
Surveillance of Antimicrobial Prescriptions in Community Pharmacies Located in Tokyo, Japan



Abstract
:1. Introduction
2. Materials and Methods
2.1. Analysis of Prescription Data
2.2. Calculation of Antimicrobial Usage
2.3. Statistical Analysis
3. Results
3.1. Annual Transition of Antimicrobial Prescription in Community Pharmacies
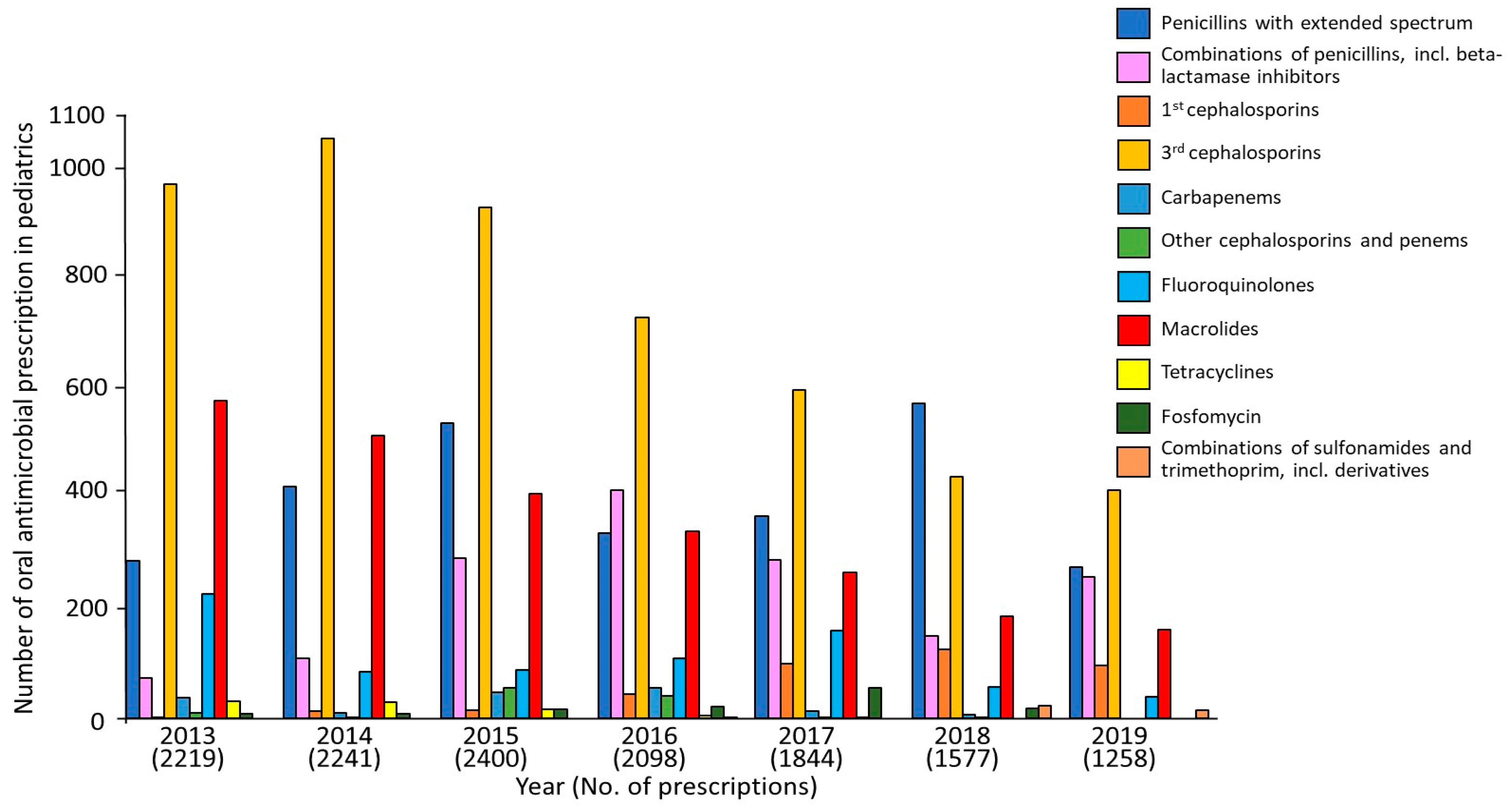
3.2. Impact of the Additional Support for the Appropriate Use of Pediatric Antimicrobial Agents
3.3. The DPY of Antimicrobial Agents
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tsuzuki, S.; Matsunaga, N.; Ohmagari, N. Road to comprehensive estimation of antimicrobial resistance (AMR) disease burden in Japan. Glob. Health Med. 2020, 2, 164–167. [Google Scholar] [CrossRef] [PubMed]
- Nippon AMR One Health Report (NAOR). 2021. Available online: https://www.mhlw.go.jp/content/10900000/000938734.pdf (accessed on 27 July 2022).
