Abstract
Antimicrobial resistance is a huge threat against the public health sphere and is a major cause of global mortality and morbidity. Antibiotic misuse and overuse have led to the development of many resistant bacterial strains. One particular bacterium of concern is methicillin-resistant Staphylococcus aureus (MRSA), which is the most common resistant bacteria in humans. Antibiotic development has been unable to keep up with the rapid evolution of antibiotic-resistant organisms, and there is an urgent need to identify alternative agents to combat this problem. The purpose of this systematic review is to explore the literature on the antibacterial properties of Eucalyptus globulus essential oil against MRSA. The articles used in this review were obtained through a systematic search of the literature across four databases, with the timeline being between 2002 and 2022. Twenty studies were included in this review, which used various methods to investigate the antibacterial properties of E. globulus essential oil, alone or in combination with other agents, against MRSA. The findings suggest that E. globulus essential oil has antibacterial properties against MRSA, which can be enhanced when used in combination with other agents, such as other essential oils and antibiotics.
1. Introduction
Antibiotic resistance is a phenomenon in which bacteria are able to evade antibiotics via various mechanisms, including neutralisation of the drug, excreting the drug, modifying structural components to prevent the drug from acting on the cell and DNA transfer between bacteria [1,2]. Drivers of this resistance include overuse and misuse of antibiotics in clinical and agricultural settings [1,3]. When antibiotics are used, they act on drug-sensitive bacteria, eradicating them and leaving behind resistant bacteria, which reproduce and proliferate [3]. Since the advent of modern antibiotics in the 1940s, bacteria have developed resistance to almost all available antibiotics and pose a huge threat to public health [3]. It is a major cause of global mortality and is classified by the World Health Organisation (WHO) as being in the top ten threats to global health [4].
Methicillin-resistant Staphylococcus aureus (MRSA) was first described in 1961 and, since then, it has become the most common resistant strain of bacteria in healthcare [2,5]. MRSA causes a wide range of infections, with the most common sites being the skin and subcutaneous tissue, followed by sites, including, but not limited to, the meninges, endocardium and bone [5,6].
The first three decades of MRSA cases were predominantly in those who had contact with hospitals, but in the 1990s, infections began to emerge in community settings in those that had no healthcare contact, presenting a major problem to the public health sphere. Management of MRSA depends on the specific disease and involves strict infection prevention methods and antibiotic administration. In the hospital setting, intravenous vancomycin is often the drug of choice, with daptomycin being a suitable alternative. However, cases of vancomycin-resistant Staphylococcus aureus have also emerged, complicating the situation even further [5].
The discovery of new antibiotics has not been able to keep up with the emergence of these resistant strains, highlighting the need to urgently find alternatives to antibiotics [7]. One such alternative is essential oils. Essential oils are complex mixtures, generally composed of over 20 different compounds. Over 3000 essential oils have been identified and each is composed of varying compounds and quantities. They have been used for centuries in traditional medicine to treat various conditions, from cuts and wounds to coughs and colds. Many essential oils possess antibacterial qualities that can be, in part, attributed to the low molecular weight of their active compounds and their lipophilic nature, enabling them to cross cell membranes and have cytotoxic effects [8]. The mechanism of action of essential oils differs from the mechanism of antibiotics, in that it inhibits various physiological and structural components rather than a single target like antibiotics. Examples of targets include inhibition of cell membranes, efflux pumps, biofilm and motility. The combination of various mechanisms complements one another, leading to a greater inhibition of bacterial growth compared to traditional antibiotics. This highlights their potential as alternative agents to antibiotics [9]. Additionally, evidence exists to demonstrate that antibacterial properties of essential oils can be enhanced when they are used in combination with other agents, such as essential oils and antibiotics [10].
Eucalyptus globulus is a plant that belongs to the Myrtaceae family. The essential oil derived from this plant is used widely around the world for many purposes, such as for pharmaceuticals, perfumes, food products and cosmetics. The oil has been shown to possess antibacterial, anti-inflammatory and antioxidant properties [11]. It has antibacterial effects against a broad range of microorganisms and, though the exact mechanism of action is unknown, multiple factors have been proposed, such as the ability to disrupt cell wall and membranes, leading to ATP and metabolite leakage. Additionally, the hydrophobic nature of the oil enables increased cell permeability, leading to bacterial cell leakage [12]. However, there remains a research gap, wherein it is unclear how effective these oils are against multidrug-resistant bacteria, in particular against MRSA. Thus, the aim of this systematic review was to identify whether eucalyptus essential oil, alone or in combination with other compounds, shows antimicrobial effects against MRSA.
2. Results
2.1. Search Results
Searching the four databases using the search strategy yielded a total of 242 articles. After duplicates were removed, 113 articles remained. The titles and abstracts of these articles were screened to yield 45 results. After reading the full texts of these 45 results, 25 articles were removed, due to reasons, such as not testing MRSA, not using E. globulus species, not using the essential oil and not being a primary article; 20 articles were included in this review, as these directly answered the focused question. The study selection process is presented in Figure 1 and the data extracted from the 20 included studies are presented in Table 1.
