

Current and Future Pathways in Aspergillus Diagnosis

Abstract
:1. Introduction
2. Confirmation of Aspergillosis in a Primarily Sterile Site
2.1. Histology, Culture, and Radiography
2.2. DNA Analysis and Fungal Species Identification
3. Non-Culture-Based Approaches in Bronchoalveolar Lavage Fluid
3.1. Galactomannan
3.2. 1,3-β-d-Glucan (BDG)
3.3. Aspergillus-Specific PCR, Aspergillus DNA in Panfungal PCR Assays, and Metagenomic Next-Generation Sequencing
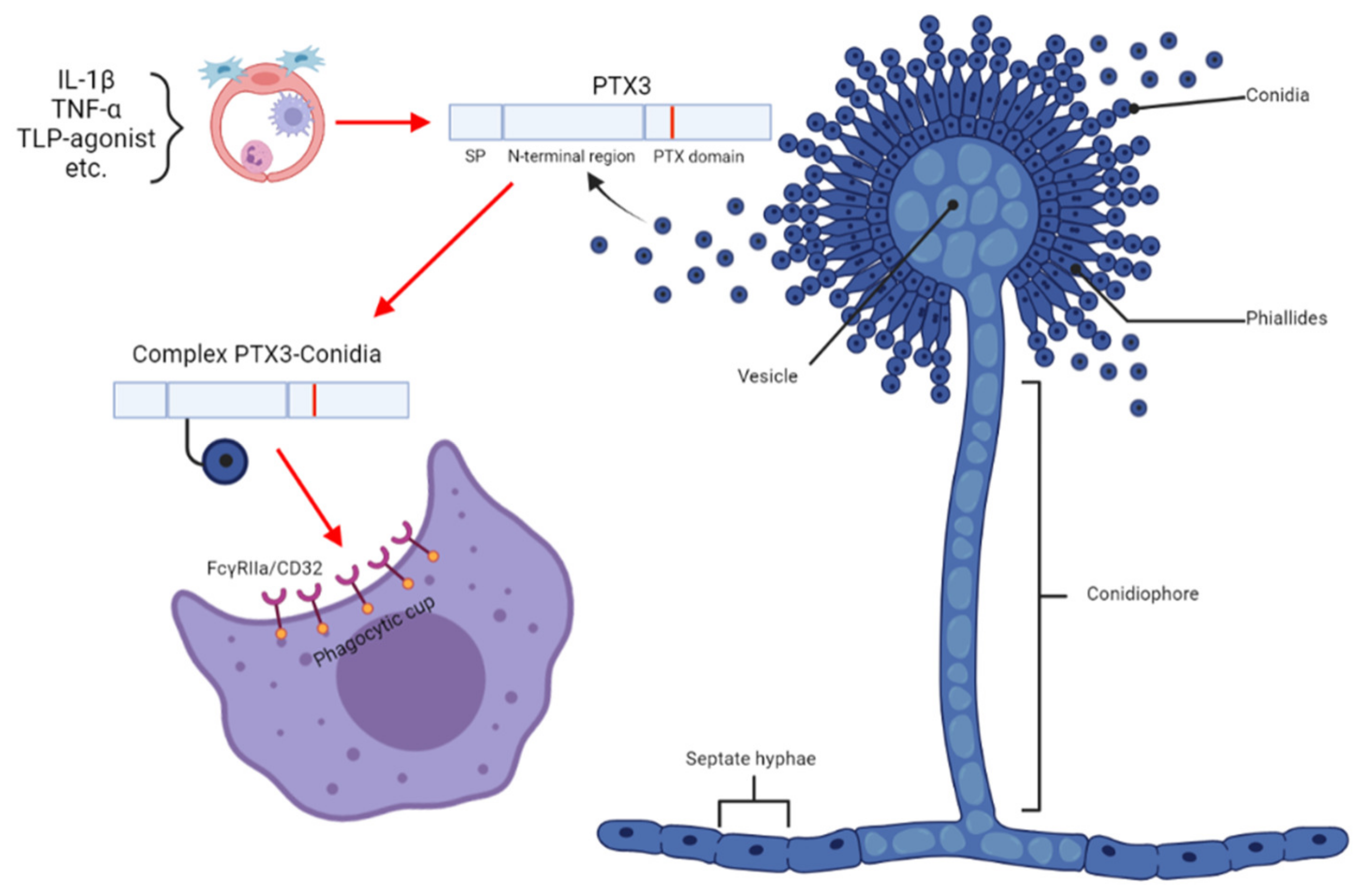
3.4. Pentraxin 3 Is a Host Factor
4. Monitoring of Serum Biomarkers
4.1. Galactomannan
4.2. 1,3-β-d-Glucan
4.3. Aspergillus-Specific PCR and Metagenomic Next-Generation Sequencing
5. The Aspergillus-Specific Lateral Flow Device
6. Antibodies
7. Gliotoxin and Bis(methylthio)gliotoxin
8. Aspergillus Metallophores
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Fungal Priority Pathogens List to Guide Research, Development and Public Health Action. Available online: https://www.who.int/publications/i/item/9789240060241 (accessed on 11 November 2022).