- Nakaminami, H.; Takadama, S.; Ito, A.; Hasegawa, M.; Jono, C.; Noguchi, M.; Shoshi, M.; Wajima, T.; Fujii, T.; Maruyama, H.; et al. Characterization of SCCmec type IV methicillin-resistant Staphylococcus aureus clones increased in Japanese hospitals. J. Med. Microbiol. 2018, 67, 769–774. [Google Scholar] [CrossRef] [PubMed]
- Harada, D.; Nakaminami, H.; Miyajima, E.; Sugiyama, T.; Sasai, N.; Kitamura, Y.; Tamura, T.; Kawakubo, T.; Noguchi, N. Change in genotype of methicillin-resistant Staphylococcus aureus (MRSA) affects the antibiogram of hospital-acquired, MRSA. J. Infect. Chemother. 2018, 24, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Yamasaki, D.; Tanabe, M.; Muraki, Y.; Kato, G.; Ohmagari, N.; Yagi, T. The first report of Japanese antimicrobial use measured by national database based on health insurance claims data (2011–2013): Comparison with sales data, and trend analysis stratified by antimicrobial category and age group. Infection 2018, 46, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, H.; Saito, M.; Sato, J.; Goda, K.; Mitsutake, N.; Kitsuregawa, M.; Nagai, R.; Hatakeyama, S. Indications and classes of outpatient antibiotic prescriptions in Japan: A descriptive study using the national database of electronic health insurance claims, 2012–2015. Int. J. Infect.Dis. 2020, 91, 1–8. [Google Scholar] [CrossRef]
- Kimura, Y.; Fukuda, H.; Hayakawa, K.; Ide, S.; Ota, M.; Saito, S.; Ishikane, M.; Kusama, Y.; Matsunaga, N.; Ohmagari, N. Longitudinal trends of and factors associated with inappropriate antibiotic prescribing for non-bacterial acute respiratory tract infection in Japan: A retrospective claims database study, 2012–2017. PLoS ONE 2019, 14, e0223835. [Google Scholar] [CrossRef]
- Ji, L.; Yoshida, S.; Kawakami, K. Trends and patterns in antibiotic prescribing for adult outpatients with acute upper respiratory tract infection in Japan, 2008–2018. J. Infect. Chemother. 2021, 27, 1584–1590. [Google Scholar] [CrossRef]
- Gerber, J.S.; Ross, R.K.; Bryan, M.; Localio, A.R.; Szymczak, J.E.; Wasserman, R.; Barkman, D.; Odeniyi, F.; Conaboy, K.; Bell, L.; et al. Association of Broad- vs Narrow-Spectrum Antibiotics With Treatment Failure, Adverse Events, and Quality of Life in Children With Acute Respiratory Tract Infections. JAMA 2017, 318, 2325–2336. [Google Scholar] [CrossRef]
- Kusama, Y.; Tsuzuki, S.; Muraki, Y.; Koizumi, R.; Ishikane, M.; Ohmagari, N. The effects of Japan’s National Action Plan on Antimicrobial Resistance on antimicrobial use. Int. J. Infect. Dis. 2021, 103, 154–156. [Google Scholar] [CrossRef]
- Gu, Y.; Fujitomo, Y.; Ohmagari, N. Outcomes and Future Prospect of Japan’s National Action Plan on Antimicrobial Resistance (2016–2020). Antibiotics 2021, 10, 1293. [Google Scholar] [CrossRef]
- Muraki, Y.; Maeda, M.; Inose, R.; Yoshimura, K.; Onizuka, N.; Takahashi, M.; Kawakami, E.; Shikamura, Y.; Son, N.; Iwashita, M.; et al. Exploration of Trends in Antimicrobial Use and Their Determinants Based on Dispensing Information Collected from Pharmacies throughout Japan: A First Report. Antibiotics 2022, 11, 682. [Google Scholar] [CrossRef] [PubMed]
- Muraki, Y.; Yagi, T.; Tsuji, Y.; Nishimura, N.; Tanabe, M.; Niwa, T.; Watanabe, T.; Fujimoto, S.; Takayama, K.; Murakami, N.; et al. Japanese antimicrobial consumption surveillance: First report on oral and parenteral antimicrobial consumption in Japan (2009–2013). J. Glob. Antimicrob. Resist. 2016, 7, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Tsutsui, A.; Yahara, K.; Shibayama, K. Trends and patterns of national antimicrobial consumption in Japan from 2004 to 2016. J. Infect. Chemother. 2018, 24, 414–421. [Google Scholar] [CrossRef] [PubMed]
- Statistics Department BoGA, Tokyo Metropolitan Government. Available online: https://www.toukei.metro.tokyo.lg.jp/ (accessed on 18 July 2023).
