
Antimicrobial Stewardship for Outpatients with Chronic Bone and Joint Infections in the Orthopaedic Clinic of an Academic Tertiary Hospital, South Africa

 , ,
, ,  ,
,  and
and 
Abstract
1. Introduction
2. Results
2.1. Patient Demographics
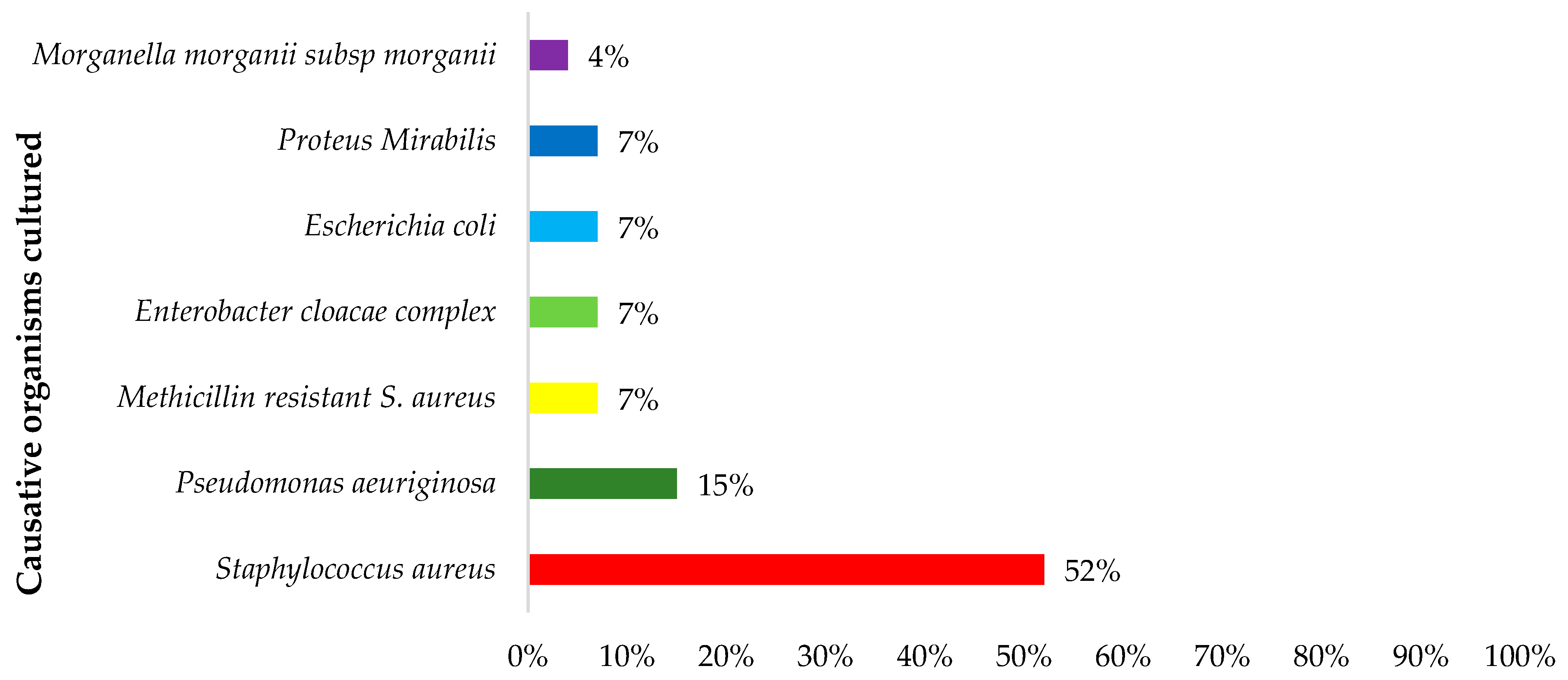
2.2. Microbiology Results
2.3. Antibiotic Treatment
2.4. Adherence
2.5. Knowledge of the Condition and Medication
2.6. Interventions
3. Discussion
4. Materials and Methods
4.1. Study Design, Setting and Population
4.2. Data Collection Tools
4.3. Data Collection Procedure
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Colston, J.; Atkins, B. Bone and Joint Infection. Clin. Med. 2018, 18, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Masters, E.A.; Ricciardi, B.F.; Bentley, K.L.d.M.; Moriarty, T.F.; Schwarz, E.M.; Muthukrishnan, G. Skeletal Infections: Microbial Pathogenesis, Immunity and Clinical Management. Nat. Rev. Microbiol. 2022, 20, 385–400. [Google Scholar] [CrossRef]
- McNally, M.; Dudareva, M.; Govaert, G.; Morgenstern, M.; Metsemakers, W.J. Definition and Diagnosis of Fracture-Related Infection. EFORT Open Rev. 2020, 5, 614–619. [Google Scholar] [CrossRef] [PubMed]
- Sigmund, I.K.; McNally, M.A. Diagnosis of Bone and Joint Infections. Orthop. Trauma 2019, 33, 144–152. [Google Scholar] [CrossRef]
- Kim, B.N.; Kim, E.S.; Oh, M.D. Oral Antibiotic Treatment of Staphylococcal Bone and Joint Infections in Adults. J. Antimicrob. Chemother. 2014, 69, 309–322. [Google Scholar] [CrossRef] [PubMed]
- Malizos, K.N. Global Forum: The Burden of Bone and Joint Infections: A Growing Demand for More Resources. J. Bone Jt. Surg. Am. Vol. 2017, 99, e20.1–e20.7. [Google Scholar] [CrossRef] [PubMed]
- Olivier, K.; Eugene, U.; Lynn, L.; Don Eliseo, L.-P., III. Chronic Osteomyelitis in Sub-Saharan Africa—A Review. Glob. Surg. 2019, 5, 3. [Google Scholar] [CrossRef]
- Diémé, C.; Sarr, L.; Guèye, A.B.; Coulibaly, N.F.; Sané, A.; Ndiaye, A.; Sèye, S. Therapeutic Aspects of Chronic Bone Infections and Management Challenges. Open J. Orthop. 2014, 4, 21–26. [Google Scholar] [CrossRef]
- Ribeiro, M.; Monteiro, F.J.; Ferraz, M.P. Infection of Orthopedic Implants with Emphasis on Bacterial Adhesion Process and Techniques Used in Studying Bacterial-Material Interactions. Biomatter 2012, 2, 176–194. [Google Scholar] [CrossRef]
- Lomas, J. Antimicrobial Treatment in Bone and Joint Infections. Orthop. Trauma 2019, 33, 153–159. [Google Scholar] [CrossRef]
- South African Government. Standard Treatment Guidelines and Essential Medicines List for South Africa: Hospital Level: Adults; The National Department of Health: Pretoria, South Africa, 2020; ISBN 9781920031718. [Google Scholar]
- World Health Organization. The WHO AWaRe (Access, Watch, Reserve) Antibiotic Book. 2022. Available online: https://apps.who.int/iris/bitstream/handle/10665/365237/9789240062382-eng.pdf (accessed on 30 June 2023).
