
Optimizing Antibiotic Prescribing for Acute Respiratory Tract Infections in German Primary Care: Results of the Regional Intervention Study CHANGE-3 and the Nested cRCT

 , , , and
, , , and
Abstract
1. Introduction
2. Results
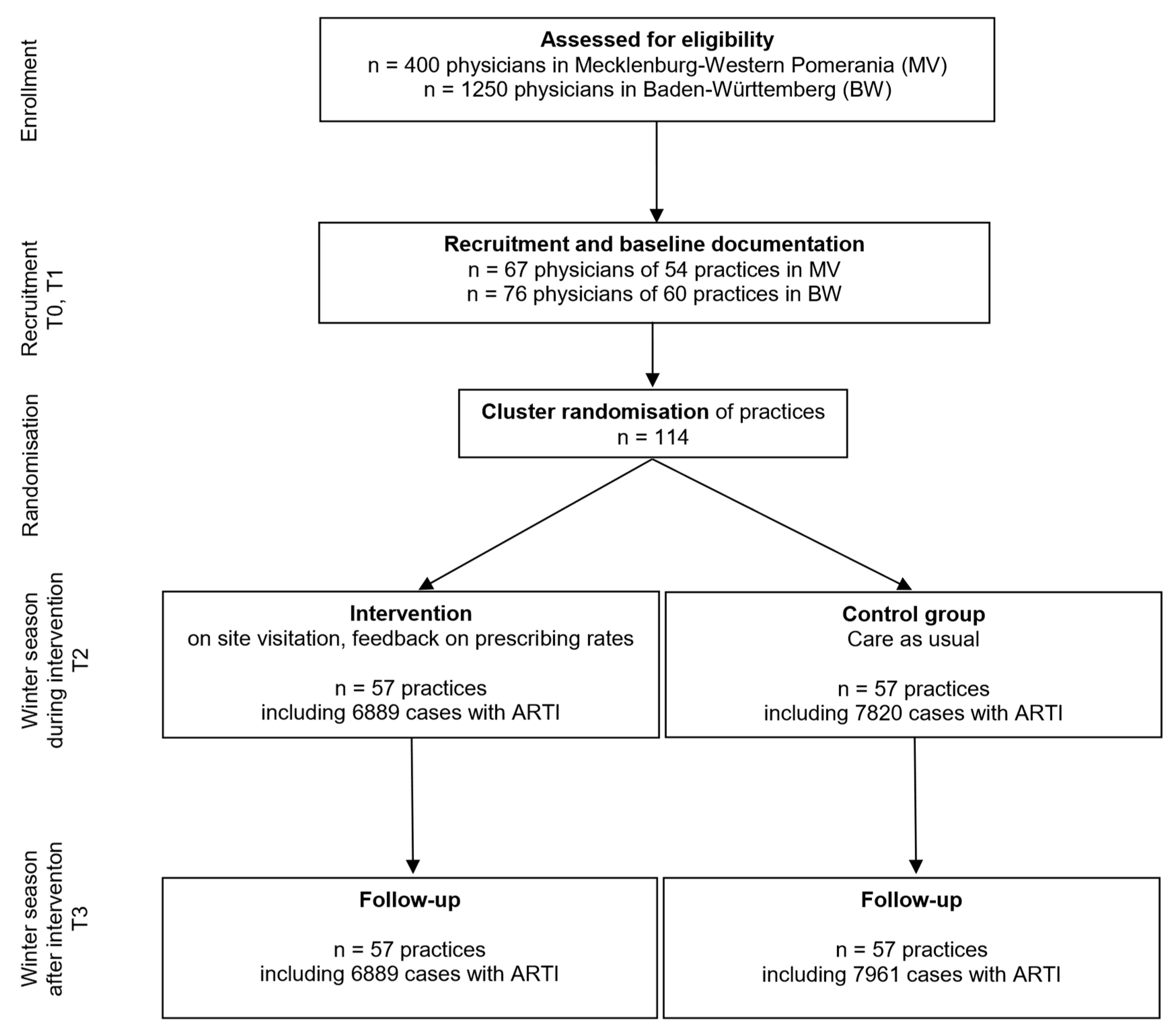
2.1. Baseline Data cRCT
2.2. Antibiotic Prescribing for ARTIs in the cRCT
2.3. Baseline Data of the Regional Intervention Group
2.4. Antibiotic Prescribing for ARTIs in Public Campaign Regions
2.5. Secondary Outcomes
3. Materials and Methods
3.1. Study Design
3.2. Recruitment
3.3. Randomisation of Practices in cRCT
3.4. Interventions
3.5. Data Protection and Consent
3.6. Outcome Data
3.7. Sample Size
3.8. Data Collection, Completeness, and Quality
3.9. Statistical Methods
3.10. Study Registration and Ethical Approval
4. Discussion
4.1. Summary of Findings
4.2. Findings in Research Context
4.3. Strengths and Limitations
4.4. Implications for Practice
4.5. Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AOK | Largest statutory health insurance provider in Germany |
| ARTI | Acute Respiratory Tract Infection |
| BW | Baden-Württemberg |
| cRCT | Cluster Randomised Controlled Trial |
| DE | Design effect |
| ESAC-Net | European Surveillance of Antimicrobial Consumption Network |
| GP | General Practitioner |
| HMG | Hierarchised Morbidity Groups |
| ICC | Intra-cluster Correlation Coefficient |
| ICD | International Statistical Classification of Diseases and Related Health Problems |
| MV | Mecklenburg-Western Pomerania |
| OR | Odds Ratio |
References
- Bundesministerium für Gesundheit; Bundesministerium für Ernährung und Landwirtschaft; Bundesministerium für Bildung und Forschung. DART 2020—Antibiotika-Resistenzen Bekämpfen zum Wohl von Mensch und Tier; Die Bundesregierung: Berlin, Germany, 2015.
