
Predictors of Mortality in Patients with Infections Due to Carbapenem-Resistant Gram-Negative Bacteria

 , , , , ,
, , , , ,  ,
,
Abstract
1. Introduction
2. Methods
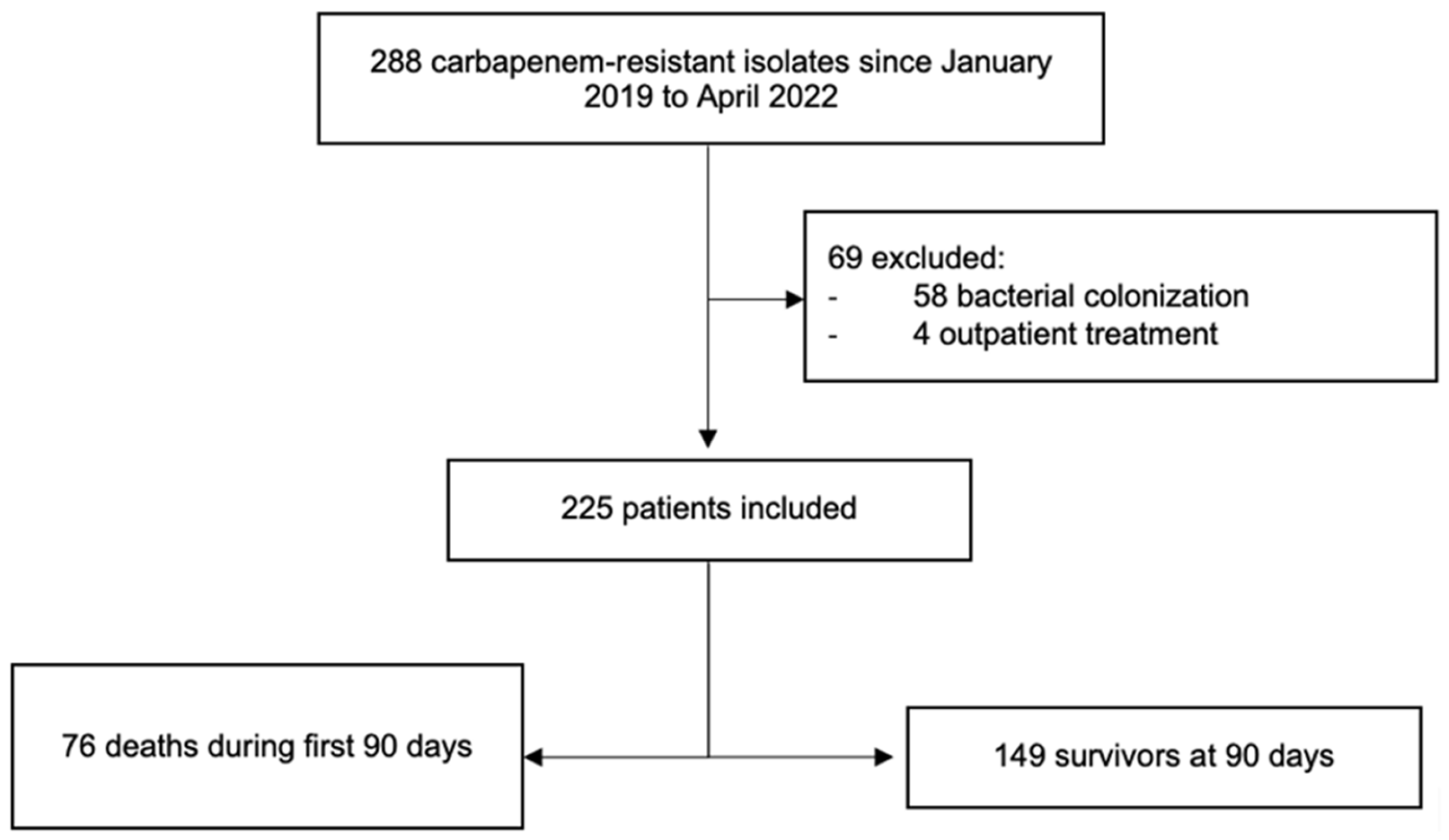
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AMR | antimicrobial resistance |
| CR | carbapenem-resistant |
| CRE | carbapenem-resistant Enterobacterales |
| CR-GNB | Gram-negative bacteria |
| eCIM | EDTA-modified carbapenem inactivation method |
| HR | hazard ratio |
| ICU | intensive care unit |
| IMV | invasive mechanical ventilation |
| IQR | interquartile range |
| MALDI-TOF | matrix-assisted laser desorption/ionisation time-of-flight |
| mCIM | modified carbapenem inactivation method |
| MDR | multidrug-resistant |
| PCR | polymerase chain reaction |
References
- Zhou, N.; Cheng, Z.; Zhang, X.; Lv, C.; Guo, C.; Liu, H.; Dong, K.; Zhang, Y.; Liu, C.; Chang, Y.; et al. Global Antimicrobial Resistance: A System-Wide Comprehensive Investigation Using the Global One Health Index. Infect. Dis. Poverty 2022, 11, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Nordmann, P.; Naas, T.; Poirel, L. Global Spread of Carbapenemase-Producing Enterobacteriaceae. Emerg. Infect. Dis. 2011, 17, 1791–1798. [Google Scholar] [CrossRef] [PubMed]
- Schwaber, M.J.; Carmeli, Y. Carbapenem-Resistant Enterobacteriaceae: A Potential Threat. JAMA 2008, 300, 2911–2913. [Google Scholar] [CrossRef]
- Martinez-Guerra, B.A.; Gonzalez-Lara, M.F.; De-Leon-Cividanes, N.A.; Tamez-Torres, K.M.; Roman-Montes, C.M.; Rajme-Lopez, S.; Villalobos-Zapata, G.I.; Lopez-Garcia, N.I.; Martínez-Gamboa, A.; Sifuentes-Osornio, J.; et al. Antimicrobial Resistance Patterns and Antibiotic Use during Hospital Conversion in the COVID-19 Pandemic. Antibiotics 2021, 10, 182. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.J.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Robles Aguilar, G.