

Systemic Antimicrobial Therapy for Diabetic Foot Infections: An Overview of Systematic Reviews
Abstract
1. Introduction
2. Methods
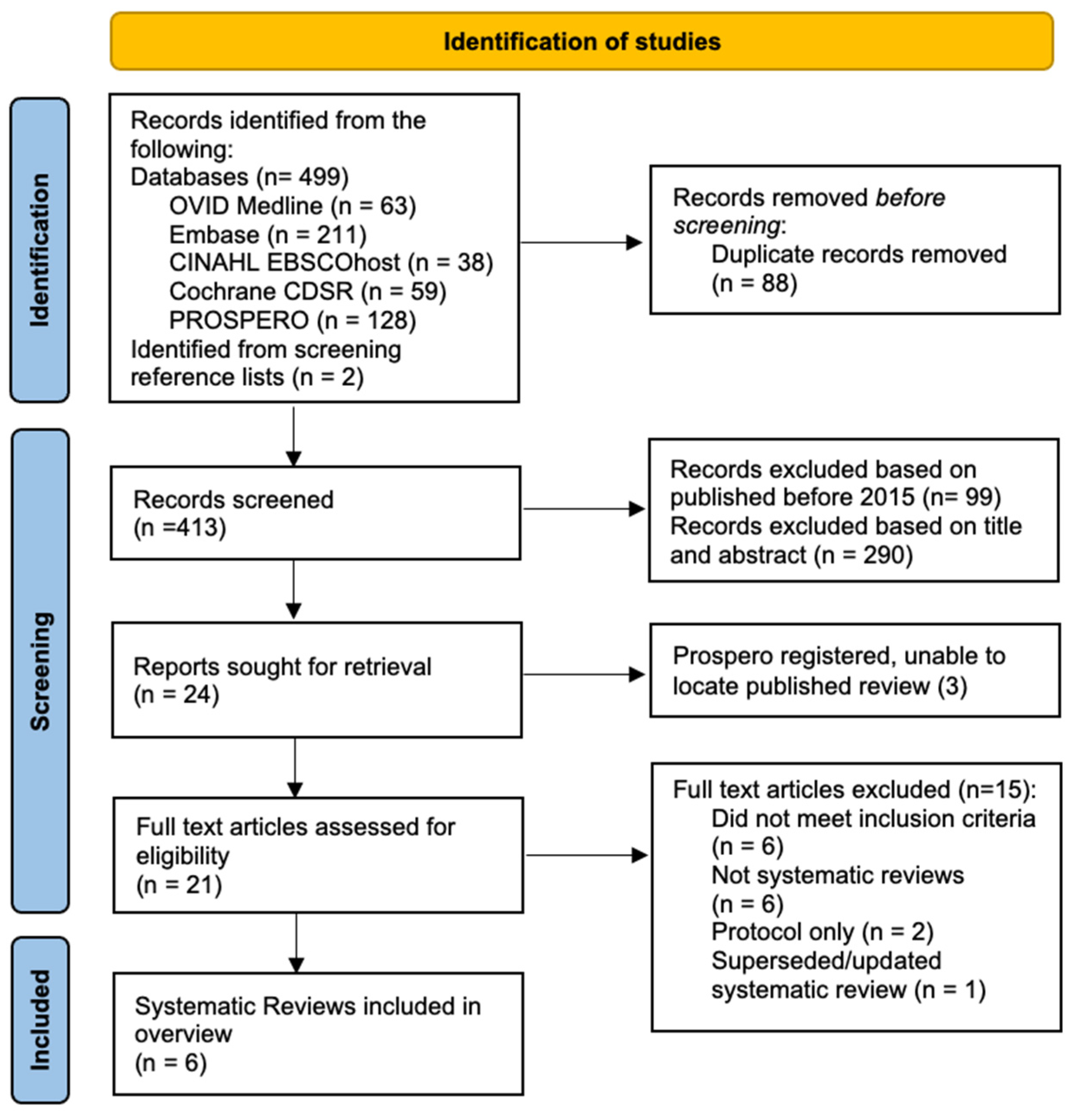
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Collection and Extraction
2.4. Quality Assessment
3. Results
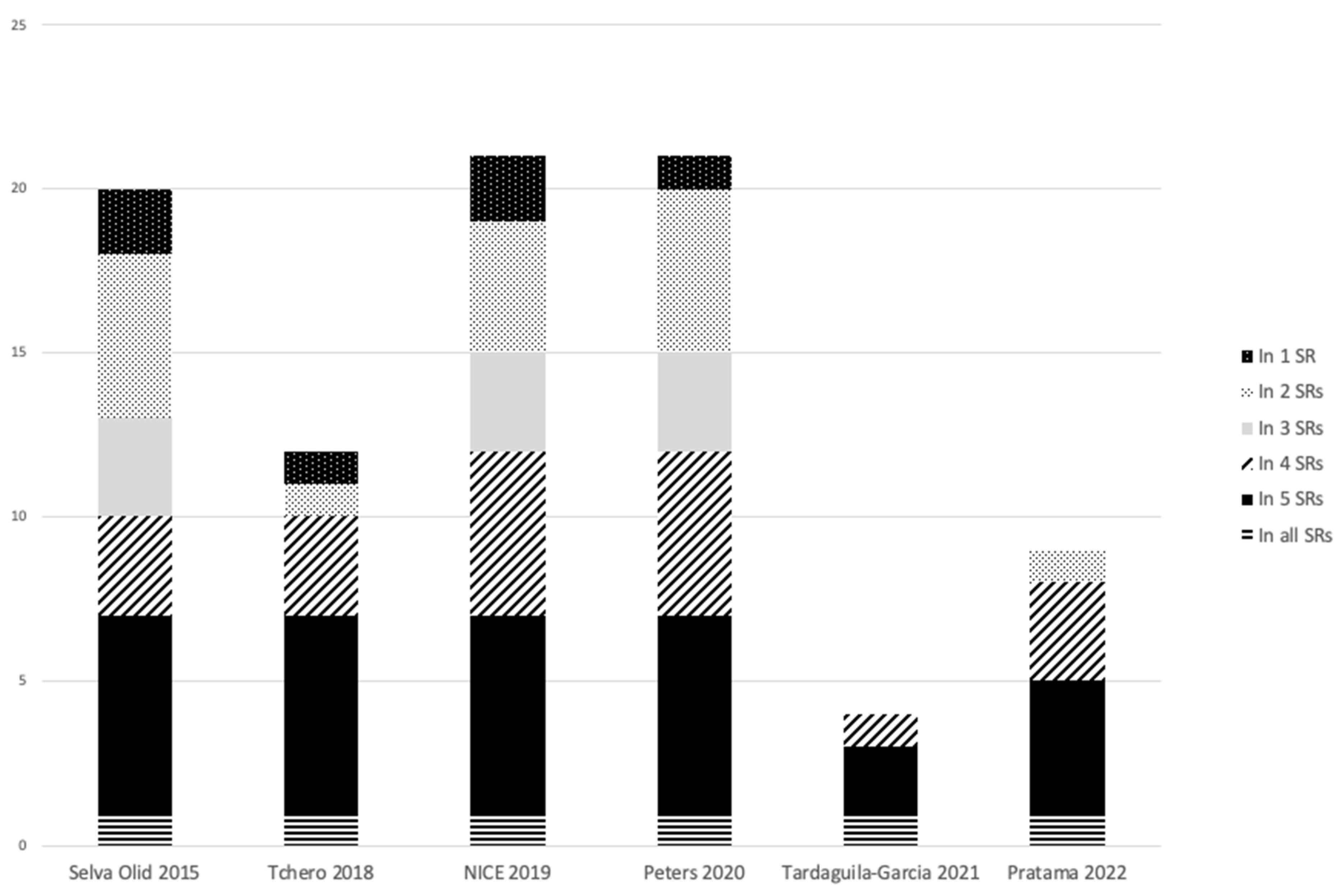
3.1. Summary of Included Systematic Reviews
3.2. Quality of the Systematic Reviews
3.3. Outcomes: Antimicrobial Interventions
3.3.1. Fluoroquinolones versus Piperacillin–Tazobactam (TZP)/Amoxicillin–Clavulanic Acid (AMC)
3.3.2. Ertapenem (ETP) versus TZP
3.3.3. Tigecycline (TGC) versus Ertapenem (ETP) ± Vancomycin (VAN)
3.3.4. Ampicillin–Sulbactam (SAM) versus Cefoxitin (FOX)
3.3.5. Adverse Drug Events
4. Discussion
4.1. Antibiotic Outcomes
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

| Ovid Medline 1946 to 20 January 2023 |
| 63 results |
| Embase via OVID, 1947 to present |
| 211 results |
| Cochrane Database of Systematic Reviews, issue 1 of 12 January 2023 |
| 59 results |
| CINAHL plus (EBSCOhost) |
| 38 results |
| Prospero database of systematic reviews | MeSH DESCRIPTOR Diabetic Foot EXPLODE ALL TREES | 128 results |
Appendix B
| Study | Exclusion Reason |
|---|---|
| Abolghasemi et al. 2019 | Not a systematic review |
| Awasthi et al. 2021 | Not a systematic review |
| Bartoszko et al. 2018 | Protocol only |
| Esposito et al. 2016 | Did not meet inclusion criteria |
