

Antibiotic Utilization during COVID-19: Are We Over-Prescribing?
 , ,
, ,  ,
,  and
and
Abstract
:1. Introduction
2. Results
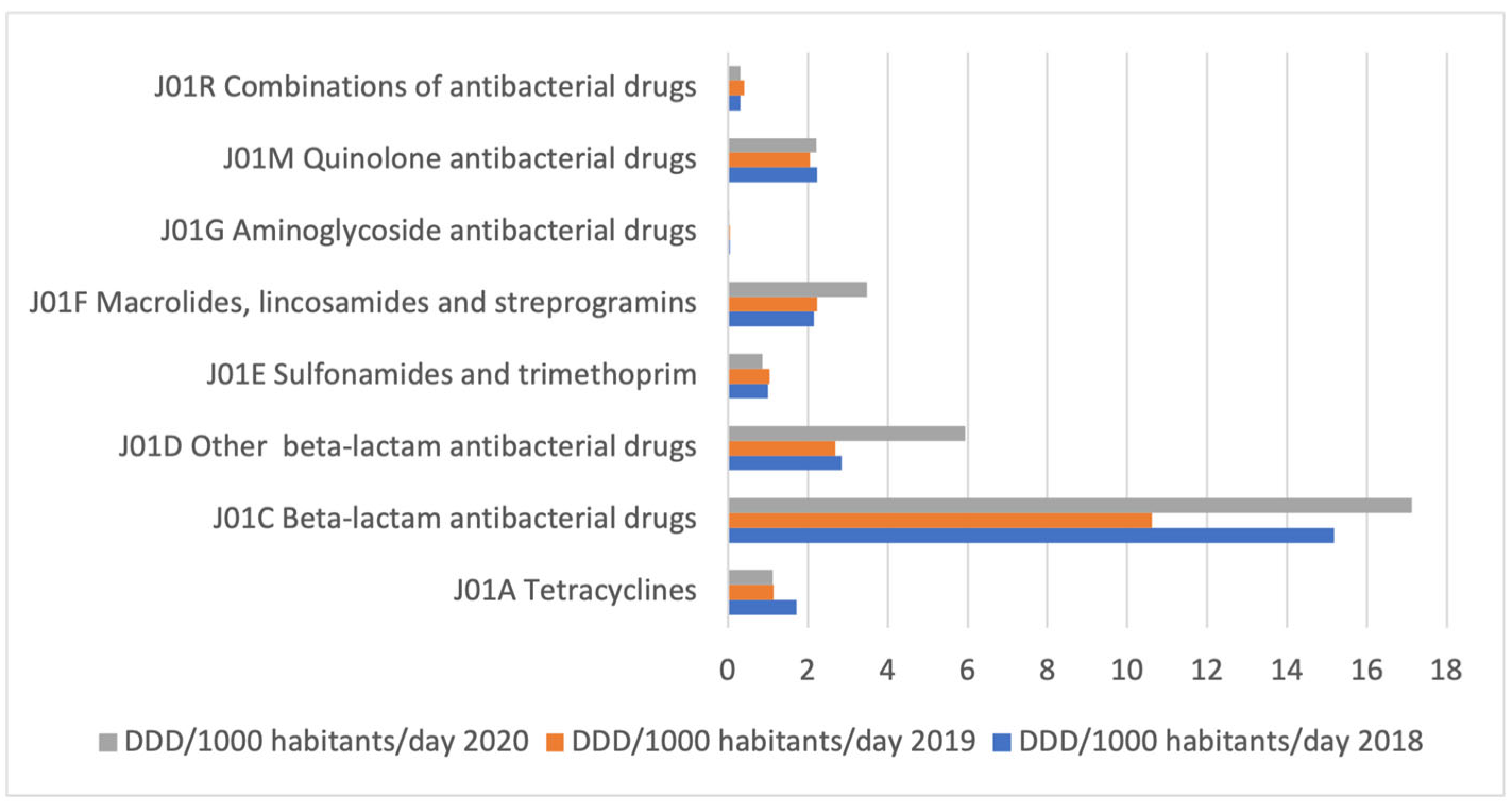
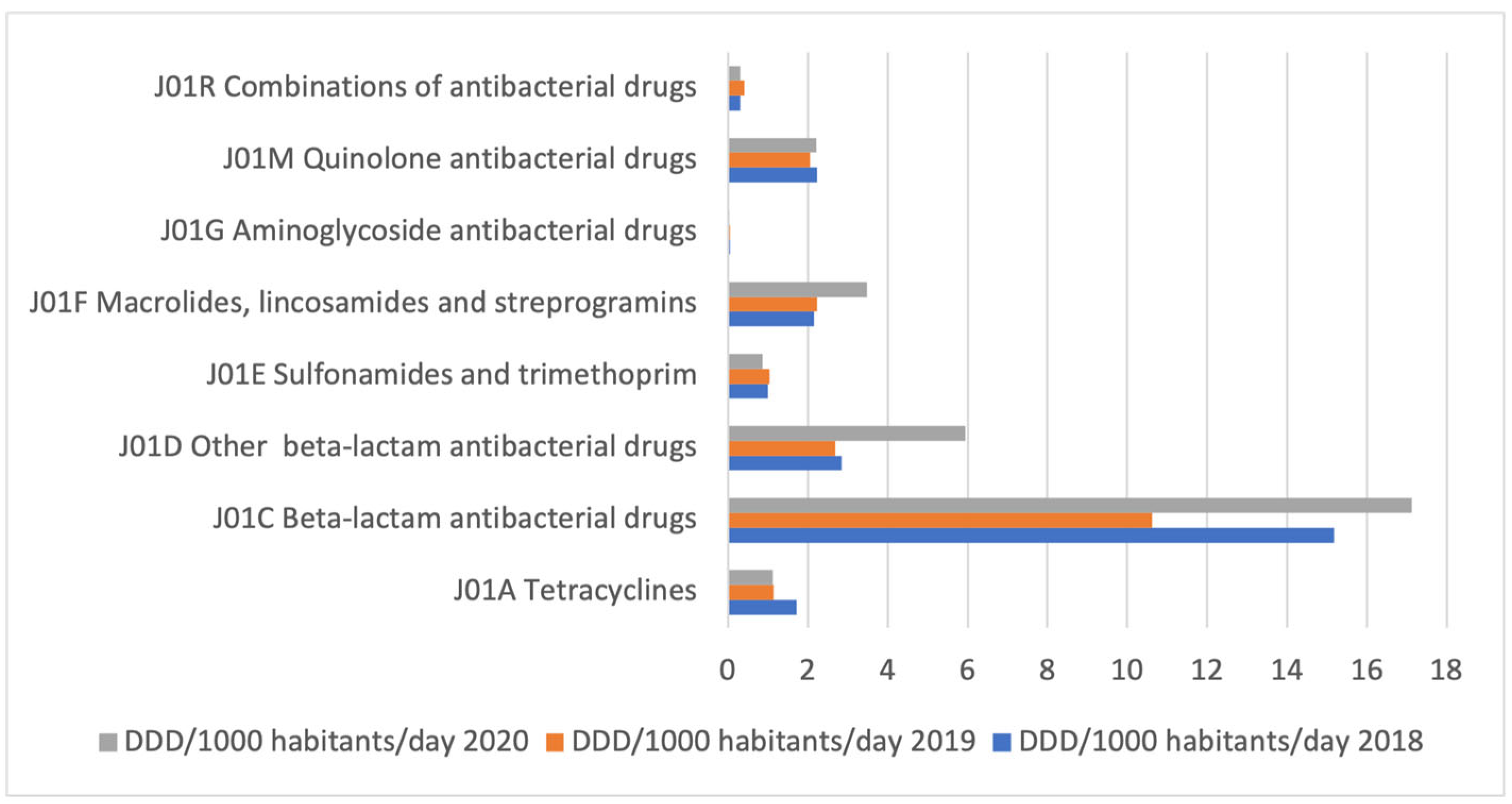
2.1. Medicine Utilization
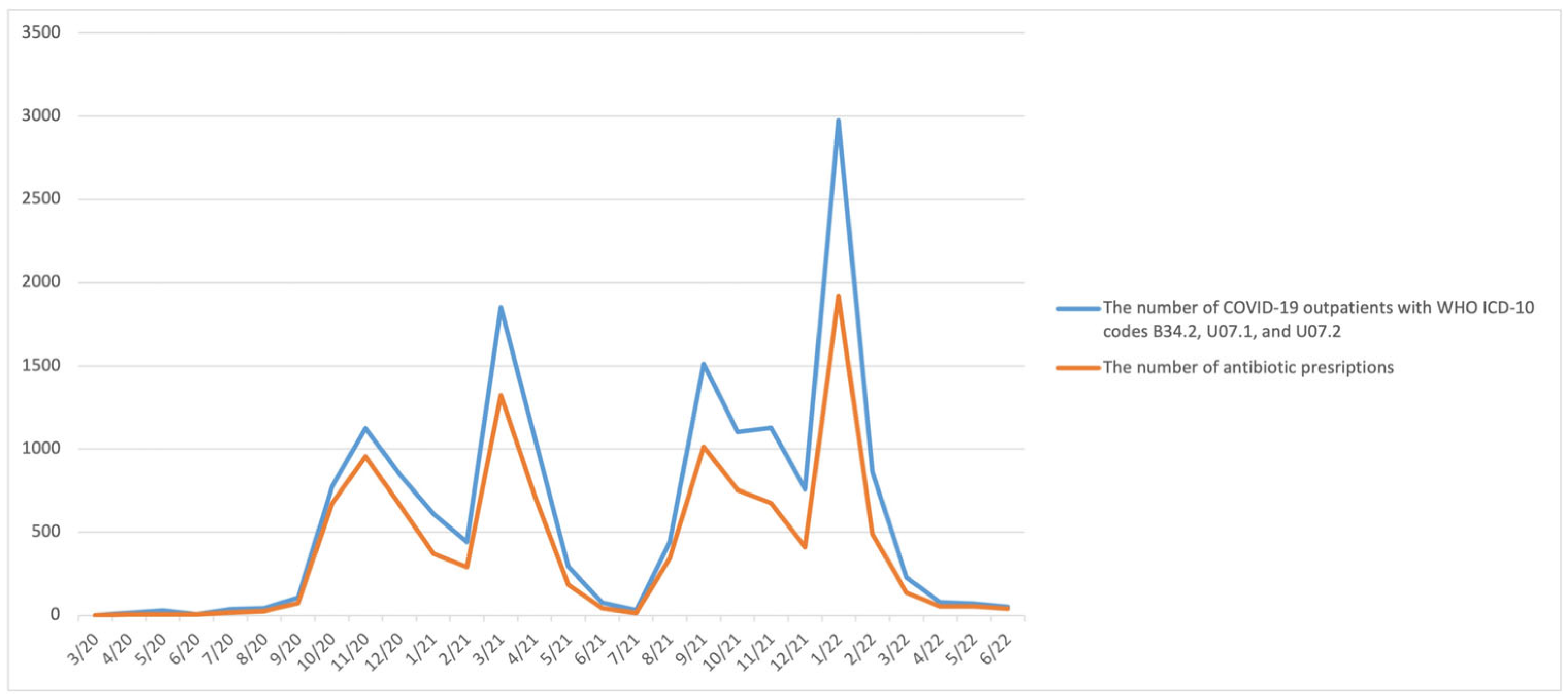
2.2. Medical Records
3. Discussion
4. Strength and Limitations
5. Materials and Methods
5.1. Medicine Utilization
5.2. Medical Records
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Singh, T.U.; Parida, S.; Lingaraju, M.C.; Kesavan, M.; Kumar, D.; Singh, R.K. Drug repurposing approach to fight COVID-19. Pharmacol. Rep. 2020, 72, 1479–1508. [Google Scholar] [PubMed]
- Adebisi, Y.A.; Jimoh, N.D.; Ogunkola, I.O.; Uwizeyimana, T.; Olayemi, A.H.; Ukor, N.A.; Lucero-Prisno, D.E. The use of antibiotics in COVID-19 management: A rapid review of national treatment guidelines in 10 African countries. Trop. Med. Health 2021, 49, 51. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.-C.; Chen, S.-Y.; Ko, W.-C.; Hsueh, P.-R. Increased antimicrobial resistance during the COVID-19 pandemic. Int. J. Antimicrob. Agents 2021, 57, 106324. [Google Scholar] [CrossRef] [PubMed]
- Van Duin, D.; Barlow, G.; Nathwani, D. The impact of the COVID-19 pandemic on antimicrobial resistance: A debate. JAC-Antimicrob. Resist. 2020, 3, dlaa053. [Google Scholar] [CrossRef]
- Loganathan, B.; Phillips, M.; Mowery, H.; Jones-Lepp, T.L. Contamination profiles and mass loadings of macrolide antibiotics and illicit drugs from a small urban wastewater treatment plant. Chemosphere 2009, 75, 70–77. [Google Scholar] [CrossRef]
- Al Bahar, F.; Curtis, C.E.; Alhamad, H.; Marriott, J.F. The impact of a computerised decision support system on antibiotic usage in an English hospital. Int. J. Clin. Pharm. 2020, 42, 765–771. [Google Scholar] [CrossRef]
- World Health Organization. Living guideline, 23 June 2022. In Clinical Management of COVID-19; WHO: Geneva, Switzerland, 2022. [Google Scholar]