- Zimmerli, W.; Sendi, P. Orthopaedic Biofilm Infections. APMIS 2017, 125, 353–364. [Google Scholar] [CrossRef] [PubMed]
- Rao, N.; Ziran, B.H.; Lipsky, B.A. Treating Osteomyelitis: Antibiotics and Surgery. Plast. Reconstr. Surg. 2011, 127, 177S–187S. [Google Scholar] [CrossRef] [PubMed]
- Tong, S.; Pan, J.; Lu, S.; Tang, J. Patient Compliance with Antimicrobial Drugs: A Chinese Survey. Am. J. Infect. Control 2018, 46, e25–e29. [Google Scholar] [CrossRef] [PubMed]
- Mohiuddin, A.K. Risks and Reasons Associated with Medication Non-Adherence. Inno J. Clin. Pharm. 2019, 1, 50–53. [Google Scholar]
- Manchanayake, M.G.C.A.; Bandara, G.R.W.S.K.; Samaranayake, N.R. Patients’ Ability to Read and Understand Dosing Instructions of Their Own Medicines—A Cross Sectional Study in a Hospital and Community Pharmacy Setting. BMC Health Serv. Res. Serv. Res. 2018, 18, 425. [Google Scholar] [CrossRef] [PubMed]
- Atinga, R.A.; Yarney, L.; Gavu, N.M. Factors Influencing Long-Term Medication Non-Adherence among Diabetes and Hypertensive Patients in Ghana: A Qualitative Investigation. PLoS ONE 2018, 13, e0193995. [Google Scholar] [CrossRef]
- Jankowska-Polańska, B.; Uchmanowicz, I.; Dudek, K.; Mazur, G. Relationship between Patients’ Knowledge and Medication Adherence among Patients with Hypertension. Patient Prefer. Adherence 2016, 10, 2437–2447. [Google Scholar] [CrossRef]
- Saqib, A.; Atif, M.; Ikram, R.; Riaz, F.; Abubakar, M.; Scahill, S. Factors Affecting Patients’ Knowledge about Dispensed Medicines: A Qualitative Study of Healthcare Professionals and Patients in Pakistan. PLoS ONE 2019, 13, e0197482. [Google Scholar] [CrossRef]
- Paige, S.; Stellefson, M.; Singh, B. Patient Perspectives on Factors Associated with Enrollment and Retention in Chronic Disease Self-Management Programs: A Systematic Review. Patient Intell. 2016, 8, 21–37. [Google Scholar] [CrossRef]
- Costa, E.; Giardini, A.; Savin, M.; Menditto, E.; Lehane, E.; Laosa, O.; Pecorelli, S.; Monaco, A.; Marengoni, A. Interventional Tools to Improve Medication Adherence: Review of Literature. Patient Prefer. Adherence 2015, 9, 1303–1314. [Google Scholar] [CrossRef]
- Campbell, S.M.; Meyer, J.C.; Godman, B. Why Compliance to National Prescribing Guidelines Is Important Especially across Sub-Saharan Africa and Suggestions for the Future. J. Biomed. Pharm. Sci. 2021, 4, 6. [Google Scholar]
- Fischer, F.; Lange, K.; Klose, K.; Greiner, W.; Kraemer, A. Barriers and Strategies in Guideline Implementation—A Scoping Review. Healthcare 2016, 4, 36. [Google Scholar] [CrossRef] [PubMed]
- Nathwani, D.; Varghese, D.; Stephens, J.; Ansari, W.; Martin, S.; Charbonneau, C. Value of Hospital Antimicrobial Stewardship Programs [ASPs]: A Systematic Review. Antimicrob. Resist. Infect. Control 2019, 8, 49. [Google Scholar] [CrossRef]