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global Burden of Bacterial Antimicrobial Resistance in 2019: A Systematic Analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Ben-David, D.; Kordevani, R.; Keller, N.; Tal, I.; Marzel, A.; Gal-Mor, O.; Maor, Y.; Rahav, G. Outcome of Carbapenem Resistant Klebsiella Pneumoniae Bloodstream Infections. Clin. Microbiol. Infect. 2012, 18, 54–60. [Google Scholar] [CrossRef]
- Fraenkel-Wandel, Y.; Raveh-Brawer, D.; Wiener-Well, Y.; Yinnon, A.M.; Assous, M.V. Mortality due to BlaKPC Klebsiella Pneumoniae Bacteraemia. J. Antimicrob. Chemother. 2016, 71, 1083–1087. [Google Scholar] [CrossRef]
- Bartsch, S.M.; McKinnell, J.A.; Mueller, L.E.; Miller, L.G.; Gohil, S.K.; Huang, S.S.; Lee, B.Y. Potential Economic Burden of Carbapenem-Resistant Enterobacteriaceae (CRE) in the United States. Clin. Microbiol. Infect. 2017, 23, 48.e9–48.e16. [Google Scholar] [CrossRef]
- McEwen, S.A.; Collignon, P.J. Antimicrobial Resistance: A One Health Perspective. Microbiol. Spectr. 2018, 6, 521–547. [Google Scholar] [CrossRef]
- Logan, L.K.; Weinstein, R.A. The Epidemiology of Carbapenem-Resistant Enterobacteriaceae: The Impact and Evolution of a Global Menace. J. Infect. Dis. 2017, 215, S28–S36. [Google Scholar] [CrossRef]
- Horan, T.C.; Andrus, M.; Dudeck, M.A. CDC/NHSN Surveillance Definition of Health Care-Associated Infection and Criteria for Specific Types of Infections in the Acute Care Setting. Am. J. Infect. Control 2008, 36, 309–332. [Google Scholar] [CrossRef]
- CLSI. Performance Standards for Antimicrobial Susceptibility Testing, 30th ed.; CLSI Supplement M100; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2020. [Google Scholar]
- Bogaerts, P.; Rezende de Castro, R.; de Mendonça, R.; Huang, T.-D.; Denis, O.; Glupczynski, Y. Validation of Carbapenemase and Extended-Spectrum β-Lactamase Multiplex Endpoint PCR Assays According to ISO 15189. J. Antimicrob. Chemother. 2013, 68, 1576–1582. [Google Scholar] [CrossRef] [PubMed]