- World Health Organization. Living guidance, 25 January 2021. In COVID-19 Clinical Management; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- World Health Organization. Interim guidance, 27 May 2020. In Clinical Management of COVID-19; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Soucy, J.-P.R.; Westwood, D.; Daneman, N.; MacFadden, D.R. Antibiotic prescribing in patients with COVID-19: Rapid review and meta-analysis. Clin. Microbiol. Infect. 2021, 27, 520–531. [Google Scholar] [CrossRef]
- Neto, A.G.M.; Lo, K.B.; Wattoo, A.; Salacup, G.; Pelayo, J.; DeJoy, R.; Bhargav, R.; Gul, F.; Peterson, E.; Albano, J. Bacterial infections and patterns of antibiotic use in patients with COVID-19. J. Med. Virol. 2021, 93, 1489–1495. [Google Scholar] [CrossRef]
- Karami, Z.; Knoop, B.T.; Dofferhoff, A.S.M.; Blaauw, M.J.T.; Janssen, N.A.; van Apeldoorn, M.; Kerckhoffs, A.P.M.; van de Maat, J.S.; Hoogerwerf, J.J.; Ten Oever, J. Few bacterial co-infections but frequent empiric antibiotic use in the early phase of hospitalized patients with COVID-19: Results from a multicentre retrospective cohort study in The Netherlands. Infect. Dis. 2021, 53, 102–110. [Google Scholar] [CrossRef]
- Karaba, S.M.; Jones, G.; Helsel, T.; Smith, L.L.; Avery, R.; Dzintars, K.; Salinas, A.B.; Keller, S.C.; Townsend, J.L.; Klein, E. Prevalence of co-infection at the time of hospital admission in COVID-19 patients, a multicenter study. In Proceedings of the Open Forum Infectious Diseases; Oxford University Press: Oxford, UK, 2021; Volume 8, p. ofaa578. [Google Scholar]
- Crisafulli, S.; Ientile, V.; L’Abbate, L.; Fontana, A.; Linguiti, C.; Manna, S.; Mercaldo, M.; Pagliaro, C.; Vezzaro, M.; Santacà, K. COVID-19 Patient Management in Outpatient Setting: A Population-Based Study from Southern Italy. J. Clin. Med. 2021, 11, 51. [Google Scholar] [CrossRef]
