



The National Implementation of a Community Pharmacy Antimicrobial Stewardship Intervention (PAMSI) through the English Pharmacy Quality Scheme 2020 to 2022

 , ,
, ,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting and Participants
2.3. Data Collection
2.3.1. As Part of the PQS 2020/21
2.3.2. As Part of the PQS 2021/22
2.3.3. A Follow-Up Questionnaire after Completing PQS 2021/22
2.4. Data Analysis
2.5. Ethics
3. Results
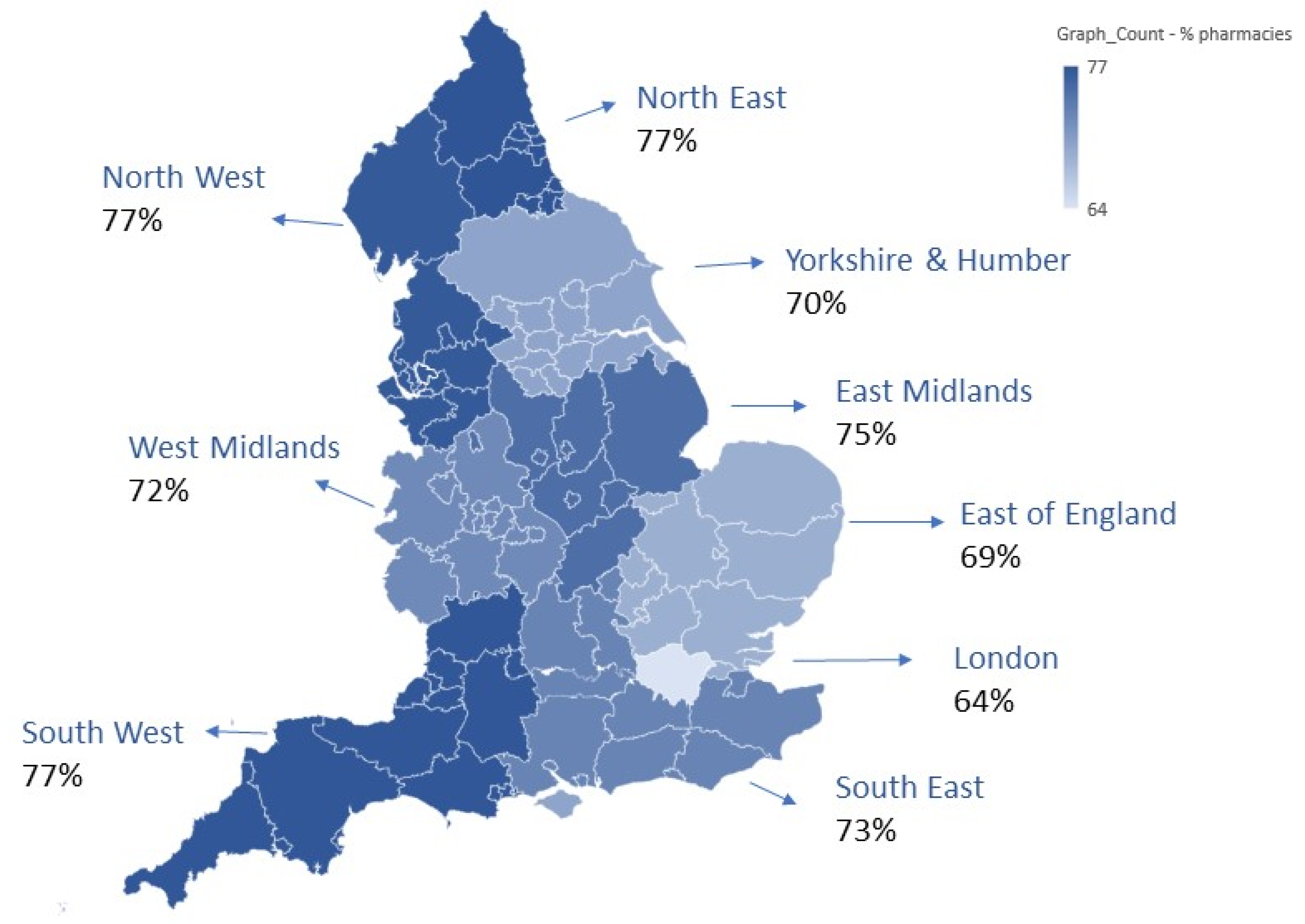
3.1. PQS 2020/21 Implementation of AMS E-Learning Module and Antibiotic Guardian Pledge
3.2. PQS 2021/22 Implementation of TARGET Antibiotic Checklist
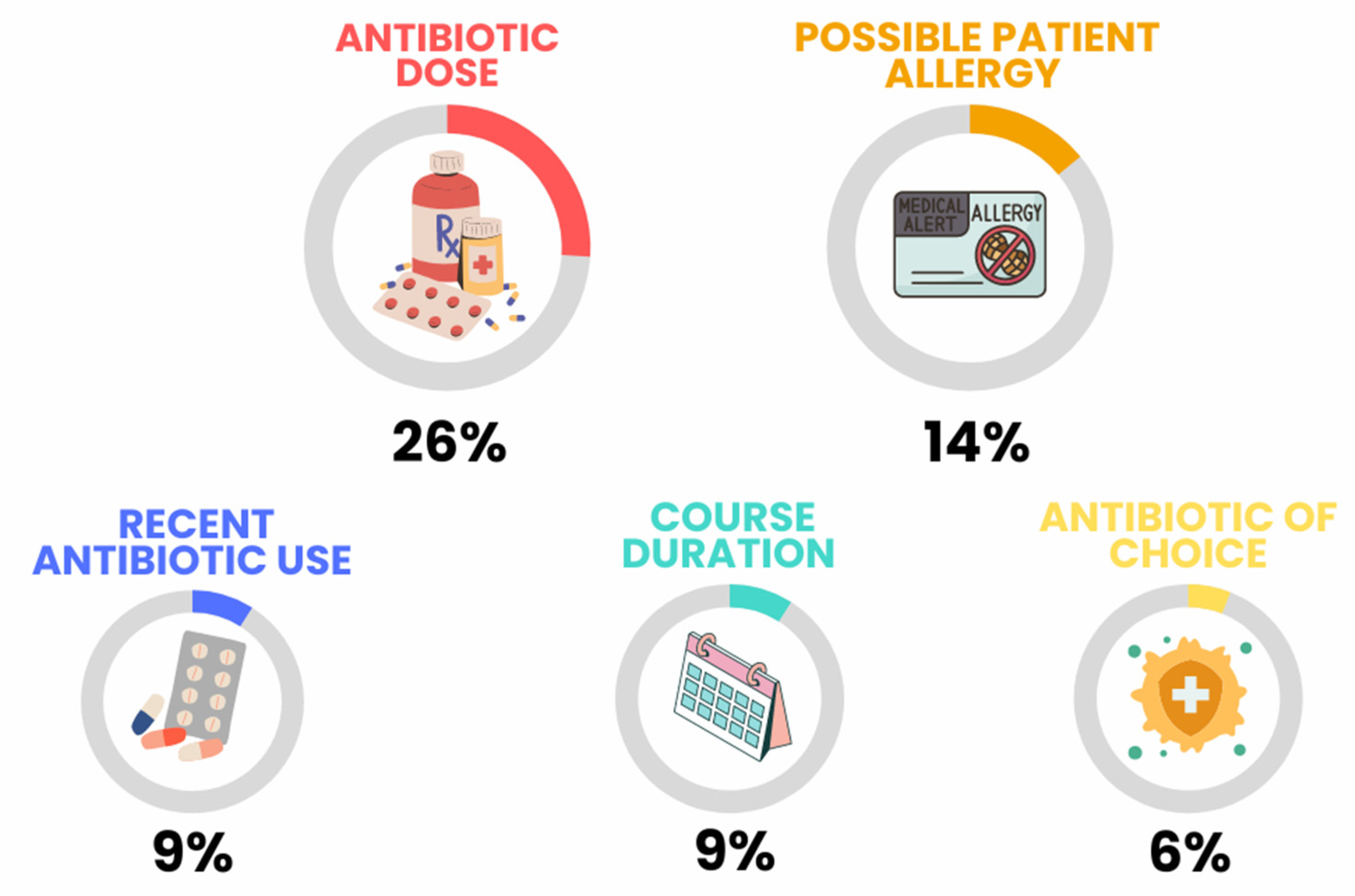
3.2.1. Pharmacy Team Antibiotic Checks
3.2.2. Interventions by Community Pharmacy Teams
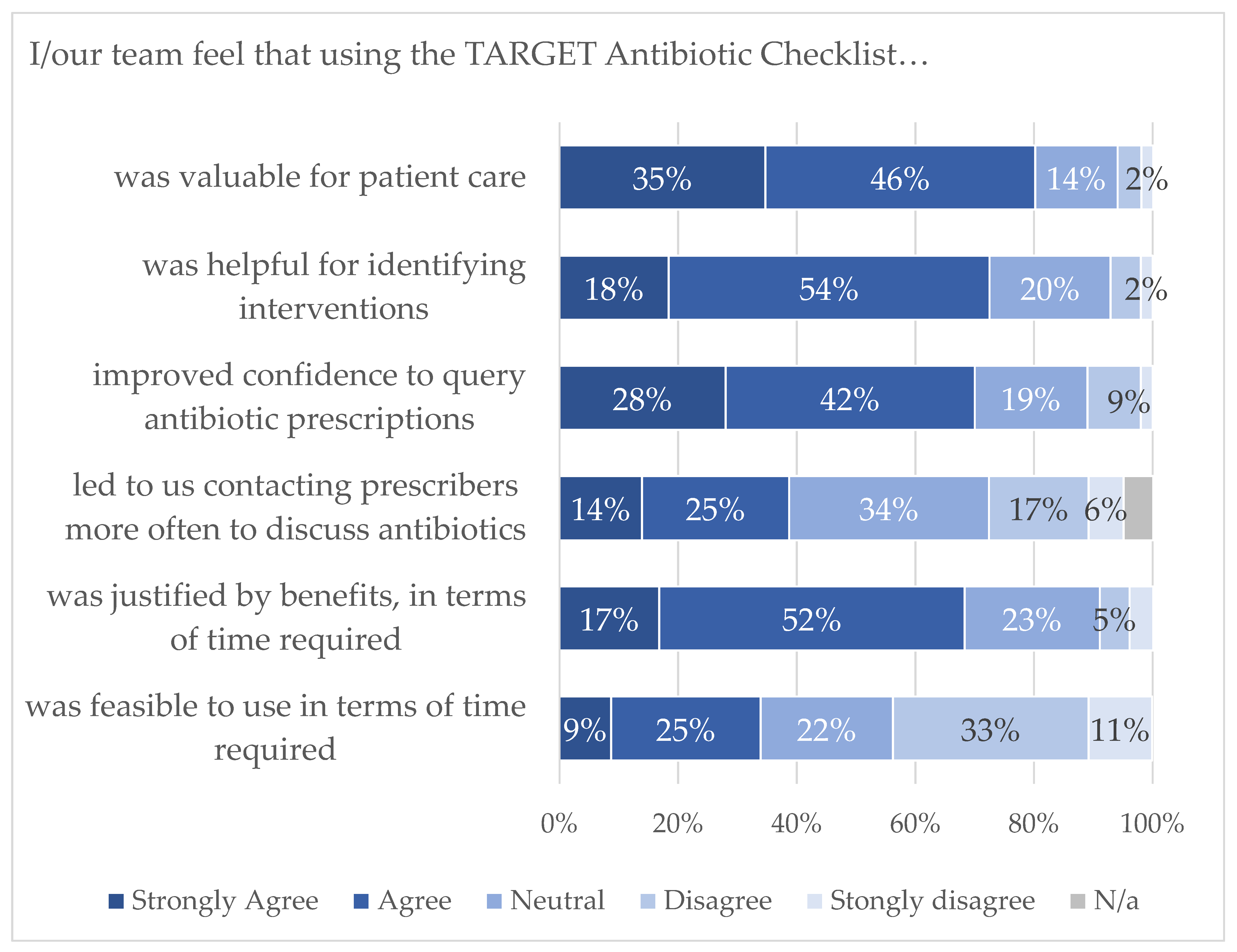
3.2.3. Pharmacy Staff Follow-Up Questionnaire
“The aim is laudable, but this was a PQS hoop-jumping exercise. You’re targeting the wrong people, pharmacies are happy to help patients get best use out of the antibiotics they have been prescribed, but the real levers for change are in the hands of the GPs. We don’t have the time, staff or authority to makes a significant impact”
“It is really valuable and important but like every part of community pharmacy, every resource is stretched. We are constantly just trying to keep the essentials done”
