Pharmacokinetic and Pharmacodynamic Considerations of Antibiotic Use in Neonates


Abstract
:1. Introduction
2. Pharmacokinetics
2.1. Volume of Distribution (Vd)
- (a)
- albumin and alpha-1 acid glycoprotein concentrations are lower at birth and gradually increase to adult levels by 1 year of age;
- (b)
- some drugs may have a lower binding affinity to fetal albumin that may persist in neonates;
- (c)
- high bilirubin and free fatty acid concentrations can displace drugs from albumin-binding sites;
- (d)
- specific interactions between albumin and globulins can affect the albumin binding affinity.
2.2. Clearance (CL)
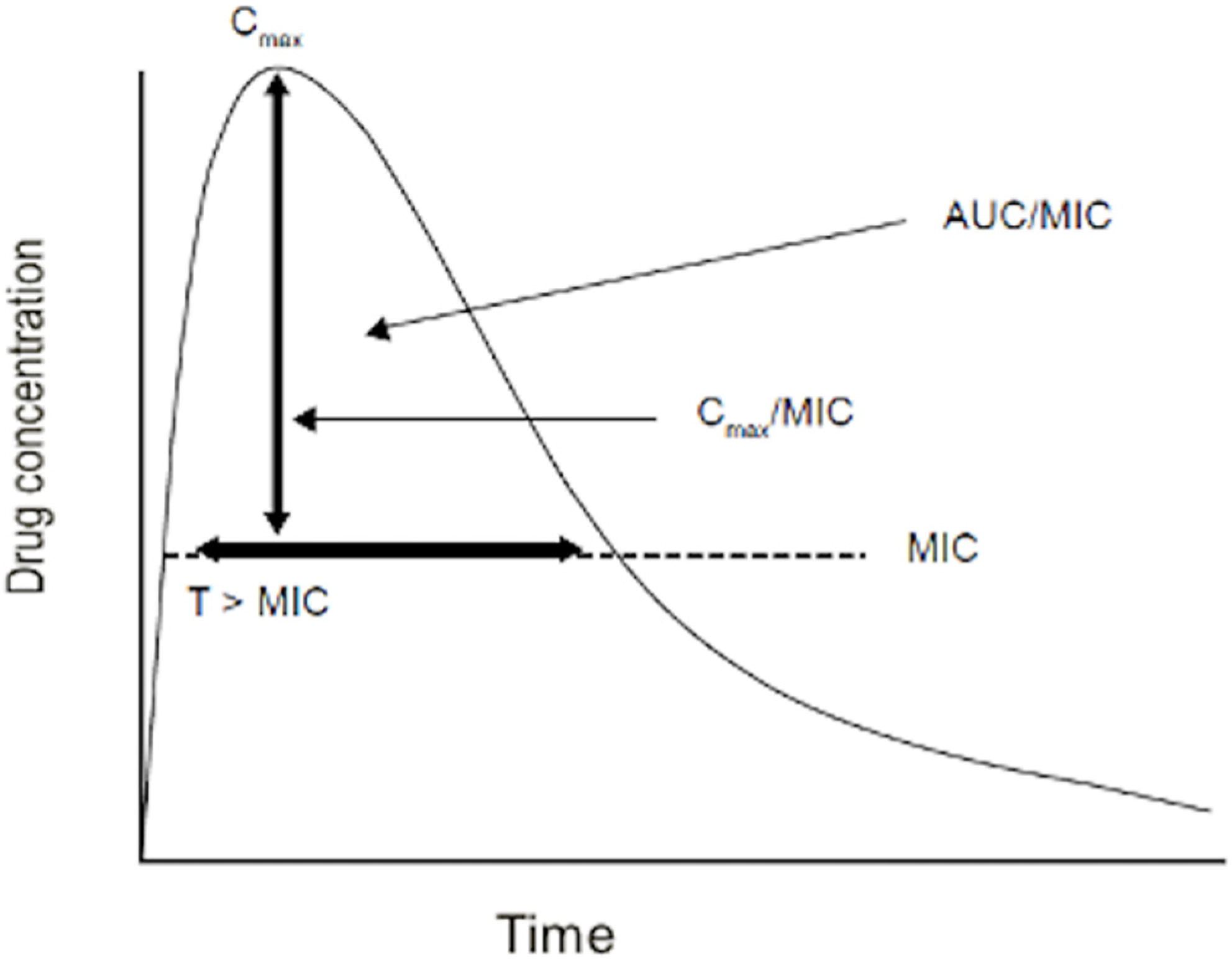
3. Pharmacodynamics
- (1)
- the ratio of the area under the plasma drug concentration-time curve (during the interval dosage, e.g., 24 h) to the MIC (AUC/MIC);
- (2)
- the ratio of peak plasma drug concentration and the MIC (Cmax/MIC);
- (3)
- the number of hours or percentage of time the drug plasma concentration remains above the MIC during a dosing interval (T > MIC (%)) (Figure 1).