- Siachalinga, L.; Mufwambi, W.; Lee, I.H. Impact of Antimicrobial Stewardship Interventions to Improve Antibiotic Prescribing for Hospital Inpatients in Africa: A Systematic Review and Meta-Analysis. J. Hosp. Infect. 2022, 129, 124–143. [Google Scholar] [CrossRef] [PubMed]
- Saleem, Z.; Godman, B.; Cook, A.; Khan, M.A.; Campbell, S.M.; Seaton, R.A.; Siachalinga, L.; Haseeb, A.; Amir, A.; Kurdi, A.; et al. Ongoing Efforts to Improve Antimicrobial Utilization in Hospitals among African Countries and Implications for the Future. Antibiotics 2022, 11, 1824. [Google Scholar] [CrossRef] [PubMed]
- Schellack, N.; Bronkhorst, E.; Coetzee, R.; Godman, B.; Gous, A.G.S.; Kolman, S.; Labuschagne, Q.; Malan, L.; Messina, A.P.; Naested, C.; et al. SASOCP Position Statement on the Pharmacist’s Role in Antibiotic Stewardship 2018. S. Afr. J. Infect. Dis. 2018, 33, 28–35. [Google Scholar] [CrossRef]
- Otieno, P.A.; Campbell, S.; Maley, S.; Obinju Arunga, T.; Otieno Okumu, M. A Systematic Review of Pharmacist-Led Antimicrobial Stewardship Programs in Sub-Saharan Africa. Int. J. Clin. Pract. 2022, 2022, 3639943. [Google Scholar] [CrossRef]
- Murray, C.J.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Aguilar, G.R.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global Burden of Bacterial Antimicrobial Resistance in 2019: A Systematic Analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Ma, X.; Han, S.; Ma, J.; Chen, X.; Bai, W.; Yan, W.; Wang, K. Epidemiology, Microbiology and Therapeutic Consequences of Chronic Osteomyelitis in Northern China: A Retrospective Analysis of 255 Patients. Sci. Rep. 2018, 8, 14895. [Google Scholar] [CrossRef]
- Vassallo, C.; Borg, A.A.; Farrugia, D.; Mercieca, C. The Epidemiology and Outcomes of Septic Arthritis in the Maltese Islands: A Hospital-Based Retrospective Cohort Study. Mediterr. J. Rheumatol. 2020, 31, 195–205. [Google Scholar] [CrossRef]
- Aghdassi, S.J.S.; Schröder, C.; Gastmeier, P. Gender-Related Risk Factors for Surgical Site Infections. Results from 10 Years of Surveillance in Germany. Antimicrob. Resist. Infect. Control 2019, 8, 95. [Google Scholar] [CrossRef]
- Makwela, A.B.; Grootboom, W.M.; Abraham, V.; Witika, B.; Godman, B.; Skosana, P.P. Antimicrobial Management of Skin and Soft Tissue Infections among Surgical Wards in South Africa: Findings and Implications. Antibiotics 2023, 12, 275. [Google Scholar] [CrossRef] [PubMed]
- Romanò, C.L.; Romanò, D.; Logoluso, N.; Drago, L. Bone and Joint Infections in Adults: A Comprehensive Classification Proposal. Eur. Orthop. Traumatol. 2011, 1, 207–217. [Google Scholar] [CrossRef] [PubMed]
- Chakaya, J.; Petersen, E.; Nantanda, R.; Mungai, B.N.; Migliori, G.B.; Amanullah, F.; Lungu, P.; Ntoumi, F.; Kumarasamy, N.; Maeurer, M.; et al. The WHO Global Tuberculosis 2021 Report–Not so Good News and Turning the Tide Back to End TB. Int. J. Infect. Dis. 2022, 124, S26–S29. [Google Scholar] [CrossRef] [PubMed]
- Kamerman, P. Underdiagnosis of Hypertension and Diabetes Mellitus in South Africa. S. Afr. Med. J. 2022, 112, 53–60. [Google Scholar] [CrossRef]