“can’t get to speak to them in a reasonable time when patients waiting to take script”
“Hard to get a phone back from prescriber and met with stubborn/rude response”
“Although all patients agree that antibiotics should be used appropriately—each individual is not keen to wait and see and prefers to use antibiotics in case they get worse and have to take time out of life to get well”
4. Discussion
4.1. Summary
4.2. Comparison with the Literature
4.3. Strengths and Limitations
4.4. Implications and Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Department of Health and Social Care. UK AMR 5 Year National Action Plan; Department of Health and Social Care: London, UK, 2019. [Google Scholar]
- Department of Health and Social Care. The UK’s 20-Year Vision for Antimicrobial Resistance; Department of Health and Social Care: London, UK, 2019. [Google Scholar]
- National Institute for Health and Care Excellence. Antimicrobial Stewardship: Systems and Processes for Effective Antimicrobial Medicine Use; National Institute for Health and Care Excellence: London, UK, 2015. [Google Scholar]
- UK Health Security Agency. English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR) Report 2021 to 2022; UK Health Security Agency, Ed.; UK Health Security Agency: London, UK, 2022. [Google Scholar]
- Res, R.; Hoti, K.; Charrois, T.L. Pharmacists’ perceptions regarding optimization of antibiotic prescribing in the community. J. Pharm. Pract. 2017, 30, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Tonna, A.P.; Weidmann, A.E.; Sneddon, J.; Stewart, D. Views and experiences of community pharmacy team members on antimicrobial stewardship activities in Scotland: A qualitative study. Int. J. Clin. Pharm. 2020, 42, 1261–1269. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.F.; Owens, R.; Sallis, A.; Ashiru-Oredope, D.; Thornley, T.; Francis, N.A.; Butler, C.; McNulty, C. Qualitative study using interviews and focus groups to explore the current and potential for antimicrobial stewardship in community pharmacy informed by the Theoretical Domains Framework. BMJ Open 2018, 8, e025101. [Google Scholar] [CrossRef] [PubMed]
- Saha, S.K.; Kong, D.C.M.; Thursky, K.; Mazza, D. Antimicrobial stewardship by Australian community pharmacists: Uptake, collaboration, challenges, and needs. J. Am. Pharm. Assoc. JAPhA 2021, 61, 158–168.e7. [Google Scholar] [CrossRef] [PubMed]