- Riley, R.D.; Ensor, J.; Snell, K.I.E.; Harrell, F.E.; Martin, G.P.; Reitsma, J.B.; Moons, K.G.M.; Collins, G.; van Smeden, M. Calculating the Sample Size Required for Developing a Clinical Prediction Model. BMJ 2020, 368, m441. [Google Scholar] [CrossRef]
- Zhao, S.; Kennedy, S.; Perry, M.R.; Wilson, J.; Chase-Topping, M.; Anderson, E.; Woolhouse, M.E.J.; Lockhart, M. Epidemiology of and Risk Factors for Mortality Due to Carbapenemase-Producing Organisms (CPO) in Healthcare Facilities. J. Hosp. Infect. 2021, 110, 184–193. [Google Scholar] [CrossRef] [PubMed]
- Gualtero, S.; Valderrama, S.; Valencia, M.; Rueda, D.; Munõz-Velandia, O.; Ariza, B.; Cortes, G.; Salgado, D.; Porras, Y.; Ninõ, A. Factors Associated with Mortality in Infections Caused by Carbapenem-Resistant Enterobacteriaceae. J. Infect. Dev. Ctries. 2020, 14, 654–659. [Google Scholar] [CrossRef] [PubMed]
- Bar-Yoseph, H.; Cohen, N.; Korytny, A.; Andrawus, E.R.; Even Dar, R.; Geffen, Y.; Hussein, K.; Paul, M. Risk Factors for Mortality among Carbapenem-Resistant Enterobacteriaceae Carriers with Focus on Immunosuppression. J. Infect. 2019, 78, 101–105. [Google Scholar] [CrossRef]
- Zheng, Y.L.; Wan, Y.F.; Zhou, L.Y.; Ye, M.L.; Liu, S.; Xu, C.Q.; He, Y.Q.; Chen, J.H. Risk Factors and Mortality of Patients with Nosocomial Carbapenem-Resistant Acinetobacter Baumannii Pneumonia. Am. J. Infect. Control 2013, 41, e59–e63. [Google Scholar] [CrossRef]
- Lemos, E.V.; de la Hoz, F.P.; Einarson, T.R.; Mcghan, W.F.; Quevedo, E.; Castañeda, C.; Kawai, K. Carbapenem Resistance and Mortality in Patients with Acinetobacter Baumannii Infection: Systematic Review and Meta-Analysis. Clin. Microbiol. Infect. 2014, 20, 416–423. [Google Scholar] [CrossRef]