4. Precision Dosing and Therapeutic Monitoring
- (a)
- when there is a weak correlation between dose and concentration and the concentration is more closely related to toxicity (or effect) than dosage;
- (b)
- when the drug has a narrow therapeutic index (high risk of toxicity);
- (c)
- when the interindividual variability is elevated; or for some drugs with nonlinear PK.
Author Contributions
Funding
Conflicts of Interest
References
- Van den Anker, J.N.; McCune, S.; Annaert, P.; Baer, G.R.; Mulugeta, Y.; Abdelrahman, R.; Wu, K.; Krudys, K.M.; Fisher, J.; Slikker, W.; et al. Approaches to dose finding in neonates, Illustrating the variability between neonatal drug development programs. Pharmaceutics 2020, 12, 685. [Google Scholar] [CrossRef] [PubMed]
- Perin, J.; Mulick, A.; Yeung, D.; Villavicencio, F.; Lopez, G.; Strong, K.L.; Prieto-Merino, D.; Cousens, S.; Black, R.E.; Liu, L. Global, regional, and national causes of under-5 mortality in 2000–19: An updated systematic analysis with implications for the Sustainable Development Goals. Lancet Child Adolesc. Health 2022, 6, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Cai, S.; Thompson, D.K.; Anderson, P.J.; Yang, J.Y. Short- and long-term neurodevelopmental outcomes of very preterm infants with neonatal sepsis: A systematic review and meta-analysis. Children 2019, 6, 131. [Google Scholar] [CrossRef] [PubMed]
- Mukhopadhyay, S.; Puopolo, K.M.; Hansen, N.I.; Lorch, S.A.; DeMauro, S.B.; Greenberg, R.G.; Cotton, C.M.; Sánchez, P.J.; Bell, E.F.; Eichenwald, E.C.; et al. Impact of Early-Onset Sepsis and Antibiotic Use on Death or Survival with Neurodevelopmental Impairment at 2 Years of Age among Extremely Preterm Infants. J. Pediatr. 2020, 221, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Car, K.P.; Nakwa, F.; Solomon, F.; Velaphi, S.C.; Tann, C.J.; Izu, A.; Lala, S.G.; Madhi, S.A.; Dangor, Z. The association between early-onset sepsis and neonatal encephalopathy. J. Perinatol. 2022, 42, 354–358. [Google Scholar] [CrossRef] [PubMed]
- Bhat, V.; Bhandar, V. Does neonatal sepsis independently increase neurodevelopmental impairment? Children 2022, 9, 568. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann, C.; Reichert, F.; Cassini, A.; Horner, R.; Harder, T.; Markwart, R.; Tröndle, M.; Savova, Y.; Kissoon, N.; Schlattmann, P.; et al. Global incidence and mortality of neonatal sepsis: A systematic review and meta-analysis. Arch. Dis. Child. 2021, 106, 745–752. [Google Scholar] [CrossRef] [PubMed]
- Stoll, B.J.; Puopolo, K.M.; Hansen, N.I.; Sánchez, P.J.; Bell, E.F.; Carlo, W.A.; Cotton, C.M.; D’Angio, C.T.; Kazzi, S.N.J.; Poindexter, B.B.; et al. Early-onset neonatal sepsis 2015 to 2017, the rise of Escherichia coli, and the need for novel prevention strategies. JAMA Pediatr. 2020, 174, e200593. [Google Scholar] [CrossRef]