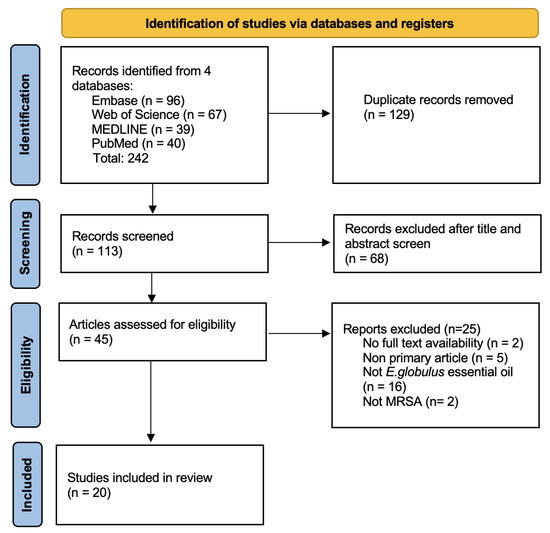
Figure 1.
Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) flow diagram of study selection process.

Table 1.
Antibacterial properties of Eucalyptus globulus essential oil against MRSA: a systematic review.
2.2. Effectiveness of Essential Oil against MRSA Alone as Per Different Methodology
2.2.1. Chemical Composition—GC/MS
Six studies studied the chemical composition of the oil using gas chromatography/mass spectrometry (GC/MS) [13,19,22,25,26,30] and one study used gas chromatography alone [28]. The composition of the oils varied between studies, between oils extracted from different parts of the plant and between various plant stages. All investigations, except for the fruit oil tested by Mulyaningsih et al., 2011 [25], found that 1,8 cineole was the main component of the extracts, with percentage values ranging from 32.19% [28] to 86.51% [25]. The values for 1,8 cineole were 84.8%, as per Acs et al., 2016 [13], 81.93%, as per Hamoud et al., 2012 [19], 84.2%, as per Horvath et al., 2011 [22], 86.51%, as per Mulyaningsih et al., 2010 [25], 32.19%, as per Salem et. al. 2018 [28] and 47.2%, as per Tohidpour et al., 2010 [30].
Salem et al., 2018 [28] and Tohidpour et al., 2010 [30] extracted the oils from “aerial parts” and did not specify that the extracts were from the leaf. Mulyaningsih et al., 2011 was the only study that tested oil from both the leaves and the fruit of E. globulus [25]. In the fruit oil, they identified aromadendrene as the main component, with 31.17%, followed by 1,8 cineole at 14.55%, whereas the two main components of the leaf oil were 1,8-cineole (86.51%), followed by α-pinene (4.74%).
Salem et al., 2018 was the only study to investigate the composition of oil based on the plant stage [28]. They discovered that the chemical composition differed depending on the plant stage. 1,8-cineole was the major compound at vegetative and full flowering (32.19%) but p- cymene was the major compound at fructification stages (37.82%).
2.2.2. MIC
Of the 19 studies, 13 determined the MIC of eucalyptus oil, with a large range of values from 0.032 mg/mL [7] up to 307 mg/mL [23]. Four studies carried out the procedure as per CLSI guidelines [17,21,23,26], one study used the microdilution method as per German DIN regulation [19], one study used the microdilution method as per De Lima Marques et al. (2015) [28], one study used the agar dilution method approved by NCCLS [30] and all other studies did not specify. All 13 studies concluded that eucalyptus essential oil has antibacterial properties against MRSA. The MIC values for studies that only tested the oil were 5.6 mg/mL as per Acs et al., 2016 [13], 0.33 mg/mL as per Ali et al., 2022 [14], 200 mg/mL as per Bouras et al., 2016 [15], 0.313 v/v% as per Cui et al., 2021 [17], 10 mg/mL as per Hamoud et al., 2012 [19], 32 µg/mL as per Iseppi et al., 2021 [7] and 85.6 µg/mL as per Tohidpour et al., 2010 [30].
Kwiatkowski et al., 2019 [23], Simsek et al., 2017 [29], Hendry et al., 2009 [21] and Merghni et al., 2018 [24], tested 1,8-cineole. Kwiatkowski et al., 2019 revealed the MIC was 307.00 mg/mL against Mupirocin-sensitive MRSA and 57.56 mg/mL against Mupirocin-resistant MRSA [23]. Simsek and Duman 2017 demonstrated that the MIC of 1,8 cineole was 128 g/L [29].
Merghni et al., 2018 [24] and Hendry et al., 2009 [21] tested both the MIC of the oil and its main component 1,8 cineole. Merghni et al., 2018 demonstrated that E. globulus oil had an MIC of 10 mg/mL and 1,8-cineole 1.25 mg/mL [24], whilst Hendry et al., 2009 showed that the MIC of E. globulus oil was 2 g/L and 1,8 cineole was 64 g/L [21].
Mulyaningsih et al., 2010 demonstrated that the eucalyptus leaf oil had an MIC between 2000 and >4000 µg/mL, fruit oil had an MIC of 250 µg/mL and aromadendrene was 0.25–1 mg/mL [26]. Salem et al., 2018 tested the oil at various growing stages to reveal MIC at vegetative stage 2 mg/mL, full flowering 4 mg/mL and fructification 4 mg/mL [28].
2.2.3. Biofilm
Five studies examined the ability of eucalyptus oil to reduce MRSA biofilm formation [7,20,21,24,27].
Hendry et al., 2012 examined wipes containing 5% and 2% eucalyptus oil, 2% chlorhexidine digluconate (CHG) and 70% isopropyl alcohol (IPA) [20]. They revealed that microbial biofilms were eliminated within 10 min (p < 0.05) when exposed to 2% EO formulation and within 5 min for 2% EO compared with the control, which took greater than 30 min. Hendry et al. (2009) revealed that eucalyptus oil was more effective at reducing biofilm, as the MIC of eucalyptus oil required to remove the biofilm was lower than that of 1,8 cineole [21].
