Abstract
Bloodstream infections (BSI) are an increasing cause of admissions to hospitals. Non-hospital-acquired BSI are defined by blood cultures that are positive less than 48 hours after admission, but a relevant difference exists between community-acquired and healthcare-associated (HCA) BSI in terms of risk of multidrug resistance (MDR). We planned a retrospective study in three different cohorts in order to develop and to temporally and spatially validate an easy and rapid prognostic model for identifying MDR non-hospital-acquired (non-HA) BSI. The pathogens most involved in BSI are Staphylococcus spp. and Escherichia coli, responsible for about 75% of all MDR isolated. The model includes age, gender, long-term care facility admission, immunocompromise, any recent invasive procedures and central line placement, recent intravenous treatment and antibiotic treatment. It shows an acceptable performance, especially for intermediate probabilities of MDR infection, with a C-index of 70%. The model was proposed in a nomogram that could allow better targeting of antibiotic therapy for non-HA BSI admitted in hospital. However, it should be further validated to determine its applicability in other populations.
1. Introduction
Considering population-based studies conducted in North America and Europe between 2000 and 2015, the bacteriemia or bloodstream infection (BSI) incidence ranges between 113 and 220 per 100,000 persons. However, these studies do not include BSI due to difficult-to-culture microorganism such as Borrelia, Bartonella, Coxiella, Rickettsia and Mycobacteria; the addition of these pathogens may produce a more realistic estimate of BSI incidence and burden, in particular regarding community-onset disease [1].
Key pathogens in studies from high-income countries are S. aureus, Escherichia coli, Klebsiella spp., Pseudomonas aeruginosa, Enterococci, Streptococci and Coagulase-negative staphylococci. The spectrum of organisms is different for community-acquired (Streptococcus pneumoniae, other Streptococci and Escherichia coli) versus healthcare-associated infections (Pseudomonas aeruginosa and Staphylococci) [1]. Furthermore, it is important to keep in mind the worldwide increase in the proportion of antimicrobial resistance among the pathogens causing bloodstream infections [2]. According to surveillance data from 2016 reported by WHO/EARS-Net, the European countries with a carbapenem resistance rate ≥ 25% among Klebsiella pneumoniae blood and central nervous system isolates include Italy, Greece, Serbia, Romania, Belarus and Turkey. The situation outside Europe is highly heterogeneous [1].
BSI results in significant short-term morbidity and mortality worldwide, but is also associated with poor long-term outcome when compared to matched controls [3,4].
1.1. Pathogen-Related Prognostic Risk Factors
Prognosis partly varies according to the pathogen. A recent systematic review established that the most important predictors of mortality in patients with MRSA (Methicillin-Resistant Staphylococcus aureus) bloodstream infection are age, patient condition, timing and appropriateness of antimicrobial treatment, surgical intervention and disease severity as evaluated by the APACHE II score [5]. The incidence of BSI due to Escherichia coli is higher than that of Staphylococcus aureus bacteremia, but the mortality is lower: the in-hospital and 30-day case-fatality is approximately 10–15%; mortality is highly dependent on age, hospital acquisition and co-morbidity, initial presentation with septic shock/severe disease and resistance to fluoroquinolones and third-generation cephalosporin resistance [1]. Although less frequent than E. coli among bacteremia isolates, BSI due to extended-spectrum beta-lactamase (ESBL)-positive K. pneumoniae carries a worse prognosis, including more frequent intensive care unit admission and higher 30-day case-fatality or in-hospital mortality. Many European and North American studies show an association between ESBL-positive Enterobacterales and both excess length of stay and increased mortality rate [1,6,7,8]. Klebsiella pneumoniae is also the most prominent among carbapenem-resistant Gram-negative bacteria causing BSI. The case-fatality of BSI due to carbapenem-resistant Klebsiella is higher than that due to carbapenem-susceptible K. pneumoniae, and the likelihood of initially inappropriate therapy and of suboptimal definitive therapy was significant and a major prognostic factor for poor outcomes before the availability of newer antibiotics. A particularly high risk of fatal outcome after BSI due to carbapenem-resistant Gram-negative bacteria in general has been reported for immunocompromised patients [1].