- Cienfuegos-Gallet, A.V.; Ocampo De Los Ríos, A.M.; Sierra Viana, P.; Ramirez Brinez, F.; Restrepo Castro, C.; Roncancio Villamil, G.; Del Corral Londoño, H.; Jiménez, J.N. Risk Factors and Survival of Patients Infected with Carbapenem-Resistant Klebsiella Pneumoniae in a KPC Endemic Setting: A Case-Control and Cohort Study. BMC Infect. Dis. 2019, 19, 830. [Google Scholar] [CrossRef]
- Kohler, P.P.; Volling, C.; Green, K.; Uleryk, E.M.; Shah, P.S.; McGeer, A. Carbapenem Resistance, Initial Antibiotic Therapy, and Mortality in Klebsiella Pneumoniae Bacteremia: A Systematic Review and Meta-Analysis. Infect. Control. Hosp. Epidemiol. 2017, 38, 1319–1328. [Google Scholar] [CrossRef]
- Van Duin, D.; Lok, J.J.; Earley, M.; Cober, E.; Richter, S.S.; Perez, F.; Salata, R.A.; Kalayjian, R.C.; Watkins, R.R.; Doi, Y.; et al. Colistin Versus Ceftazidime-Avibactam in the Treatment of Infections Due to Carbapenem-Resistant Enterobacteriaceae. Clin. Infect. Dis. 2018, 66, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Echols, R.; Matsunaga, Y.; Ariyasu, M.; Doi, Y.; Ferrer, R.; Lodise, T.P.; Naas, T.; Niki, Y.; Paterson, D.L.; et al. Efficacy and Safety of Cefiderocol or Best Available Therapy for the Treatment of Serious Infections Caused by Carbapenem-Resistant Gram-Negative Bacteria (CREDIBLE-CR): A Randomised, Open-Label, Multicentre, Pathogen-Focused, Descriptive, Phase 3 Trial. Lancet Infect. Dis. 2021, 21, 226–240. [Google Scholar] [CrossRef] [PubMed]
- Wunderink, R.G.; Giamarellos-Bourboulis, E.J.; Rahav, G.; Mathers, A.J.; Bassetti, M.; Vazquez, J.; Cornely, O.A.; Solomkin, J.; Bhowmick, T.; Bishara, J.; et al. Effect and Safety of Meropenem-Vaborbactam versus Best-Available Therapy in Patients with Carbapenem-Resistant Enterobacteriaceae Infections: The TANGO II Randomized Clinical Trial. Infect. Dis. Ther. 2018, 7, 439–455. [Google Scholar] [CrossRef]
