 375 ChromID C. difficile Medium Combined with Gram Staining and PRO Disc Testing: A 376 Proposal for a Simple Culture Process. Ann. Lab. Med. 2015, 35, 404–409. [Google Scholar] [CrossRef]
- Stubbs, S.; Rupnik, M.; Gibert, M.; Brazier, J.; Duerden, B.; Popoff, M. Production of actin-specific ADP-ribosyltransferase (binary toxin) by strains of Clostridium difficile. FEMS Microbiol. Lett. 2000, 186, 307–312. [Google Scholar] [CrossRef]
- Charlson, M.E.; Carrozzino, D.; Guidi, J.; Patierno, C. Charlson Comorbidity Index: A Critical Review of Clinimetric Properties. Psychother. Psychosom. 2022, 91, 8–35. [Google Scholar] [CrossRef]

{kind=link}
| Toxin Gene Profile (n = 236) | Toxin EIA Results | N (%) |
|---|---|---|
| A+B+CDT- strain | positive | 92 (39.0) |
| negative | 68 (28.8) | |
| A-B+CDT- strain | positive | 11 (4.7) |
| negative | 11 (4.7) | |
| A+B+CDT+ strain | positive | 4 (1.7) |
| negative | 4 (1.7) | |
| A-B-CDT- strain | negative | 46 (19.5) |
| Non-Toxigenic (n = 46) | Toxigenic (n = 107) | p-Value | |
|---|---|---|---|
| Age ≥ 65 y | 23 (50.0) | 68 (63.6) | 0.117 |
| Hospital stays, days, median (IQR) | 7.5 (1.0–20.5) | 7.5 (1.0–25.3) | 0.562 |
| ICU | 9 (19.6) | 12 (11.2) | 0.169 |
| Male sex | 24 (52.2) | 53 (49.5) | 0.764 |
| Category of infection | |||
| Community onset | 9 (19.6) | 5 (4.7) | 0.006 |
| Community-onset healthcare facility associated | 8 (17.4) | 32 (29.9) | 0.106 |
| Hospital onset | 29 (63.0) | 70 (65.4) | 0.778 |
| Underlying disease | |||
| Diabetes | 16 (34.8) | 19 (17.8) | 0.022 |
| Cerebrovascular disease | 14 (30.4) | 44 (41.1) | 0.212 |
| Cardiovascular disease | 6 (13.0) | 21 (19.6) | 0.327 |
| Chronic lung disease | 5 (10.9) | 9 (8.4) | 0.760 |
| Liver cirrhosis | 2 (4.3) | 3 (2.8) | 0.637 |
| Chronic renal disease without dialysis | 8 (17.4) | 12 (11.2) | 0.299 |
| Dialysis | 4 (8.7) | 7 (6.5) | 0.735 |
| Solid tumour | 8 (17.4) | 22 (20.6) | 0.651 |
| Solid organ transplantation | 1 (2.2) | 2 (1.9) | 0.661 |
| Charlson’s score, median (IQR) | 2 (0–4) | 2 (1–5) | 0.175 |
| Previous medical history within 1 month | |||
| Operation | 11 (23.9) | 25 (23.4) | 0.942 |
| Immunosuppression | 5 (10.9) | 11 (10.3) | 0.559 |
| Antibiotic exposure | 36 (78.3) | 96 (90.6) | 0.039 |
| Extended spectrum cephalosporin | 9 (20.5) | 27 (26.5) | 0.439 |
| Quinolone | 8 (18.2) | 26 (25.5) | 0.338 |
| β-lactam/β-lactamases | 8 (18.2) | 20 (19.6) | 0.841 |
| Carbapenem | 11 (25.0) | 29 (28.4) | 0.670 |
| Glycopeptide | 8 (18.2) | 6 (5.9) | 0.031 |
| Gastrointestinal medication use at diagnosis | |||
| PPI | 10 (21.7) | 43 (40.6) | 0.025 |
| H2 receptor antagonist | 16 (34.8) | 35 (33.0) | 0.832 |
| Probiotics | 6 (13.0) | 19 (17.9) | 0.456 |
| Concurrent systemic infection | 27 (58.7) | 51 (47.7) | 0.211 |
| Antibiotics use at the time of diagnosis | 27 (58.7) | 65 (60.7) | 0.812 |
| OR (95% CI) | p-Value | Adjusted OR (95% CI) a | p-Value | |
|---|---|---|---|---|
| Age ≥ 65 y | 0.57 (0.29–1.15) | 0.119 | ||
| * Hospital stays | 1.02 (0.76–1.36) | 0.903 | ||
| ICU | 1.93 (0.75–4.95) | 0.174 | ||
| Male sex | 1.11 (0.56–2.22) | 0.765 | ||
| Category of infection | ||||