1.2. Host-Related Prognostic Risk Factors
In patients with a history of malignancy, the most common predictors of mortality among BSI caused by Enterobacteriaceae are septic shock, pneumonia and ICU admission; furthermore, children and hematological malignancy are associated with higher mortality [6,7,8]. The relationship between some malignancies and prolonged bacterial infection has already been shown. For example, the etiology of gastric cancer is related to alcohol, smoking and unhealthy diet, but also to H. pylori infection and the following changes in gastric microbial population as the cancer develops [9,10,11].
A recent Japanese study shows that an estimated glomerular filtration rate (eGFR) lower than 30 mL/min/1.73 m2, procalcitonin of at least 100 ng/mL and primary infectious foci in the gastrointestinal tract or in the respiratory system are independent prognostic factors for short-term survival in patients with BSI [12].
Other studies evaluated prognostic factors in more selected clusters of patients: a machine-learning-based study showed that the most important predictors of death in patients with concomitant candidemia and bacteriaemia are age, serum creatinine level, leukocyte and lymphocyte counts, total bilirubin level, procalcitonin level, endotoxic shock, length of stay in the intensive care unit (ICU), length of stay in the hospital and total parental nutrition [13]; another recent Chinese cohort study indicates that ICU admission, coronary heart disease, biliary infection and the use of tigecycline are independent prognostic factors of 90-day mortality in elderly people (≥65 years old) with both typical (e.g., transplant recipient, hematological malignancy) and atypical (e.g., diabetes mellitus, liver cirrhosis, burns, postoperative) immunosuppression status, and that a decrease in body mass index is a protective factor [14].
1.3. Bloodstream Infection Classification
BSI are usually categorized as community-acquired (CA-BSI) or hospital-acquired (HA-BSI) based on the timing of the positivity of blood cultures (i.e., before or after 48 h since the arrival in hospital, respectively) [15]. HA-BSI pose a higher risk of morbidity and mortality compared with CA-BSI. However, an additional, intermediate, category of BSI, healthcare-associated (HCA-BSI), has been proposed [16]. This category is similar to CA-BSI in terms of the timing of culture results, but it also has at least one risk factor from among the following: recent hospitalization (i.e., at least 2 days in the last 3 months); admission in a long-term care facility in the last 30 days; antibiotic treatment (at least 5 days in the last month); intravenous therapy for chronic ulcers in the last month; hemodialysis in the last 30 days; and immunocompromise [15]. The risk of multidrug resistance (MDR) in the non-HA BSI, specifically in the HCA-BSI, has been increasing in the past few years [17].
Due to this possible higher risk of MDR among some non-HA BSI, and specifically among HCA-BSI compared with CA-BSI, we hypothesized the need of a rapid, empiric antibiotic treatment for these patients, and we aimed to develop a prognostic model for identifying non-HA BSI at high risk of MDR pathogens and to internally and externally validate such a model.
2. Results
2.1. Demographic Characteristics and Risk Factors
The development cohort included 556 patients enrolled between January 2012 and December 2013. The CA-BSI cases numbered 182 (32.7%), and, based on the blood cultures results, 28 were MDR infections (14.7% of all MDR infections included in the development cohort). The HCA-BSI cases numbered 374 (67.3%), and 162 (85.3% of all MDR infections) were MDR. Female patients numbered 82 and 155 among the CA- and HCA-BSI, respectively (p = 0.419), and the median ages were 75 years (range 25–99) and 69 years (range 26–99), respectively (p = 0.1).
The validation cohorts enrolled 609 and 253 patients between January 2014 and December 2015 and between January 2014 and December 2014, respectively, for temporal and spatial external validations (i.e., in the Città della Salute e della Scienza di Torino University Hospital and in the San Giovanni Bosco University affiliated hospital (Local Healthcare Unit of the Città di Torino, Turin, Italy).
In the cohort used for temporal external validation, the female patients numbered 149 and 121 among the CA- and HCA-BSI cases (p = 0.03). The median ages of the enrolled patients were 73.5 years (range 18–97) for CA-BSI and 73 years (range 24–94) for HCA-BSI (p = 0.98).
In the spatial external validation cohort, the female patients numbered 65 and 56 among the CA- and HCA-BSI cases (p = 0.818). The median ages of the enrolled patients for spatial external validation were 72.4 years (range 18–95) for CA-BSI and 73.4 years (range 25–90) for HCA-BSI (p = 0.629).