- Puopolo, K.M.; Mukhopadhay, S.; Frymoyer, A.; Benitz, W.E. The term newborn: Early-onset sepsis. Clin. Perinatol. 2021, 48, 471–484. [Google Scholar] [CrossRef]
- Flannery, D.D.; Edwards, E.M.; Coggins, S.A.; Horbar, J.D.; Puopolo, K.M. Late-onset sepsis among very preterm infants. Pediatrics 2022, 150, e2022058813. [Google Scholar] [CrossRef]
- Flannery, D.D.; Edwards, E.M.; Puopolo, K.M.; Horbar, J.D. Early-onset sepsis among very preterm infants. Pediatrics 2021, 148, e2021052456. [Google Scholar] [CrossRef] [PubMed]
- Mukhopadhyay, S.; Wade, K.C.; Puopolo, K.M. Drugs for the prevention and treatment of sepsis in the newborn. Clin. Perinatol. 2019, 46, 327–347. [Google Scholar] [CrossRef] [PubMed]
- Huncikova, Z.; Stensvold, H.J.; Øymar, K.A.A.; Vatne, A.; Lang, A.M.; Støen, R.; Brigtsen, A.K.; Moster, D.; Eriksen, B.H.; Selberg, T.; et al. Variation in antibiotic consumption in very preterm infants—A 10 year population-based study. J. Antimicrob. Chemother. 2023, dkad358. [Google Scholar] [CrossRef] [PubMed]
- Shane, A.L.; Sánchez, P.J.; Stoll, B.J. Neonatal sepsis. Lancet 2017, 390, 1770–1780. [Google Scholar] [CrossRef] [PubMed]
- Rallis, D.; Giapros, V.; Serbis, A.; Kosmeri, C.; Baltogianni, M. Fighting antimicrobial resistance in neonatal intensive care units: Rational use of antibiotics in neonatal sepsis. Antibiotics 2023, 12, 508. [Google Scholar] [CrossRef] [PubMed]
- Garrido, F.; Allegaert, K.; Arribas, C.; Villamor, E.; Raffaeli, G.; Paniagua, M.; Cavallaro, G.; on behalf of European Antibiotics Study Group Easg. Variations in antibiotic use and sepsis management in neonatal intensive care units: A European survey. Antibiotics 2021, 10, 1046. [Google Scholar] [CrossRef] [PubMed]
- Prusakov, P.; Goff, D.A.; Wozniak, P.S.; Cassim, A.; Scipion, C.E.A.; Urzúa, S.; Ronchi, A.; Zeng, L.; Ladipo-Ajayi, O.; Aviles-Otero, N.; et al. A global point prevalence survey of antimicrobial use in neonatal intensive care units: The no-more-antibiotics and resistance (NO-MAS-R) study. eClinicalMedicine 2021, 32, 100727. [Google Scholar] [CrossRef] [PubMed]
- Euteneuer, J.C.; Kamatkar, S.; Fukuda, T.; Vinks, A.A.; Akinbi, H.T. Suggestions for model informed precision dosing to optimize neonatal drug therapy. J. Clin. Pharmacol. 2019, 59, 168–176. [Google Scholar] [CrossRef]
- European Commission. Regulation (EC) No 1901/2006 of the European Parliament and of the Council of 12 December 2006 on Medicinal Products for Pediatric Use and amending Regulation (EEC) No 1768/92, Directive 2001/20/EC, Directive 2001/83/ECand Regulation (EC) No 726/2004. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=celex%3A32006R1901 (accessed on 30 October 2023).