| Game et al. 2016 | Did not meet inclusion criteria |
| Karri V et al. 2016 | Not a systematic review |
| Norman et al. 2016 | Did not meet inclusion criteria |
| Perez-Panero et al. 2019 | Did not meet inclusion criteria |
| Peters et al. 2016 | Superseded systematic review |
| Singh et al. 2021 | Not a systematic review (narrative review) |
| Tchero et al. 2019 | Not a systematic review (scoping review) |
| Urtugrul et al. 2020 | Not a systematic review (narrative review) |
| Vas et al. 2018 | Did not meet inclusion criteria |
| Yazdanapah et al. 2015 | Did not meet inclusion criteria |
| Zhang et al. 2020 | Protocol only |
References
- Lipsky, B.A.; Senneville, É.; Abbas, Z.G.; Aragón-Sánchez, J.; Diggle, M.; Embil, J.M.; Kono, S.; Lavery, L.A.; Malone, M.; van Asten, S.A.; et al. Guidelines on the diagnosis and treatment of foot infection in persons with diabetes (IWGDF 2019 update). Diabetes Metab. Res. Rev. 2020, 36 (Suppl. 1), e3280. [Google Scholar] [CrossRef]
- Karri, V.V.S.R.; Kuppusamy, G.; Talluri, S.V.; Yamjala, K.; Mannemala, S.S.; Malayandi, R. Current and emerging therapies in the management of diabetic foot ulcers. Curr. Med. Res. Opin. 2016, 32, 519–542. [Google Scholar] [CrossRef] [PubMed]
- Antibiotic Expert Group. Therapeutic Guidelines: Antibiotic; Version 16; Therapeutic Guidelines Limited: Melbourne, Australia, 2019; Available online: https://www.tg.org.au (accessed on 29 January 2023).