| Community onset | 4.96 (1.56–15.77) | 0.007 | 4.13 (1.07–15.97) | 0.040 |
| Community-onset healthcare facility associated | 0.49 (0.21–1.18) | 0.110 | ||
| Hospital onset | 0.90 (0.44–1.85) | 0.778 | ||
| Underlying disease | ||||
| Diabetes | 2.47 (1.13–5.41) | 0.024 | 3.64 (1.46–9.25) | 0.006 |
| Cerebrovascular disease | 0.63 (0.30–1.31) | 0.213 | ||
| Cardiovascular disease | 0.61 (0.23–1.64) | 0.331 | ||
| Chronic lung disease | 1.33 (0.42–4.20) | 0.630 | ||
| Liver cirrhosis | 1.58 (0.25–9.76) | 0.625 | ||
| Chronic renal disease without dialysis | 1.67 (0.63–4.40) | 0.302 | ||
| Dialysis | 1.36 (0.38–4.90) | 0.637 | ||
| Solid tumour | 0.81 (0.33–1.99) | 0.651 | ||
| Solid organ transplantation | 1.17 (0.10–13.20) | 0.901 | ||
| Charlson’s score * | 0.76 (0.42–1.35) | 0.347 | ||
| Previous medical history within 1 month | ||||
| Operation | 1.03 (0.46–2.32) | 0.942 | ||
| Immunosuppression | 1.06 (0.35–3.26) | 0.913 | ||
| Antibiotic exposure | 0.38 (0.14–0.98) | 0.044 | ||
| Extended spectrum cephalosporin | 0.71 (0.30–1.68) | 0.440 | ||
| Quinolone | 0.65 (0.27–1.58) | 0.340 | ||
| β-lactam/β-lactamases | 0.91 (0.37–2.26) | 0.841 | ||
| Carbapenem | 0.84 (0.38–1.88) | 0.670 | ||
| Glycopeptide | 3.56 (1.15–10.96) | 0.027 | 4.75 (1.37–16.42) | 0.014 |
| Gastrointestinal medication use at diagnosis | ||||
| No PPI | 0.41 (0.18–0.91) | 0.028 | 0.28 (0.11–0.72) | 0.009 |
| H2 receptor antagonist | 1.08 (0.52–2.24) | 0.832 | ||
| Probiotics | 0.69 (0.26–1.85) | 0.458 | ||
| Concurrent systemic infection | 1.56 (0.78–3.14) | 0.212 | ||
| Antibiotics use at the time of diagnosis | 0.92 (0.45–1.86) | 0.812 |
| Non-Toxigenic (n = 46) | Toxigenic (n = 107) | p-Value | |
|---|---|---|---|
| Signs at diagnosis | |||
| Body temperature > 38.0 °C | 14 (30.4) | 51 (47.7) | 0.048 |
| Shock | 1 (2.3) | 9 (8.6) | 0.282 |
| Ileus | 0 (0) | 6 (5.8) | 0.179 |
| Laboratory finding | |||
| White blood cell count > 15,000/µL | 8 (18.6) | 35 (35.4) | 0.046 |
| Acute kidney injury | 2 (4.8) | 6 (6.2) | 0.545 |
| Albumin level, g/dL, mean ± SD | 3.5 ± 0.9 | 3.2 ± 0.7 | 0.073 |
| CRP, mmol/L, mean ± SD | 65.5 ± 78.7 | 71.7 ± 63.8 | 0.634 |
| CDI development within 90 days | 1 (2.2) | 12 (11.2) | 0.055 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeon, C.-H.; Kim, S.-H.; Wi, Y.M. Prevalence of Non-Toxigenic Clostridioides difficile in Diarrhoea Patients and Their Clinical Characteristics. Antibiotics 2023, 12, 1360. https://doi.org/10.3390/antibiotics12091360
Jeon C-H, Kim S-H, Wi YM. Prevalence of Non-Toxigenic Clostridioides difficile in Diarrhoea Patients and Their Clinical Characteristics. Antibiotics. 2023; 12(9):1360. https://doi.org/10.3390/antibiotics12091360
Chicago/Turabian StyleJeon, Cheon-Hoo, Si-Ho Kim, and Yu Mi Wi. 2023. "Prevalence of Non-Toxigenic Clostridioides difficile in Diarrhoea Patients and Their Clinical Characteristics" Antibiotics 12, no. 9: 1360. https://doi.org/10.3390/antibiotics12091360
APA StyleJeon, C.-H., Kim, S.-H., & Wi, Y. M. (2023). Prevalence of Non-Toxigenic Clostridioides difficile in Diarrhoea Patients and Their Clinical Characteristics. Antibiotics, 12(9), 1360. https://doi.org/10.3390/antibiotics12091360