- Preparedness of Medicines’ Clinical Trials in Paediatrics Recommendations by the Enpr-EMA Working Group on Trial Preparedness. 31 August 2020 EMA/56009/2019. Available online: https://www.ema.europa.eu/en/documents/other/preparedness-medicines-clinical-trials-paediatrics-recommendations-enpr-ema-working-group-trial_en.pdf (accessed on 30 October 2023).
- Liu, Q.; Liu, L.; Yuan, Y.; Xie, F. A validated UHPLC–MS/MS method to quantify eight antibiotics in quantitative dried blood spots in support of pharmacokinetic studies in neonates. Antibiotics 2023, 12, 199. [Google Scholar] [CrossRef]
- Smits, A.; Annaert, P.; Allegaert, K. Drug disposition and clinical practice in neonates: Cross talk between developmental physiology and pharmacology. Int. J. Pharm. 2013, 452, 8–13. [Google Scholar] [CrossRef]
- Somani, A.A.; Thelen, K.; Zheng, S.; Trame, M.N.; Coboeken, K.; Meyer, M.; Schnizler, K.; Ince, I.; Willmann, S.; Schmidt, S. Evaluation of changes in oral drug absorption in preterm and term neonates for Biopharmaceutics Classification System (BCS) class I and II compounds. Br. J. Clin. Pharmacol. 2016, 81, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Lutsar, I.; Metsvaht, T. Understanding pharmacokinetics/pharmacodynamics in managing neonatal sepsis. Curr. Opin. Infect. Dis. 2010, 23, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Butranova, O.I.; Ushkalova, E.A.; Zyryanov, S.K.; Chenkurov, M.S. Developmental pharmacokinetics of antibiotics Used in neonatal ICU: Focus on preterm infants. Biomedicines 2023, 11, 940. [Google Scholar] [CrossRef] [PubMed]
- van Donge, T.; Van den Anker, J.; Pfister, M. Key Components for Antibiotic Dose Optimization of Sepsis in Neonates and Infants. Front. Pediatr. 2018, 29, 325. [Google Scholar] [CrossRef] [PubMed]
- Bennet, L.Z.; Massoud, N. Pharmacokinetics. In Pharmacokinetic Basis for Drug Treatment; Bennet, L.Z., Massoud, N., Gambertoglio, J.G., Eds.; Raven Press: New York, NY, USA, 1983; pp. 1–27. [Google Scholar]
- Shentag, J.J.; Meagher, A.K.; Jelliffe, R.W. Aminoglycosides. In Applied Pharmacokinetics & Pharmacodymanics: Principles of Therapeutic Drug Monitoring, 4th ed.; Burton, M., Shaw, L.M., Shentag, J.J., Evan, W.E., Eds.; Lippincott Williams & Wilkins: Baltimore, MD, USA, 2006; pp. 286–327. [Google Scholar]
- Pacifici, G.M. Clinical pharmacokinetics of aminoglycosides in the neonate: A review. Eur. J. Clin. Pharmacol. 2009, 65, 419–427. [Google Scholar] [CrossRef] [PubMed]
- De Sutter, P.J.; Rossignol, P.; Breëns, L.; Gasthuys, E.; Vermeulen, A. Predicting Volume of Distribution in Neonates: Performance of Physiologically Based Pharmacokinetic Modelling. Pharmaceutics 2023, 15, 2348. [Google Scholar] [CrossRef] [PubMed]
- Ku, L.C.; Brian Smith, P. Dosing in neonates: Special considerations in physiology and trial design. Pediatr. Res. 2015, 77, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Sherwin, J.; Heath, T.; Watt, K. Pharmacokinetics and Dosing of Anti-Infective Drugs in Patients on Extracorporeal Membrane Oxygenation: A Review of the Current Literature. Clin. Ther. 2016, 38, 1976–1994. [Google Scholar] [CrossRef]