- Macdonald, K.E.; Boeckh, S.; Stacey, H.J.; Jones, J.D. The microbiology of diabetic foot infections: A meta-analysis. BMC Infect Dis. 2021, 21, 770. [Google Scholar] [CrossRef]
- National Institute of Health and Care Excellence. Diabetic Foot Problems: Prevention and Management [NG19]; NICE: London, UK, 2019; Available online: https://www.nice.org.uk/guidance/ng19 (accessed on 29 January 2023).
- Lipsky, B.A.; Berendt, A.R.; Cornia, P.B.; Pile, J.C.; Peters, E.J.; Armstrong, D.G.; Deery, H.G.; Embil, J.M.; Joseph, W.S.; Karchmer, A.W.; et al. 2012 Infectious Diseases Society of America clinical practice guideline for the diagnosis and treatment of diabetic foot infections. Clin. Infect. Dis. 2012, 54, e132–e173. [Google Scholar] [CrossRef]
- Smith, V.; Devane, D.; Begley, C.M.; Clarke, M. Methodology in conducting a systematic review of systematic reviews of healthcare interventions. BMC Med. Res. Methodol. 2011, 11, 15. [Google Scholar] [CrossRef]
- Pollock, M.; Fernandes, R.M.; Becker, L.A.; Pieper, D.; Hartling, L. Chapter V: Overviews of Reviews. In Cochrane Handbook for Systematic Reviews of Interventions; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Version 6.3 (Updated February 2022); Cochrane: London, UK, 2022; Available online: www.training.cochrane.org/handbook (accessed on 5 March 2023).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Bramer, W.; Bain, P. Updating search strategies for systematic reviews using EndNote. J. Med. Libr. Assoc. 2017, 105, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Selva Olid, A.; Sola, I.; Barajas-Nava, L.A.; Gianneo, O.D.; Bonfill Cosp, X.; Lipsky, B.A. Systemic antibiotics for treating diabetic foot infections. Cochrane Database Syst. Rev. 2015, 9, CD009061. [Google Scholar] [CrossRef] [PubMed]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef]
- National Institute of Health and Care Excellence. Diabetic Foot Infection: Antimicrobial Prescribing, Evidence Review [NG19]; NICE: London, UK, 2019; Available online: https://www.nice.org.uk/guidance/ng19/evidence (accessed on 29 January 2023).
- Peters, E.J.G.; Lipsky, B.A.; Senneville, É.; Abbas, Z.G.; Aragón-Sánchez, J.; Diggle, M.; Embil, J.M.; Kono, S.; Lavery, L.A.; Malone, M.; et al. Interventions in the management of infection in the foot in diabetes: A systematic review. Diabetes Metab. Res. Rev. 2020, 36 (Suppl 1), e3282. [Google Scholar] [CrossRef]
- Tchero, H.; Kangambega, P.; Noubou, L.; Becsangele, B.; Fluieraru, S.; Teot, L. Antibiotic therapy of diabetic foot infections: A systematic review of randomized controlled trials. Wound Repair Regen. 2018, 26, 381–391. [Google Scholar] [CrossRef] [PubMed]
- Tardaguila-Garcia, A.; Sanz-Corbalan, I.; Garcia-Alamino, J.M.; Ahluwalia, R.; Uccioli, L.; Lazaro-Martinez, J.L. Medical versus surgical treatment for the management of diabetic foot osteomyelitis: A systematic review. J. Clin. Med. 2021, 10, 1237. [Google Scholar] [CrossRef] [PubMed]
- Pratama, V.; Risni, H.W.; Yunir, E.; Sauriasari, R. A Systematic Review of Randomized Controlled Trials of Antibiotic Use in Diabetic Foot Ulcer Infections: Focus on Clinical Cure. Infect. Chemother. 2022, 54, 125–139. [Google Scholar] [CrossRef] [PubMed]
- Giordano, P.; Song, J.; Pertel, P.; Herrington, J.; Kowalsky, S. Sequential intravenous/oral moxifloxacin versus intravenous piperacillin-tazobactam followed by oral amoxicillin-clavulanate for the treatment of complicated skin and skin structure infection. Int. J. Antimicrob. Agents 2005, 26, 357–365. [Google Scholar] [CrossRef]
- Schaper, N.C.; Dryden, M.; Kujath, P.; Nathwani, D.; Arvis, P.; Reimnitz, P.; Alder, J.; Gyssens, I.C. Efficacy and safety of IV/PO moxifloxacin and IV piperacillin/tazobactam followed by PO amoxicillin/clavulanic acid in the treatment of diabetic foot infections: Results of the RELIEF study. Infection 2013, 41, 175–186. [Google Scholar] [CrossRef]