Iseppi et al., 2021 tested eucalyptus oil alone to reveal it had an optical density of 0.1 at 570 nm, and this was even more effective in combination with Melaleuca alternifolia (tea tree) essential oil, in which the optical density was <0.05 (p < 0.001) [7]. Merghni et al., 2018 measured the percentage reduction in eucalyptus oil and its main component, 1,8 cineole [24]. 1,8 cineole was more effective than the whole oil, with a mean percentage reduction in the oil of 74.74% to 89.15% compared with 1,8 cineol, which was 77.46% to 90.81%. Punitha et al., 2014 also demonstrated that biofilm was inhibited considerably by eucalyptus oil, with average zones of inhibition ranging from 12.2 mm to 26.2 mm [27].
2.2.4. Zones of Inhibition
Three methods were used to study the zones of inhibitions: well diffusion, direct bioautography assays and disc diffusion, which was used by the majority.
Nine studies used the agar disc diffusion method to determine the zone of inhibition of E. globulus essential oil [7,15,16,18,24,27,28,30,31], with all except one [16] revealing antibacterial activity. Bouras et al., 2016 revealed a diameter between 8 and 14 mm, which, according to their classification, indicated that it was very sensitive (++) for all MRSA strains tested [15]. Chao et al., 2008 revealed that the zone of inhibition for eucalyptus oil was 0 mm; this was the only study that did not produce any activity on disc diffusion [16]. Farsi et al. demonstrated that the eucalyptus oil inhibition zone’s diameter was 11.33 mm and was significantly increased (p < 0.001) when loaded onto silica dioxide nanoparticles, with a diameter of 18.66 mm [18]. Iseppi et al., 2021 revealed that the inhibitory zone diameter was between 11 and 20 mm [7]. Merghni et al., 2018 investigated the inhibition zones of both eucalyptus oil and its main component 1,8 cineole to reveal that the oil had a reduced zone of inhibition compared to 1,8 cineole [24]. Eucalyptus oil diameter ranged from 10.7 mm to 26.3 mm, whilst 1,8-cineole was ≥29 mm. Salem et al. demonstrated varying levels of antibacterial activity between the oil, depending on the plant stage [28]. Inhibition zones reached up to 38 mm during vegetative stage but only 24 mm during flowering and fruitification. Punitha et al., 2014 examined the zone of inhibition in relation to biofilm and demonstrated that average zones of inhibition ranged from 12.2 mm to 26.2 mm [27]. Tohidpour et al., 2010 revealed that the inhibition zone of E. globulus oil was 8 mm [30], and for Warnke et al., it was 14 mm [31].
Ali et al., 2022 used the well diffusion method to determine zones of inhibition for multiple essential oils, including Syzygium aromaticum, Eucalyptus globulus, Cinnamomum verum and Ferula assafoetida, to reveal that eucalyptus oil recorded the second-highest zone of inhibition of 18.67 ± 2.51 mm [14].
Horvath et al. trialled various volumes of the essential oil using direct bioautography assays to determine the inhibition zones and revealed that eucalyptus oil produced 0 mm for 1 μL oil, 2.5 mm for 5 μL oil and 6.5 mm for 10 μL oil [22].
2.2.5. Vapour Phase
Only one study, Acs et al., 2016, showed the effects of E. globulus oil in the vapour phase [13]. They demonstrated that eucalyptus oil did not present inhibition against any test bacteria, even in a 1500 μL/L concentration, which differed from their tube dilution results, which showed antibacterial effects against MRSA in liquid medium.
2.2.6. Time-Kill Assays
Three studies [7,17,19] used time–kill assays.
Iseppi et al., 2021 [7] showed synergistic activity between tea tree oil and eucalyptus oil, with bacterial load reduction obtained at low concentrations in both synthetic and natural compounds. The optical density at 595 nm was 0.2 after 24 h and was not statistically significant for eucalyptus oil alone or for oxacillin alone; however, it was for the combination mentioned above. The optical density of oxacillin was 0.8 after 24 h. The optical density for tea tree oil in combination with eucalyptus oil was almost >0.05 after 24 h.
Hamoud et al., 2012 [19] demonstrated that Olbas oil exhibited a bactericidal effect against MRSA (reduction of 3 × log10 cfu/mL) at a concentration of 8 × MIC (10 mg/mL Olbas) after 24 h. Lower concentrations only exhibited a weak bacteriostatic effect within the first six hours, which was then followed by significant regrowth.
Cui et al., 2021 [17] did not trial eucalyptus oil for their time–kill assays.
2.3. Effectiveness of E. globulus Essential Oil in Combination with Other Agents
Seven studies [7,17,18,19,20,23,26] examined the effects of eucalyptus oil when used in combination with other compounds. Hamoud et al., 2012 [19] and Iseppi et al., 2021 [7] examined the synergy between eucalyptus essential oil and various other essential oils. Hamoud et al., 2012 examined Olbas, an essential oil distillate composed of peppermint oil, eucalyptus oil, cajuput oil, juniper berry oil and wintergreen oil, which had greater antibacterial effects than eucalyptus alone [19]. Iseppi et al., 2021 demonstrated synergistic activity between Melaleuca alternifolia (tea tree) essential oil and eucalyptus essential oil [7].
Cui et al., 2021 [17], Iseppi et al., 2021 [7] and Kwiatkowski et al., 2019 [23] studied the synergistic effects of eucalyptus oil and antibiotics, with all studies concluding a greater antibacterial effect than with each agent acting alone. Cui et al., 2021 revealed that there was a low level of synergy between eucalyptus oil and antibiotics, including vancomycin, streptomycin, gentamicin and tetracycline [17]. Iseppi et al., 2021 revealed synergy between eucalyptus oil and oxacillin [7], and Kwiatkowski et al., 2019 demonstrated synergy between mupirocin and 1,8-cineole [23].