- Craig, W.A.; Kunin, C.M. Significance of serum protein and tissue binding of antimicrobial agents. Annu. Rev. Med. 1976, 27, 287–300. [Google Scholar] [CrossRef]
- Merrikin, D.J.; Briant, J.; Rolinson, G.N. Effect of protein binding on antibiotic activity in vivo. J. Antimicrob. Chemother. 1983, 11, 233–238. [Google Scholar] [CrossRef]
- McNamara, P.J.; Alcorn, J. Protein binding predictions in infants. AAPS PharmSci 2002, 4, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Cantey, J.B. Optimizing the Use of Antibacterial Agents in the Neonatal Period. Pediatr. Drugs 2016, 18, 109–122. [Google Scholar] [CrossRef] [PubMed]
- Smits, A.; Annaert, P.; Van Cruchten, S.; Allegaert, K. A Physiology-Based Pharmacokinetic Framework to Support Drug Development and Dose Precision During Therapeutic Hypothermia in Neonates. Front. Pharmacol. 2020, 11, 587. [Google Scholar] [CrossRef] [PubMed]
- De Wildt, S.N.; Kearns, G.L.; Leeder, J.S.; Van Den Anker, J.N. Cytochrome P450 3A: Ontogeny and drug disposition. Clin. Pharmacokinet. 1999, 37, 485–505. [Google Scholar] [CrossRef] [PubMed]
- Ince, I.; Knibbe, C.A.; Danhof, M.; De Wildt, S.N. Developmental changes in the expression and function of cytochrome P450 3A isoforms: Evidence from in vitro and in vivo investigations. Clin. Pharmacokinet. 2013, 52, 333–345. [Google Scholar] [CrossRef] [PubMed]
- Allegaert, K.; Vanhaesebrouck, S.; Verbesselt, R.; Van Den Anker, J.N. In vivo glucuronidation activity of drugs in neonates: Extensive interindividual variability despite their young age. Ther. Drug Monit. 2009, 31, 411–415. [Google Scholar] [CrossRef] [PubMed]
- Tracy, T.S.; Chaudhry, A.S.; Prasad, B.; Thummel, K.E.; Schuetz, E.G.; Zhong, X.; Tien, Y.-C.; Jeong, H.; Pan, X.; Shireman, L.M.; et al. Interindividual variability in cytochrome P450–mediated drug metabolism. Drug Metab. Dispos. 2016, 44, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Rodieux, F.; Wilbaux, M.; van den Anker, J.N.; Pfister, M. Effect of kidney function on drug kinetics and dosing in neonates, infants, and children. Clin. Pharmacokinet. 2015, 54, 1183–1204. [Google Scholar] [CrossRef]
- Allegaert, K.; Anderson, B.J.; van den Anker, J.N.; Vanhaesebrouck, S.; de Zegher, F. Renal drug clearance in preterm neonates: Relation to prenatal growth. Ther. Drug Monit. 2007, 29, 284–291. [Google Scholar] [CrossRef]
- Muller, A.E.; Huttner, B.; Huttner, A. Therapeutic drug monitoring of beta-lactams and other antibiotics in the intensive care unit: Which agents, which patients and which infections? Drugs 2018, 78, 439–451. [Google Scholar] [CrossRef]
- Rodríguez-Gascón, A.; Solinís, M.Á.; Isla, A. The role of PK/PD analysis in the development and evaluation of antimicrobials. Pharmaceutics 2021, 13, 833. [Google Scholar] [CrossRef] [PubMed]
- Men, P.; Li, H.-B.; Zhai, S.-D.; Zhao, R.-S. Association between the AUC0-24/MIC ratio of vancomycin and its clinical effectiveness: A systematic review and meta-analysis. PLoS ONE 2016, 11, e0146224. [Google Scholar] [CrossRef] [PubMed]