Table 1 summarizes the baseline characteristics in each cohort, including the risk factors for HCA-BSI.

Table 1.
Baseline characteristics of patients enrolled in each cohort and risk factors for HCA-BSI.
In the model development cohort, immunocompromise was due to prolonged steroid treatment in 116 patients (20.9%), chemotherapy in 80 (14.4%), and/or radiation therapy in 10 (1.8%) in the last month, and/or treatment for previous transplantation (solid or hematological) or for other medical conditions in 58 patients (10.4%), splenectomy in 11 (2%) and known human immunodeficiency virus infection in 4 (0.7%).
In the temporal and spatial validation cohorts, respectively, prolonged steroid treatment was reported in 66 and 30 patients (10.8% and 11.9%), chemotherapy in 36 and 19 (5.9% and 7.5%), and/or radiation therapy in 3 and 2 (0.5% and 0.8%) in the last 30 days, and/or treatment for previous solid or hematological transplantation or for other conditions in 23 and 11 (3.8% and 4.4%), splenectomy in 3 and 2 (0.5% and 0.8%) and known human immunodeficiency virus infection in 6 and 1 (1% and 0.4%).
Table 2 reports the additional risk factors evaluated for MDR.
Table 2.
Additional risk factors for MDR evaluated for the prognostic model.
Gram-negative agents were detected in 51.6% of the patients in the development cohort, and in 53.7% and 59% of the patients in the temporal and spatial validation cohorts, respectively.
Table 3 shows the results of MDR pathogens identified in the blood cultures as single agents. A polymicrobial positivity was found in 30, 34 and 21 patients, in the development, temporal and spatial validation cohorts, respectively.
Table 3.
MDR agents isolated in the blood cultures in the three cohorts used for the prognostic model.
In the development cohort, 51 patients suffered from septic shock (9.2%), compared with 58 (9.5%) in the temporal validation cohort, and 18 (7.1%) in the spatial validation cohort.
Mortality risk was 7.7% among CA-BSI and 15% among HCA-BSI in the development cohort (p = 0.009), 11.3% and 20.1% (p = 0.008), respectively, in the temporal validation cohort, and 10.4% and 16.8% (p = 0.139), respectively, in the spatial validation cohort.
2.2. Prognostic Model Development
Based on the data available in the development cohort and previous data already published and suggested as potential predictors in the international literature, we identified eight predictors of MDR among non-HA BSI: age, gender, long-term care facility admission, immunocompromise, any recent invasive procedures, any central venous catheterization, recent intravenous treatment and antibiotic treatment. This model showed an area under the receiver operating characteristic curve of 71.6% (95% confidence interval 61.8–72.4%).
Table 4 shows the odds ratios (OR) of MDR for each of these variables in the uni- and multivariable models.
Table 4.
Variables included in the logistic models for multidrug-resistant bloodstream infection risk (age, gender, long-term care facility admission, immunocompromise, any recent invasive procedures, central venous catheterization, intravenous treatment and antibiotic treatment).
Figure 1 shows the calibration of the developed prognostic model along with its nomogram. It was built using the already reported covariates. Such a model had a C-index of 70%.
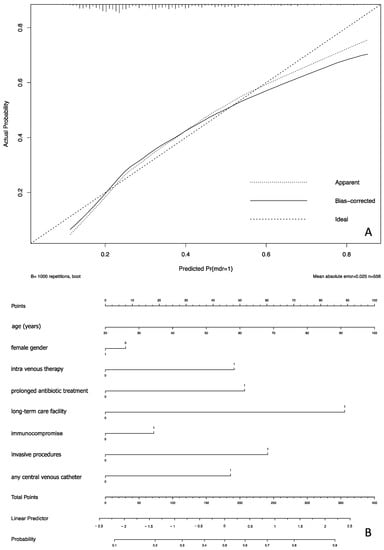
Figure 1.
Calibration (panel A) of the prognostic model and its nomogram (panel B) including the eight selected covariates.
2.3. Model External Validation
2.3.1. Temporal Study
The prognostic model built in the development cohort was validated in two different cohorts. One of them was collected in the same hospital (i.e., Città della Salute e della Scienza University Hospital, Molinette) but over a different time period. This cohort included 609 patients with 177 MDR BSI.
Figure 2 reports the predicted versus observed probability of MDR BSI (calibration) as calculated in this temporally different cohort.