- Allison, R.; Chapman, S.; Howard, P.; Thornley, T.; Ashiru-Oredope, D.; Walker, S.; Jones, L.F.; McNulty, C.A.M. Feasibility of a community pharmacy antimicrobial stewardship intervention (PAMSI): An innovative approach to improve patients’ understanding of their antibiotics. JAC-Antimicrob. Resist. 2020, 2, 4. [Google Scholar] [CrossRef] [PubMed]
- Hayes, C.V.; Lecky, D.M.; Pursey, F.; Thomas, A.; Ashiru-Oredope, D.; Saei, A.; Thornley, T.; Howard, P.; Dickinson, A.; Ingram, C.; et al. Mixed-Method Evaluation of a Community Pharmacy Antimicrobial Stewardship Intervention (PAMSI). Healthcare 2022, 10, 1288. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [PubMed]
- Royal College of General Practitioners. TARGET Antibiotic Checklist. 2023. Available online: https://elearning.rcgp.org.uk/mod/book/view.php?id=13511&chapterid=784 (accessed on 31 January 2023).
- Antimicrobial Stewardship for Community Pharmacy Staff e-Learning. 2020. Available online: https://www.e-lfh.org.uk/programmes/antimicrobial-resistance-and-infections/ (accessed on 7 December 2022).
- UK Health Security Agency. Antibiotic Guardian. 2023. Available online: https://antibioticguardian.com/ (accessed on 31 January 2023).
- Royal College of General Practitioners. TARGET Antibiotics Toolkit Hub. 2023. Available online: https://elearning.rcgp.org.uk/course/view.php?id=553 (accessed on 7 December 2022).