- Paul, M.; Daikos, G.L.; Durante-Mangoni, E.; Yahav, D.; Carmeli, Y.; Benattar, Y.D.; Skiada, A.; Andini, R.; Eliakim-Raz, N.; Nutman, A.; et al. Colistin Alone versus Colistin plus Meropenem for Treatment of Severe Infections Caused by Carbapenem-Resistant Gram-Negative Bacteria: An Open-Label, Randomised Controlled Trial. Lancet Infect. Dis. 2018, 18, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Li, X.; Li, W.; Du, X.; He, J.Q.; Tao, C.; Feng, Y. Influence of Carbapenem Resistance on Mortality of Patients with Pseudomonas Aeruginosa Infection: A Meta-Analysis. Sci. Rep. 2015, 5, 11715. [Google Scholar] [CrossRef]
- Poston, J.T.; Koyner, J.L. Sepsis Associated Acute Kidney Injury. BMJ 2019, 364, k4891. [Google Scholar] [CrossRef]
- Khairoun, M.; Uffen, J.W.; Ocak, G.; Koopsen, R.; Haitjema, S.; Oosterheert, J.J.; Kaasjager, K. The Incidence, Mortality and Renal Outcomes of Acute Kidney Injury in Patients with Suspected Infection at the Emergency Department. PLoS ONE 2021, 16, e0260942. [Google Scholar] [CrossRef]
- Kadri, S.S.; Adjemian, J.; Lai, Y.L.; Spaulding, A.B.; Ricotta, E.; Rebecca Prevots, D.; Palmore, T.N.; Rhee, C.; Klompas, M.; Dekker, J.P.; et al. Difficult-to-Treat Resistance in Gram-Negative Bacteremia at 173 US Hospitals: Retrospective Cohort Analysis of Prevalence, Predictors, and Outcome of Resistance to All First-Line Agents. Clin. Infect. Dis. 2018, 67, 1803–1814. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total n = 225 (100%) | Deaths at 90 Days n = 76 (33.8%) | Survivors at 90 Days n = 149 (66.2%) | p |
|---|---|---|---|---|
| Male, n (%) | 145 (64.4) | 53 (69.7) | 92 (61.7) | 0.236 |
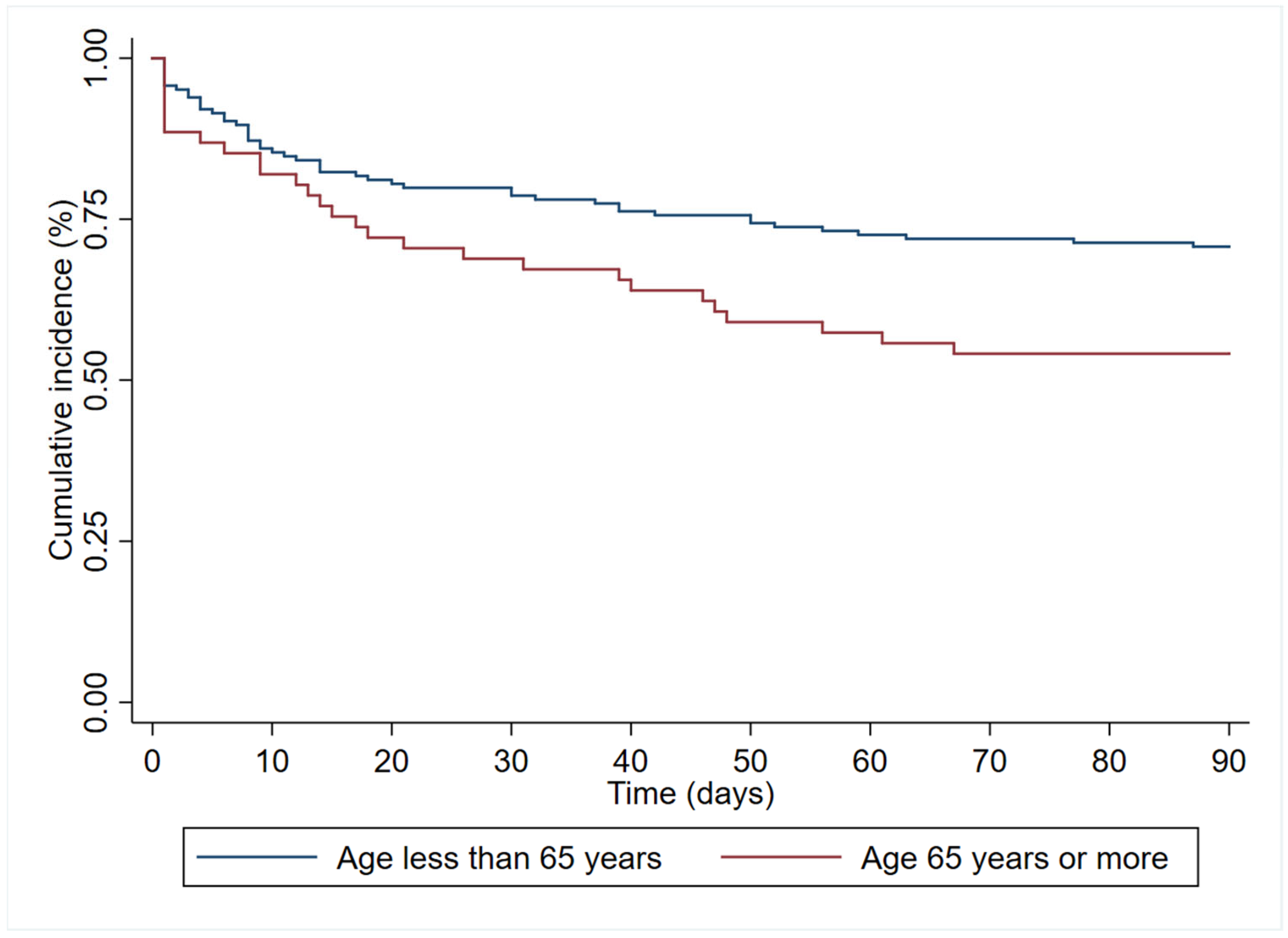
| Age—yr, median (IQR) | 54 (40–66) | 60 (47–70) | 52 (38–63) | 0.0055 |
| Days from admission to diagnosis, median (IQR) | 13 (4–28) | 17 (5–32) | 12 (4–27) | 0.3421 |
| Admission diagnosis, n (%) | 0.468 | |||
| Bacterial infection | 125 (55.6) | 42 (55.3) | 83 (55.7) | |
| COVID-19 | 45 (20.0) | 13 (17.1) | 32 (21.5) | |
| Neoplasm | 24 (10.7) | 12 (15.8) | 12 (8.1) | |
| Elective surgery | 18 (8.0) | 4 (5.3) | 14 (9.4) | |
| Urgent surgery | 8 (3.6) | 3 (4.0) | 5 (3.4) | |