- MacGowan, A. Revisiting beta-lactams-PK/PD improves dosing of old antibiotics. Curr. Opin. Pharmacol. 2011, 11, 470–476. [Google Scholar] [CrossRef] [PubMed]
- Marsot, A.; Boulamery, A.; Bruguerolle, B.; Simon, N. Population pharmacokinetic analysis during the first 2 years of life: An overview. Clin. Pharmacokinet. 2012, 51, 787–798. [Google Scholar] [CrossRef] [PubMed]
- Bleyzac, N.; Varnier, V.; Labaune, J.M.; Corvaisier, S.; Maire, P.; Jelliffe, R.W.; Putet, G.; Aulagner, G. Population pharmacokinetics of amikacin at birth and interindividual variability in renal maturation. Eur. J. Clin. Pharmacol. 2001, 57, 499–504. [Google Scholar] [CrossRef] [PubMed]
- Pullen, J.; Stolk, L.M.; Nieman, F.H.; Degraeuwe, P.L.; van Tiel, F.H.; Zimmermann, L.J. Population pharmacokinetics and dosing of amoxicillin in (pre)term neonates. Ther. Drug Monit. 2006, 28, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Capparelli, E.; Hochwald, C.; Rasmussen, M.; Parham, A.; Bradley, J.; Moya, F. Population pharmacokinetics of cefepime in the neonate. Antimicrob. Agents Chemother. 2005, 49, 2760–2766. [Google Scholar] [CrossRef] [PubMed]
- Lima-Rogel, V.; Medina-Rojas, E.L.; Del Carmen Milàn-Segovia, R.; Noyola, D.E.; Nieto-Aguirre, K.; Lòpez-Delarosa, A.; Romano-Moreno, S. Population pharmacokinetics of cefepime in neonates with severe nosocomial infections. J. Clin. Pharm. Ther. 2008, 33, 295–306. [Google Scholar] [CrossRef]
- Karna, P.; Lee, C.; Kumar, A.; Dyke, J.; Gooch, W.M. 3rd. Population pharmacokinetics of ceftizoxime in premature newborns. Dev. Pharmacol. Ther. 1993, 20, 135–143. [Google Scholar] [CrossRef]
- Jensen, P.D.; Edgren, B.E.; Brundage, R.C. Population pharmacokinetics of gentamicin in neonates using a nonlinear, mixedeffects model. Pharmacotherapy 1992, 12, 178–182. [Google Scholar] [CrossRef]
- Botha, J.H.; du Preez, M.J.; Adhikari, M. Population pharmacokinetics of gentamicin in South African newborns. Eur. J. Clin. Pharmacol. 2003, 59, 755–759. [Google Scholar] [CrossRef] [PubMed]
- Garcıa, B.; Barcia, E.; Perez, F.; Molina, I.T. Population pharmacokinetics of gentamicin in premature newborns. J. Antimicrob. Chemother. 2006, 58, 372–379. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, E.I.; Sandstrom, M.; Honore, P.H.; Ewald, U.; Friberg, L.E. Developmental pharmacokinetics of gentamicin in preterm and term neonates: Population modelling of a prospective study. Clin. Pharmacokinet. 2009, 48, 253–263. [Google Scholar] [CrossRef] [PubMed]
- Bradley, J.S.; Sauberan, J.B.; Ambrose, P.G.; Bhavnani, S.M.; Rasmussen, M.R.; Capparelli, E.V. Meropenem pharmacokinetics, pharmacodynamics, and Monte Carlo simulation in the neonate. Pediatr. Infect. Dis. J. 2008, 27, 794–799. [Google Scholar] [CrossRef] [PubMed]
- Yasuhara, M.; Iga, T.; Zenda, H.; Okumura, K.; Oguma, T.; Yano, Y.; Hori, R. Population pharmacokinetics of vancomycin in Japanese pediatric patients. Ther. Drug Monit. 1998, 20, 612–618. [Google Scholar] [CrossRef] [PubMed]