- Department of Health and Social Care; NHS England and NHS Improvement; Pharmaceutical Services Negotiating Committee (PSNC). The Community Pharmacy Contractual Framework for 2019/20 to 2023/24: Supporting Delivery for the NHS Long Term Plan. 2019. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/819601/cpcf-2019-to-2024.pdf (accessed on 7 December 2022).
- NHS. The NHS Long Term Plan; NHS: London, UK, 2019. [Google Scholar]
- Pharmaceutical Services Negotiating Committee. Pharmacy Quality Scheme. 2022. Available online: https://psnc.org.uk/quality-and-regulations/pharmacy-quality-scheme/ (accessed on 25 October 2022).
- Parekh, S.; Hayes, C.V.; Loader, J.; Ashiru-Oredope, D.; Hand, K.; Hicks, G.; Lecky, D. The Use of the TARGET Antibiotic Checklist to support Antimicrobial Stewardship, in England community pharmacies through the Pharmacy Quality Scheme. Antibiotics 2023, 12, 647. [Google Scholar] [CrossRef]
- NHS England. Pharmacy Quality Scheme (PQS) 2021/22 Announcement; NHS: London, UK, 2021. [Google Scholar]
- NHS Health Research Authority. Is My Study Research? 2023. Available online: https://www.hra-decisiontools.org.uk/research/ (accessed on 16 March 2023).
- General Pharmaceutical Council. The GPhC Register as of 31 May 2022—Trend data. 2023. Available online: https://www.pharmacyregulation.org/ (accessed on 25 October 2022).
- National Institute for Health and Care Excellence. Sore Throat (Acute): Antimicrobial Prescribing; National Institute for Health and Care Excellence: London, UK, 2018. [Google Scholar]
- National Institute for Health and Care Excellence, Urinary Tract Infection (Lower): Antimicrobial Prescribing. NICE Guideline NG109; National Institute for Health and Care Excellence: London, UK, 2018. [Google Scholar]
- Budd, E.; Cramp, E.; Sharland, M.; Hand, K.; Howard, P.; Wilson, P.; Wilcox, M.; Muller-Pebody, B.; Hopkins, S. Adaptation of the WHO Essential Medicines List for national antibiotic stewardship policy in England: Being AWaRe. J. Antimicrob. Chemother. 2019, 74, 3384–3389. [Google Scholar] [CrossRef] [PubMed]
- Durand, C.; Douriez, E.; Chappuis, A.; Poulain, F.; Yazdanpanah, Y.; Lariven, S.; Lescure, F.-X.; Peiffer-Smadja, N. Contributions and challenges of community pharmacists during the COVID-19 pandemic: A qualitative study. J. Pharm. Policy Pract. 2022, 15, 43. [Google Scholar] [CrossRef] [PubMed]
- Seaton, D.; Ashiru-Oredope, D.; Charlesworth, J.; Gemmell, I.; Harrison, R. Evaluating UK Pharmacy Workers’ Knowledge, Attitudes and Behaviour towards Antimicrobial Stewardship and Assessing the Impact of Training in Community Pharmacy. Pharmacy 2022, 10, 98. [Google Scholar] [CrossRef] [PubMed]
- Durand, C.; Chappuis, A.; Douriez, E.; Poulain, F.; Ahmad, R.; Lescure, F.-X.; Peiffer-Smadja, N. Perceptions, current practices, and interventions of community pharmacists regarding antimicrobial stewardship: A qualitative study. J. Am. Pharm. Assoc. 2022, 62, 1239–1248.e1. [Google Scholar] [CrossRef] [PubMed]
- Wilcock, M.; Wisner, K.; Lee, F. Community pharmacists and antimicrobial stewardship—What is their role. J. Med. Optim. 2017, 3, 47–50. [Google Scholar]