- Belleudi, V.; Finocchietti, M.; Fortinguerra, F.; Di Filippo, A.; Trotta, F.; Davoli, M.; Addis, A. Drug prescriptions in the outpatient management of Covid-19: Evidence-based recommendations versus real practice. Front. Pharmacol. 2022, 13, 825479. [Google Scholar] [CrossRef]
- Zhu, N.; Aylin, P.; Rawson, T.; Gilchrist, M.; Majeed, A.; Holmes, A. Investigating the impact of COVID-19 on primary care antibiotic prescribing in North West London across two epidemic waves. Clin. Microbiol. Infect. 2021, 27, 762–768. [Google Scholar] [CrossRef]
- Lepak, A.J.; Taylor, L.N.; Stone, C.A.; Schulz, L.T.; Anderson, M.C.; Fox, B.C.; Temte, J.L. Association of changes in seasonal respiratory virus activity and ambulatory antibiotic prescriptions with the COVID-19 pandemic. JAMA Intern. Med. 2021, 181, 1399–1402. [Google Scholar] [CrossRef] [PubMed]
- Gillies, M.B.; Burgner, D.P.; Ivancic, L.; Nassar, N.; Miller, J.E.; Sullivan, S.G.; Todd, I.M.F.; Pearson, S.; Schaffer, A.L.; Zoega, H. Changes in antibiotic prescribing following COVID-19 restrictions: Lessons for post-pandemic antibiotic stewardship. Br. J. Clin. Pharmacol. 2022, 88, 1143–1151. [Google Scholar] [CrossRef] [PubMed]
- Buehrle, D.J.; Wagener, M.M.; Nguyen, M.H.; Clancy, C.J. Trends in outpatient antibiotic prescriptions in the United States during the COVID-19 pandemic in 2020. JAMA Netw. Open 2021, 4, e2126114. [Google Scholar] [CrossRef]
- Malcolm, W.; Seaton, R.A.; Haddock, G.; Baxter, L.; Thirlwell, S.; Russell, P.; Cooper, L.; Thomson, A.; Sneddon, J. Impact of the COVID-19 pandemic on community antibiotic prescribing in Scotland. JAC-Antimicrob. Resist. 2020, 2, dlaa105. [Google Scholar] [CrossRef] [PubMed]
- Silva, T.M.; Estrela, M.; Gomes, E.R.; Piñeiro-Lamas, M.; Figueiras, A.; Roque, F.; Herdeiro, M.T. The impact of the COVID-19 pandemic on antibiotic prescribing trends in outpatient care: A nationwide, quasi-experimental approach. Antibiotics 2021, 10, 1040. [Google Scholar] [CrossRef]