- Kanj, A.; Abdallah, N.; Soubani, A.O. The spectrum of pulmonary aspergillosis. Respir. Med. 2018, 141, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Azoulay, E.; Kullberg, B.-J.; Ruhnke, M.; Shoham, S.; Vazquez, J.; Giacobbe, D.R.; Calandra, T. EORTC/MSGERC Definitions of Invasive Fungal Diseases: Summary of Activities of the Intensive Care Unit Working Group. Clin. Infect. Dis. 2021, 72, S121–S127. [Google Scholar] [CrossRef] [PubMed]
- Giacobbe, D.R.; Prattes, J.; Wauters, J.; Dettori, S.; Signori, A.; Salmanton-García, J.; Maertens, J.; Bourgeois, M.; Reynders, M.; Rutsaert, L.; et al. Prognostic Impact of Bronchoalveolar Lavage Fluid Galactomannan and Aspergillus Culture Results on Survival in COVID-19 Intensive Care Unit Patients: A Post Hoc Analysis from the European Confederation of Medical Mycology (ECMM) COVID-19-Associated Pulmonary Aspergillosis Study. J. Clin. Microbiol. 2022, 60, e0229821. [Google Scholar] [CrossRef] [PubMed]
- El-Baba, F.; Gao, Y.; Soubani, A.O. Pulmonary Aspergillosis: What the Generalist Needs to Know. Am. J. Med. 2020, 133, 668–674. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Giacobbe, D.R.; Grecchi, C.; Rebuffi, C.; Zuccaro, V.; Scudeller, L.; Akova, M.; Alastruey-Izquierdo, A.; Arikan-Akdagli, S.; Azoulay, E.; et al. Performance of existing definitions and tests for the diagnosis of invasive aspergillosis in critically ill, adult patients: A systematic review with qualitative evidence synthesis. J. Infect. 2020, 81, 131–146. [Google Scholar] [CrossRef]
- Fernández-Cruz, A.; Magira, E.; Heo, S.T.; Evans, S.; Tarrand, J.; Kontoyiannis, D.P. Bronchoalveolar Lavage Fluid Cytology in Culture-Documented Invasive Pulmonary Aspergillosis in Patients with Hematologic Diseases: Analysis of 67 Episodes. J. Clin. Microbiol. 2018, 56, e00962-18. [Google Scholar] [CrossRef]
- Lass-Flörl, C.; Aigner, M.; Nachbaur, D.; Eschertzhuber, S.; Bucher, B.; Geltner, C.; Bellmann, R.; Lackner, M.; Orth-Höller, D.; Würzner, R.; et al. Diagnosing filamentous fungal infections in immunocompromised patients applying computed tomography-guided percutaneous lung biopsies: A 12-year experience. Infection 2017, 45, 867–875. [Google Scholar] [CrossRef]
- Lass-Flörl, C. How to make a fast diagnosis in invasive aspergillosis. Med. Mycol. 2019, 57, S155–S160. [Google Scholar] [CrossRef]
- Lyskova, P.; Hubka, V.; Svobodova, L.; Barrs, V.; Dhand, N.K.; Yaguchi, T.; Matsuzawa, T.; Horie, Y.; Kolarik, M.; Dobias, R.; et al. Antifungal Susceptibility of the Aspergillus viridinutans Complex: Comparison of Two In Vitro Methods. Antimicrob. Agents Chemother. 2018, 62, e01927-17. [Google Scholar] [CrossRef]
- Berkow, E.L.; Lockhart, S.R.; Ostrosky-Zeichner, L. Antifungal Susceptibility Testing: Current Approaches. Clin. Microbiol. Rev. 2020, 33, e00069-19. [Google Scholar] [CrossRef]
- Lau, A.; Chen, S.; Sorrell, T.; Carter, D.; Malik, R.; Martin, P.; Halliday, C. Development and Clinical Application of a Panfungal PCR Assay To Detect and Identify Fungal DNA in Tissue Specimens. J. Clin. Microbiol. 2007, 45, 380–385. [Google Scholar] [CrossRef]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2019, 71, 1367–1376. [Google Scholar] [CrossRef]
- Chong, W.; Neu, K. Incidence, diagnosis and outcomes of COVID-19-associated pulmonary aspergillosis (CAPA): A systematic review. J. Hosp. Infect. 2021, 113, 115–129. [Google Scholar] [CrossRef]