- Bundesamts für Verbraucherschutz und Lebensmittelsicherheit. GERMAP 2012—Antibiotika-Resistenz und -Verbrauch; Antiinfectives Intelligence—Gesellschaft für klinisch-mikrobiologische Forschung und Kommunikation mbH: Berlin, Germany, 2014. [Google Scholar]
- Kassenärztliche Bundesvereinigung; Arzneimittelkommission der deutschen Ärzteschaft. Wirkstoff Aktuell: Rationale Antibiotikatherapie bei Infektionen der Oberen Atemwege, Ausgabe 1/2012; KBV: Berlin, Germany, 2012. [Google Scholar]
- Kassenärztliche Bundesvereinigung; Arzneimittelkommission der deutschen Ärzteschaft. Wirkstoff Aktuell: Rationale Antibiotikatherapie bei Infektionen der Unteren Atemwege, Ausgabe 3/2013; KBV: Berlin, Germany, 2013. [Google Scholar]
- Altiner, A.; Bell, J.; Duerden, M.; Essack, S.; Kozlov, R.; Noonan, L.; Oxford, J.; Pignatari, A.C.; Sessa, A.; Van Der Velden, A. More action, less resistance: Report of the 2014 summit of the Global Respiratory Infection Partnership. Int. J. Pharm. Pract. 2015, 23, 370–377. [Google Scholar] [CrossRef] [PubMed]
- Adriaenssens, N.; Coenen, S.; Tonkin-Crine, S.; Verheij, T.J.M.; Little, P.; Goossens, H.; on behalf of the ESAC Project Group. European Surveillance of Antimicrobial Consumption (ESAC): Disease-specific quality indicators for outpatient antibiotic prescribing. BMJ Qual. Saf. 2011, 20, 764–772. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Antimicrobial Consumption in the EU/EEA (ESAC-Net)—Annual Epidemiological Report for 2021; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2022; Available online: https://www.ecdc.europa.eu/en/publications-data/downloadable-tables-antimicrobial-consumption-annual-epidemiological-report-2021 (accessed on 28 February 2023).