- Bara, W.; Brun-Buisson, C.; Coignard, B.; Watier, L. Outpatient Antibiotic Prescriptions in France: Patients and Providers Characteristics and Impact of the COVID-19 Pandemic. Antibiotics 2022, 11, 643. [Google Scholar] [CrossRef]
- Andrews, A.; Budd, E.L.; Hendrick, A.; Ashiru-Oredope, D.; Beech, E.; Hopkins, S.; Gerver, S.; Muller-Pebody, B.; Group, A.M.U.C. Surveillance of antibacterial usage during the COVID-19 pandemic in England, 2020. Antibiotics 2021, 10, 841. [Google Scholar] [CrossRef]
- Knight, B.D.; Shurgold, J.; Smith, G.; MacFadden, D.R.; Schwartz, K.L.; Daneman, N.; Tropper, D.G.; Brooks, J. The impact of COVID-19 on community antibiotic use in Canada: An ecological study. Clin. Microbiol. Infect. 2022, 28, 426–432. [Google Scholar] [CrossRef]
- Kitano, T.; Brown, K.A.; Daneman, N.; MacFadden, D.R.; Langford, B.J.; Leung, V.; So, M.; Leung, E.; Burrows, L.; Manuel, D. The impact of COVID-19 on outpatient antibiotic prescriptions in Ontario, Canada; An interrupted time series analysis. In Proceedings of the Open Forum Infectious Diseases; Oxford University Press: Oxford, UK, 2021; Volume 8, p. ofab533. [Google Scholar]
- Blix, H.S.; Høye, S. Use of antibiotics during the COVID-19 pandemic. Tidsskr. Nor. Legeforening 2021. [Google Scholar] [CrossRef] [PubMed]
- Al-Azzam, S.; Mhaidat, N.M.; Banat, H.A.; Alfaour, M.; Ahmad, D.S.; Muller, A.; Al-Nuseirat, A.; Lattyak, E.A.; Conway, B.R.; Aldeyab, M.A. An assessment of the impact of coronavirus disease (COVID-19) pandemic on national antimicrobial consumption in Jordan. Antibiotics 2021, 10, 690. [Google Scholar] [CrossRef] [PubMed]
- Faculty of Medicine. Priručnik Za Liječenje Infekcije Izazvane Novim Virusom Korona, 1. Izdanje. Available online: https://www.vladars.net/sr-SP-Cyrl/Vlada/Ministarstva/MZSZ/Pages/default.aspx (accessed on 16 December 2022).
- Faculty of Medicine. Priručnik Za Liječenje Infekcije Izazvane Novim Virusom Korona, 3. Izdanje. Available online: https://www.vladars.net/sr-SP-Cyrl/Vlada/Ministarstva/MZSZ/Pages/default.aspx (accessed on 16 December 2022).