- Douglas, A.P.; Smibert, O.C.; Bajel, A.; Halliday, C.L.; Lavee, O.; McMullan, B.; Yong, M.K.; van Hal, S.J.; Chen, S.C.; Slavin, M.A.; et al. Consensus guidelines for the diagnosis and management of invasive aspergillosis, 2021. Intern. Med. J. 2021, 51, 143–176. [Google Scholar] [CrossRef]
- Schelenz, S.; Barnes, R.; Barton, R.C.; Cleverley, J.R.; Lucas, S.B.; Kibbler, C.C.; Denning, D.W. British Society for Medical Mycology best practice recommendations for the diagnosis of serious fungal diseases. Lancet Infect. Dis. 2015, 15, 461–474. [Google Scholar] [CrossRef]
- Ullmann, A.J.; Aguado, J.M.; Arikan-Akdagli, S.; Denning, D.W.; Groll, A.H.; Lagrou, K.; Lass-Flörl, C.; Lewis, R.E.; Munoz, P.; Verweij, P.E.; et al. Diagnosis and management of Aspergillus diseases: Executive summary of the 2017 ESCMID-ECMM-ERS guideline. Clin. Microbiol. Infect. 2018, 24 (Suppl. 1), e1–e38. [Google Scholar] [CrossRef]
- Meersseman, W.; Lagrou, K.; Maertens, J.; Wilmer, A.; Hermans, G.; Vanderschueren, S.; Spriet, I.; Verbeken, E.; Van Wijngaerden, E. Galactomannan in Bronchoalveolar Lavage Fluid: A tool for diagnosing aspergillosis in intensive care unit patients. Am. J. Respir. Crit. Care Med. 2008, 177, 27–34. [Google Scholar] [CrossRef]
- D’Haese, J.; Theunissen, K.; Vermeulen, E.; Schoemans, H.; De Vlieger, G.; Lammertijn, L.; Meersseman, P.; Meersseman, W.; Lagrou, K.; Maertens, J. Detection of Galactomannan in Bronchoalveolar Lavage Fluid Samples of Patients at Risk for Invasive Pulmonary Aspergillosis: Analytical and Clinical Validity. J. Clin. Microbiol. 2012, 50, 1258–1263. [Google Scholar] [CrossRef]
- Bassetti, M.; Bouza, E. Invasive mould infections in the ICU setting: Complexities and solutions. J. Antimicrob. Chemother. 2017, 72, i39–i47. [Google Scholar] [CrossRef]
- Cao, X.-J.; Li, Y.-P.; Xie, L.-M.; Zhang, H.-L.; Qin, Y.-S.; Guo, X.-G. Diagnostic Accuracy of Bronchoalveolar Lavage Fluid Galactomannan for Invasive Aspergillosis. BioMed Res. Int. 2020, 2020, 5434589. [Google Scholar] [CrossRef]
- Farmakiotis, D.; Le, A.; Weiss, Z.; Ismail, N.; Kubiak, D.W.; Koo, S. False positive bronchoalveolar lavage galactomannan: Effect of host and cut-off value. Mycoses 2018, 62, 204–213. [Google Scholar] [CrossRef] [PubMed]
- Izumikawa, K.; Yamamoto, Y.; Mihara, T.; Takazono, T.; Morinaga, Y.; Kurihara, S.; Nakamura, S.; Imamura, Y.; Miyazaki, T.; Nishino, T.; et al. Bronchoalveolar lavage galactomannan for the diagnosis of chronic pulmonary aspergillosis. Med. Mycol. 2012, 50, 811–817. [Google Scholar] [CrossRef]
- Sehgal, I.S.; Dhooria, S.; Choudhary, H.; Aggarwal, A.N.; Garg, M.; Chakrabarti, A.; Agarwal, R. Utility of Serum and Bronchoalveolar Lavage Fluid Galactomannan in Diagnosis of Chronic Pulmonary Aspergillosis. J. Clin. Microbiol. 2019, 57, e01821-18. [Google Scholar] [CrossRef] [PubMed]
- Fayemiwo, S.; Moore, C.B.; Foden, P.; Denning, D.W.; Richardson, M.D. Comparative performance of Aspergillus galactomannan ELISA and PCR in sputum from patients with ABPA and CPA. J. Microbiol. Methods 2017, 140, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Kawayama, T.; Fujiki, R.; Honda, J.; Rikimaru, T.; Aizawa, H. High Concentration of (1→3)-β-D-Glucan in BAL Fluid in Patients With Acute Eosinophilic Pneumonia. Chest 2003, 123, 1302–1307. [Google Scholar] [CrossRef]
- Ashitani, J.-I.; Kyoraku, Y.; Yanagi, S.; Matsumoto, N.; Nakazato, M. Elevated Levels of β-D-Glucan in Bronchoalveolar Lavage Fluid in Patients with Farmer’s Lung in Miyazaki, Japan. Respiration 2008, 75, 182–188. [Google Scholar] [CrossRef]