Mulyaningsih et al., 2010 examined the combination of eucalyptus essential oil components, noting synergy between the two major components, aromadendrene and 1,8 cineole [26]. Farsi and Alaidaroos 2022 examined eucalyptus oil loaded in silica dioxide nanoparticles, which revealed a significant increase in the diameters of inhibition zones (p < 0.001) compared with the diameters of the individual agents [18]. Hendry et al., 2009 demonstrated synergistic activity between CHG and both eucalyptus oil and 1,8-cineole against suspensions of MRSA [21].
3. Discussion
Antibiotic resistance has become a major cause of global mortality and is classified by the World Health Organisation as being in the top ten threats to global health (WHO, 2020) [4]. It is a process wherein bacteria evade antibiotics via various mechanisms, the drivers of which include overuse and abuse of antibiotics in clinical and agricultural settings [1,3]. Since the 1940s, with the advent of modern antibiotics, bacteria have developed resistance to almost all available antibiotics and, thus, there is an urgent need to identify alternative compounds to combat this issue. An example of such an alternative is essential oils. Eucalyptus essential oil is composed of a myriad of volatile compounds, each of which have varying levels of antibacterial activity. The oil in its whole form has been proven to possess antibacterial qualities against MRSA and its biofilm. Its antibacterial properties can be enhanced when used in conjunction with other agents, such as other essential oils and antibiotics.
3.1. Composition of E. globulus Essential Oil
Essential oils are composed of complex combinations of volatile plant compounds, with the main compounds often being terpenoid and phenylpropanoid derivatives [32]. The chemical composition of the oils can be determined using gas chromatography along with other analytical tools, such as mass spectrometry [32]. Based on the results of the gas chromatography/mass spectrometry, the composition of the eucalyptus essential oils varies greatly depending on which part of the plant the oil was extracted from. For example, Mulyaningsih et al., 2011 reveal that the main component of the oil extracted from the leaves of the plant is 1,8 cineole, whereas the main component of oil extracted from the fruit is aromadendrene and only contains one-fifth the amount of 1,8 cineole as the leaf oil [25].
The composition also varies depending upon the growing stage of the plant; for example, Salem et al. showed that 1,8-cineole was the major compound at vegetative and full flowering, but p-cymene was the major compound at fructification stages [28]. Thus, this may explain the reason for such varied values among the studies that did not specify where the oil was extracted from. Salem et al., 2018 [28] and Tohidpour et al., 2010 [30] had significantly lower values and did not specify where from the plant they retrieved the oil, only mentioning “aerial parts”, which includes any part of the plant above the ground, such as fruits, leaves, stems and flowers, all of which have vastly different compositions [33]. This is also suggested by the results of Mulyaningsih et al.’s 2011 study of both leaves and fruit oils [25]. Additionally, other than Salem et al., none of the studies indicated what growing stage the plants were in, and this is also likely to contribute to the differences in composition, as indicated by the results of Salem et al. [28].
Thus, the plant growing stage and the part of the plant the oil is extracted from should be specified to accurately correlate antibacterial activity with individual oil constituents to ensure accuracy and reproducibility of the results [28]. The method of extraction may also change the composition and, thus, this should also be noted [32].
3.2. MIC of E. globulus Essential Oil against MRSA Strains
The minimum inhibitory concentration (MIC) is the lowest concentration of an antimicrobial agent that is required to visibly inhibit the growth of a bacterium after incubation overnight [34]. The MIC values of the whole essential oil range from 0.032 mg/mL [7] to 200 mg/mL [15], being 300-times the value of the second-highest MIC, which was only 10 mg/mL [15]. The values for all other studies were relatively similar, within a range of 0.032 mg/mL to 10 mg/mL [7,13,14,15,17,19,30].
The studies that only tested 1,8 cineole had much higher MIC values than those of the whole oil [21,23,29]. The lowest MIC for 1,8 cineole was 1800-times the value of the lowest MIC for the whole oil. This was 230-times higher than the MIC of aromadendrene, suggesting that the antibacterial activity of 1,8 cineole is much lower than that of the whole oil and aromadendrene. Additionally, the MIC of eucalyptus leaf oil was 16-times higher than that of fruit oil. As demonstrated by Mulyaningsih et al., 2011, this may be explained by the fact that the main component of the leaf oil is 1,8 cineole, whereas the main component of the fruit oil is aromadendrene [25]. Aromadendrene has more antibacterial potency than 1,8 cineole, resulting in a lower MIC of the leaf oil [25].
The MIC of eucalyptus oil varies during different phases of the plant growth cycle, with MIC during the vegetative stage being half than that of full flowering and fruitification [28]. This may also be explained by the changes in composition during these phases, as explained in the previous paragraph. Additionally, variations in MIC may be explained by factors, including, but not limited to, the MRSA strain it was tested against, the geographic origin of the plant, the period in which it was harvested, how it was processed and the conditions in which it was stored [35]. All these factors have an impact on the composition of the oils as well as the proportion and interaction of their volatile molecules [35,36].
3.3. Zones of Inhibition Produced by E. globulus Essential Oil
The disc diffusion test is used to determine the susceptibility of a microorganism to an antimicrobial agent [37]. The diameter of growth that was inhibited is known as the zone of inhibition [37]. The zone of inhibition diameters for eucalyptus essential oil vary between studies, with values ranging from 0 mm to 38 mm. Only one study [16] showed that the oil did not produce any inhibition, while another study [22] demonstrated no inhibition for small volumes (1 μL) of oil but inhibition for greater volumes. Since 30 μL of oil was used in the first study [16], insufficient volume of the oil cannot be the reason for non-inhibition. It is notable that the disc diffusion method is a qualitative method that is not very effective for essential oils because their volatile nature reduces their potency, and, thus, the results may show reduced antibacterial activity [38].