- Faculty of Medicine. Priručnik Za Liječenje Pacijenata Sa COVID-19, 4. Izdanje. Available online: https://med.unibl.org/wp-content/uploads/2021/02/COVID-19-Smjernice-IV-izdanje.pdf?fbclid=IwAR3sb1nR7ix7Yf0I2JJkHpZEiSeAh6nS5ktMJ3FDF_nYbc7yBdSmRhVjNr0 (accessed on 16 December 2022).
- European Centre for Disease Prevention and Control Antimicrobial Consumption Dashboard (ESAC-Net). Available online: https://qap.ecdc.europa.eu/public/extensions/AMC2_Dashboard/AMC2_Dashboard.html#eu-consumption-tab (accessed on 12 December 2022).
- Llor, C.; Bjerrum, L. Antimicrobial resistance: Risk associated with antibiotic overuse and initiatives to reduce the problem. Ther. Adv. Drug Saf. 2014, 5, 229–241. [Google Scholar] [CrossRef] [PubMed]
- Hashmi, H.; Sasoli, N.A.; Sadiq, A.; Raziq, A.; Batool, F.; Raza, S.; Iqbal, Q.; Haider, S.; Umer, S.; Mengal, M.A. Prescribing patterns for Upper Respiratory Tract Infections: A prescription-review of primary care practice in Quetta, Pakistan and the implications. Front. Public Health 2021, 9, 787933. [Google Scholar] [CrossRef] [PubMed]
- Lakkis, N.A.; Alameddine, R.; Issa, H.G.; Mahmassani, D.; Osman, M.H. Prescribing antibiotics in adults with respiratory tract infections in Lebanon. Int. J. Clin. Pract. 2021, 75, e14514. [Google Scholar] [CrossRef] [PubMed]
- Yanagihara, K.; Kohno, S.; Matsusima, T. Japanese guidelines for the management of community-acquired pneumonia. Int. J. Antimicrob. Agents 2001, 18, 45–48. [Google Scholar] [CrossRef]
- Huang, F.; Zhang, C.; Liu, Q.; Zhao, Y.; Zhang, Y.; Qin, Y.; Li, X.; Li, C.; Zhou, C.; Jin, N. Identification of amitriptyline HCl, flavin adenine dinucleotide, azacitidine and calcitriol as repurposing drugs for influenza A H5N1 virus-induced lung injury. PLoS Pathog. 2020, 16, e1008341. [Google Scholar] [CrossRef]
- Gautret, P.; Lagier, J.-C.; Parola, P.; Meddeb, L.; Mailhe, M.; Doudier, B.; Courjon, J.; Giordanengo, V.; Vieira, V.E.; Dupont, H.T. Hydroxychloroquine and azithromycin as a treatment of COVID-19: Results of an open-label non-randomized clinical trial. Int. J. Antimicrob. Agents 2020, 56, 105949. [Google Scholar] [CrossRef]
- Hinks, T.S.C.; Cureton, L.; Knight, R.; Wang, A.; Cane, J.L.; Barber, V.S.; Black, J.; Dutton, S.J.; Melhorn, J.; Jabeen, M. Azithromycin versus standard care in patients with mild-to-moderate COVID-19 (ATOMIC2): An open-label, randomised trial. Lancet Respir. Med. 2021, 9, 1130–1140. [Google Scholar] [CrossRef]
- Butler, C.C.; Dorward, J.; Yu, L.-M.; Gbinigie, O.; Hayward, G.; Saville, B.R.; Van Hecke, O.; Berry, N.; Detry, M.; Saunders, C. Azithromycin for community treatment of suspected COVID-19 in people at increased risk of an adverse clinical course in the UK (PRINCIPLE): A randomised, controlled, open-label, adaptive platform trial. Lancet 2021, 397, 1063–1074. [Google Scholar] [CrossRef]
- Gendrot, M.; Andreani, J.; Jardot, P.; Hutter, S.; Delandre, O.; Boxberger, M.; Mosnier, J.; Le Bideau, M.; Duflot, I.; Fonta, I. In vitro antiviral activity of doxycycline against SARS-CoV-2. Molecules 2020, 25, 5064. [Google Scholar] [CrossRef] [PubMed]
- Hoyt, J.C.; Ballering, J.; Numanami, H.; Hayden, J.M.; Robbins, R.A. Doxycycline modulates nitric oxide production in murine lung epithelial cells. J. Immunol. 2006, 176, 567–572. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-S.; Luo, L.; Pflugfelder, S.C.; Li, D.-Q. Doxycycline inhibits TGF-β1–induced MMP-9 via Smad and MAPK pathways in human corneal epithelial cells. Invest. Ophthalmol. Vis. Sci. 2005, 46, 840–848. [Google Scholar] [CrossRef] [PubMed]
- Hsu, A.T.; Barrett, C.D.; DeBusk, M.G.; Ellson, C.D.; Gautam, S.; Talmor, D.S.; Gallagher, D.C.; Yaffe, M.B. Kinetics and role of plasma matrix metalloproteinase-9 expression in acute lung injury and the acute respiratory distress syndrome. Shock 2015, 44, 128. [Google Scholar] [CrossRef]
- Yates, P.A.; Newman, S.A.; Oshry, L.J.; Glassman, R.H.; Leone, A.M.; Reichel, E. Doxycycline treatment of high-risk COVID-19-positive patients with comorbid pulmonary disease. Ther. Adv. Respir. Dis. 2020, 14, 1753466620951053. [Google Scholar] [CrossRef] [PubMed]
- Malek, A.E.; Granwehr, B.P.; Kontoyiannis, D.P. Doxycycline as a potential partner of COVID-19 therapies. IDCases 2020, 21, e00864. [Google Scholar] [CrossRef] [PubMed]
- Department of Information and Publicity Government of Goa. Home Isolation Monitoring Kits for Covid-19 Launched. Available online: https://www.goa.gov.in/wp-content/uploads/2020/10/Home-Isolation-Monitoring-Kits-For-COVID-19-Launched.pdf (accessed on 16 December 2022).