- Linder, K.A.; Kauffman, C.A.; Zhou, S.; Richards, B.J.; Kleiboeker, S.; Miceli, M.H. Performance of the (1,3)-Beta-d-Glucan Assay on Bronchoalveolar Lavage Fluid for the Diagnosis of Invasive Pulmonary Aspergillosis. Mycopathologia 2020, 185, 925–929. [Google Scholar] [CrossRef]
- Weinbergerova, B.; Kabut, T.; Kocmanova, I.; Lengerova, M.; Pospisil, Z.; Kral, Z.; Mayer, J. Bronchoalveolar lavage fluid and serum 1,3-β-d-glucan testing for invasive pulmonary aspergillosis diagnosis in hematological patients: The role of factors affecting assay performance. Sci. Rep. 2020, 10, 17963. [Google Scholar] [CrossRef]
- Urabe, N.; Sakamoto, S.; Sano, G.; Suzuki, J.; Hebisawa, A.; Nakamura, Y.; Koyama, K.; Ishii, Y.; Tateda, K.; Homma, S. Usefulness of Two Aspergillus PCR Assays and Aspergillus Galactomannan and β-d-Glucan Testing of Bronchoalveolar Lavage Fluid for Diagnosis of Chronic Pulmonary Aspergillosis. J. Clin. Microbiol. 2017, 55, 1738–1746. [Google Scholar] [CrossRef]
- Imbert, S.; Meyer, I.; Palous, M.; Brossas, J.-Y.; Uzunov, M.; Touafek, F.; Gay, F.; Trosini-Desert, V.; Fekkar, A. Aspergillus PCR in Bronchoalveolar Lavage Fluid for the Diagnosis and Prognosis of Aspergillosis in Patients with Hematological and Non-hematological Conditions. Front. Microbiol. 2018, 9, 1877. [Google Scholar] [CrossRef]
- Wehrle-Wieland, E.; Affolter, K.; Goldenberger, D.; Sutter, S.T.; Halter, J.; Passweg, J.; Tamm, M.; Khanna, N.; Stolz, D. Diagnosis of invasive mold diseases in patients with hematological malignancies using Aspergillus, Mucorales, and panfungal PCR in BAL. Transpl. Infect. Dis. Off. J. Transplant. Soc. 2018, 20, e12953. [Google Scholar] [CrossRef]
- Mikulska, M.; Furfaro, E.; De Carolis, E.; Drago, E.; Pulzato, I.; Borghesi, M.L.; Zappulo, E.; Raiola, A.M.; Di Grazia, C.; Del Bono, V.; et al. Use of Aspergillus fumigatus real-time PCR in bronchoalveolar lavage samples (BAL) for diagnosis of invasive aspergillosis, including azole-resistant cases, in high risk haematology patients: The need for a combined use with galactomannan. Med. Mycol. 2019, 57, 987–996. [Google Scholar] [CrossRef]
- Pelzer, B.W.; Seufert, R.; Koldehoff, M.; Liebregts, T.; Schmidt, D.; Buer, J.; Rath, P.-M.; Steinmann, J. Performance of the AsperGenius® PCR assay for detecting azole resistant Aspergillus fumigatus in BAL fluids from allogeneic HSCT recipients: A prospective cohort study from Essen, West Germany. Med. Mycol. 2020, 58, 268–271. [Google Scholar] [CrossRef]
- Mikulska, M.; Furfaro, E.; Dettori, S.; Giacobbe, D.R.; Magnasco, L.; Dentone, C.; Ball, L.; Russo, C.; Taramasso, L.; Vena, A.; et al. Aspergillus-PCR in bronchoalveolar lavage-diagnostic accuracy for invasive pulmonary aspergillosis in critically ill patients. Mycoses 2022, 65, 411–418. [Google Scholar] [CrossRef]
- Peng, J.-M.; Du, B.; Qin, H.-Y.; Wang, Q.; Shi, Y. Metagenomic next-generation sequencing for the diagnosis of suspected pneumonia in immunocompromised patients. J. Infect. 2021, 82, 22–27. [Google Scholar] [CrossRef]
- Dobiáš, R.; Jaworská, P.; Skopelidou, V.; Strakoš, J.; Višňovská, D.; Káňová, M.; Škríba, A.; Lysková, P.; Bartek, T.; Janíčková, I.; et al. Distinguishing invasive from chronic pulmonary infections: Host pentraxin 3 and fungal siderophores in bronchoalveolar lavage fluids. J. Fungi 2022, 8, 1194. [Google Scholar] [CrossRef]
- Kabbani, D.; Bhaskaran, A.; Singer, L.; Bhimji, A.; Rotstein, C.; Keshavjee, S.; Liles, W.C.; Husain, S. Pentraxin 3 levels in bronchoalveolar lavage fluid of lung transplant recipients with invasive aspergillosis. J. Heart Lung Transplant. 2017, 36, 973–979. [Google Scholar] [CrossRef]