- Grundlingh, N.; Zewotir, T.T.; Roberts, D.J.; Manda, S. Assessment of Prevalence and Risk Factors of Diabetes and Pre-Diabetes in South Africa. J. Health Popul. Nutr. 2022, 41, 7. [Google Scholar] [CrossRef]
- Dellamonica, P.; Bernard, E.; Etesse, H.; Garraffo, R.; Drugeon, H.B. Evaluation of Pefloxacin, Ofloxacin and Ciprofloxacin in the Treatment of Thirty-Nine Cases of Chronic Osteomyelitis. Eur. J. Clin. Microbiol. Infect. Dis. 1989, 8, 1024–1030. [Google Scholar] [CrossRef]
- Frippiat, F.; Meunier, F.; Derue, G.; Darley, E.S.R.; MacGowan, A.P. Place of Newer Quinolones and Rifampicin in the Treatment of Gram-Positive Bone and Joint Infections. J. Antimicrob. Chemother. 2004, 54, 1158. [Google Scholar] [CrossRef]
- Senneville, E.; Yazdanpanah, Y.; Cazaubiel, M.; Cordonnier, M.; Valette, M.; Beltrand, E.; Khazarjian, A.; Maulin, L.; Alfandari, S.; Caillaux, M.; et al. Rifampicin-Ofloxacin Oral Regimen for the Treatment of Mild to Moderate Diabetic Foot Osteomyelitis. J. Antimicrob. Chemother. 2001, 48, 927–930. [Google Scholar] [CrossRef]
- Mukinda, F.K.; Theron, D.; Van Der Spuy, G.D.; Jacobson, K.R.; Roscher, M.; Streicher, E.M.; Musekiwa, A.; Coetzee, G.J.; Victor, T.C.; Marais, B.J.; et al. Rise in Rifampicin-Monoresistant Tuberculosis in Western Cape, South Africa. Int. J. Tuberc. Lung Dis. 2012, 16, 196–202. [Google Scholar] [CrossRef][Green Version]
- WHO. World Health Organization Global Tuberculosis Report 2022; WHO: Geneva, Switzerland, 2022. [Google Scholar]
- Maduna, L.D.; Kock, M.M.; Van Der Veer, B.M.J.W.; Radebe, O.; Mcintyre, J. Crossm Antimicrobial Resistance of Neisseria Gonorrhoeae Isolates. Antimicrob. Agents Chemother. 2020, 64, e00906-20. [Google Scholar] [CrossRef]
- Sithole, V.; Amoako, D.G.; Abia, A.L.K.; Perrett, K.; Bester, L.A.; Essack, S.Y. Occurrence, Antimicrobial Resistance, and Molecular Characterization of Campylobacter Spp. In Intensive Pig Production in South Africa. Pathogens 2021, 10, 439. [Google Scholar] [CrossRef] [PubMed]
- Founou, R.C.; Founou, L.L.; Allam, M.; Ismail, A.; Essack, S.Y. First Report of a Clinical Multidrug-Resistant Pseudomonas Aeruginosa ST532 Isolate Harbouring a Ciprofloxacin-Modifying Enzyme (CrpP) in South Africa. J. Glob. Antimicrob. Resist. 2020, 22, 145–146. [Google Scholar] [CrossRef] [PubMed]
- Skosana, P.P.; Schellack, N.; Godman, B.; Kurdi, A.; Bennie, M.; Kruger, D.; Meyer, J.C. A National, Multicentre Web-Based Point Prevalence Survey of Antimicrobial Use in Community Healthcare Centres across South Africa and the Implications. Hosp. Pract. 2022, 50, 306–317. [Google Scholar] [CrossRef] [PubMed]
- Skosana, P.P.; Schellack, N.; Godman, B.; Kurdi, A.; Bennie, M.; Kruger, D.; Meyer, J.C. A Point Prevalence Survey of Antimicrobial Utilisation Patterns and Quality Indices amongst Hospitals in South Africa; Findings and Implications. Expert Rev. Anti. Infect. Ther. 2021, 19, 1353–1366. [Google Scholar] [CrossRef]