Figure 2.
Model temporal external validation, predicted versus observed probability of MDR BSI plot.
The C-index was 75.9%.
2.3.2. Spatial Study
A third cohort was collected for performing an additional external validation of the proposed prognostic model. This cohort referred to an entire single year of blood cultures including 253 patients and 83 MDR BSI infections. The data were collected in a different University-affiliated hospital in Turin, Italy (San Giovanni Bosco Hospital—Local Healthcare Unit of the Città di Torino).
Figure 3 shows the calibration of the model in such a cohort (spatially external validation). The C-index was 77%.
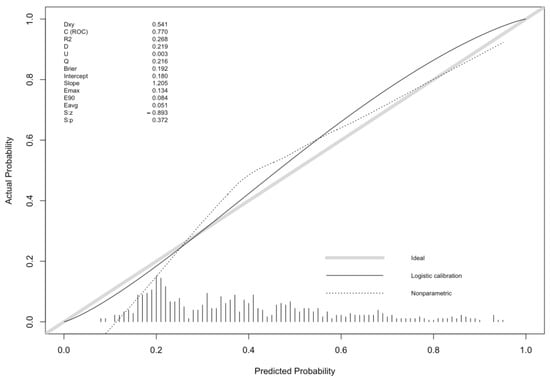
Figure 3.
Model spatial external validation, predicted versus observed probability of MDR BSI plot.
3. Discussion
We have developed and validated an eight-variable prognostic model for the risk of MDR non-HA BSI in three different cohorts of patients admitted to hospital.
Our results suggest this possible prognostic model for high risk for MDR BSI among the non-HA BSI. This model was developed and then separately validated in three different cohorts. The external validation was repeated using two sets of data; one of them was collected in the same University Hospital, the second one in a different University-affiliated hospital in Turin, Italy. The double validation was performed in order to better understand the validity of the prognostic model.
This model was summarized in a nomogram, a fast-performing tool for assessing the risk of MDR at a patient’s admission to hospital.
The need to identify high risk of MDR among non-HA BSI, usually due to frequent contacts with the healthcare systems (for this reason, called HCA-BSI), is linked to the different MDR risk within the large group of patients presenting for BSI and with a blood culture positivity before 48 h after admission. During the past few decades, the number of patients who were treated and followed up outside the hospital has gradually increased, and this has changed the number of patients affected by BSI and the most frequent pathogens [1,2]. For these reasons, the idea of “healthcare-related” infection is a relatively new one, but it is crucial for the correct management of patients affected by BSI [15].
Our data confirmed a significant different mortality risk for CA- and HCA-BSI, except for the spatial validation cohort, where the difference was present but without any significance; likely this is due to its smaller size compared with the other 2 cohorts.
Moreover, as previously reported in the international literature, the pathogens most likely involved in BSI are Staphylococcus spp., and Escherichia coli [19]. In our study, they are responsible of about 75% of all MDR isolated.
The presented model was developed using readily available data. Unlike previous studies and prognostic models [12,13,14,20,21], all parameters reflect patient demographics (i.e., age and gender) and recent medical history data. It shares some parameters with the healthcare-associated infection definition [15] by adding information about the need of central lines and any recent invasive procedures. Some of these procedures might be very frequent, as the placement of a urinary catheter, not only in the Emergency Department for acute illness, but also among out-of-hospital patients for worsening of chronic diseases (e.g., solid or hematologic neoplasm).
In general, the prognostic model shows a good performance across the three validation cohorts. In the development cohort, it had a better performance for the intermediate risk of MDR infection, between 20 and 70%. In the validation cohorts, performance remained acceptable for the same probabilities of MDR infection.
Our study has limitations. Firstly, we collected data in two large hospitals, a University one and a University-affiliated one. The patients referred to similar hospitals might be partially selected by some types of diseases (e.g., hematological and/or advanced oncological diseases) that are not usually treated in all hospitals. This situation might then have an impact on the generalizability of our model as well as the absence of comorbidities in the prognostic models. The inclusion of these comorbidities might have an impact on model performance.