- Takazono, T.; Izumikawa, K. Recent Advances in Diagnosing Chronic Pulmonary Aspergillosis. Front. Microbiol. 2018, 9, 1810. [Google Scholar] [CrossRef]
- Shin, B.; Koh, W.-J.; Jeong, B.-H.; Yoo, H.; Park, H.Y.; Suh, G.Y.; Kwon, O.J.; Jeon, K. Serum galactomannan antigen test for the diagnosis of chronic pulmonary aspergillosis. J. Infect. 2014, 68, 494–499. [Google Scholar] [CrossRef]
- Dobias, R.; Jaworska, P.; Tomaskova, H.; Kanova, M.; Lyskova, P.; Vrba, Z.; Holub, C.; Svobodová, L.; Hamal, P.; Raska, M. Diagnostic value of serum galactomannan, (1,3)-β-d -glucan, and Aspergillus fumigatus-specific IgA and IgG assays for invasive pulmonary aspergillosis in non-neutropenic patients. Mycoses 2018, 61, 576–586. [Google Scholar] [CrossRef]
- Dobias, R.; Filip, M.; Vragova, K.; Dolinska, D.; Zavodna, P.; Dujka, A.; Linzer, P.; Jurek, P.; Studena, B.; Cerna, E.; et al. Successful surgical excision of cerebral abscess caused by Fonsecaea monophora in an immunocompetent patient and review of literature. Folia Microbiol. 2018, 64, 383–388. [Google Scholar] [CrossRef] [PubMed]
- Dobiáš, R.; Káňová, M.; Petejová, N.; Pisti, Š.K.; Bocek, R.; Krejčí, E.; Stružková, H.; Cachová, M.; Tomášková, H.; Hamal, P.; et al. Combined Use of Presepsin and (1,3)-β-D-glucan as Biomarkers for Diagnosing Candida Sepsis and Monitoring the Effectiveness of Treatment in Critically Ill Patients. J. Fungi 2022, 8, 308. [Google Scholar] [CrossRef] [PubMed]
- Karageorgopoulos, D.; Qu, J.-M.; Korbila, I.; Zhu, Y.-G.; Vasileiou, V.; Falagas, M. Accuracy of β-D-glucan for the diagnosis of Pneumocystis jirovecii pneumonia: A meta-analysis. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2013, 19, 39–49. [Google Scholar] [CrossRef]
- White, P.L.; Linton, C.J.; Perry, M.D.; Johnson, E.M.; Barnes, R.A. The Evolution and Evaluation of a Whole Blood Polymerase Chain Reaction Assay for the Detection of Invasive Aspergillosis in Hematology Patients in a Routine Clinical Setting. Clin. Infect. Dis. 2006, 42, 479–486. [Google Scholar] [CrossRef]
- Mengoli, C.; Cruciani, M.; Barnes, R.; Loeffler, J.; Donnelly, J.P. Use of PCR for diagnosis of invasive aspergillosis: Systematic review and meta-analysis. Lancet Infect. Dis. 2009, 9, 89–96. [Google Scholar] [CrossRef] [PubMed]
- White, P.L.; Mengoli, C.; Bretagne, S.; Cuenca-Estrella, M.; Finnstrom, N.; Klingspor, L.; Melchers, W.J.G.; McCulloch, E.; Barnes, R.A.; Donnelly, J.P.; et al. Evaluation of Aspergillus PCR Protocols for Testing Serum Specimens. J. Clin. Microbiol. 2011, 49, 3842–3848. [Google Scholar] [CrossRef]
- Springer, J.; Morton, C.O.; Perry, M.; Heinz, W.J.; Paholcsek, M.; Alzheimer, M.; Rogers, T.R.; Barnes, R.A.; Einsele, H.; Loeffler, J.; et al. Multicenter Comparison of Serum and Whole-Blood Specimens for Detection of Aspergillus DNA in High-Risk Hematological Patients. J. Clin. Microbiol. 2013, 51, 1445–1450. [Google Scholar] [CrossRef]
- White, P.L.; Barnes, R.A.; Springer, J.; Klingspor, L.; Cuenca-Estrella, M.; Morton, C.O.; Lagrou, K.; Bretagne, S.; Melchers, W.J.G.; Mengoli, C.; et al. Clinical Performance of Aspergillus PCR for Testing Serum and Plasma: A Study by the European Aspergillus PCR Initiative. J. Clin. Microbiol. 2015, 53, 2832–2837. [Google Scholar] [CrossRef]