- Wiedenmayer, K.; Ombaka, E.; Kabudi, B.; Canavan, R.; Rajkumar, S.; Chilunda, F.; Sungi, S.; Stoermer, M. Adherence to Standard Treatment Guidelines among Prescribers in Primary Healthcare Facilities in the Dodoma Region of Tanzania. BMC Health Serv. Res. 2021, 21, 272. [Google Scholar] [CrossRef]
- De Bruycker, M.; Van den Bergh, R.; Dahmane, A.; Khogali, M.; Schiavetti, B.; Nzomukunda, Y.; Alders, P.; Allaouna, M.; Cloquet, C.; Enarson, D.A.; et al. Non-Adherence to Standard Treatment Guidelines in a Rural Paediatric Hospital in Sierra Leone. Public Health Action 2013, 3, 118–124. [Google Scholar] [CrossRef]
- Chigome, A.K.; Matlala, M.; Godman, B.; Meyer, J.C. Availability and Use of Therapeutic Interchange Policies in Managing Antimicrobial Shortages among South African Public Sector Hospitals; Findings and Implications. Antibiotics 2020, 9, 4. [Google Scholar] [CrossRef]
- Schellack, N.; Benjamin, D.; Brink, A.; Duse, A.; Faure, K.; Goff, D.; Mendelson, M.; Meyer, J.; Miot, J.; Perovic, O.; et al. A Situational Analysis of Current Antimicrobial Governance, Regulation, and Utilization in South Africa. Int. J. Infect. Dis. 2017, 64, 100–106. [Google Scholar] [CrossRef]
- National Department of Health. South African Antimicrobial Resistance National Strategy Framework 2018–2024; National Department of Health: Pretoria, South Africa, 2018. [Google Scholar]
- Sharland, M.; Pulcini, C.; Harbarth, S.; Zeng, M.; Gandra, S.; Mathur, S.; Magrini, N. Classifying Antibiotics in the WHO Essential Medicines List for Optimal Use—Be AWaRe. Lancet Infect. Dis. 2018, 18, 18–20. [Google Scholar] [CrossRef]
- Nauta, E.; Mattie, H. Pharmacokinetics of Flucloxacillin and Cloxacillin in Healthy Subjects and Patients on Chronic Intermittent Haemodialysis. Br. J. Clin. Pharmacol. 1975, 2, 111–121. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Zidan, A.; Awisu, A.; El-Hajj, M.S.; Al-Abdulla, S.A.; Figueroa, D.C.R.; Kheir, N. Medication-Related Burden among Patients with Chronic Disease Conditions: Perspectives of Patients Attending Non-Communicable Disease Clinics in a Primary Healthcare Setting in Qatar. Pharmacy 2018, 6, 85. [Google Scholar] [CrossRef] [PubMed]
- Paterick, T.E.; Patel, N.; Tajik, A.J.; Chandrasekaran, K. Improving Health Outcomes through Patient Education and Partnerships with Patients. Baylor Univ. Med. Cent. Proc. 2017, 30, 112–113. [Google Scholar] [CrossRef]
- Choudhry, N.K.; Kronish, I.M.; Vongpatanasin, W.; Ferdinand, K.C.; Pavlik, V.N.; Egan, B.M.; Schoenthaler, A.; Miller, N.H.; Hyman, D.J. Medication Adherence and Blood Pressure Control: A Scientific Statement from the American Heart Association. Hypertension 2022, 79, E1–E14. [Google Scholar] [CrossRef]