- Aplicativo do Ministério da Saúde Recomenda Medicamentos sem Eficácia Comprovada para Tratar Covid. Available online: https://www.reuters.com/article/saude-covid-app-cloroquina-idLTAKBN29P29Y (accessed on 16 December 2022).
- COVID-19 Rapid Guideline: Managing Suspected or Confirmed Pneumonia in Adults in the Community. Available online: https://www.nice.org.uk/guidance/ng165 (accessed on 16 December 2022).
- Butler, C.C.; Yu, L.-M.; Dorward, J.; Gbinigie, O.; Hayward, G.; Saville, B.R.; Van Hecke, O.; Berry, N.; Detry, M.A.; Saunders, C. Doxycycline for community treatment of suspected COVID-19 in people at high risk of adverse outcomes in the UK (PRINCIPLE): A randomised, controlled, open-label, adaptive platform trial. Lancet Respir. Med. 2021, 9, 1010–1020. [Google Scholar] [CrossRef]
- Family phisicians society of the Republic of Srspka. Klinički Vodiči u Porodičnoj Medicini. Available online: https://www.porodicnamedicina.com/tech/klinicki-vodici/288-klinicki-vodici-u-porodicnoj-medicini (accessed on 16 December 2022).
- Lim, W.S.; Baudouin, S.V.; George, R.C.; Hill, A.T.; Jamieson, C.; Le Jeune, I.; Macfarlane, J.T.; Read, R.C.; Roberts, H.J.; Levy, M.L. BTS guidelines for the management of community acquired pneumonia in adults: Update 2009. Thorax 2009, 64, iii1–iii55. [Google Scholar] [CrossRef]
- Mandell, L.A.; Marrie, T.J.; Grossman, R.F.; Chow, A.W.; Hyland, R.H.; Group, C.C.-A.P.W. Canadian guidelines for the initial management of community-acquired pneumonia: An evidence-based update by the Canadian Infectious Diseases Society and the Canadian Thoracic Society. Clin. Infect. Dis. 2000, 31, 383–421. [Google Scholar] [CrossRef]
- Centers for Disease Control and Preventio Testing Guidance for Clinicians When SARS-CoV-2 and Influenza Viruses Are Co-Circulating. Available online: https://www.cdc.gov/flu/professionals/diagnosis/testing-guidance-for-clinicians.htm?fbclid=IwAR3523TwuQ_8p1wUR2wLWJZ18d6n5mkdC6Xt83P-Gu6R3fNVH0Vjf4FO8xg#print (accessed on 12 December 2022).
- Metlay, J.P.; Waterer, G.W.; Long, A.C.; Anzueto, A.; Brozek, J.; Crothers, K.; Cooley, L.A.; Dean, N.C.; Fine, M.J.; Flanders, S.A. Diagnosis and treatment of adults with community-acquired pneumonia. An official clinical practice guideline of the American Thoracic Society and Infectious Diseases Society of America. Am. J. Respir. Crit. Care Med. 2019, 200, e45–e67. [Google Scholar] [CrossRef]
- Italian Medicines Agency AIFA Recomendations on Medicines to Be Used in Home Management of COVID-19 Cases. Available online: https://www.aifa.gov.it/en/aggiornamento-sui-farmaci-utilizzabili-per-il-trattamento-della-malattia-covid19 (accessed on 12 December 2022).
- Bojanić, L.; Marković-Peković, V.; Škrbić, R.; Stojaković, N.; Dermanović, M.; Bojanić, J.; Fürst, J.; Kurdi, A.B.; Godman, B. Recent initiatives in the Republic of Srpska to enhance appropriate use of antibiotics in ambulatory care; Their influence and implications. Front. Pharmacol. 2018, 9, 442. [Google Scholar] [CrossRef] [PubMed]
- Marković-Peković, V.; Grubiša, N. Self-medication with antibiotics in the Republic of Srpska community pharmacies: Pharmacy staff behavior. Pharmacoepidemiol. Drug Saf. 2012, 21, 1130–1133. [Google Scholar] [CrossRef] [PubMed]
- Marković-Peković, V.; Grubiša, N.; Burger, J.; Bojanić, L.; Godman, B. Initiatives to reduce nonprescription sales and dispensing of antibiotics: Findings and implications. J. Res. Pharm. Pract. 2017, 6, 120. [Google Scholar] [PubMed]
- Public Health Institute of the Republic of Srpska. Izvještaj o Potrošnji i Prometu Gotovih Lijekova u Republici Srpskoj; Banja Luka. Available online: https://www.phi.rs.ba/index.php?lang=EN (accessed on 16 December 2022).
- Norwegian Institute of Public Health WHOCC Collaborating Centre for Drug Statistics Methodology. Available online: https://www.whocc.no/atc_ddd_index_and_guidelines/atc_ddd_index/ (accessed on 16 December 2022).