- Wojt, I.R.; Cairns, R.; Gillooly, I.; Patanwala, A.E.; Tan, E.C.K. Clinical factors associated with increased length of stay and readmission in patients with medication-related hospital admissions: A retrospective study. Res. Soc. Adm. Pharm. 2022, 18, 3184–3190. [Google Scholar] [CrossRef]
- Kusama, Y.; Muraki, Y.; Tanaka, C.; Koizumi, R.; Ishikane, M.; Yamasaki, D.; Tanabe, M.; Ohmagari, N. Characteristics and limitations of national antimicrobial surveillance according to sales and claims data. PLoS ONE 2021, 16, e0251299. [Google Scholar] [CrossRef]
- DUVAT (Drug Use Visualization Assisting Tool). Available online: https://kpu-cpe.sakura.ne.jp/duvathp/index.html (accessed on 25 March 2022).
- Muraki, Y.; Kusama, Y.; Tanabe, M.; Hayakawa, K.; Gu, Y.; Ishikane, M.; Yamasaki, D.; Yagi, T.; Ohmagari, N. Impact of antimicrobial stewardship fee on prescribing for Japanese pediatric patients with upper respiratory infections. BMC Health Serv. Res. 2020, 20, 399. [Google Scholar] [CrossRef]
- Okubo, Y.; Nishi, A.; Michels, K.B.; Nariai, H.; Kim-Farley, R.J.; Arah, O.A.; Uda, K.; Kinoshita, N.; Miyairi, I. The consequence of financial incentives for not prescribing antibiotics: A Japan’s nationwide quasi-experiment. Int. J. Epidemiol. 2022, 51, 1645–1655. [Google Scholar] [CrossRef]
- Hayashi, T.; Kitamura, K.; Hashimoto, S.; Hotomi, M.; Kojima, H.; Kudo, F.; Maruyama, Y.; Sawada, S.; Taiji, H.; Takahashi, G.; et al. Clinical practice guidelines for the diagnosis and management of acute otitis media in children-2018 update. Auris Nasus Larynx 2020, 47, 493–526. [Google Scholar] [CrossRef]
- Shinkai, M.; Rubin, B.K. Macrolides and airway inflammation in children. Paediatr. Respir. Rev. 2005, 6, 227–235. [Google Scholar] [CrossRef]
- Sun, J.; Li, Y. Long-term, low-dose macrolide antibiotic treatment in pediatric chronic airway diseases. Pediatr. Res. 2022, 91, 1036–1042. [Google Scholar] [CrossRef]
- Shimizu, T.; Suzaki, H. Past, present and future of macrolide therapy for chronic rhinosinusitis in Japan. Auris Nasus Larynx 2016, 43, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Koizumi, R.; Kusama, Y.; Muraki, Y.; Ishikane, M.; Yamasaki, D.; Tanabe, M.; Ohmagari, N. Effect of population inflow and outflow between rural and urban areas on regional antimicrobial use surveillance. PLoS ONE 2021, 16, e0248338. [Google Scholar] [CrossRef] [PubMed]
- National Action Plan on Antimicrobial Resistance (AMR) 2023–2027. Available online: https://www.mhlw.go.jp/content/10900000/001096228.pdf (accessed on 18 June 2023).