- Clifford, E.D.S.; Mills, J.; Yazdani, B.; Hawksworth, G.; Howard, P. The Role of Community Pharmacists in Delivering the 5-Year Antimicrobial Resistance Strategy; UK Clinical Pharmacy Association: London, UK, 2016. [Google Scholar]
- Krishna, M.T.; Huissoon, A.P.; Li, M.; Richter, A.; Pillay, D.G.; Sambanthan, D.; Raman, S.C.; Nasser, S.; Misbah, S.A. Enhancing antibiotic stewardship by tackling “spurious” penicillin allergy. Clin. Exp. Allergy 2017, 47, 1362–1373. [Google Scholar] [CrossRef] [PubMed]
- Saha, S.K.; Hawes, L.; Mazza, D. Effectiveness of interventions involving pharmacists on antibiotic prescribing by general practitioners: A systematic review and meta-analysis. J. Antimicrob. Chemother. 2019, 74, 1173–1181. [Google Scholar] [CrossRef] [PubMed]
- Courtenay, M.; Lim, R.; Castro-Sanchez, E.; Deslandes, R.; Hodson, K.; Morris, G.; Reeves, S.; Weiss, M.; Ashiru-Oredope, D.; Bain, H.; et al. Development of consensus-based national antimicrobial stewardship competencies for UK undergraduate healthcare professional education. J. Hosp. Infect. 2018, 100, 245–256. [Google Scholar] [CrossRef] [PubMed]
- Paudyal, V.; Cadogan, C.; Fialová, D.; Henman, M.C.; Hazen, A.; Okuyan, B.; Lutters, M.; Stewart, D. Provision of clinical pharmacy services during the COVID-19 pandemic: Experiences of pharmacists from 16 European countries. Res. Soc. Adm. Pharm. 2020, 17, 1507–1517. [Google Scholar] [CrossRef] [PubMed]
- Royal College of General Practitioners. UTI Women under 65 Leaflet for Community Pharmacies. 2023. Available online: https://elearning.rcgp.org.uk/mod/book/view.php?id=13511&chapterid=786 (accessed on 31 January 2023).
- Royal College of General Practitioners. RTI Leaflet for Community Pharmacies. 2023. Available online: https://elearning.rcgp.org.uk/mod/book/view.php?id=13511&chapterid=787 (accessed on 31 January 2023).
- Department of Health and Social Care. Community Pharmacy Contractual Framework 5-Year Deal: Year 4 (2022 to 2023) and Year 5 (2023 to 2024); Department of Health and Social Care: London, UK, 2022. [Google Scholar]
- International Pharmaceutical Federation. FIP Primary Health Care World Ma2023. Available online: https://primaryhealthcare.fip.org/worldmap/ (accessed on 5 March 2023).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | Total |
|---|---|---|---|---|---|---|---|
| 8259 | 1983 | 2687 | 1536 | 2211 | 28,369 | 27,334 | 72,379 |
| Total number of Antibiotic Checklists Submitted | 213,105 | ||
|---|---|---|---|
| Number of Pharmacies Who Submitted Antibiotic Checklists | 8374 | ||
| Range of Antibiotic Checklists Submitted Per Pharmacy | 1–181 | ||
| Completion of Criteria | Number | Percentage of Submitting Pharmacies (n = 8374) | Percentage of Total Pharmacies in England (n = 11,232) |
| Pharmacies who completed at least 25 Antibiotic Checklists | 7225 | 86% | 64% |
| Pharmacies who completed more than 25 Antibiotic Checklists | 3653 | 44% | 32% |
| Pharmacies who completed fewer than 25 Antibiotic Checklists | 1149 | 14% | 10% |