- Godman, B.; Wettermark, B.; Van Woerkom, M.; Fraeyman, J.; Alvarez-Madrazo, S.; Berg, C.; Bishop, I.; Bucsics, A.; Campbell, S.; Finlayson, A.E. Multiple policies to enhance prescribing efficiency for established medicines in Europe with a particular focus on demand-side measures: Findings and future implications. Front. Pharmacol. 2014, 5, 106. [Google Scholar] [CrossRef]
- Malo, S.; Bjerrum, L.; Feja, C.; Lallana, M.J.; Abad, J.M.; Rabanaque-Hernández, M.J. The quality of outpatient antimicrobial prescribing: A comparison between two areas of northern and southern Europe. Eur. J. Clin. Pharmacol. 2014, 70, 347–353. [Google Scholar] [CrossRef]
- Versporten, A.; Bolokhovets, G.; Ghazaryan, L.; Abilova, V.; Pyshnik, G.; Spasojevic, T.; Korinteli, I.; Raka, L.; Kambaralieva, B.; Cizmovic, L. Antibiotic use in eastern Europe: A cross-national database study in coordination with the WHO Regional Office for Europe. Lancet Infect. Dis. 2014, 14, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Abilova, V.; Kurdi, A.; Godman, B. Ongoing initiatives in Azerbaijan to improve the use of antibiotics; findings and implications. Expert Rev. Anti. Infect. Ther. 2018, 16, 77–84. [Google Scholar] [CrossRef]
- World Health Organization. Emergency Use ICD Codes for COVID-19 Disease Outbreak. Available online: https://www.who.int/standards/classifications/classification-of-diseases/emergency-use-icd-codes-for-covid-19-disease-outbreak (accessed on 16 December 2022).
- World Health Organization. List of Official ICD-10 Updates. Available online: https://www.who.int/standards/classifications/classification-of-diseases/list-of-official-icd-10-updates (accessed on 16 December 2022).
- Verheij, R.A.; Curcin, V.; Delaney, B.C.; McGilchrist, M.M. Possible sources of bias in primary care electronic health record data use and reuse. J. Med. Internet Res. 2018, 20, e9134. [Google Scholar] [CrossRef]
- Pannucci, C.J.; Wilkins, E.G. Identifying and avoiding bias in research. Plast. Reconstr. Surg. 2010, 126, 619. [Google Scholar] [CrossRef]
- Bennie, M.; Godman, B.; Bishop, I.; Campbell, S. Multiple initiatives continue to enhance the prescribing efficiency for the proton pump inhibitors and statins in Scotland. Expert Rev. Pharmacoecon. Outcomes Res. 2012, 12, 125–130. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| 2018 | 2019 | GI 19/18 * | 2020 | GI 20/19 ** | |
|---|---|---|---|---|---|
| III level of the ATC classification | |||||
| J01C (beta-lactam antibiotics) | 15.17 | 10.61 | −30.06% | 17.12 | 61.31% |
| J01D (other beta-lactam antibiotics) | 2.85 | 2.68 | −5.96% | 5.93 | 121.40% |
| J01F (macrolides, lincosamides, and streptogramines) | 2.15 | 2.23 | 3.72% | 3.48 | 55.85% |
| J01M (quinolones) | 2.23 | 2.05 | −8.07% | 2.22 | 8.49% |
| J01A (tetracyclines) | 1.71 | 1.15 | −32.75% | 1.13 | −2.31% |
| J01E (sulfonamides and trimethoprim) | 1.01 | 1.04 | 2.97% | 0.86 | −16.80% |
| J01X (other antibiotics) | 0.43 | 0.36 | −17.13% | ||
| J01G (aminoglycosides) | 0.05 | 0.05 | 0.00% | 0.04 | −24.31% |
| IV level of the ATC classification | |||||
| J01DB (first-generation cephalosporins) | 1.84 | 1.59 | −13.59% | 4.77 | 200% |
| J01DC (second-generation cephalosporins) | 0.72 | 0.61 | −15.28% | 0.52 | −14.75% |
| J01DD (third-generation cephalosporins) | 0.29 | 0.46 | 58.62% | 0.63 | 36.96% |
| J01DE (fourth-generation cephalosporins | 0 | 0.000178 | 1.81 × 10−5 | −89.83% | |
| J01FA (macrolides) | 2.06 | 2.14 | 3.88% | 3.41 | 59.34% |
| J01FF (lincosamides) | 0.08 | 0.09 | 12.50% | 0.07 | −22.22% |
| J01MA (fluoroquinolones) | 2.11 | 1.99 | −5.69% | 2.22 | 11.56% |
| J01MB (other quinolones) | 0.13 | 0.05 | −61.54% | 4.82 × 10−5 | −99.90% |
| V level of the ATC classification | |||||
| J01CA04 (amoxicillin) | 11.08 | 6.6 | −40.43% | 13.21 | 100.08% |
| J01DB01 (cephalexin) | 1.84 | 1.6 | −13.04% | 4.77 | 198.44% |