- Ntuli, N.P.; Natalie, S.; Gous Andries, G.S. What Difference Can Pharmacist-Driven Management of Adult Patients with Chronic Persistent Asthma Make at a Tertiary Academic Hospital in Gauteng, South Africa? Eur. J. Clin. Pharm. 2017, 19, 112–124. [Google Scholar]
- Lee, P.; Rico, M.; Muench, S.; Yost, C.; Zimmerman, L.H. Impact of Outpatient Antimicrobial Stewardship Guideline Implementation in an Urgent Care Setting. J. Am. Pharm. Assoc. 2022, 62, 1792–1798. [Google Scholar] [CrossRef]
- Sravani, G.R.; Sravani, D.; Rameela, M.; Prasanna, P.K.; Dudekula, S.; Prasad, T.D. Clinical Pharmacist Interventions in Outpatient General Clinical Pharmacist Interventions in Outpatient General Medicine. WORLD J. Pharm. Med. Res. 2018, 4, 286–290. [Google Scholar]
- Viswanathan, M.; Kahwati, L.C.; Golin, C.E.; Blalock, S.J.; Coker-Schwimmer, E.; Posey, R.; Lohr, K.N. Medication Therapy Management Interventions in Outpatient Settings: A Systematic Review and Meta-Analysis. JAMA Intern. Med. 2015, 175, 76–87. [Google Scholar] [CrossRef]
- Kripalani, S.; Risser, J.; Gatti, M.E.; Jacobson, T.A. Development and Evaluation of the Adherence to Refills and Medications Scale (ARMS) among Low-Literacy Patients with Chronic Disease. Value Health 2009, 12, 118–123. [Google Scholar] [CrossRef] [PubMed]
- Andanalusia, M.; Athiyah, U.; Nita, Y. Medication Adherence in Diabetes Mellitus Patients at Tanjung Karang Primary Health Care Center, Mataram. J. Basic Clin. Physiol. Pharmacol. 2019, 30, 6. [Google Scholar] [CrossRef]
- Jackson, I.L.; Umoh, S.S.; Erah, P.O. Medication Adherence and Health Status in HIV Positive Patients in Akwa Ibom State, Nigeria. Trop. J. Pharm. Res. 2020, 19, 2197–2204. [Google Scholar] [CrossRef]


{kind=link}
| Medication | Route of Administration | Dose | Frequency and Duration |
|---|---|---|---|
| Cloxacillin | IV | 2 g | 6 hourly for 4 weeks |
| OR | |||
| Cefazolin | IV | 2 g | 8 hourly for 4 weeks |
| After 2 weeks of IV therapy, a change to oral therapy may be considered in patients with a good clinical response. | |||
| Flucloxacillin | oral | 1 g | 6 hourly to complete the 4 weeks’ treatment |
| Severe penicillin allergy | |||
| Clindamycin | IV | 600 mg | 8 hourly for 4 weeks |
| After 2 weeks of IV therapy, a change to oral therapy may be considered in patients with a good clinical response. | |||
| Clindamycin | oral | 450 mg | 8 hourly to complete the 4 weeks’ treatment |
| Demographics (n = 44) | n (%) | |
|---|---|---|
| Age groups | 18–29 | 10 (23) |
| 30–49 | 21 (48) | |
| 50–69 | 12 (27) | |
| 70 and above | 1 (2) | |
| Gender | Male | 38 (87) |
| Female | 6 (14) | |
| Level of education | Primary school | 3 (7) |
| High school | 33 (75) | |
| University/college | 7 (16) | |
| No formal education | 1 (2) | |
| Comorbidities | HIV positive | 12 (46) |
| Hypertension | 5 (19) | |
| Diabetes mellitus | 3 (12) | |
| IV drug use | 3 (12) | |
| Epilepsy | 1 (4) | |
| Asthma | 1 (4) | |
| Hypercholesterolemia | 1 (4) | |
| Microbiology tests | Conducted | 31 (70) |