Secondly, we restricted our analysis to the first blood cultures collected for each patient included in the study (for each cohort). It is likely that some patients might be admitted in hospital more than once during each study period, specifically for patients suffering from chronic diseases with high risk of immunocompromise. However, we chose to externally validate our model twice, and its performance remained acceptable. Based on the features of the cohorts we used, the model is not applicable to different settings like out-of-hospital clinics or intensive care units.
The study also presents some strengths. It is based on three large cohorts collected in different period of time. This allowed us to develop the model with enough degrees of freedom and to externally validate it. This second procedure was performed twice. The first external validation was based on data collected in the same hospital where the development cohort was collected, but in a different time frame (2012–2013 vs. 2014–2015). A temporal validation, performed in more-recently treated patients, is a possible way for assessing model performance [22]. However, for better understanding the real performance of the suggested prognostic model, we chose a second external validation, a spatial (or, so called, geographical) one, in a different site. This second process allowed us to confirm our results, but, as already well described in the literature [22], with the drawback of a smaller cohort than the development and temporal validation cohorts. This also allowed us to underline the general consistency of the model.
4. Materials and Methods
The present study was held in the Città della Salute e della Scienza di Torino University Hospital and in the San Giovanni Bosco University affiliated hospital (Local Healthcare Unit of the Città di Torino), Turin, Italy. Data were retrospectively collected based on the laboratory information system results on positive blood cultures.
The hospital Ethics Committee approved the study protocol (n. 0033874). Informed consent was waived because of the retrospective nature of the study and because the analysis used anonymous data. All data were collected from the laboratory information system, and then from medical records, by five investigators (A.C., A.B., P. Pet., E.G. and M.G.).
The primary outcome of the study was to predict the risk of MDR infection among the non-HA BSI (i.e., CA- and HCA-BSI).
For the development cohort, we recruited adult patients (i.e., age ≥ 18 years) with positive blood cultures admitted at the Città della Salute e della Scienza di Torino, Molinette Hospital between January 2012 and December 2013. Samples collected in intensive care, neurosurgery and cardiac surgery units were excluded. Patients with multiple admissions were included in the study only at their first admission, and data relative to subsequent admissions were excluded.
Since the study outcome was MDR in non-HA BSI, we excluded all positive cultures collected more than 48 hours after admission to hospital, as well as those collected in the Emergency Department while patients were waiting for admission due to hospital overcrowding.
Demographic and clinical characteristics of enrolled patients were reported as median and range for continuous data or number and percentage for ordinal data, as appropriate.
The continuous and the categorical variables were tested by using the non-parametric Wilcoxon rank-sum test for unmatched samples, and the Chi-squared or Fisher’s exact test, as appropriate, respectively [23,24].
Multivariable analysis was used to predict MDR among non-HA BSI in the development cohort. Covariates tested were age, gender, long-term care facility admission, immunocompromise, any recent invasive procedures, any central venous catheterization, recent intravenous treatment and antibiotic treatment. The decision to include these variables was taken a priori, based on prior knowledge and the available literature [15,16,22,25,26,27]. The number of predictors was kept to a minimum in order to avoid overfitting and to maximize the use of the predictive model in future applications.
The accuracy of the proposed model was reported as the area under the receiver operating characteristic curve (AUC ROC) [28]. The model was internally validated by bootstrapping (1000 replications) to obtain overfit-corrected estimates of discrimination and calibration [22].
The discrimination ability was measured using the optimism-corrected C-index [29]. Apparent and internally validated (after a 1000 replication bootstrapping procedure) calibration was visually assessed by evaluating the plot of the observed vs. predictive probability of MDR BSI [22].
A second cohort, using the same inclusion criteria, was identified in the same hospital (Città della Salute e della Scienza di Torino, Molinette Hospital), between January 2014 and December 2015. This cohort was used for an external validation of the model in a different time frame (i.e., temporal validation).
A third cohort, again based on the same criteria for enrollment, was collected using the data referring to a different University-affiliated hospital, the San Giovanni Bosco Hospital, Local Healthcare Unit of Città di Torino, Turin, Italy. This hospital shares a similar population of patients and the period of collection was the same as that for the temporal external validation cohort in the Città della Salute e della Scienza di Torino, Molinette Hospital. This last cohort was also used for external validation (i.e., between January 2014 and December 2015, spatial external validation of the model).
Figure 4 briefly summarizes the data collection for these three cohorts.

Figure 4.
Diagram illustrating the collection of data for the three used cohorts (HA BSI, hospital acquired bloodstream infection).