| J01CR02 (amoxicillin/clavulanic acid) | 3.04 | 2.99 | −1.64% | 3.24 | 8.32% |
| J01FA10 (azithromycin) | 1.14 | 1.28 | 12.28% | 2.79 | 117.43% |
| J01MA02 (ciprofloxacin) | 1.52 | 1.45 | −4.60% | 1.33 | −8.76% |
| J01AA02 (doxycycline) | 1.45 | 1.15 | −20.69% | 1.13 | −1.83% |
| J01EE01 (sulfamethoxazole, trimethoprim) | 1.01 | 1.04 | 2.97% | 0.86 | −16.80% |
| J01MA12 (levofloxacin) | 0.33 | 0.32 | −3.03% | 0.65 | 101.58% |
| J01CE02 (phenoxymethylpenicillin) | 0.9 | 0.84 | −6.67% | 0.55 | −34.31% |
| J01DC02 (cefuroxime) | 0.68 | 0.58 | −14.71% | 0.51 | −12.90% |
| J01FA09 (clarithromycin) | 0.49 | 0.49 | 0.00% | 0.41 | −17.35% |
| J01DD08 (cefixime) | 0.19 | 0.24 | 26.31% | 0.38 | 60.02% |
| J01DD04 (ceftriaxone) | 0.07 | 0.18 | 157.14% | 0.2 | 9.19% |
| J01FA01 (erythromycin) | 0.42 | 0.34 | −19.05% | 0.19 | −42.56% |
| J01MA06 (norfloxacin) | 0.21 | 0.19 | −9.52% | 0.17 | −11.51% |
| J01CA01 (ampicillin) | 0.12 | 0.15 | 25.00% | 0.09 | −36.97% |
| J01MA14 (moxifloxacin) | 0.03 | 0.04 | 33.33% | 0.08 | 124.60% |
| J01DD13 (cefpodoxime) | 0.02 | 0.04 | 100.00% | 0.05 | 21.39% |
| Variables | 2020 | 2021 | H1 2022 1 | |||
|---|---|---|---|---|---|---|
| N (%) | N (%) | N (%) | ||||
| Gender | ||||||
| Female | 1559 (52.32) | 5217 (56.06) | 2508 (58.63) | |||
| Age (years) | ||||||
| <15 | 15 (0.50) | 164 (1.76) | 131 (3.06) | |||
| 16–25 | 257 (8.62) | 891 (9.57) | 347 (8.11) | |||
| 26–35 | 463 (15.54) | 1320 (14.18) | 607 (14.19) | |||
| 36–45 | 748 (25.10) | 1948 (20.93) | 904 (21.13) | |||
| 46–55 | 547 (18.36) | 1581 (16.99) | 691 (16.15) | |||
| 56–65 | 514 (17.25) | 1704 (18.31) | 757 (17.70) | |||
| >66 | 436 (14.63) | 1698 (18.24) | 840 (19.64) | |||
| Number of patients according to WHO ICD-10 2 Codes | ||||||
| B34.2 3 | 229 (7.68) | 327 (3.51) | 212 (4.96) | |||
| U07.1 4 | 645 (21.64) | 3236 (34.77) | 1399 (32.70) | |||
| U07.2 5 | 2106 (70.67) | 5744 (61.72) | 2667 (62.34) | |||
| N (%) | |||
|---|---|---|---|
| Antibiotics According to V Level of ATC Classification | 2020 | 2021 | H1 2022 |
| amoxicillin | 38 (1.25) | 145 (1.61) | 84 (2.51) |
| amoxicillin/clavulanic acid | 284 (9.37) | 1758 (19.56) | 1085 (32.46) |
| azithromycin | 2009 (66.28) | 3454 (38.43) | 1195 (35.75) |
| cefixime | 48 (1.58) | 187 (2.08) | 48 (1.44) |
| ceftriaxone | 5 (0.16) | 45 (0.5) | |
| cefuroxime | 5 (0.16) | 16 (0.18) | 4 (0.12) |
| ciprofloxacin | 30 (0.99) | 133 (1.48) | 46 (0.12) |
| doxycycline | 236 (7.79) | 1520 (16.91) | 559 (16.72) |
| levofloxacin | 310 (10.23) | 400 (4.45) | 161 (4.82) |
| moxifloxacin | 41 (1.35) | 1181 (13.14) | 109 (3.26) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bednarčuk, N.; Golić Jelić, A.; Stoisavljević Šatara, S.; Stojaković, N.; Marković Peković, V.; Stojiljković, M.P.; Popović, N.; Škrbić, R. Antibiotic Utilization during COVID-19: Are We Over-Prescribing? Antibiotics 2023, 12, 308. https://doi.org/10.3390/antibiotics12020308
Bednarčuk N, Golić Jelić A, Stoisavljević Šatara S, Stojaković N, Marković Peković V, Stojiljković MP, Popović N, Škrbić R. Antibiotic Utilization during COVID-19: Are We Over-Prescribing? Antibiotics. 2023; 12(2):308. https://doi.org/10.3390/antibiotics12020308
Chicago/Turabian StyleBednarčuk, Nataša, Ana Golić Jelić, Svjetlana Stoisavljević Šatara, Nataša Stojaković, Vanda Marković Peković, Miloš P. Stojiljković, Nina Popović, and Ranko Škrbić. 2023. "Antibiotic Utilization during COVID-19: Are We Over-Prescribing?" Antibiotics 12, no. 2: 308. https://doi.org/10.3390/antibiotics12020308
APA StyleBednarčuk, N., Golić Jelić, A., Stoisavljević Šatara, S., Stojaković, N., Marković Peković, V., Stojiljković, M. P., Popović, N., & Škrbić, R. (2023). Antibiotic Utilization during COVID-19: Are We Over-Prescribing? Antibiotics, 12(2), 308. https://doi.org/10.3390/antibiotics12020308