- Springer, J.; White, P.L.; Hamilton, S.; Michel, D.; Barnes, R.A.; Einsele, H.; Löffler, J. Comparison of Performance Characteristics of Aspergillus PCR in Testing a Range of Blood-Based Samples in Accordance with International Methodological Recommendations. J. Clin. Microbiol. 2016, 54, 705–711. [Google Scholar] [CrossRef]
- White, P.L.; Wiederhold, N.P.; Loeffler, J.; Najvar, L.K.; Melchers, W.; Herrera, M.; Bretagne, S.; Wickes, B.; Kirkpatrick, W.R.; Barnes, R.A.; et al. Comparison of Nonculture Blood-Based Tests for Diagnosing Invasive Aspergillosis in an Animal Model. J. Clin. Microbiol. 2016, 54, 960–966. [Google Scholar] [CrossRef]
- Ma, X.; Zhang, S.; Xing, H.; Li, H.; Chen, J.; Li, H.; Jiao, M.; Shi, Q.; Xu, A.; Xing, L.; et al. Invasive Pulmonary Aspergillosis Diagnosis via Peripheral Blood Metagenomic Next-Generation Sequencing. Front. Med. 2022, 9, 751617. [Google Scholar] [CrossRef]
- Hogan, C.; Yang, S.; Garner, O.B.; Green, D.; Gomez, C.; Bard, J.D.; Pinsky, B.; Banaei, N. Clinical Impact of Metagenomic Next-Generation Sequencing of Plasma Cell-Free DNA for the Diagnosis of Infectious Diseases: A Multicenter Retrospective Cohort Study. Clin. Infect. Dis. 2020, 72, 239–245. [Google Scholar] [CrossRef]
- Heldt, S.; Hoenigl, M. Lateral Flow Assays for the Diagnosis of Invasive Aspergillosis: Current Status. Curr. Fungal Infect. Rep. 2017, 11, 45–51. [Google Scholar] [CrossRef]
- Thornton, C.R. Development of an Immunochromatographic Lateral-Flow Device for Rapid Serodiagnosis of Invasive Aspergillosis. Clin. Vaccine Immunol. 2008, 15, 1095–1105. [Google Scholar] [CrossRef]
- Held, J.; Schmidt, T.; Thornton, C.R.; Kotter, E.; Bertz, H. Comparison of a novel Aspergillus lateral-flow device and the Platelia® galactomannan assay for the diagnosis of invasive aspergillosis following haematopoietic stem cell transplantation. Infection 2013, 41, 1163–1169. [Google Scholar] [CrossRef]
- White, P.L.; Parr, C.; Thornton, C.; Barnes, R.A. Evaluation of Real-Time PCR, Galactomannan Enzyme-Linked Immunosorbent Assay (ELISA), and a Novel Lateral-Flow Device for Diagnosis of Invasive Aspergillosis. J. Clin. Microbiol. 2013, 51, 1510–1516. [Google Scholar] [CrossRef]
- Latgé, J.-P.; Chamilos, G. Aspergillus fumigatus and Aspergillosis in 2019. Clin. Microbiol. Rev. 2019, 33, e00140-18. [Google Scholar] [CrossRef]
- Stevens, D.A.; Moss, R.B.; Kurup, V.P.; Knutsen, A.P.; Greenberger, P.; Judson, M.; Denning, D.; Crameri, R.; Brody, A.S.; Light, M.; et al. Allergic Bronchopulmonary Aspergillosis in Cystic Fibrosis—State of the Art: Cystic Fibrosis Foundation Consensus Conference. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2003, 37, S225–S264. [Google Scholar] [CrossRef]
- Muthu, V.; Singh, P.; Choudhary, H.; Sehgal, I.S.; Dhooria, S.; Prasad, K.T.; Aggarwal, A.N.; Garg, M.; Chakrabarti, A.; Agarwal, R. Diagnostic Cutoffs and Clinical Utility of Recombinant Aspergillus fumigatus Antigens in the Diagnosis of Allergic Bronchopulmonary Aspergillosis. J. Allergy Clin. Immunol. Pract. 2020, 8, 579–587. [Google Scholar] [CrossRef]
- Seo, H.; Kang, S.; Park, Y.-S.; Yun, C.-W. The Role of Zinc in Gliotoxin Biosynthesis of Aspergillus fumigatus. Int. J. Mol. Sci. 2019, 20, 6192. [Google Scholar] [CrossRef]
- Savelieff, M.; Pappalardo, L. Novel cutting-edge metabolite-based diagnostic tools for aspergillosis. PLoS Pathog. 2017, 13, e1006486. [Google Scholar] [CrossRef] [PubMed]