| Not conducted | 13 (30) | |
| Diagnosis | Osteomyelitis | 39 (89) |
| Septic arthritis | 5 (11) |
| AWaRe Classification | Antibiotic | n (%) |
|---|---|---|
| Access | Cloxacillin | 14 (20) |
| Flucloxacillin | 11 (15) | |
| Amoxicillin/clavulanic acid | 2 (3) | |
| Watch | Rifampicin | 28 (39) |
| Ciprofloxacin | 16 (23) | |
| Total | 71 | 100% |
| Baseline | Follow up 1 | Follow up 2 | |
|---|---|---|---|
| Number of patients at each visit | 44 | 16 | 5 |
| ‘Don’t know’ | 25 (57%) | 3 (19%) | 0 |
| Bone infection | 11(25%) | 5 (31%) | 0 |
| Chronic osteomyelitis | 1 (2%) | 6 (38%) | 4 (80%) |
| Chronic septic arthritis | 3 (7%) | 2 (13%) | 1 (20%) |
| Other | 4 (9%) | 0 | 0 |
| Baseline | Follow up 1 | Follow up 2 | |
|---|---|---|---|
| Total number of patients at each visit | 44 | 16 | 5 |
| ‘Don’t know’ | 19 (43%) | 2 (13%) | 0 |
| Kills the bacteria | 24 (55%) | 14 (87%) | 5 (100%) |
| Other | 1 (2%) | 0 | 0 |
| Categories of Interventions | Intervention | n (%) |
|---|---|---|
| Knowledge of condition and medication (n = 145) | Name of the condition | 51 (35%) |
| Common signs and symptoms | 7 (5%) | |
| Causes of their condition | 10 (7%) | |
| Purpose of therapy | 46 (32%) | |
| Side effects of their medication | 12 (8%) | |
| Duration of treatment | 17 (12%) | |
| Adherence (n = 65) | Educating patients on adherence | 65 (100) |
| Drug treatment (n = 29) | Drug change | 18 (62%) |
| Correcting dose | 4 (14%) | |
| Educating prescribers | 4 (14%) | |
| Correcting frequency | 3 (10%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masetla, M.A.; Ntuli, P.N.; Abraham, V.; Godman, B.; Witika, B.A.; Mudenda, S.; Skosana, P.P. Antimicrobial Stewardship for Outpatients with Chronic Bone and Joint Infections in the Orthopaedic Clinic of an Academic Tertiary Hospital, South Africa. Antibiotics 2023, 12, 1142. https://doi.org/10.3390/antibiotics12071142
Masetla MA, Ntuli PN, Abraham V, Godman B, Witika BA, Mudenda S, Skosana PP. Antimicrobial Stewardship for Outpatients with Chronic Bone and Joint Infections in the Orthopaedic Clinic of an Academic Tertiary Hospital, South Africa. Antibiotics. 2023; 12(7):1142. https://doi.org/10.3390/antibiotics12071142
Chicago/Turabian StyleMasetla, Mankoana A., Pinky N. Ntuli, Veena Abraham, Brian Godman, Bwalya A. Witika, Steward Mudenda, and Phumzile P. Skosana. 2023. "Antimicrobial Stewardship for Outpatients with Chronic Bone and Joint Infections in the Orthopaedic Clinic of an Academic Tertiary Hospital, South Africa" Antibiotics 12, no. 7: 1142. https://doi.org/10.3390/antibiotics12071142
APA StyleMasetla, M. A., Ntuli, P. N., Abraham, V., Godman, B., Witika, B. A., Mudenda, S., & Skosana, P. P. (2023). Antimicrobial Stewardship for Outpatients with Chronic Bone and Joint Infections in the Orthopaedic Clinic of an Academic Tertiary Hospital, South Africa. Antibiotics, 12(7), 1142. https://doi.org/10.3390/antibiotics12071142