3.4. Effectiveness of Combination of Agents against MRSA Strains
Synergy is achieved when the sum of the antibacterial activity of two agents is greater than when acting alone [39,40]. This may be attributed to the presence of multiple active antibacterial constituents and interactions between various constituents of both oils [39,40], the combination of which may have various actions, such as increasing the solubility and/or bioavailability of one or more constituents of the oil or acting on different targets, leading to an enhanced antibacterial effect [39]. Synergy is noted between various agents, such as Olbas (composed of peppermint oil, eucalyptus oil, cajuput oil, juniper berry oil and wintergreen oil) [19], between tea tree oil and eucalyptus oil [7], various antibiotics and eucalyptus oil [7,17,23,41].
Synergy is also noted between eucalyptus oil loaded in silica dioxide nanoparticles [18]. The encapsulation of the essential oils reduces their volatility by decreasing their sensitivity to moisture, oxygen, light and heat and, thus, can enhance their antibacterial effects [40]. Additionally, eucalyptus oil tested with 2% chlorhexidine digluconate (CHG) and 70% isopropyl alcohol (IPA) within a wipe showed synergy between eucalyptus oil and CHG against MRSA grown in biofilm and planktonic cultures [20]. The wipes that contained eucalyptus oil, CGH and IPA were significantly quicker and more effective at eliminating biofilm than the wipes that contained only CHG and IPA [20]. This shows that eucalyptus essential oil has potential to enhance the efficacy of hard surface disinfectant wipes that can be used in clinical settings to minimise the risk of hospital-acquired infections.
3.5. Biofilm Inhibition by E. globulus Essential Oil
Biofilm enables bacteria to evade antibiotics and the host immune system and is, thus, a cause of nosocomial infections [42]. It enables the bacterium to embed itself into the biofilm and establish planktonic forms [42]. Hendry et al. (2012) [20] is the only study that tested E.globulus oil against planktonic growth and demonstrated that it is effective against both biofilm and planktonic modes of growth [21]. They also revealed that the MIC of eucalyptus oil required to remove the biofilm was lower than that of 1,8 cineole, in contrast with Merghni et al., 2018, who revealed that the opposite is true, with 1,8 cineole having a greater mean percentage reduction in biofilm and, thus, being more effective than the whole oil [24]. Merghni et al., 2018 [24] did not measure the MIC and, thus, a direct comparison with Hendry et al., 2012 [20] may not be accurate to make a conclusion about which agent is more effective at biofilm inhibition. Punitha et al., 2014 also demonstrated that biofilm was inhibited considerably by eucalyptus oil [27]; however, as they measured the effectiveness using zones of inhibition, it is once again inaccurate to compare these results with those of the other studies. Additionally, a combination of eucalyptus oil and tea tree oil is more effective at reducing biofilm than either agent alone [7].
3.6. Vapour Phase of E. globulus Essential Oil
The vapours from essential oils have shown potential to possess antibacterial properties, which can be altered in the liquid phase; however, only a limited number of studies have tested the oils in their vapour phase [43,44]. Of the studies included in this review, Acs et al., 2016 was the only one that tested the antibacterial properties of eucalyptus oil in the vapour phase, the rationale for which was to evaluate it as a potential treatment for respiratory tract infection, wherein the vapour can be inhaled [13]. Eucalyptus oil did not inhibit any bacterial growth, even at high concentrations, which contradicted the results of the tube dilution method, indicating that it may be more potent in liquid form rather than vapour form. The vapour form places emphasis on the testing of volatile compounds rather than all compounds within the oil and, thus, these results may demonstrate that the concertation and potency of the volatile compounds within the oil have less antibacterial properties than the other constituents of the oil [13].
3.7. Time–Kill Test to Determine Bactericidal Potential of E. globulus
The time–kill test is a robust test for determining the bactericidal potential of an agent [45]; however, only two studies utilised this method to test eucalyptus oil [7,19]. Hamoud et al., 2012 demonstrates that there is a dose-dependent antibacterial effect against MRSA [19]. Iseppi et al. did not test the oil at various concentrations, but rather revealed that there is a time-dependent antimicrobial effect [7].
3.8. Strengths and Limitations of Study
This study has many strengths. Many of the included studies follow laboratory guidelines, such as CLSI, thus ensuring high quality. Additionally, the studies tested various parameters, such as variations between different parts of the eucalyptus plant, oils from different plant growth stages, biofilm inhibition, antibacterial properties of the oil in vapour phase and combinations of agents. This provides a more holistic understanding of the antimicrobial properties of the oil and allows for a clearer understanding of its multifaceted nature. These studies were carried out in different parts of the world, ensuring that antibacterial effects of eucalyptus oil are ubiquitously reported.
This study also has some limitations. Only four databases were searched and, thus, some articles may have been missed. Additionally, only English texts were included, and this may have led to exclusion of other relevant studies. Furthermore, there is limited research on this topic and, thus, the number of studies included in this review is minimal. This diminishes the ability to make conclusive judgments and, thus, more data are required. Within these studies, there are a wide variety of methods used, which, although providing valuable insight into various paraments, affects the overall reliability and applicability of the data.
4. Materials and Methods
4.1. Focused Question
Does eucalyptus essential oil, alone or in combination with other compounds, exhibit antibacterial effects against MRSA?