- Altiner, A.; Knauf, A.; Moebes, J.; Sielk, M.; Wilm, S. Acute cough: A qualitative analysis of how GPs manage the consultation when patients explicitly or implicitly expect antibiotic prescriptions. Fam. Pract. 2004, 21, 500–506. [Google Scholar] [CrossRef] [PubMed]
- Tonkin-Crine, S.K.; Tan, P.S.; van Hecke, O.; Wang, K.; Roberts, N.W.; McCullough, A.; Hansen, M.P.; Butler, C.C.; Del Mar, C.B. Clinician-targeted interventions to influence antibiotic prescribing behaviour for acute respiratory infections in primary care: An overview of systematic reviews. Cochrane Database Syst. Rev. 2017, 9, CD012252. [Google Scholar] [CrossRef] [PubMed]
- Stuart, B.; Hounkpatin, H.; Becque, T.; Yao, G.; Zhu, S.; Alonso-Coello, P.; Altiner, A.; Arroll, B.; Böhning, D.; Bostock, J.; et al. Delayed antibiotic prescribing for respiratory tract infections: Individual patient data meta-analysis. BMJ 2021, 373, n808. [Google Scholar] [CrossRef] [PubMed]
- Arnold, S.R.; Straus, S.E. Interventions to improve antibiotic prescribing practices in ambulatory care. Cochrane Database Syst. Rev. 2005, 2005, CD003539. [Google Scholar] [CrossRef] [PubMed]
- Köchling, A.; Löffler, C.; Reinsch, S.; Hornung, A.; Böhmer, F.; Altiner, A.; Chenot, J.F. Reduction of antibiotic prescriptions for acute respiratory tract infections in primary care: A systematic review. Implement. Sci. 2018, 13, 47. [Google Scholar] [CrossRef] [PubMed]
- Spurling, G.K.; Del Mar, C.B.; Dooley, L.; Foxlee, R.; Farley, R. Delayed antibiotic prescriptions for respiratory infections. Cochrane Database Syst. Rev. 2017, 9, CD004417. [Google Scholar] [PubMed]
- Poss-Doering, R.; Kronsteiner, D.; Kamradt, M.; Kaufmann-Kolle, P.; Andres, E.; Wambach, V.; Bleek, J.; Wensing, M.; Szecsenyi, J.; ARena-Study Group. Assessing Reduction of Antibiotic Prescribing for Acute, Non-Complicated Infections in Primary Care in Germany: Multi-Step Outcome Evaluation in the Cluster-Randomized Trial ARena. Antibiotics 2021, 10, 1151. [Google Scholar] [CrossRef] [PubMed]
- Wensing, M.; Broge, B.; Riens, B.; Kaufmann-Kolle, P.; Akkermans, R.; Grol, R.; Szecsenyi, J. Quality circles to improve prescribing of primary care physicians. Three comparative studies. Pharmacoepidemiol. Drug Saf. 2009, 18, 763–769. [Google Scholar] [CrossRef] [PubMed]
- Coxeter, P.; Del Mar, C.B.; McGregor, L.; Beller, E.M.; Hoffmann, T.C. Interventions to facilitate shared decision making to address antibiotic use for acute respiratory infections in primary care. Cochrane Database Syst. Rev. 2015, 11, CD010907. [Google Scholar] [CrossRef] [PubMed]
- Hallsworth, M.; Chadborn, T.; Sallis, A.; Sanders, M.; Berry, D.; Greaves, F.; Clements, L.; Davies, S.C. Provision of social norm feedback to high prescribers of antibiotics in general practice: A pragmatic national randomised controlled trial. Lancet 2016, 387, 1743–1752. [Google Scholar] [CrossRef] [PubMed]
- Meeker, D.; Linder, J.A.; Fox, C.R.; Friedberg, M.W.; Persell, S.D.; Goldstein, N.J.; Knight, T.K.; Hay, J.W.; Doctor, J.N. Effect of Behavioral Interventions on Inappropriate Antibiotic Prescribing Among Primary Care Practices: A Randomized Clinical Trial. JAMA 2016, 315, 562–570. [Google Scholar] [CrossRef] [PubMed]