- Lipsky, B.A.; Giordano, P.; Choudhri, S.; Song, J. Treating diabetic foot infections with sequential intravenous to oral moxifloxacin compared with piperacillin–tazobactam/amoxicillin–clavulanate. J. Antimicrob. Chemother. 2007, 60, 370–376. [Google Scholar] [CrossRef]
- Siami, G.; Christou, N.; Eiseman, I.; Tack, K.J.; Severe Skin and Soft Tissue Infections Study Group. Clinafloxacin versus piperacillin-tazobactam in treatment of patients with severe skin and soft tissue infections. Antimicrob. Agents Chemother. 2001, 45, 525–531. [Google Scholar] [CrossRef]
- Graham, D.R.; Talan, D.A.; Nichols, R.L.; Lucasti, C.; Corrado, M.; Morgan, N.; Fowler, C.L. Once-daily, high-dose levofloxacin versus ticarcillin-clavulanate alone or followed by amoxicillin-clavulanate for complicated skin and skin-structure infections: A randomized, open-label trial. Clin. Infect. Dis. 2002, 35, 381–389. [Google Scholar] [CrossRef]
- Vick-Fragoso, R.; Hernández-Oliva, G.; Cruz-Alcázar, J.; Amábile-Cuevas, C.F.; Arvis, P.; Reimnitz, P.; Bogner, J.R.; STIC Study Group. Efficacy and safety of sequential intravenous/oral moxifloxacin vs intravenous/oral amoxicillin/clavulanate for complicated skin and skin structure infections. Infection 2009, 37, 407–417. [Google Scholar] [CrossRef]
- Lipsky, B.A.; Baker, P.D.; Landon, G.C.; Fernau, R. Antibiotic therapy for diabetic foot infections: Comparison of two parenteral-to-oral regimens. Clin. Infect. Dis. 1997, 24, 643–648. [Google Scholar] [CrossRef]
- Xu, Z.R.; Ran, X.W.; Xian, Y.; Yan, X.D.; Yuan, G.Y.; Mu, S.M.; Shen, J.F.; Zhang, B.S.; Gan, W.J.; Wang, J. Ertapenem versus piperacillin/tazobactam for diabetic foot infections in China: A Phase 3, multicentre, randomized, double-blind, active-controlled, non-inferiority trial. J. Antimicrob. Chemother. 2016, 71, 1688–1696. [Google Scholar] [CrossRef] [PubMed]
- Graham, D.R.; Lucasti, C.; Malafaia, O.; Nichols, R.L.; Holtom, P.; Perez, N.Q.; McAdams, A.; Woods, G.L.; Ceesay, T.P.; Gesser, R. Ertapenem once daily versus piperacillin-tazobactam 4 times per day for treatment of complicated skin and skin-structure infections in adults: Results of a prospective, randomized, double-blind multicenter study. Clin. Infect. Dis. 2002, 34, 1460–1468. [Google Scholar] [CrossRef] [PubMed]
- Lipsky, B.A.; Armstrong, D.G.; Citron, D.M.; Tice, A.D.; Morgenstern, D.E.; Abramson, M.A. Ertapenem versus piperacillin/tazobactam for diabetic foot infections (SIDESTEP): Prospective, randomised, controlled, double-blinded, multicentre trial. Lancet 2005, 366, 1695–1703. [Google Scholar] [CrossRef]
- Bouter, K.P.; Visseren, F.L.; van Loenhout, R.M.; Bartelink, A.K.; Erkelens, D.W.; Diepersloot, R.J. Treatment of diabetic foot infection: An open randomised comparison of imipenem/cilastatin and piperacillin/clindamycin combination therapy. Int. J. Antimicrob. Agents 1996, 7, 143–147. [Google Scholar] [CrossRef]
- Harkless, L.; Boghossian, J.; Pollak, R.; Caputo, W.; Dana, A.; Gray, S.; Wu, D. An open-label, randomized study comparing efficacy and safety of intravenous piperacillin/tazobactam and ampicillin/sulbactam for infected diabetic foot ulcers. Surg. Infect. (Larchmt.) 2005, 6, 27–40. [Google Scholar] [CrossRef] [PubMed]
- Saltoglu, N.; Dalkiran, A.; Tetiker, T.; Bayram, H.; Tasova, Y.; Dalay, C.; Sert, M. Piperacillin/tazobactam versus imipenem/cilastatin for severe diabetic foot infections: A prospective, randomized clinical trial in a university hospital. Clin. Microbiol. Infect. 2010, 16, 1252–1257. [Google Scholar] [CrossRef]
- Grayson, M.L.; Gibbons, G.W.; Habershaw, G.M.; Freeman, D.V.; Pomposelli, F.B.; Rosenblum, B.I.; Levin, E.; Karchmer, A.W. Use of ampicillin/sulbactam versus imipenem/cilastatin in the treatment of limb-threatening foot infections in diabetic patients. Clin. Infect. Dis. 1994, 18, 683–693. [Google Scholar] [CrossRef]