| Other | 5 (2.2) | 2 (2.6) | 3 (2.1) | |
| Patient location at diagnosis, n (%) | ||||
| ICU | 81 (36.0) | 37 (48.7) | 44 (29.5) | 0.005 |
| Hospital ward | 144 (64.0) | 39 (51.3) | 105 (70.5) | |
| Type of CR-GNB infection, n (%) | ||||
| Bloodstream infection | 19 (8.4) | 8 (10.5) | 11 (7.4) | 0.422 |
| Respiratory tract infection | 88 (39.1) | 39 (51.3) | 49 (32.9) | 0.007 |
| Intraabdominal infection | 85 (37.8) | 16 (21.1) | 69 (46.3) | <0.001 |
| Urinary tract infection | 28 (12.5) | 5 (6.6) | 23 (15.5) | 0.055 |
| Bone and soft tissues infections | 18 (8.0) | 10 (13.2) | 8 (5.4) | 0.042 |
| Others | 4 (1.8) | 0 (0) | 4 (2.7) | 0.303 |
| Secondary bacteraemia | 59 (26.2) | 18 (23.7) | 41 (31.5) | 0.536 |
| Comorbidities, n (%) | ||||
| Charlson index >3 | 88 (39.1) | 41 (54.0) | 47 (31.5) | 0.001 |
| COVID-19 | 56 (24.9) | 17 (22.4) | 39 (26.2) | 0.532 |
| Obesity | 50 (22.4) | 15 (19.7) | 35 (23.8) | 0.489 |
| Diabetes | 55 (24.4) | 20 (26.3) | 35 (23.5) | 0.641 |
| Heart disease | 45 (20) | 22 (29.0) | 23 (15.4) | 0.017 |
| Hypertension | 78 (34.7) | 29 (38.2) | 49 (32.9) | 0.432 |
| COPD | 5 (2.2) | 3 (4.0) | 2 (1.3) | 0.339 |
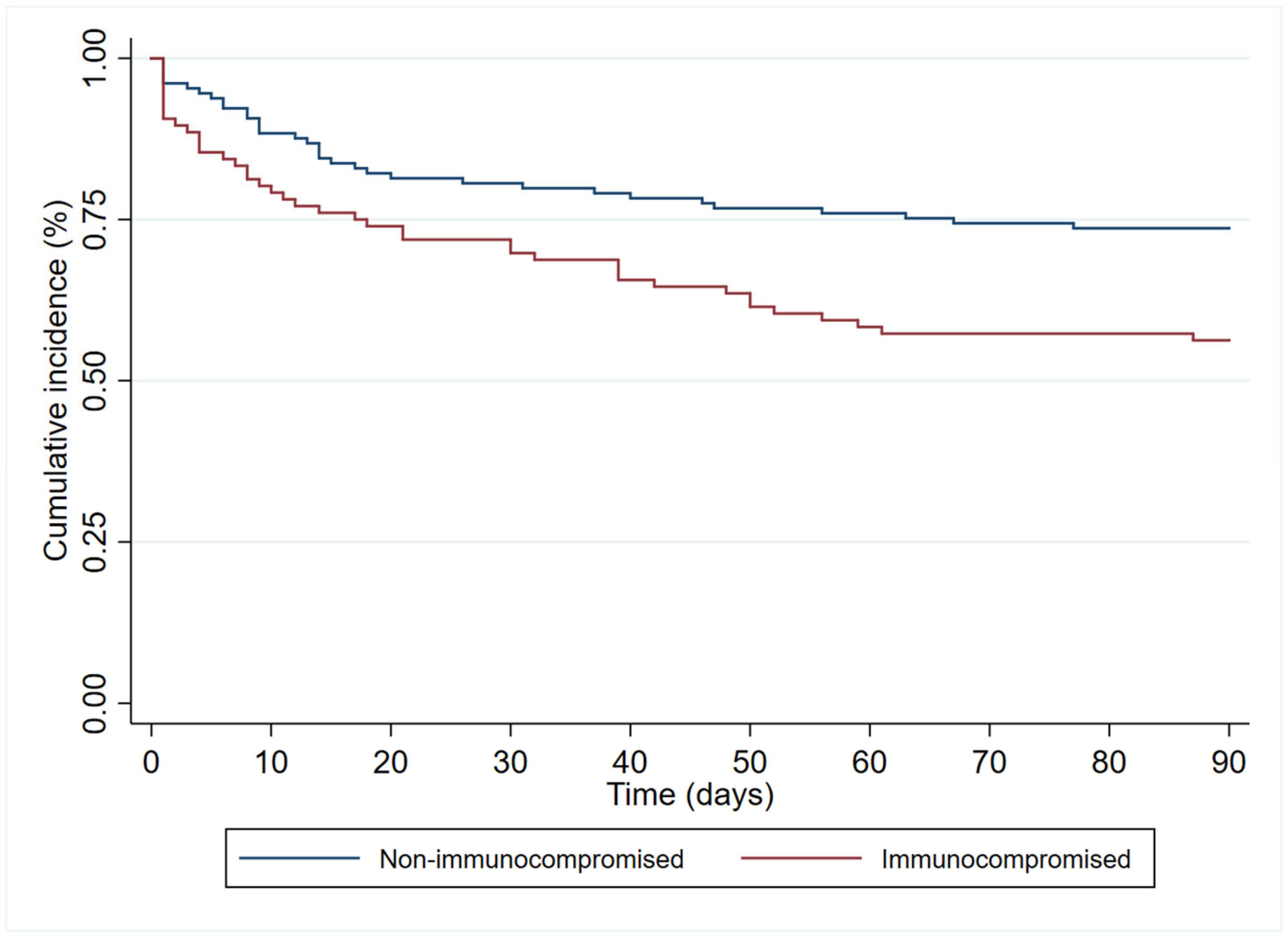
| Immunosuppression | 96 (42.7) | 42 (55.3) | 54 (36.2) | 0.006 |
| Iatrogenic bile duct injury | 34 (15.1) | 7 (9.3) | 27 (18.1) | 0.078 |
| Liver cirrhosis | 13 (5.8) | 3 (4.0) | 10 (6.7) | 0.551 |
| Renal replacement therapy for CKD | 21 (9.3) | 11 (14.5) | 10 (6.7) | 0.058 |
| Cerebrovascular disease | 7 (3.1) | 4 (5.3) | 3 (2.0) | 0.230 |
| Urological disorders | 24 (10.7) | 4 (5.3) | 20 (13.4) | 0.061 |
| Tracheostomy carrier | 31 (13.8) | 9 (11.8) | 22 (14.8) | 0.547 |
| Bacterial coinfection | 120 (53.3) | 41 (54.0) | 79 (53.0) | 0.895 |
| Disease presentation severity, n (%) | ||||
| Mechanical ventilation at diagnosis | 67 (29.8) | 29 (38.2) | 38 (25.5) | 0.050 |
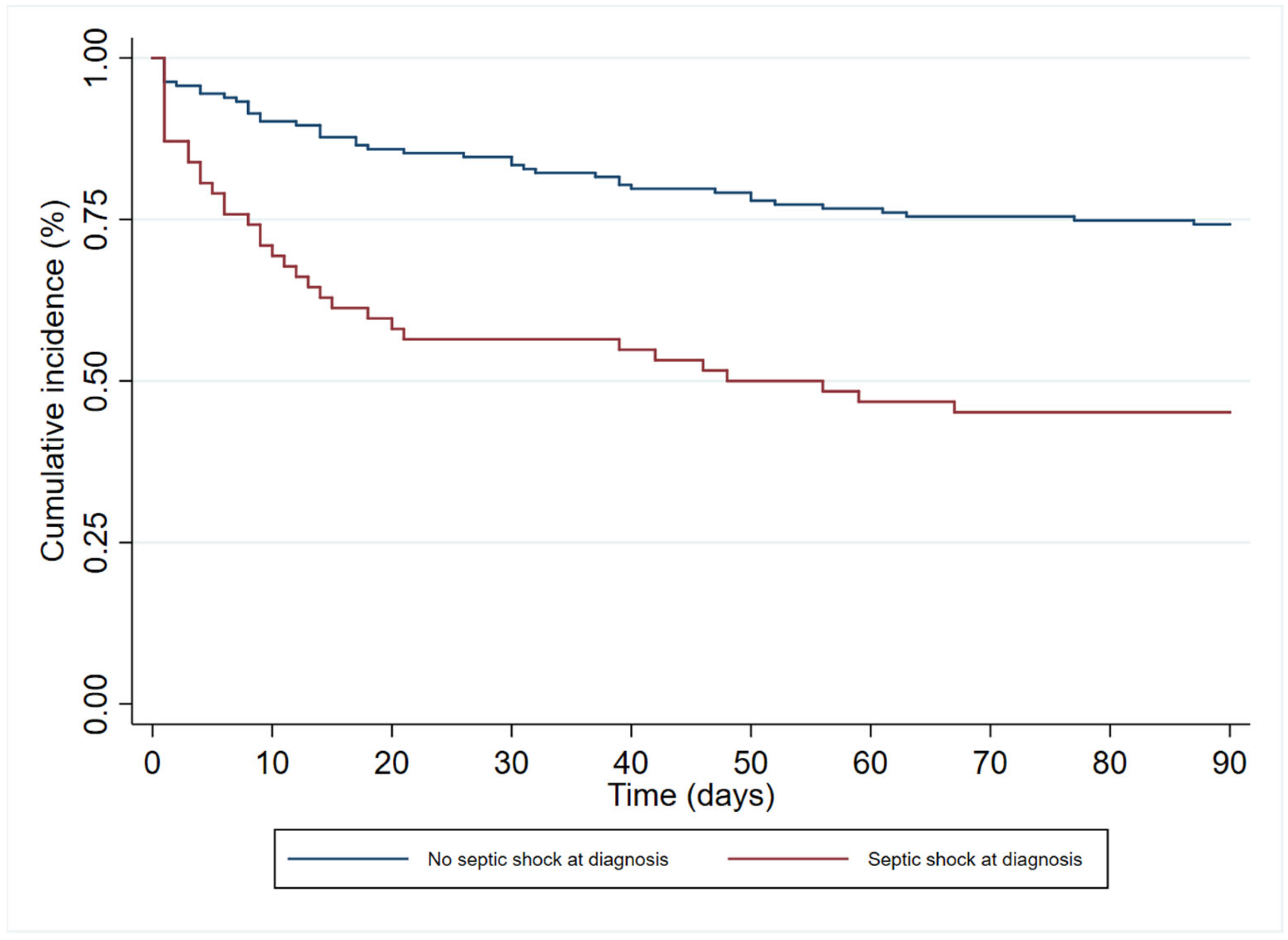