- Mercier, T.; Sharpe, A.R.; Waumans, D.; Desmet, K.; Lagrou, K.; Maertens, J. Gliotoxin and bis(methylthio)gliotoxin are not reliable as biomarkers of invasive aspergillosis. Mycoses 2019, 62, 945–948. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Lopez, A.; Rueda, C.; Pozo, R.P.; Gonzalez, L.M.S. Dynamics of gliotoxin and bis(methylthio)gliotoxin production during the course of Aspergillus fumigatus infection. Med. Mycol. 2022, 60, myac025. [Google Scholar] [CrossRef]
- Luptáková, D.; Patil, H.R.; Dobiáš, R.; Stevens, D.A.; Pluháček, T.; Palyzová, A.; Káňová, M.; Navrátil, M.; Vrba, Z.; Hubáček, P.; et al. Siderophore-based noninvasive differentiation of Aspergillus fumigatus colonization and invasion in pulmonary aspergillosis. Microbiol. Spectr. 2023, e04068-22. [Google Scholar] [CrossRef] [PubMed]
- Mehdiratta, K.; Singh, S.; Sharma, S.; Bhosale, R.S.; Choudhury, R.; Masal, D.P.; Manocha, A.; Dhamale, B.D.; Khan, N.; Asokachandran, V.; et al. Kupyaphores are zinc homeostatic metallophores required for colonization of Mycobacterium tuberculosis. Proc. Natl. Acad. Sci. USA 2022, 119, e2110293119. [Google Scholar] [CrossRef]
- Golonka, R.; Yeoh, B.S.; Vijay-Kumar, M. The Iron Tug-of-War between Bacterial Siderophores and Innate Immunity. J. Innate Immun. 2019, 11, 249–262. [Google Scholar] [CrossRef]
- Abergel, R.J.; Wilson, M.K.; Arceneaux, J.E.L.; Hoette, T.M.; Strong, R.K.; Byers, B.R.; Raymond, K.N. Anthrax pathogen evades the mammalian immune system through stealth siderophore production. Proc. Natl. Acad. Sci. USA 2006, 103, 18499–18503. [Google Scholar] [CrossRef]
- Danion, F.; van Rhijn, N.; Dufour, A.C.; Legendre, R.; Sismeiro, O.; Varet, H.; Olivo-Marin, J.-C.; Mouyna, I.; Chamilos, G.; Bromley, M.; et al. Aspergillus fumigatus, One Uninucleate Species with Disparate Offspring. J. Fungi 2021, 7, 30. [Google Scholar] [CrossRef]
- Kriegl, L.; Havlicek, V.; Dichtl, K.; Egger, M.; Hoenigl, M. Siderophores: A potential role as a diagnostic for invasive fungal disease. Curr. Opin. Infect. Dis. 2022, 35, 485–492. [Google Scholar] [CrossRef]
- Petřík, M.; Palyzová, A.; Nový, Z.; Houšť, J.; Havlíček, V.; Khoylou, M.; Popper, M.; Bendová, K.; Haas, H.; Decristoforo, C.; et al. Monitoring Aspergillus fumigatus infection in rats using(68)Ga-siderophores. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, S18. [Google Scholar]
- Petrik, M.; Haas, H.; Dobrozemsky, G.; Lass-Flörl, C.; Helbok, A.; Blatzer, M.; Dietrich, H.; Decristoforo, C. 68Ga-Siderophores for PET Imaging of Invasive Pulmonary Aspergillosis: Proof of Principle. J. Nucl. Med. 2010, 51, 639–645. [Google Scholar] [CrossRef]
- Patil, R.H.; Luptáková, D.; Havlíček, V. Infection metallomics for critical care in the post-COVID era. Mass Spectrom. Rev. 2021. [Google Scholar] [CrossRef]
- Novák, J.; Škríba, A.; Havlíček, V. CycloBranch 2: Molecular Formula Annotations Applied to imzML Data Sets in Bimodal Fusion and LC-MS Data Files. Anal. Chem. 2020, 92, 6844–6849. [Google Scholar] [CrossRef]
- Dobiáš, R.; Jahn, P.; Tóthová, K.; Dobešová, O.; Višňovská, D.; Patil, R.; Škríba, A.; Jaworská, P.; Škorič, M.; Podojil, L.; et al. Diagnosis of Aspergillosis in Horses. J. Fungi 2023, 9, 161. [Google Scholar] [CrossRef]
- Dobiáš, R.; Škríba, A.; Pluháček, T.; Petřík, M.; Palyzová, A.; Káňová, M.; Čubová, E.; Houšť, J.; Novák, J.; Stevens, D.A.; et al. Noninvasive Combined Diagnosis and Monitoring of Aspergillus and Pseudomonas Infections: Proof of Concept. J. Fungi 2021, 7, 730. [Google Scholar] [CrossRef]