- Anderson, B.J.; Allegaert, K.; Van den Anker, J.N.; Cossey, V.; Holford, N.H. Vancomycin pharmacokinetics in preterm neonates and the prediction of adult clearance. Br. J. Clin. Pharmacol. 2007, 63, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Duspara, K.; Smits, A.; Allegaert, K.; Heljic, S.; Turcic, P.; Racovac, T.L.; Kusturica, J.; Rakanovic-Todic, M.; Burnazovic-Ristic, L.; Maleskic, S.; et al. The role of population pharmacokinetic analysis in rational antibiotic therapy in neonates. In CMBEBIH 2017. IFMBE Proceedings; Badnjevic, A., Ed.; Springer: Singapore, 2017; Volume 62, p. 762. [Google Scholar] [CrossRef]
- Leroux, S.; Jacqz-Aigrain, E.; Biran, V.; Lopez, E.; Madeleneau, D.; Wallon, C. Clinical utility and safety of a model-based patient-tailored dose of vancomycin in neonates. Antimicrob. Agents Chemother. 2016, 60, 2039–2042. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Blanco, J.S.; Lanao, J.M. Model-Informed Precision Dosing (MIPD). Pharmaceutics 2022, 14, 2731. [Google Scholar] [CrossRef]
- Pons, G.; Tréluyer, J.M.; Dimet, J.; Merlé, Y. Potential Benefit of Bayesian Forecasting for Therapeutic Drug Monitoring in Neonates. Ther. Drug Monit. 2002, 24, 9–14. [Google Scholar] [CrossRef]
- Wicha, S.G.; Märtson, A.G.; Nielsen, E.I.; Koch, B.C.P.; Friberg, L.E.; Alffenaar, J.W.; Minichmayr, I.K. From therapeutic drug monitoring to model-informed precision dosing for antibiotics. Clin. Pharm. Ther. 2021, 109, 918–941. [Google Scholar] [CrossRef]
- Abdulla, A.; Edwina, E.E.; Flint, R.B.; Allegaert, K.; Wildschut, E.D.; Koch, B.C.P.; de Hoog, M. Model-informed precision dosing of antibiotics in pediatric patients: A narrative review. Front. Pediatr. 2021, 9, 624639. [Google Scholar] [CrossRef] [PubMed]
- Samardzic, J.; Allegaert, K.; Wilbaux, M.; Pfister, M.; van den Anker, J.N. Quantitative clinical pharmacology practice for optimal use of antibiotics during the neonatal period. Expert Opin. Drug Metab. Toxicol. 2016, 12, 367–375. [Google Scholar] [CrossRef] [PubMed]
- Sinkeler, F.S.; de Haan, T.R.; Hodiamont, C.J.; Bijleveld, Y.A.; Pajkrt, D.; Mathôt, R.A. Inadequate vancomycin therapy in term and preterm neonates: A retrospective analysis of trough serum concentrations in relation to minimal inhibitory concentrations. BMC Pediatr. 2014, 14, 193. [Google Scholar] [CrossRef] [PubMed]
- Tzialla, C.; Borghesi, A.; Serra, G.; Stronati, M.; Corsello, G. Antimicrobial therapy in neonatal intensive care unit. Ital. J. Pediatr. 2015, 41, 27. [Google Scholar] [CrossRef] [PubMed]
- Ting, J.Y.; Roberts, A. Association of early life antibiotics and health outcomes: Evidence from clinical studies. Semin. Perinatol. 2020, 44, 151322. [Google Scholar] [CrossRef] [PubMed]
- Weimer, K.E.D.; Smith, P.B.; Puia-Dumitrescu, M.; Aleem, S. Invasive fungal infections in neonates: A review. Pediatr. Res. 2022, 91, 404–412. [Google Scholar] [CrossRef] [PubMed]