| Septic shock at time of infection | 62 (27.6) | 34 (44.7) | 28 (18.8) | <0.001 |
| Outcome | Total n = 225 (100%) | Deaths at 90 Days n = 76 (33.8%) | Survivors at 90 Days n = 149 (66.2%) | p |
|---|---|---|---|---|
| Mechanical ventilation after diagnosis, n (%) | 19 (8.4) | 13 (17.1) | 6 (4.0) | 0.002 |
| ICU stay after diagnosis, n (%) | 25 (11.1) | 16 (21.1) | 9 (6.0) | 0.001 |
| Infection relapse, n (%) | 41 (18.2) | 8 (10.5) | 33 (22.2) | 0.033 |
| Rehospitalisation for any cause, n (%) n = 224 * | 41 (18.2) | 8 (10.5) | 33 (22.2) | 0.033 |
| C. difficile infection, n (%) | 9 (4.0) | 3 (4.0) | 6 (4.0) | 1.000 |
| Antibiotic-related renal replacement therapy, n (%) | 2 (0.9) | 1 (1.3) | 1 (0.7) | 1.000 |
| Acute kidney injury within the first 10 days of appropriate treatment, n (%) n = 181 | 40 (22.1) | 21 (41.2) | 19 (14.6) | <0.001 |
| Days from diagnosis to death, median (IQR) | - | 13 (4–38) | - | - |
| Variable | aHR (CI 95%), p |
|---|---|
| Male gender | 1.08 (0.64–1.83), 0.779 |
| Age * | 1.19 (1.00–1.83), 0.048 |
| Bloodstream infection | 1.55 (0.60–4.00), 0.364 |
| Respiratory tract infection | 1.25 (0.54–2.94), 0.599 |
| Intraabdominal infection | 0.57 (0.22–1.47), 0.245 |
| Urinary tract infection | 0.33 (0.10–1.10), 0.072 |
| Bone and soft tissue infections | 1.61 (0.59–4.38), 0.347 |
| Obesity | 0.84 (0.46–1.53), 0.564 |
| Diabetes | 0.97 (0.51–1.82), 0.919 |
| Heart disease | 1.51 (0.83–2.73), 0.179 |
| Hypertension | 0.69 (0.39–1.21), 0.193 |
| Immunosuppression | 1.84 (1.06–3.18), 0.030 |
| Cirrhosis | 1.37 (0.40–4.72), 0.618 |
| Renal replacement therapy | 1.65 (0.75–3.62), 0.212 |
| Mechanical ventilation at diagnosis | 1.26 (0.65–2.41), 0.493 |
| Septic shock at time of infection | 2.40 (1.41–4.08), 0.001 |
| Non-fermenting Gram-negative bacilli | 0.84 (0.50–1.42), 0.519 |
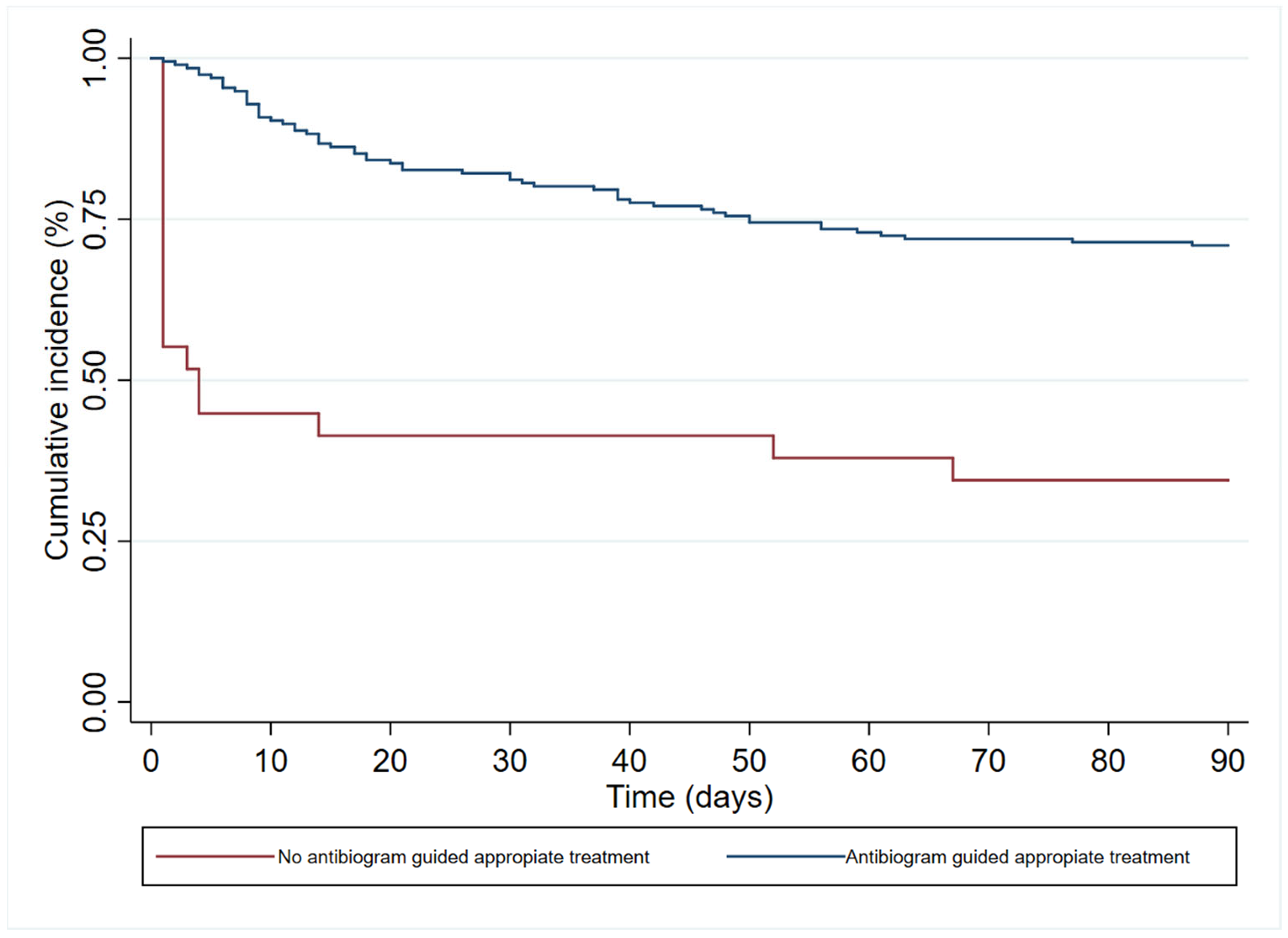