{kind=link}
| Antimicrobial Class | Number of Prescriptions in Each Year | |||||||
|---|---|---|---|---|---|---|---|---|
| 2013 From April | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | Total | |
| AWaRe (Access) | ||||||||
| Penicillins with extended spectrum | 3269 | 4776 | 5034 | 5056 | 4813 | 5551 | 5121 | 33,620 |
| Combinations of penicillins, incl. beta-lactamase inhibitors | 772 | 1109 | 1361 | 1736 | 1491 | 998 | 1089 | 8556 |
| 1st cephalosporins | 1019 | 1210 | 1181 | 1226 | 1074 | 1397 | 1182 | 8289 |
| Combinations of sulfonamides and trimethoprim, incl. derivatives | 219 | 354 | 441 | 495 | 603 | 733 | 847 | 3692 |
| Lincomycins | 52 | 78 | 50 | 51 | 38 | 49 | 39 | 357 |
| AWaRe (Watch) | ||||||||
| 3rd cephalosporins | 28,742 | 36,632 | 37,459 | 32,354 | 27,686 | 24,238 | 21,969 | 209,080 |
| Macrolides | 18,292 | 25,449 | 23,537 | 22,092 | 17,545 | 15,869 | 15,178 | 137,962 |
| Fluoroquinolones | 12,043 | 15,981 | 16,699 | 16,034 | 15,051 | 14,849 | 13,817 | 104,474 |
| Fosfomycin | 796 | 841 | 748 | 655 | 594 | 514 | 432 | 4580 |
| Carbapenems | 193 | 45 | 245 | 261 | 136 | 43 | 17 | 940 |
| 2nd cephalosporins | 62 | 45 | 68 | 69 | 48 | 4 | 5 | 301 |
| Aminoglycoside | 26 | 48 | 39 | 22 | 9 | 0 | 0 | 144 |
| AWaRe (Access and Watch) | ||||||||
| Tetracyclines | 989 | 1151 | 1460 | 1693 | 1450 | 1256 | 1256 | 9255 |
| AWaRe (Reserve) | ||||||||
| Other cephalosporins and penems | 166 | 109 | 315 | 230 | 190 | 199 | 177 | 1386 |
| AWaRe (Watch and Not Classified) | ||||||||
| Anti-tuberculous drug | 135 | 287 | 245 | 265 | 269 | 263 | 287 | 1751 |
| AWaRe (Not Classified) | ||||||||
| Combinations for the eradication of Helicobacter pylori | 359 | 610 | 446 | 483 | 462 | 384 | 354 | 3098 |
| Other antimicrobials | 0 | 1 | 1 | 2 | 2 | 8 | 10 | 24 |
| Total | 67,134 | 88,726 | 89,329 | 82,724 | 71,461 | 66,355 | 61,780 | 527,509 |
| Antimicrobial Class | DPY per Year | p-Value * | ||||||
|---|---|---|---|---|---|---|---|---|
| 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | ||
| AWaRe (Watch) | ||||||||
| 3rd cephalosporins | 157.2 | 139.5 | 149.7 | 129.2 | 110.8 | 103.7 | 98.8 | 0.02 |
| Fluoroquinolones | 110.6 | 123.5 | 125.5 | 138.9 | 143.3 | 146.7 | 148.9 | 0.04 |
| Macrolides | 178.7 | 176.9 | 179.2 | 175.3 | 157.2 | 135.3 | 125.4 | 0.02 |
| Antimicrobial Class | DPY per Year | p-Value * | ||||||
|---|---|---|---|---|---|---|---|---|
| 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | ||
| AWaRe (Watch) | ||||||||
| 3rd cephalosporins | 275.8 | 263.1 | 282.9 | 226.4 | 185.6 | 183.0 | 161.7 | 0.02 |
| Fluoroquinolones | 187.7 | 116.5 | 134.6 | 123.1 | 107.7 | 101.8 | 105.7 | 0.02 |
| Macrolides | 464.2 | 393.3 | 393.2 | 371.3 | 272.6 | 260.4 | 226.7 | 0.02 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hasegawa, K.; Mori, T.; Asakura, T.; Matsumura, Y.; Nakaminami, H. Surveillance of Antimicrobial Prescriptions in Community Pharmacies Located in Tokyo, Japan. Antibiotics 2023, 12, 1325. https://doi.org/10.3390/antibiotics12081325
Hasegawa K, Mori T, Asakura T, Matsumura Y, Nakaminami H. Surveillance of Antimicrobial Prescriptions in Community Pharmacies Located in Tokyo, Japan. Antibiotics. 2023; 12(8):1325. https://doi.org/10.3390/antibiotics12081325
Chicago/Turabian StyleHasegawa, Kosuke, Tomoko Mori, Toshio Asakura, Yuriko Matsumura, and Hidemasa Nakaminami. 2023. "Surveillance of Antimicrobial Prescriptions in Community Pharmacies Located in Tokyo, Japan" Antibiotics 12, no. 8: 1325. https://doi.org/10.3390/antibiotics12081325
APA StyleHasegawa, K., Mori, T., Asakura, T., Matsumura, Y., & Nakaminami, H. (2023). Surveillance of Antimicrobial Prescriptions in Community Pharmacies Located in Tokyo, Japan. Antibiotics, 12(8), 1325. https://doi.org/10.3390/antibiotics12081325