- Chantelau, E.; Tanudjaja, T.; Altenhöfer, F.; Ersanli, Z.; Lacigova, S.; Metzger, C. Antibiotic treatment for uncomplicated neuropathic forefoot ulcers in diabetes: A controlled trial. Diabet. Med. 1996, 13, 156–159. [Google Scholar] [CrossRef]
- Tan, J.S.; Wishnow, R.M.; Talan, D.A.; Duncanson, F.P.; Norden, C.W. Treatment of hospitalized patients with complicated skin and skin structure infections: Double-blind, randomized, multicenter study of piperacillin-tazobactam versus ticarcillin-clavulanate. The Piperacillin/Tazobactam Skin and Skin Structure Study Group. Antimicrob. Agents Chemother. 1993, 37, 1580–1586. [Google Scholar] [CrossRef]
- Erstad, B.L.; McIntyre, K.E. Prospective, Randomized Comparison of Ampicillin/Sulbactam and Cefoxitin for Diabetic Foot Infections. J. Vasc. Surg. 1997, 31, 419–426. [Google Scholar] [CrossRef]
- Bradsher, R.W.; Snow, R.M. Ceftriaxone treatment of skin and soft tissue infections in a once daily regimen. Am. J. Med. 1984, 77, 63–67. [Google Scholar]
- Clay, P.G.; Graham, M.R.; Lindsey, C.C.; Lamp, K.C.; Freeman, C.; Glaros, A. Clinical efficacy, tolerability, and cost savings associated with the use of open-label metronidazole plus ceftriaxone once daily compared with ticarcillin/clavulanate every 6 hours as empiric treatment for diabetic lower-extremity infections in older males. Am. J. Geriatr. Pharmacother. 2004, 2, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Lobmann, R.; Ambrosch, A.; Seewald, M.; Dietlein, M.; Zink, K.; Kullmann, K.H.; Lehnert, H. Antibiotic therapy for diabetic foot infections: Comparison of cephalosporines with chinolones. Diabetes Nutr. Metab. 2004, 17, 156–162. [Google Scholar]
- Patil, S.V.; Mane, R.R. Comparison of efficacy of levofloxacin-metronidazole combination versus ceftriaxone in cases of moderate diabetic foot infection. Int. J. Basic Clin. Pharmacol. 2016, 5, 1775–1779. [Google Scholar] [CrossRef]
- Noel, G.J.; Bush, K.; Bagchi, P.; Ianus, J.; Strauss, R.S. A randomized, double-blind trial comparing ceftobiprole medocaril with vancomycin plus ceftazidime for the treatment of patients with complicated skin and skin-structure infections. Clin. Infect. Dis. 2008, 46, 647–655. [Google Scholar] [CrossRef]
- Hughes, C.E.; Johnson, C.C.; Bamberger, D.M.; Reinhardt, J.F.; Peterson, L.R.; Mulligan, M.E.; Gerding, D.N.; George, W.L.; Finegold, S.M. Treatment and long-term follow-up of foot infections in patients with diabetes or ischemia: A randomized, prospective, double-blind comparison of cefoxitin and ceftizoxime. Clin. Ther. 1987, 10 (Suppl. A), 36–49. [Google Scholar]
- File, T.M., Jr.; Tan, J.S. Amdinocillin plus cefoxitin versus cefoxitin alone in therapy of mixed soft tissue infections (including diabetic foot infections). Am. J. Med. 1983, 75, 100–105. [Google Scholar] [CrossRef]
- Lipsky, B.A.; Pecoraro, R.E.; Larson, S.A.; Hanley, M.E.; Ahroni, J.H. Outpatient management of uncomplicated lower-extremity infections in diabetic patients. Arch. Intern. Med. 1990, 150, 790–797. [Google Scholar] [CrossRef]
- Arbeit, R.D.; Maki, D.; Tally, F.P.; Campanaro, E.; Eisenstein, B.I.; Daptomycin 98-01 and 99-01 Investigators. The safety and efficacy of daptomycin for the treatment of complicated skin and skin-structure infections. Clin. Infect. Dis. 2004, 38, 1673–1681. [Google Scholar] [CrossRef]
- Lipsky, B.A.; Stoutenburgh, U. Daptomycin for treating infected diabetic foot ulcers: Evidence from a randomized, controlled trial comparing daptomycin with vancomycin or semi-synthetic penicillins for complicated skin and skin-structure infections. J. Antimicrob. Chemother. 2005, 55, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Lauf, L.; Ozsvár, Z.; Mitha, I.; Regöly-Mérei, J.; Embil, J.M.; Cooper, A.; Sabol, M.B.; Castaing, N.; Dartois, N.; Yan, J.; et al. Phase 3 study comparing tigecycline and ertapenem in patients with diabetic foot infections with and without osteomyelitis. Diagn. Microbiol. Infect. Dis. 2014, 78, 469–480. [Google Scholar] [CrossRef] [PubMed]