| Antibiogram guided appropriate treatment | 0.25 (0.14–0.46), <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rivera-Villegas, H.O.; Martinez-Guerra, B.A.; Garcia-Couturier, R.; Xancal-Salvador, L.F.; Esteban-Kenel, V.; Jaimes-Aquino, R.A.; Mendoza-Rojas, M.; Cervantes-Sánchez, A.; Méndez-Ramos, S.; Alonso-Montoya, J.E.; et al. Predictors of Mortality in Patients with Infections Due to Carbapenem-Resistant Gram-Negative Bacteria. Antibiotics 2023, 12, 1130. https://doi.org/10.3390/antibiotics12071130
Rivera-Villegas HO, Martinez-Guerra BA, Garcia-Couturier R, Xancal-Salvador LF, Esteban-Kenel V, Jaimes-Aquino RA, Mendoza-Rojas M, Cervantes-Sánchez A, Méndez-Ramos S, Alonso-Montoya JE, et al. Predictors of Mortality in Patients with Infections Due to Carbapenem-Resistant Gram-Negative Bacteria. Antibiotics. 2023; 12(7):1130. https://doi.org/10.3390/antibiotics12071130
Chicago/Turabian StyleRivera-Villegas, Hector Orlando, Bernardo Alfonso Martinez-Guerra, Rosalia Garcia-Couturier, Luis Fernando Xancal-Salvador, Veronica Esteban-Kenel, Ricardo Antonio Jaimes-Aquino, Miguel Mendoza-Rojas, Axel Cervantes-Sánchez, Steven Méndez-Ramos, Jorge Eduardo Alonso-Montoya, and et al. 2023. "Predictors of Mortality in Patients with Infections Due to Carbapenem-Resistant Gram-Negative Bacteria" Antibiotics 12, no. 7: 1130. https://doi.org/10.3390/antibiotics12071130
APA StyleRivera-Villegas, H. O., Martinez-Guerra, B. A., Garcia-Couturier, R., Xancal-Salvador, L. F., Esteban-Kenel, V., Jaimes-Aquino, R. A., Mendoza-Rojas, M., Cervantes-Sánchez, A., Méndez-Ramos, S., Alonso-Montoya, J. E., Munguia-Ramos, D., Tamez-Torres, K. M., Roman-Montes, C. M., Rajme-Lopez, S., Martínez-Gamboa, A., Bobadilla-del-Valle, M., Gonzalez-Lara, M. F., Sifuentes-Osornio, J., & Ponce-de-Leon, A. (2023). Predictors of Mortality in Patients with Infections Due to Carbapenem-Resistant Gram-Negative Bacteria. Antibiotics, 12(7), 1130. https://doi.org/10.3390/antibiotics12071130