4.2. PICO Question
Population—MRSA strains
Intervention—eucalyptus essential oil
Control—no oil/antibiotic
Outcome—antimicrobial effects
4.3. Search Strategy
The literature search was performed on 30 June 2022 and included four databases: PubMed, Web of Science, MEDLINE and Embase. The timeline restricted to twenty years, from 1 July 2002 until 30 June 2022. Keywords included “(Antimicrobial OR antibacterial OR antifungal OR antiviral) AND (eucalyptus oil OR eucalyptus OR aromadendrene OR 1,8 cineole OR globulol) AND (MRSA OR methicillin resistant staph aureus OR methicillin resistant staphylococcus aureus OR methicillin resistant s aureus)”.
4.4. Eligibility Criteria
4.4.1. Inclusion Criteria
Only full-text primary articles in English were included. All methodologies, such as vapour and broth microdilution, were included. Studies that used the oil as a whole or isolated compounds from the oil were included. Studies that used oil as the only agent or used combination of oil with other agents and various forms of oil, e.g., fruit oil and leaf oil, were all included.
4.4.2. Exclusion Criteria
Grey literature, conference abstracts, posters and review articles were excluded. Studies that used eucalyptus leaf extracts, rather than essential oil, were excluded, as were studies that tested species of Eucalyptus other than E. globulus or tested the agents against pathogens other than MRSA.
4.5. Study Selection
Titles and abstracts were reviewed and inclusion and exclusion criteria were applied to ensure only relevant articles were included, after which full text was screened to further exclude any articles that did not align with the criteria. The search selection was carried out by two independent authors (SE and PM) and conflicts were resolved by mutual consensus.
4.6. Study Quality and Risk of Bias
Study quality was ascertained by inclusion of studies using methodologies with standardised procedures, such as CLSI guidelines.
4.7. Data Extraction
Data were extracted from the included studies and organised in a table containing information on location of study, methodology used, objectives and relevant findings.
5. Conclusions
Thus, given that the majority of studies provide evidence in the form of MIC values, zones of inhibition diameters and time–kill studies, it can be concluded that E. globulus essential oil does possess antibacterial properties against MRSA and its biofilm. Despite many variations between the values published by the studies, there seems to be consensus that eucalyptus essential oil has bactericidal properties. Additionally, the studies also demonstrate that these antibacterial properties can be enhanced by combining the oil with other agents, such as other essential oils and antibiotics. Numerous compounds have been extracted from the plant, each with varying levels of antimicrobial activity, allowing for potency to be improved through isolation and combination of such constituents. These results provide evidence that supports the potential use of eucalyptus essential oil as an antimicrobial agent to combat the rapidly evolving problem of antimicrobial-resistant bacteria. More data are needed on this topic to draw conclusive results. Additionally, adopting a more standardised approach between studies would further enhance the reproducibility and accuracy of the results.
Author Contributions
Conceptualization, P.M.; methodology, S.E. and P.M.; validation, S.E. and P.M.; formal analysis, S.E.; investigation, S.E.; data curation, S.E.; writing—original draft preparation, S.E.; writing—review and editing, S.E. and P.M.; resources, P.M.; supervision, P.M.; project administration, P.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data are contained within this article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Habboush, Y.; Guzman, N. Antibiotic Resistance; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Richardson, L.A. Understanding and overcoming antibiotic resistance. PLoS Biol. 2017, 15, e2003775. [Google Scholar] [CrossRef] [PubMed]
- Ventola, C.L. The antibiotic resistance crisis: Part 1: Causes and threats. Pharm. Ther. 2015, 40, 277–283. [Google Scholar]
- WHO. WHO World Antimicrobial Awareness Week-WAAW from 18 to 24 November 2020. Available online: https://www.who.int/campaigns/world-antimicrobial-awareness-week/2020 (accessed on 9 April 2021).
- Siddiqui, A.H.; Koirala, J. Methicillin Resistant Staphylococcus Aureus; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Turner, N.A.; Sharma-Kuinkel, B.K.; Maskarinec, S.A.; Eichenberger, E.M.; Shah, P.P.; Carugati, M.; Holland, T.L.; Fowler, V.G., Jr. Methicillin-resistant Staphylococcus aureus: An overview of basic and clinical research. Nat. Rev. Microbiol. 2019, 17, 203–218. [Google Scholar] [CrossRef] [PubMed]