- Freund, T.; Peters-Klimm, F.; Boyd, C.M.; Mahler, C.; Gensichen, J.; Erler, A.; Beyer, M.; Gondan, M.; Rochon, J.; Gerlach, F.M.; et al. Medical Assistant-Based Care Management for High-Risk Patients in Small Primary Care Practices: A Cluster Randomized Clinical Trial. Ann. Intern. Med. 2016, 164, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Altiner, A.; Brockmann, S.; Sielk, M.; Wilm, S.; Wegscheider, K.; Abholz, H.H. Reducing antibiotic prescriptions for acute cough by motivating GPs to change their attitudes to communication and empowering patients: A cluster-randomized intervention study. J. Antimicrob. Chemother. 2007, 60, 638–644. [Google Scholar] [CrossRef] [PubMed]
- Poß- Doering, R.; Kuehn, L.; Kamradt, M.; Glassen, K.; Fleischhauer, T.; Kaufmann-Kolle, P.; Koeppen, M.; Wollny, A.; Altiner, A.; Wensing, M. Converting habits of antibiotic use for respiratory tract infections in German primary care (CHANGE-3)—Process evaluation of a complex intervention. BMC Fam. Pract. 2020, 21, 274. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Group | Intervention | Control | ||||||
|---|---|---|---|---|---|---|---|---|
| Time | T0 | T1 | T2 | T3 | T0 | T1 | T2 | T3 |
| Cases | n = 6481 (%) | n = 7269 | n = 6889 | n = 6769 | n = 8903 | n = 9298 | n = 7820 | n = 7961 |
| Cases from BW versus MV | 4601 (71.0) | 4999 (68.8) | 4883 (70.9) | 4702 (69.5) | 6483 (72.8) | 6476 (69.6) | 5397 (69.0) | 5550 (69.7) |
| Age (patients) | ||||||||
| 622 (9.6) | 696 (9.6) | 652 (9.5) | 631 (9.3) | 901 (10.1) | 974 (10.5) | 893 (11.4) | 857 (10.8) |
| 5121 (79.0) | 5827 (80.2) | 5593 (81.2) | 5562 (82.2) | 7158 (80.4) | 7479 (80.4) | 6315 (80.8) | 6529 (82.0) |
| 738 (11.4) | 746 (10.3) | 644 (9.3) | 576 (8.5) | 844 (9.5) | 845 (9.1) | 612 (7.8) | 575 (7.2) |
| Female (versus male patients) | 3449 (53.2) | 3860 (53.1) | 3617 (52.5) | 3609 (53.3) | 4734 (53.2) | 4860 (52.3) | 4070 (52.0) | 4134 (51.9) |
| Number of hierarchised morbidity groups | ||||||||
| 3245 (50.1) | 3658 (50.3) | 3590 (52.1) | 3548 (52.4) | 4625 (51.9) | 4968 (53.4) | 4373 (55.9) | 4561 (57.3) |
| 1901 (29.3) | 2196 (30.2) | 1964 (28.5) | 1999 (29.5) | 2664 (29.9) | 2696 (29.0) | 2209 (28.2) | 2239 (28.1) |
| 789 (12.2) | 836 (11.5) | 755 (11.0) | 703 (10.4) | 931 (10.5) | 918 (9.9) | 707 (9.0) | 682 (8.6) |
| 546 (8.4) | 579 (8.0) | 580 (8.4) | 519 (7.7) | 683 (7.7) | 716 (7.7) | 531 (6.8) | 479 (6.0) |
| Disease | ||||||||
| 4837 (74.6) | 5637 (77.5) | 5363 (77.8) | 5438 (80.3) | 6881 (77.3) | 7630 (82.1) | 6321 (80.8) | 6580 (82.7) |
| 1435 (22.1) | 1381 (19.0) | 1229 (17.8) | 1133 (16.7) | 2002 (22.5) | 1902 (20.5) | 1379 (17.6) | 1379 (17.3) |
| 357 (5.5) | 359 (4.9) | 393 (5.7) | 335 (4.9) | 381 (4.3) | 305 (3.3) | 326 (4.2) | 308 (3.9) |
| 203 (3.1) | 202 (2.8) | 200 (2.9) | 174 (2.6) | 662 (7.4) | 594 (6.4) | 602 (7.7) | 612 (7.7) |
| 344 (5.3) | 355 (4.9) | 338 (4.9) | 290 (4.3) | 328 (3.7) | 297 (3.2) | 281 (3.6) | 262 (3.3) |
| Antibiotic prescription | 1537 (23.7) | 1462 (20.1) | 1113 (16.2) | 1020 (15.1) | 1585 (17.8) | 1356 (14.6) | 1067 (13.6) | 991 (12.4) |