- Le Govic, Y.; Havlíček, V.; Capilla, J.; Luptáková, D.; Dumas, D.; Papon, N.; Le Gal, S.; Bouchara, J.-P.; Vandeputte, P. Synthesis of the Hydroxamate Siderophore Nα-Methylcoprogen B in Scedosporium apiospermum Is Mediated by sidD Ortholog and Is Required for Virulence. Front. Cell. Infect. Microbiol. 2020, 10, 587909. [Google Scholar] [CrossRef]
- Luptáková, D.; Pluháček, T.; Petřík, M.; Novák, J.; Palyzová, A.; Sokolová, L.; Škríba, A.; Šedivá, B.; Lemr, K.; Havlíček, V. Non-invasive and invasive diagnoses of aspergillosis in a rat model by mass spectrometry. Sci. Rep. 2017, 7, 16523. [Google Scholar] [CrossRef]
- Patil, R.H.; Kotta-Loizou, I.; Palyzová, A.; Pluháček, T.; Coutts, R.H.A.; Stevens, D.A.; Havlíček, V. Freeing Aspergillus fumigatus of polymycovirus infection renders it more resistant to competition with Pseudomonas aeruginosa due to altered iron-acquiring tactics. J. Fungi 2021, 7, 497. [Google Scholar] [CrossRef]
- Matthaiou, E.I.; Sass, G.; Stevens, D.A.; Hsu, J.L. Iron: An essential nutrient for Aspergillus fumigatus and a fulcrum for pathogenesis. Curr. Opin. Infect. Dis. 2018, 31, 506–511. [Google Scholar] [CrossRef]
- Vidal-García, M.; Redrado, S.; Domingo, M.P.; Marquina, P.; Colmenarejo, C.; Meis, J.F.; Rezusta, A.; Pardo, J.; Galvez, E.M. Production of the Invasive Aspergillosis Biomarker Bis(methylthio)gliotoxin within the Genus Aspergillus: In Vitro and in Vivo Metabolite Quantification and Genomic Analysis. Front. Microbiol. 2018, 9, 1246. [Google Scholar] [CrossRef]
- Škríba, A.; Pluhacek, T.; Palyzova, A.; Novy, Z.; Lemr, K.; Hajduch, M.; Petrik, M.; Havlicek, V. Early and Non-invasive Diagnosis of Aspergillosis Revealed by Infection Kinetics Monitored in a Rat Model. Front. Microbiol. 2018, 9, 2356. [Google Scholar] [CrossRef] [PubMed]
- Orasch, T.; Prattes, J.; Faserl, K.; Eigl, S.; Düttmann, W.; Lindner, H.; Haas, H.; Hoenigl, M. Bronchoalveolar lavage triacetylfusarinine C (TAFC) determination for diagnosis of invasive pulmonary aspergillosis in patients with hematological malignancies. J. Infect. 2017, 75, 370–373. [Google Scholar] [CrossRef] [PubMed]
- Raffa, N.; Won, T.H.; Sukowaty, A.; Candor, K.; Cui, C.; Halder, S.; Dai, M.; Landero-Figueroa, J.A.; Schroeder, F.C.; Keller, N.P. Dual-purpose isocyanides produced by Aspergillus fumigatus contribute to cellular copper sufficiency and exhibit antimicrobial activity. Proc. Natl. Acad. Sci. USA 2021, 118, e2015224118. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Risk Group | Aspergillus Infection, % |
|---|---|
| Acute leukemia | 100 |
| Solid cancer | 0 |
| Neutropenia only | 94 |
| Neutropenia or bone marrow transplant | 72 |
| Bone marrow transplant only | 82 |
| Corticosteroids | 63–65 |
| Antibiotics | 39 |
| HIV | 14 |
| Solid organ transplant | 56 |
| Chronic obstructive lung disease | 15–22 |
| Non-neutropenic, mechanically ventilated, ICU | 20 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dobiáš, R.; Stevens, D.A.; Havlíček, V. Current and Future Pathways in Aspergillus Diagnosis. Antibiotics 2023, 12, 385. https://doi.org/10.3390/antibiotics12020385
Dobiáš R, Stevens DA, Havlíček V. Current and Future Pathways in Aspergillus Diagnosis. Antibiotics. 2023; 12(2):385. https://doi.org/10.3390/antibiotics12020385
Chicago/Turabian StyleDobiáš, Radim, David A. Stevens, and Vladimír Havlíček. 2023. "Current and Future Pathways in Aspergillus Diagnosis" Antibiotics 12, no. 2: 385. https://doi.org/10.3390/antibiotics12020385
APA StyleDobiáš, R., Stevens, D. A., & Havlíček, V. (2023). Current and Future Pathways in Aspergillus Diagnosis. Antibiotics, 12(2), 385. https://doi.org/10.3390/antibiotics12020385