- Lipsky, B.A.; Itani, K.; Norden, C.; Linezolid Diabetic Foot Infections Study Group. Treating foot infections in diabetic patients: A randomized, multicenter, open-label trial of linezolid versus ampicillin-sulbactam/amoxicillin-clavulanate. Clin. Infect. Dis. 2004, 38, 17–24. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Types/# Studies | PICO Question/s | Comments | |
|---|---|---|---|
| Selva Olid et al. 2015 (Cochrane Review) [11] | Twenty RCTs | P—T1DM/T2DM with foot infection. I—Systemic antibiotics (oral or parenteral). C—Any other antibiotic control group, placebo or topical foot care. O—Resolution of infection, time to resolution, adverse effects, and complications. | Meta-analysis on two interventions: ETP vs. TZP (two studies) and fluoroquinolones vs. TZP/AMC (three studies). Uses Cochrane Risk of Bias tool. |
| Tchero et al. 2018 [15] | Twelve RCTs—open label and blind (relevant to this review) | P—T1DM/T2DM moderate–severe DFI ± OM, >18. I—All antimicrobials (including topical). C—Other antimicrobials, placebo, foot care, and surgery. O—Clinical cure or improvement rate. | Solely people with diabetes with complicated DFI. No meta-analysis. Uses Cochrane Risk of Bias tool. |
| NICE 2019 [13] | Twenty-two RCTs | P—≥72 h old, T1DM/T2DM, and foot ulcer with SSTI ± OM. I—Any antibiotic regimen. C—Standard care, other antimicrobials, and other treatments (not surgery). O—Cure rate, amputation, adverse events, length of stay, and QOL. | Completed to inform the NICE guideline. Children/young people in inclusion criteria; nil studies found. Recalculated results for studies presenting RR, 95% CI, and absolute differences. Uses GRADE assessment for risk of bias and quality. |
| Peters et al. 2020 (IWGDF) [14] | Twenty RCTs; one cohort study (relevant to this review) | P—T1DM/T2DM, ≥18. I—Antibiotics, antiseptic, surgery, and adjunctive therapy. C—Another intervention, placebo, no treatment, or usual care. O—Clinical cure of infection, amputation, recurrence, death, hospitalization, resolution of ulcer, eradication of microbial pathogens, QOL, adverse effects, or cost of treatment. | Completed to inform the IWGDF guideline. Analyzed SSTI and DFO separately. No meta-analysis. Uses Dutch Cochrane quality tool and SIGN level of evidence tool. |
| Tardaguila-Garcia et al. 2021 [16] | Four RCTs (relevant to this review) | P—>18 with DFO. I—Antibiotics or surgery. C—Antibiotics or surgery. O—Cure rates. | Focused on diabetic foot osteomyelitis. No meta-analysis Uses Cochrane Risk of Bias tool |
| Pratama et al. 2022 [17] | Nine RCTs (relevant to this review) | P—T1DM/T2DM, DFUI with/without OM, ≥18. I—Antibiotics (parenteral, oral, and topical). C—Other antibiotics or placebo. O—Clinical cure. | Additionally, reported microbiological profiles. No meta-analysis. Uses Jadad criteria for risk of bias and quality. |
| AMSTAR-2 Items | Selva Olid 2015 [11] | Tchero 2018 [15] | Peters 2020 [14] | NICE 2019 [13] | Tardaguila-Garcia 2021 [16] | Pratama 2022 [17] |
|---|---|---|---|---|---|---|
| 1. PICO components | Yes | Yes | Yes | Yes | Yes | Yes |
| 2. A priori design | Yes | Partial | Partial | Yes | Partial | Partial |
| 3. Explanation of study design inclusion | No | No | No | No | No | No |
| 4. Comprehensive literature search | Yes | Yes | Yes | Yes | Partial | Partial |
| 5. Duplicate study selection | Yes | Yes | Yes | Yes | Yes | Yes |
| 6. Duplicate data extraction | Yes | Yes | Yes | Yes | Yes | Yes |
| 7. List excluded studies | Yes | No | No | Yes | No | No |
| 8. Characteristics of included studies | Yes | Partial | Yes | Yes | Partial | Partial |
| 9. Report quality of included studies | Yes | Yes | Yes | Yes | Yes | Partial |
| 10. Report funding of included studies | Yes | No | Yes | Yes | No | No |
| 11. Appropriate meta-analysis method | Yes | n/a | n/a | n/a | n/a | n/a |