| One GP per practice (versus two or more) | 4319 (66.6) | 4388 (60.4) | 3941 (57.2) | 3735 (55.2) | 4748 (53.3) | 4887 (52.6) | 4148 (53.0) | 4149 (52.1) |
| Antibiotic Prescription | OR | 95% CI | p-Value |
|---|---|---|---|
| Over Time (intervention and control) | 0.836 | 0.809; 0.863 | <0.001 |
| Intervention versus control | 1.285 | 0.874; 1.889 | 0.202 |
| Female versus male | 1.279 | 1.213; 1.349 | <0.001 |
| Age < 18 versus 18–65 years | 0.808 | 0.733; 0.89 | <0.001 |
| Age > 65 versus 18–65 years | 1.813 | 1.666; 1.972 | <0.001 |
| Over time: Intervention versus control * | 0.958 | 0.915; 1.002 | 0.063 |
| Antibiotic Prescription | OR | 95% CI | p-Value |
|---|---|---|---|
| Over time (intervention and control) | 0.842 | 0.815; 0.87 | <0.001 |
| Intervention versus control | 1.253 | 0.859; 1.827 | 0.242 |
| Female versus male | 1.26 | 1.195; 1.329 | <0.001 |
| Age < 18 versus 18–65 years | 0.938 | 0.849; 1.035 | 0.204 |
| Age > 65 versus 18–65 years | 1.297 | 1.176; 1.429 | <0.001 |
| Number of hierarchised morbidity groups 1,2 versus 0 | 1.334 | 1.254; 1.419 | <0.001 |
| Number of hierarchised morbidity groups 3,4 versus 0 | 1.568 | 1.434; 1.715 | <0.001 |
| Number of hierarchised morbidity groups 5+ versus 0 | 2.046 | 1.835; 2.281 | <0.001 |
| Region Baden-Württemberg versus Mecklenburg-Western Pomerania | 1.044 | 0.72; 1.513 | 0.822 |
| Single versus group practice | 0.817 | 0.718; 0.929 | 0.002 |
| Over time: Intervention versus control * | 0.956 | 0.913; 1.001 | 0.053 |
| T0 | T1 | T2 | T3 | |
|---|---|---|---|---|
| Number of cases | (n = 1,042,485), (%) | (n = 1,069,389) | (n = 956,707) | (n = 1,002,417) |
| Patients from BW versus MV | 972,477 (93.3) | 994,223 (93.0) | 896,799 (93.7) | 946,273 (94.4) |
| Age groups of patients | ||||
| 97,516 (9.4) | 93,461 (8.7) | 83,313 (8.7) | 82,208 (8.2) |
| 855,942 (82.1) | 892,083 (83.4) | 805,367 (84.2) | 855,017 (85.3) |
| 89,027 (8.5) | 83,845 (7.8) | 68,027 (7.1) | 65,192 (6.5) |
| Female patients (versus male) | 546,166 (52.4) | 550,301 (51.5) | 488,030 (51.0) | 512,457 (51.1) |
| Number of hierarchised morbidity groups | ||||
| 566,854 (54.4) | 590,243 (55.2) | 537,484 (56.2) | 564,413 (56.3) |
| 311,461 (29.9) | 314,149 (29.4) | 276,237 (28.9) | 291,900 (29.1) |
| 103,293 (9.9) | 103,320 (9.7) | 89,231 (9.3) | 91,951 (9.2) |
| 60,877 (5.8) | 61,677 (5.8) | 53,755 (5.6) | 54,153 (5.4) |
| One GP per practice (versus two or more) | 564,936 (54.2) | 580,523 (54.3) | 519,485 (54.3) | 540,306 (53.9) |
| Disease (patients with diagnosis) | ||||
| 766,094 (73.5) | 809,997 (75.7) | 729,924 (76.3) | 783,362 (78.1) |
| 268,274 (25.7) | 258,468 (24.2) | 209,589 (21.9) | 206,242 (20.6) |
| 66,873 (6.4) | 63,712 (6.0) | 60,519 (6.3) | 59,158 (5.9) |
| 54,209 (5.2) | 47,136 (4.4) | 46,410 (4.9) | 40,756 (4.1) |
| 34,251 (3.3) | 33,619 (3.1) | 31,542 (3.3) | 30,432 (3.0) |
| Antibiotic prescription | 267,885 (25.7) | 259,890 (24.3) | 213,161 (22.3) | 201,495 (20.1) |
| Antibiotic Prescription | OR | 95% CI | p-Value |
|---|---|---|---|
| Time | 0.903 | 0.901; 0.905 | <0.001 |
| cRCT control versus care as usual | 0.634 | 0.489; 0.821 | 0.001 |
| cRCT intervention versus care as usual | 0.768 | 0.589; 1.002 | 0.052 |
| Female versus male | 1.241 | 1.235; 1.247 | <0.001 |