A nomogram, a graphical presentation, was proposed as an easy-to-use tool for applying the prognostic model. It is based on the calculation of the linear predictor. A reference line allows the user to score each variable for the patient and identify a total score corresponding to the linear predictor that has to be transformed in the prediction read at the bottom of the nomogram [30,31].
Antimicrobial susceptibility was determined by a commercially available microdilution assay (Panel NMDR, MicroScan® WalkAway® 96 Plus; Nyon, Beckman Coulter, Switzerland), and ceftazidime/avibactam minimum inhibitory concentrations (MICs) were confirmed by Etest (bioMérieux, Paris, France). Susceptibility data were interpreted according to current European Committee on Antimicrobial Susceptibility Testing (EUCAST) breakpoints [32].
Analyses were performed using STATA 17 (Stata Corp TX, College Station, TX, USA) and R version 3.6.3 (The R Foundation for Statistical Computing, 2020).
5. Conclusions
This study proposed the development and double validation of a prognostic model for MDR non-HA BSI in hospital admitted adult patients. This model, along with the easy-to-perform nomogram, could allow better targeting of empiric antibiotic therapy for BSI before the results of blood cultures become available. However, further prospective studies are needed to confirm the present results and to better define the impact of each covariate.
Author Contributions
G.M., E.P. and E.L. take responsibility for the content of the manuscript, including the data and the analyses; G.M., P.P. (Paolo Peasso) and F.G.D.R. conceived the study; E.P. and E.L. contributed to the study design; E.P. contributed to the statistical analyses; E.P., S.C. and E.L. wrote the first draft of the manuscript and prepared figures and tables; E.P., G.M., F.G.D.R., A.C., A.B., P.P. (Paolo Peasso), P.P. (Paolo Petitti), E.G., M.G., I.C., S.C., R.C., V.G., F.A. and E.L. contributed to data acquisition and interpretation of the results and provided critical input into manuscript drafting and revisions. All authors attest to meeting the four ICMJE.org authorship criteria. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. The of Città della Salute e della Scienza di Torino University Hospital Ethics Committee approved the study protocol (n. 0033874).
Informed Consent Statement
This is a retrospective study so patients’ consent to participate was waived according to hospital Ethics Committee.
Data Availability Statement
The data are available upon reasonable request to the corresponding author.
Acknowledgments
The Authors thank Beatrice Brusasco and Eleonora Caire for their help in collecting some of the clinical data used for the present study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kern, W.V.; Rieg, S. Burden of Bacterial Bloodstream Infection—A Brief Update on Epidemiology and Significance of Multidrug-Resistant Pathogens. Clin. Microbiol. Infect. 2020, 26, 151–157. [Google Scholar] [CrossRef] [PubMed]
- De Angelis, G.; Fiori, B.; Menchinelli, G.; D’Inzeo, T.; Liotti, F.M.; Morandotti, G.A.; Sanguinetti, M.; Posteraro, B.; Spanu, T. Incidence and Antimicrobial Resistance Trends in Bloodstream Infections Caused by ESKAPE and Escherichia Coli at a Large Teaching Hospital in Rome, a 9-Year Analysis (2007–2015). Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 1627–1636. [Google Scholar] [CrossRef] [PubMed]
- Goto, M.; Al-Hasan, M.N. Overall Burden of Bloodstream Infection and Nosocomial Bloodstream Infection in North America and Europe. Clin. Microbiol. Infect. 2013, 19, 501–509. [Google Scholar] [CrossRef] [PubMed]