- Iseppi, R.; Mariani, M.; Condo, C.; Sabia, C.; Messi, P. Essential Oils: A Natural Weapon against Antibiotic-Resistant Bacteria Responsible for Nosocomial Infections. Antibiotics 2021, 10, 417. [Google Scholar] [CrossRef]
- Sharifi-Rad, J.; Sureda, A.; Tenore, G.C.; Daglia, M.; Sharifi-Rad, M.; Valussi, M.; Tundis, R.; Sharifi-Rad, M.; Loizzo, M.R.; Ademiluyi, A.O.; et al. Biological Activities of Essential Oils: From Plant Chemoecology to Traditional Healing Systems. Molecules 2017, 22, 70. [Google Scholar] [CrossRef]
- Boren, K.; Crown, A.; Carlson, R. Multidrug and Pan-Antibiotic Resistance—The Role of Antimicrobial and Synergistic Essential Oils: A Review. Nat. Prod. Commun. 2020, 15, 1934578X2096259. [Google Scholar] [CrossRef]
- Bassolé, I.H.N.; Juliani, H.R. Essential Oils in Combination and Their Antimicrobial Properties. Molecules 2012, 17, 3989–4006. [Google Scholar] [CrossRef]
- Immaroh, N.Z.; Kuliahsari, D.E.; Nugraheni, S.D. Review: Eucalyptus globulus essential oil extraction method. IOP Conf. Ser. Earth Environ. Sci. 2021, 733, 012103. [Google Scholar] [CrossRef]
- Chandorkar, N.; Tambe, S.; Amin, P.; Madankar, C. A systematic and comprehensive review on current understanding of the pharmacological actions, molecular mechanisms, and clinical implications of the genus Eucalyptus. Phytomed. Plus 2021, 1, 100089. [Google Scholar] [CrossRef]
- Acs, K.; Bencsik, T.; Boszormenyi, A.; Kocsis, B.; Horvath, G. Essential Oils and Their Vapors as Potential Antibacterial Agents against Respiratory Tract Pathogens. Nat. Prod. Commun. 2016, 11, 1709–1712. [Google Scholar]
- Ali, T.; Anjum, A.A.; Sattar MM, K.; Ali, M.A.; Kamran, M.; Tariq, M.; Manzoor, R. Antibacterial activity of plant essential oils against indigenously characterized methicillin-resistant Staphylococcus aureus (MRSA). Trop. Biomed. 2022, 39, 17–25. [Google Scholar]
- Bouras, M.; Abbaci, N.B.; Bennadja, S. Antibacterial activity of essential oil and aqueous extract of Eucalyptus globulus against methicillin resistance Staphylococcus aureus and methicillin sensitive Staphylococcus aureus. Int. J. Pharmacogn. Phytochem. Res. 2016, 8, 1717–1721. [Google Scholar]
- Chao, S.; Young, G.; Oberg, C.; Nakaoka, K. Inhibition of methicillin-resistant Staphylococcus aureus (MRSA) by essential oils. Flavour Fragr. J. 2008, 23, 444–449. [Google Scholar] [CrossRef]
- Cui, Z.H.; He, H.L.; Wu, S.B.; Dong, C.L.; Lu, S.Y.; Shan, T.J.; Fang, L.-X.; Liao, X.P.; Liu, Y.H.; Sun, J. Rapid screening of essential oils as substances which enhance antibiotic activity using a modifiedwell diffusion method. Antibiotics 2021, 10, 463. [Google Scholar] [CrossRef] [PubMed]
- Farsi, R.; Alaidaroos, B. Antibacterial Activity of Eucalyptus Essential Oil loaded on Silica Dioxide Nanoparticles (SiNPs) Against Some Pathogenic Bacteria. Int. J. Pharm. Phytopharm. Res. 2022, 12, 29–37. [Google Scholar] [CrossRef]
- Hamoud, R.; Sporer, F.; Reichling, J.; Wink, M. Antimicrobial activity of a traditionally used complex essential oil distillate (Olbas(®) Tropfen) in comparison to its individual essential oil ingredients. Phytomedicine 2012, 19, 969–976. [Google Scholar] [CrossRef] [PubMed]
- Hendry, E.; Conway, B.; Worthington, T. Antimicrobial Efficacy of a Novel Eucalyptus Oil, Chlorhexidine Digluconate and Isopropyl Alcohol Biocide Formulation. Int. J. Mol. Sci. 2012, 13, 14016–14025. [Google Scholar] [CrossRef]
- Hendry, E.R.; Worthington, T.; Conway, B.R.; Lambert, P.A. Antimicrobial efficacy of eucalyptus oil and 1,8-cineole alone and in combination with chlorhexidine digluconate against microorganisms grown in planktonic and biofilm cultures. J. Antimicrob. Chemother. 2009, 64, 1219–1225. [Google Scholar] [CrossRef]
- Horváth, G.; Jámbor, N.; Kocsis, E.; Böszörményi, A.; Lemberkovics, É.; Héthelyi, É.; Kovács, K.; Kocsis, B. Role of Direct Bioautographic Method for Detection of Antistaphylococcal Activity of Essential Oils. Nat. Prod. Commun. 2011, 6, 1379–1384. [Google Scholar] [CrossRef]
- Kwiatkowski, P.; Pruss, A.; Wojciuk, B.; Dołęgowska, B.; Wajs-Bonikowska, A.; Sienkiewicz, M.; Mężyńska, M.; Łopusiewicz, Ł. The Influence of Essential Oil Compounds on Antibacterial Activity of Mupirocin-Susceptible and Induced Low-Level Mupirocin-Resistant MRSA Strains. Molecules 2019, 24, 3105. [Google Scholar] [CrossRef]
- Merghni, A.; Noumi, E.; Hadded, O.; Dridi, N.; Panwar, H.; Ceylan, O.; Mastouri, M.; Snoussi, M. Assessment of the antibiofilm and antiquorum sensing activities of Eucalyptus globulus essential oil and its main component 1,8-cineole against methicillin-resistant Staphylococcus aureus strains. Microb. Pathog. 2018, 118, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Mulyaningsih Sporer, F.; Reichling, J.; Wink, M. Antibacterial activity of essential oils from Eucalyptus and of selected components against multidrug-resistant bacterial pathogens. Pharm. Biol. 2011, 49, 893–899. [Google Scholar] [CrossRef] [PubMed]