| Age < 18 versus 18–65 | 0.929 | 0.92; 0.937 | <0.001 |
| Age > 65 versus 18–65 | 1.24 | 1.228; 1.252 | <0.001 |
| Number of hierarchised morbidity groups 1,2 versus 0 | 1.251 | 1.244; 1.258 | <0.001 |
| Number of hierarchised morbidity groups 3,4 versus 0 | 1.57 | 1.556; 1.583 | <0.001 |
| Number of hierarchised morbidity groups 5+ vsersus 0 | 1.739 | 1.719; 1.759 | <0.001 |
| BW versus MV | 0.797 | 0.746; 0.852 | <0.001 |
| Single versus group practice | 0.831 | 0.82; 0.843 | <0.001 |
| Time: Intervention group versus care as usual * | 0.946 | 0.918; 0.974 | <0.001 |
| Time: Control group versus care as usual * | 0.913 | 0.886; 0.94 | <0.001 |
| Infections | ICD-10 |
|---|---|
| Acute bronchitis | J20 |
| Acute bronchitis | J21.0 |
| Acute bronchitis | J21.1 |
| Acute bronchitis | J21.8 |
| Acute bronchitis | J21.9 |
| Acute bronchitis | J22 |
| Acute bronchitis | J40 |
| Acute upper respiratory tract infection | J00 |
| Acute upper respiratory tract infection | J02.0 |
| Acute upper respiratory tract infection | J02.8 |
| Acute upper respiratory tract infection | J02.9 |
| Acute upper respiratory tract infection | J04 |
| Acute upper respiratory tract infection | J06 |
| Acute upper respiratory tract infection | J10.1 |
| Acute upper respiratory tract infection | J11.1 |
| Sinusitis | J01 |
| Tonsillitis | J03.0 |
| Otitis media | H65.0 |
| Otitis media | H65.1 |
| Otitis media | H65.9 |
| Otitis media | H66.0 |
| Otitis media | H66.4 |
| Otitis media | H66.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feldmeier, G.; Löffler, C.; Altiner, A.; Wollny, A.; Garbe, K.; Kronsteiner, D.; Köppen, M.; Szecsenyi, J.; Leyh, M.; Voss, A.; et al. Optimizing Antibiotic Prescribing for Acute Respiratory Tract Infections in German Primary Care: Results of the Regional Intervention Study CHANGE-3 and the Nested cRCT. Antibiotics 2023, 12, 850. https://doi.org/10.3390/antibiotics12050850
Feldmeier G, Löffler C, Altiner A, Wollny A, Garbe K, Kronsteiner D, Köppen M, Szecsenyi J, Leyh M, Voss A, et al. Optimizing Antibiotic Prescribing for Acute Respiratory Tract Infections in German Primary Care: Results of the Regional Intervention Study CHANGE-3 and the Nested cRCT. Antibiotics. 2023; 12(5):850. https://doi.org/10.3390/antibiotics12050850
Chicago/Turabian StyleFeldmeier, Gregor, Christin Löffler, Attila Altiner, Anja Wollny, Katharina Garbe, Dorothea Kronsteiner, Martina Köppen, Joachim Szecsenyi, Mirko Leyh, Arwed Voss, and et al. 2023. "Optimizing Antibiotic Prescribing for Acute Respiratory Tract Infections in German Primary Care: Results of the Regional Intervention Study CHANGE-3 and the Nested cRCT" Antibiotics 12, no. 5: 850. https://doi.org/10.3390/antibiotics12050850
APA StyleFeldmeier, G., Löffler, C., Altiner, A., Wollny, A., Garbe, K., Kronsteiner, D., Köppen, M., Szecsenyi, J., Leyh, M., Voss, A., Kamradt, M., Poß-Doering, R., Wensing, M., & Kaufmann-Kolle, P. (2023). Optimizing Antibiotic Prescribing for Acute Respiratory Tract Infections in German Primary Care: Results of the Regional Intervention Study CHANGE-3 and the Nested cRCT. Antibiotics, 12(5), 850. https://doi.org/10.3390/antibiotics12050850