- McNamara, J.F.; Righi, E.; Wright, H.; Hartel, G.F.; Harris, P.N.A.; Paterson, D.L. Long-Term Morbidity and Mortality Following Bloodstream Infection: A Systematic Literature Review. J. Infect. 2018, 77, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ju, M.; Huang, Y.; Xu, X.; Qian, Y.; Bi, Y.; Liu, S.; Dong, S.; Yuan, J.; Lin, D. Predictors of Mortality in Adult Patients with Methicillin-Resistant Staphylococcus Aureus Bloodstream Infection: A Meta-Analysis and Systematic Review. Ann. Palliat. Med. 2021, 10, 8617–8627. [Google Scholar] [CrossRef] [PubMed]
- Jiang, A.-M.; Liu, N.; Zhao, R.; Zheng, H.-R.; Chen, X.; Fan, C.-X.; Zhang, R.; Zheng, X.-Q.; Fu, X.; Yao, Y.; et al. Clinical Outcomes and Prognostic Factors in Bloodstream Infections Due to Extended-Spectrum β-Lactamase-Producing Enterobacteriaceae among Patients with Malignancy: A Meta-Analysis. Ann. Clin. Microbiol. Antimicrob. 2020, 19, 53. [Google Scholar] [CrossRef]
- Alevizakos, M.; Gaitanidis, A.; Andreatos, N.; Arunachalam, K.; Flokas, M.E.; Mylonakis, E. Bloodstream Infections Due to Extended-Spectrum β-Lactamase-Producing Enterobacteriaceae among Patients with Malignancy: A Systematic Review and Meta-Analysis. Int. J. Antimicrob. Agents 2017, 50, 657–663. [Google Scholar] [CrossRef]
- Russo, A.; Falcone, M.; Gutiérrez-Gutiérrez, B.; Calbo, E.; Almirante, B.; Viale, P.L.; Oliver, A.; Ruiz-Garbajosa, P.; Gasch, O.; Gozalo, M.; et al. Predictors of Outcome in Patients with Severe Sepsis or Septic Shock Due to Extended-Spectrum β-Lactamase-Producing Enterobacteriaceae. Int. J. Antimicrob. Agents 2018, 52, 577–585. [Google Scholar] [CrossRef]
- Wang, L.; Xin, Y.; Zhou, J.; Tian, Z.; Liu, C.; Yu, X.; Meng, X.; Jiang, W.; Zhao, S.; Dong, Q. Gastric Mucosa-Associated Microbial Signatures of Early Gastric Cancer. Front. Microbiol. 2020, 11, 1548. [Google Scholar] [CrossRef]
- Dicksved, J.; Lindberg, M.; Rosenquist, M.; Enroth, H.; Jansson, J.K.; Engstrand, L. Molecular Characterization of the Stomach Microbiota in Patients with Gastric Cancer and in Controls. J. Med. Microbiol. 2009, 58, 509–516. [Google Scholar] [CrossRef]
- Zhou, S.; Li, C.; Liu, L.; Yuan, Q.; Miao, J.; Wang, H.; Ding, C.; Guan, W. Gastric Microbiota: An Emerging Player in Gastric Cancer. Front. Microbiol. 2023, 14, 1130001. [Google Scholar] [CrossRef] [PubMed]
- Osamura, Y.; Nishiyama, H.; Hattori, T.; Gunji, M.; Yuasa, N. Clinico-Bacterial and Prognostic Factors in Patients with Suspected Blood Stream Infection and Elevated Serum Procalcitonin Levels. Nagoya J. Med. Sci. 2022, 84, 230. [Google Scholar] [PubMed]
- Gao, Y.; Tang, M.; Li, Y.; Niu, X.; Li, J.; Fu, C.; Wang, Z.; Liu, J.; Song, B.; Chen, H.; et al. Machine-Learning Based Prediction and Analysis of Prognostic Risk Factors in Patients with Candidemia and Bacteraemia: A 5-Year Analysis. PeerJ 2022, 10, e13594. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Gao, Y.; Qiu, Y.; Zhu, H.; Zhang, S.; Summah, H.D.; Shi, G.; Cheng, T.; Yang, Z.; Feng, Y. The Prognostic Factors of Bloodstream Infection in Immunosuppressed Elderly Patients: A Retrospective, Single-Center, Five-Year Cohort Study. CIA 2022, 17, 1647–1656. [Google Scholar] [CrossRef]
- Friedman, N.D. Health Care–Associated Bloodstream Infections in Adults: A Reason to Change the Accepted Definition of Community-Acquired Infections. Ann. Intern. Med. 2002, 137, 791–797. [Google Scholar] [CrossRef]
- Lujan, M.; Gallego, M.; Rello, J. Healthcare-Associated Infections. A Useful Concept? Curr. Opin. Crit. Care 2009, 15, 419–424. [Google Scholar] [CrossRef]