| Antibiotic | Allergy Detected | Antibiotic Changed or Not Dispensed Due to Allergy | Medicine Interaction | Strength, Dose, Duration, Quantity, Formulation | Multiple Antibiotics Prescribed | Choice of Antibiotic for Indication | Recent Antibiotic Use | Long Term Use, Prophylaxis, Rescue Pack | Possible Unnecessary Antibiotic | Pregnancy, Breast Feeding, Kidney Issue | Patient Factors (Adverse Reaction, Preference) | Safety-Netting/ Referral | Other Reason 1 | Unknown Reason | Grand Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Amoxicillin | 40 | 6 | 7 | 237 | 13 | 31 | 36 | 14 | 7 | 4 | 7 | 5 | 16 | 351 | 774 |
| Nitrofurantoin | 4 | 4 | 2 | 139 | 11 | 8 | 41 | 5 | 1 | 22 | 2 | 6 | 5 | 143 | 393 |
| Clarithromycin | 4 | 48 | 29 | 71 | 5 | 8 | 9 | 3 | 1 | 6 | 3 | - | 6 | 74 | 267 |
| Flucloxacillin | 16 | 4 | 3 | 55 | 9 | 15 | 10 | 4 | 2 | 4 | - | 6 | 2 | 105 | 235 |
| Doxycycline | 3 | 21 | 6 | 60 | 5 | 18 | 18 | 7 | 2 | 5 | 3 | - | 2 | 94 | 244 |
| Penicillin V | 9 | 6 | 1 | 85 | 6 | 13 | 10 | - | 2 | 4 | - | - | - | 63 | 199 |
| Metronidazole | 4 | 6 | 1 | 50 | 6 | 7 | 3 | 1 | - | 5 | 1 | - | 13 | 56 | 153 |
| Trimethoprim | 3 | 3 | 2 | 37 | 8 | 11 | 12 | 3 | - | 11 | 2 | - | 2 | 44 | 138 |
| Co-amoxiclav | 10 | 4 | 1 | 25 | 6 | 8 | 2 | 2 | 1 | - | 3 | - | - | 25 | 87 |
| Cefalexin | - | 9 | 1 | 8 | 2 | 4 | 2 | 3 | - | 4 | 1 | - | - | 9 | 43 |
| Erythromycin | 1 | 8 | 4 | 13 | 2 | 3 | - | 1 | - | 3 | 1 | - | - | 7 | 43 |
| Ciprofloxacin | - | 2 | 2 | 8 | 2 | 8 | 4 | 2 | - | 1 | - | 1 | - | 6 | 36 |
| Clindamycin | - | - | - | 12 | - | - | - | - | - | - | 1 | - | - | - | 13 |
| Pivmecillinam | - | 1 | - | 8 | 3 | 1 | 2 | - | - | 1 | - | - | 2 | 3 | 21 |
| Azithromycin | - | - | - | 9 | - | 2 | - | 2 | - | - | - | - | - | 1 | 14 |
| Antibiotic was not dispensed | - | 20 | - | 8 | - | - | 1 | 1 | 6 | 2 | 1 | - | - | 16 | 55 |
| Unknown antibiotic | 2 | 3 | 1 | 4 | - | 3 | - | 1 | - | 1 | 1 | - | 2 | 36 | 54 |
| Other antibiotic 2 | - | 1 | 3 | 16 | 1 | 4 | 1 | 4 | - | 1 | - | - | 1 | 18 | 50 |
| Grand Total | 96 | 146 | 63 | 845 | 79 | 144 | 151 | 53 | 22 | 74 | 26 | 18 | 51 | 1051 | 2819 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hayes, C.V.; Parekh, S.; Lecky, D.M.; Loader, J.; Triggs-Hodge, C.; Ashiru-Oredope, D. The National Implementation of a Community Pharmacy Antimicrobial Stewardship Intervention (PAMSI) through the English Pharmacy Quality Scheme 2020 to 2022. Antibiotics 2023, 12, 793. https://doi.org/10.3390/antibiotics12040793
Hayes CV, Parekh S, Lecky DM, Loader J, Triggs-Hodge C, Ashiru-Oredope D. The National Implementation of a Community Pharmacy Antimicrobial Stewardship Intervention (PAMSI) through the English Pharmacy Quality Scheme 2020 to 2022. Antibiotics. 2023; 12(4):793. https://doi.org/10.3390/antibiotics12040793
Chicago/Turabian StyleHayes, Catherine V., Sejal Parekh, Donna M. Lecky, Jill Loader, Carry Triggs-Hodge, and Diane Ashiru-Oredope. 2023. "The National Implementation of a Community Pharmacy Antimicrobial Stewardship Intervention (PAMSI) through the English Pharmacy Quality Scheme 2020 to 2022" Antibiotics 12, no. 4: 793. https://doi.org/10.3390/antibiotics12040793
APA StyleHayes, C. V., Parekh, S., Lecky, D. M., Loader, J., Triggs-Hodge, C., & Ashiru-Oredope, D. (2023). The National Implementation of a Community Pharmacy Antimicrobial Stewardship Intervention (PAMSI) through the English Pharmacy Quality Scheme 2020 to 2022. Antibiotics, 12(4), 793. https://doi.org/10.3390/antibiotics12040793