| 12. Assess risk of bias on meta-analysis | Yes | n/a | n/a | n/a | n/a | n/a |
| 13. Consider risk of bias with results | Yes | Yes | Yes | Yes | Yes | Yes |
| 14. Consider heterogeneity with results | Yes | Yes | Yes | Yes | Yes | Yes |
| 15. Assess publication bias | Yes | n/a | n/a | n/a | n/a | n/a |
| 16. State conflicts of interest | Yes | Yes | Yes | Yes | Yes | Yes |
| Overall Confidence | High | Low | Moderate | High | Low | Low |
| Intervention | Comparator | Study ID | Outcome | Measure of Effect (95% CI) # | Direction of Effect | SR Inclusion |
|---|---|---|---|---|---|---|
| Fluoroquinolones | ||||||
| Moxifloxacin | TZP/AMC | Giordano 2005 [18] | Clinical resolution | RR 1.11 (0.80–1.54) [11] | NS | Selva Olid 2015 [11] |
| Schaper 2013 (RELIEF) [19] | Clinical resolution Amputations Adverse events | RR 0.98 (0.84–1.13) RR 0.84 (0.51–1.38) RR 0.97 (0.66–1.42) [13] | NS NS NS | Selva Olid 2015 [11]; Tchero 2018 [15]; Peters 2020 [14]; NICE 2019 [13]; Pratama 2022 [17] | ||
| Lipsky 2007 [20] | Clinical cure Adverse events Withdrawals | RR 1.14 (0.75–1.72) RR 2.54 (1.21–5.34) RR 1.02 (0.52–1.90) [13] | NS Favors TZP NS | Tchero 2018 [15]; Peters 2020 [14]; NICE 2019 [13]; Pratama 2022 [17] | ||
| Clinafloxacin | TZP/AMC | Siami 2001 [21] | Clinical resolution | RR 1.01 (0.55–1.86) [11] | NS | Selva Olid 2015 [11]; Peters 2020 [14]; NICE 2019 [13] |
| Meta-analysis Fluoroquinolones | TZP/AMC | Giordano 2005; Schaper 2013; Siami 2001 | Clinical resolution | RR 1.03 (0.89–1.20) [11] | NS | Selva Olid 2015 [11] |
| Levofloxacin | Ticarcillin–clavulanate | Graham 2002b [22] | Clinical resolution | RR 0.97 (0.60–1.55) [11] | NS | Selva Olid 2015 [11]; Peters 2020 [14] |
| Moxifloxacin | AMC | Vick-Fragoso 2009 (STIC) [23] | clinical cure | RR 0.79 (0.57–1.08) [11] | NS | Selva Olid 2015 [11]; NICE 2019 [13]; Peters 2020 [14]; Pratama 2022 [17] |
| Ofloxacin | SAM/AMC | Lipsky 1997 [24] | Clinical resolution Amputation Adverse events | RR 1.13 (0.88–1.47) RR 0.11 (0.01–1.94) RR 1.82 (0.89–3.72) [11] | NS NS NS | Selva Olid 2015 [11]; Tchero 2018 [15]; NICE 2019 [13]; Peters 2020 [14]; Tardaguila-Garcia 2021 [16] |
| Carbapenems | ||||||
| Ertapenem | Piperacillin–tazobactam | Xu 2016 ‡ [25] | Cure rate Cure (severe DFI) Clinical resolution Adverse events | Diff: −3.8% (−8.3–0.0%) Diff: –5.7% (−12.1–−0.3%) [17] RR 0.97 (0.90–1.04) RR 1.42 (0.69–2.91) [13] | NS Favors TZP NS NS | Tchero 2018 [15]; NICE 2019 [13]; Peters 2020 [14]; Pratama 2022 [17] |
| Graham 2002a [26] | Clinical resolution | RR 0.89 (0.58–1.36) [11] | NS | Selva Olid 2015 [11]; Peters 2020 [14] | ||
| Lipsky 2005a (SIDESTEP) [27] | Clinical resolution Adverse events | RR 1.08 (0.97–1.21) RR 0.76 (0.53–1.09) [11] | NS NS | Selva Olid 2015 [11]; Tchero 2018 [15]; NICE 2019 [13]; Peters 2020 [14]; Pratama 2022 [17] | ||
| Meta-analysis Ertapenem | TZP | Graham 2002a; Lipsky 2005a | Clinical resolution | RR 1.07 (0.96–1.19) [11] | NS | Selva Olid 2015 [11] |
| Imipenem | Piperacillin + clindamycin | Bouter 1996 [28] | Clinical resolution Recurrence Adverse events | RR 0.73 (0.24–2.24) RR 7.61 (0.42–139) RR 0.27 (0.09–0.84) [11] | NS NS Favors IMP | Selva Olid 2015 [11]; NICE 2019 [13] |
| Penicillins | ||||||
| TZP | SAM | Harkless 2005 [29] | Clinical resolution Amputations Adverse events | RR 1.02 (0.86–1.20) RR 0.97 (0.51–1.84) RR 1.14 (0.99–1.32) [11] | NS NS NS | Selva Olid 2015 [11]; Tchero 2018 [15]; NICE 2019 [13]; Peters 2020 [14]; Pratama 2022 [17] |
| TZP | Imipenem | Saltoglu 2010 [30] | Clinical resolution Amputations Recurrence Adverse events | RR 1.66 (0.84–3.26) RR 0.87 (0.59–1.28) RR 5.31 (0.27–106.46) RR 3.19 (0.95–10.72) [11] | NS NS NS NS | Selva Olid 2015 [11]; Tchero 2018 [15]; NICE 2019 [13]; Peters 2020 [14]; Pratama 2022 [17] |