- Mulyaningsih, S.; Sporer, F.; Zimmermann, S.; Reichling, J.; Wink, M. Synergistic properties of the terpenoids aromadendrene and 1,8-cineole from the essential oil of Eucalyptus globulus against antibiotic-susceptible and antibiotic-resistant pathogens. Phytomedicine 2010, 17, 1061–1066. [Google Scholar] [CrossRef] [PubMed]
- Punitha, T.; Moorthy, K.; Vijayalakshmi, P.; Vinodhini, R.; Saranya, S.; Bhuvaneshwari, M.; Kanimozhi, C. In vitro antibacterial activity of essential plant oils against biofilm forming methicillin resistant staphylococcus aureus. Asian J. Pharm. Clin. Res. 2014, 7 (Suppl. S1), 220–225. [Google Scholar]
- Salem, N.; Kefi, S.; Tabben, O.; Ayed, A.; Jallouli, S.; Feres, N.; Hammami, M.; Khammassi, S.; Hrigua, I.; Nefisi, S.; et al. Variation in chemical composition of Eucalyptus globulus essential oil under phenological stages and evidence synergism with antimicrobial standards. Ind. Crop. Prod. 2018, 124, 115–125. [Google Scholar] [CrossRef]
- Simsek, M.; Duman, R. Investigation of Effect of 1,8-cineole on Antimicrobial Activity of Chlorhexidine Gluconate. Pharmacogn. Res. 2017, 9, 234–237. [Google Scholar] [CrossRef] [PubMed]
- Tohidpour, A.; Sattari, M.; Omidbaigi, R.; Yadegar, A.; Nazemi, J. Antibacterial effect of essential oils from two medicinal plants against Methicillin-resistant Staphylococcus aureus (MRSA). Phytomedicine 2010, 17, 142–145. [Google Scholar] [CrossRef]
- Warnke, P.H.; Becker, S.T.; Podschun, R.; Sivananthan, S.; Springer, I.N.; Russo, P.A.; Wiltfang, J.; Fickenscher, H.; Sherry, E. The battle against multi-resistant strains: Renaissance of antimicrobial essential oils as a promising force to fight hospital-acquired infections. J. Craniomaxillofac Surg. 2009, 37, 392–397. [Google Scholar] [CrossRef]
- Fokou, J.B.H.; Dongmo, P.M.J.; Boyom, F.F. Essential Oil’s Chemical Composition and Pharmacological Properties. In Essential Oils-Oils of Nature; El-Shemy, H.A., Ed.; IntechOpen: London, UK, 2020; Available online: https://www.intechopen.com/chapters/68008 (accessed on 19 July 2022).
- Eichert, T.; Fernández, V. Chapter 4-Uptake and Release of Elements by Leaves and Other Aerial Plant Parts. In Marschner’s Mineral Nutrition of Higher Plants, 3rd ed.; Marschner, P., Ed.; Academic Press: San Diego, CA, USA, 2012; pp. 71–84. [Google Scholar]
- Andrews, J.M. Determination of minimum inhibitory concentrations. J. Antimicrob. Chemother. 2001, 48 (Suppl. S1), 5–16. [Google Scholar] [CrossRef]
- Thielmann, J.; Muranyi, P.; Kazman, P. Screening essential oils for their antimicrobial activities against the foodborne pathogenic bacteria Escherichia coli and Staphylococcus aureus. Heliyon 2019, 5, e01860. [Google Scholar] [CrossRef]
- Dhifi, W.; Bellili, S.; Jazi, S.; Bahloul, N.; Mnif, W. Essential Oils’ Chemical Characterization and Investigation of Some Biological Activities: A Critical Review. Medicines 2016, 3, 25. [Google Scholar] [CrossRef] [PubMed]
- Reller, L.B.; Weinstein, M.; Jorgensen, J.H.; Ferraro, M.J. Antimicrobial Susceptibility Testing: A Review of General Principles and Contemporary Practices. Clin. Infect. Dis. 2009, 49, 1749–1755. [Google Scholar]
- Orchard, A.; van Vuuren, S. Commercial Essential Oils as Potential Antimicrobials to Treat Skin Diseases. Evid Based Complement Altern. Med. 2017, 2017, 4517971. [Google Scholar] [CrossRef] [PubMed]
- Wagner, H. Synergy research: Approaching a new generation of phytopharmaceuticals. Fitoterapia 2011, 82, 34–37. [Google Scholar] [CrossRef]
- Chouhan, S.; Sharma, K.; Guleria, S. Antimicrobial Activity of Some Essential Oils-Present Status and Future Perspectives. Medicines 2017, 4, 58. [Google Scholar] [CrossRef]
- Kwiatkowski, P.; Łopusiewicz, Ł.; Pruss, A.; Kostek, M.; Sienkiewicz, M.; Bonikowski, R.; Wojciechowska-Koszko, I.; Dołęgowska, B. Antibacterial Activity of Selected Essential Oil Compounds Alone and in Combination with β-Lactam Antibiotics Against MRSA Strains. Int. J. Mol. Sci. 2020, 21, 7106. [Google Scholar] [CrossRef]
- Cernohorska, L.; Votava, M. Biofilms and their significance in medical microbiology. Epidemiol. Mikrobiol. Imunol. 2002, 51, 161–164. [Google Scholar]
- Laird, K.; Phillips, C. Vapour phase: A potential future use for essential oils as antimicrobials? Lett. Appl. Microbiol. 2012, 54, 169–174. [Google Scholar] [CrossRef]
- Tyagi, A.K.; Malik, A. In situ SEM, TEM and AFM studies of the antimicrobial activity of lemon grass oil in liquid and vapour phase against Candida albicans. Micron 2010, 41, 797–805. [Google Scholar] [CrossRef]
- Balouiri, M.; Sadiki, M.; Ibnsouda, S.K. Methods for in vitro evaluating antimicrobial activity: A review. J. Pharm. Anal. 2016, 6, 71–79. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).