- Murray, C.J.L.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Robles Aguilar, G.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global Burden of Bacterial Antimicrobial Resistance in 2019: A Systematic Analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Klastersky, J.; De Naurois, J.; Rolston, K.; Rapoport, B.; Maschmeyer, G.; Aapro, M.; Herrstedt, J. Management of Febrile Neutropaenia: ESMO Clinical Practice Guidelines. Ann. Oncol. 2016, 27, v111–v118. [Google Scholar] [CrossRef]
- Pien, B.C.; Sundaram, P.; Raoof, N.; Costa, S.F.; Mirrett, S.; Woods, C.W.; Reller, L.B.; Weinstein, M.P. The Clinical and Prognostic Importance of Positive Blood Cultures in Adults. Am. J. Med. 2010, 123, 819–828. [Google Scholar] [CrossRef]
- Wang, W.; Chen, W.; Liu, Y.; Li, L.; Li, S.; Tan, J.; Sun, X. Blood Glucose Levels and Mortality in Patients With Sepsis: Dose–Response Analysis of Observational Studies. J. Intensive Care Med. 2021, 36, 182–190. [Google Scholar] [CrossRef]
- Wang, J.; Zhu, C.-K.; Yu, J.-Q.; Tan, R.; Yang, P.-L. Hypoglycemia and Mortality in Sepsis Patients: A Systematic Review and Meta-Analysis. Heart Lung 2021, 50, 933–940. [Google Scholar] [CrossRef]
- Steyerberg, E.W. Clinical Prediction Models: A Practical Approach to Development, Validation, and Updating; Statistics for biology and health; Springer: New York, NY, USA, 2009; ISBN 978-0-387-77243-1. [Google Scholar]
- Mann, H.B.; Whitney, D.R. On a Test of Whether One of Two Random Variables Is Stochastically Larger than the Other. Ann. Math. Stat. 1947, 18, 50–60. [Google Scholar] [CrossRef]
- McNemar, Q. Note on the Sampling Error of the Difference between Correlated Proportions or Percentages. Psychometrika 1947, 12, 153–157. [Google Scholar] [CrossRef]
- Kollef, M.H.; Morrow, L.E.; Baughman, R.P.; Craven, D.E.; McGowan, J.E., Jr.; Micek, S.T.; Niederman, M.S.; Ost, D.; Paterson, D.L.; Segreti, J. Health Care–Associated Pneumonia (HCAP): A Critical Appraisal to Improve Identification, Management, and Outcomes—Proceedings of the HCAP Summit. Clin. Infect. Dis. 2008, 46, S296–S334. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Zheng, Z.; Shi, Q.; Wu, H.; Li, Y.; Zheng, C. Multidrug-Resistant Acinetobacter Baumannii May Cause Patients to Develop Polymicrobial Bloodstream Infection. Can. J. Infect. Dis. Med. Microbiol. 2022, 2022, 8368578. [Google Scholar] [CrossRef]
- Lin, J.-N.; Lai, C.-H.; Chen, Y.-H.; Chang, L.-L.; Lu, P.-L.; Tsai, S.-S.; Lin, H.-L.; Lin, H.-H. Characteristics and Outcomes of Polymicrobial Bloodstream Infections in the Emergency Department: A Matched Case-Control Study: Polymicrobial bloodstream infections in the ED. Acad. Emerg. Med. 2010, 17, 1072–1079. [Google Scholar] [CrossRef]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the Areas under Two or More Correlated Receiver Operating Characteristic Curves: A Nonparametric Approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Harrell, F. Regression Modeling Strategies—With Applications to Linear Models, Logistic Regression, and Survival Analysis; Springer: New York, NY, USA, 2001; ISBN 978-1-4757-3462-1. [Google Scholar]
- Lubsen, J.; Pool, J.; van der Does, E. A Practical Device for the Application of a Diagnostic or Prognostic Function. Methods Inf. Med. 1978, 17, 127–129. [Google Scholar] [CrossRef] [PubMed]
- Schemper, M. Predictive Accuracy and Explained Variation. Stat. Med. 2003, 22, 2299–2308. [Google Scholar] [CrossRef]
- European Committee on Antimicrobial Susceptibility Testing (EUCAST) Breakpoints (Version 11.0). 2021. Available online: https://www.eucast.org/eucast_news/news_singleview?tx_ttnews%5Btt_news%5D=404&cHash=74a1f440876cb3eefb60e6ad39c622e7 (accessed on 31 December 2022).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).