| SAM | Imipenem | Grayson 1994 [31] | Clinical resolution Amputation Recurrence Adverse events | RR 0.95 (0.80–1.14) RR 0.85 (0.62–1.15) RR 0.71 (0.42–1.21) RR 1.06 (0.61–1.85) [11] | NS NS NS NS | Selva Olid 2015 [11]; Tchero 2018 [15]; NICE 2019 [13]; Peters 2020 [14]; Tardaguila-Garcia 2021 [16] |
| AMC | Placebo | Chantelau 1996 [32] | Ulcer healing rate | 27.3% vs. 45.5% [15] | Favors placebo | Tchero 2018 [15] |
| TZP | Ticarcillin-clavulanate | Tan 1993 [33] | Clinical resolution | RR 1.16 (0.59–2.29) [11] | NS | Selva Olid 2015 [11], NICE 2019 [13] |
| SAM | Cefoxitin | Erstad 1997 [34] | Clinical resolution Amputation Adverse events | RR 0.14 (0.02–1.05) RR 1.00 (0.48–2.08) RR 1.17 (0.49–2.79) [11] | NS NS NS | Selva Olid 2015 [11], NICE 2019 [13], Peters 2020 [14] |
| Cephalosporins | ||||||
| Ceftriaxone | Cefazolin | Bradsher 1984 [35] | Cure Adverse events | RR 0.84 (0.57–1.24) RR 0.92 (0.48–1.78) [13] | NS NS | NICE 2019 [13]; Peters 2020 [14] |
| Ceftriaxone + metronidazole | Ticarcillin-clavulanate | Clay 2004 [36] | Cure | RR 1.05 (0.85–1.28) [13] | NS | Selva Olid 2015 [11]; Tchero 2018 [15]; NICE 2019 [13]; Peters 2020 [14]; |
| Ceftriaxone | Fluoroquinolone | Lobmann 2004 [37] | Clinical response | 58% vs. 51.1% [14] | NS | Peters 2020 [14] |
| Ceftriaxone | Levofloxacin + metronidazole | Patil 2016 * [38] | Microbiological cure | 58.6% vs. 62.1% [17] | NS | Tchero 2018 [15]; Pratama 2022 [17] |
| Ceftobiporole | Ceftazidime + vancomycin | Noel 2008a [39] | Clinical resolution | RR 1.05 (0.90–1.23) [11] | NS | Selva Olid 2015 [11]; Peters 2020 [14] |
| Cefoxitin | Ceftizoxime | Hughes 1987 [40] | Clinical response Adverse events | RR 0.83 (0.60–1.14) RR 1.31 (0.84–2.04) [13] | NS NS | NICE 2019 [13] |
| Cefoxitin + amdinocillin | Cefoxitin | File 1983 [41] | Clinical response Amputation | RR 1.26 (0.93–1.70) RR 0.53 (0.11–2.56) [13] | NS NS | NICE 2019 [13] |
| Others | ||||||
| Clindamycin | Cephalexin | Lipsky 1990 [42] | Clinical resolution Ulcer healing Adverse events | RR 1.07 (0.79–1.45) RR 1.20 (0.59–2.46) RR 0.47 (0.04–4.84) [11] | NS NS NS | Selva Olid 2015 [11]; NICE 2019 [13]; Peters 2020 [14] |
| Daptomycin | Vancomycin or semisynthetic penicillin | Arbeit 2004 [43] | Clinical resolution Adverse effects | RR 0.94 (0.68–1.30) RR 0.61 (0.39–0.94) [11] | NS Favors daptomycin | Selva Olid 2015 [11] |
| Lipsky 2005b [44] | Cure (vs. penicillin) Cure (vs. vancomycin) | RR 0.91 (0.62–1.33) RR 1.04 (0.69–1.56) [13] | NS NS | NICE 2019 [13]; Peters 2020 [14] | ||
| Tigecycline | Ertapenem +/− vancomycin | Lauf 2014 [45] | Clinical resolution Resolution (OM) Clinical cure Clinical cure (OM) Adverse events | RR 1.09 (1.01–1.18) RR 2.08 (1.27–3.39) [11] RR 0.94 (0.99–1.14) RR 0.69 (0.35–1.32) RR 1.25 (1.13–1.38) [13] | Favors ETP Favors ETP NS NS Favors ETP | Included in all SR |
| Linezolid | SAM | Lipsky 2004 [46] | Clinical cure Adverse events | RR 1.14 (0.99–1.31) RR 2.66 (1.49–4.73) [13] | NS Favors SAM | Selva Olid 2015 [11]; NICE 2019 [13]; Peters 2020 [14]; Tardaguila-Garcia 2021 [16] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wright, A.; Wood, S.; De Silva, J.; Bell, J.S. Systemic Antimicrobial Therapy for Diabetic Foot Infections: An Overview of Systematic Reviews. Antibiotics 2023, 12, 1041. https://doi.org/10.3390/antibiotics12061041
Wright A, Wood S, De Silva J, Bell JS. Systemic Antimicrobial Therapy for Diabetic Foot Infections: An Overview of Systematic Reviews. Antibiotics. 2023; 12(6):1041. https://doi.org/10.3390/antibiotics12061041
Chicago/Turabian StyleWright, Angela, Stephen Wood, Janath De Silva, and J. Simon Bell. 2023. "Systemic Antimicrobial Therapy for Diabetic Foot Infections: An Overview of Systematic Reviews" Antibiotics 12, no. 6: 1041. https://doi.org/10.3390/antibiotics12061041
APA StyleWright, A., Wood, S., De Silva, J., & Bell, J. S. (2023). Systemic Antimicrobial Therapy for Diabetic Foot Infections: An Overview of Systematic Reviews. Antibiotics, 12(6), 1041. https://doi.org/10.3390/antibiotics12061041