- Cantey, J.B.; Pyle, A.K.; Wozniak, P.S.; Hynan, L.S.; Sánchez, P.J. Early antibiotic exposure and adverse outcomes in preterm, very low birth weight infants. J. Pediatr. 2018, 203, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Ting, J.Y.; Roberts, A.; Sherlock, R.; Ojah, C.; Cieslak, Z.; Dunn, M.; Barrington, K.; Yoon, E.W.; Shah, P.S.; on behalf of the Canadian Neonatal Network Investigators. Duration of initial empirical antibiotic therapy and outcomes in very low birth weight infants. Pediatrics 2019, 143, e20182286. [Google Scholar] [CrossRef]
- Letouzey, M.; Lorthe, E.; Marchand-Martin, L.; Kayem, G.; Charlier, C.; Butin, M.; Mitha, A.; Kaminski, M.; Benhammou, V.; Ancel, P.Y.; et al. Early antibiotic exposure and adverse outcomes in very preterm infants at low risk of early-onset sepsis: The EPIPAGE-2 Cohort Study. J. Pediatr. 2022, 243, 91–98. [Google Scholar] [CrossRef]
- Vatne, A.; Hapnes, N.; Stensvold, H.J.; Dalen, I.; Guthe, H.J.; Støen, R.; Brigtsen, A.K.; Rønnestad, A.E.; Klingenberg, C.; Norwegian Neonatal Network. Early empirical antibiotics and adverse clinical outcomes in infants born very preterm: A population-based cohort. J. Pediatr. 2023, 253, 107–114. [Google Scholar] [CrossRef]
- Awujoola, A.; Torga, A.P.; Abdul Ghayum, M.A.; Mousa, N.; Olorunsogo, T.; DeSilva, S.; Avades, M.; Prince, O.; Ankola, P. Neonatal ampicillin/gentamicin exposure and the risk of childhood obesity in South Bronx pediatric population. Am. J. Perinatol. 2023. [Google Scholar] [CrossRef] [PubMed]
- Stocker, M.; Klingenberg, C.; Navér, L.; Nordberg, V.; Berardi, A.; El Helou, S.; Fusch, G.; Bliss, J.M.; Lehnick, D.; Dimopoulou, V.; et al. Less is more: Antibiotics at the beginning of life. Nat. Commun. 2023, 14, 2423. [Google Scholar] [CrossRef] [PubMed]
- McMullan, B.; Bryant, P.A.; Duffy, E.; Bielicki, J.; De Cock, P.; Science, M.; Zembles, T.; Timberlake, K.; Monsees, E.; Hamdy, R.F.; et al. Multinational consensus antimicrobial stewardship recommendations for children managed in hospital settings. Lancet Infect. Dis. 2023, 23, e199–e207. [Google Scholar] [CrossRef] [PubMed]
- Akinboyo, I.C.; Gerber, J.S. Principles, policy and practice of antibiotic stewardship. Semin. Perinatol. 2020, 44, 151324. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; An, S.H. Impact of pharmacist intervention in antibiotic stewardship programmes for critically ill neonates: A systematic review and meta-analysis. J. Clin. Pharm. Ther. 2022, 47, 430–444. [Google Scholar] [CrossRef] [PubMed]
- Unni, J.C.; Chacko, M.; Jacob, J.; Warrier, A. Randomised control trial on impact of clinical pharmacist led interventions on antibiotic stewardship program in children 0 to 18 years age in a tertiary care hospital in southern India. Am. J. Infect. Control, 2023; in press. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Population Averages (±SD) in Patients with Normal Renal Function. | |||||
|---|---|---|---|---|---|
| Parameter | Children | Neonates | |||
| <2000 g | >2000 g | ||||
| <1 Week | >1 Week | <1 Week | >1 Week | ||
| Clearance mL/min/1.73 m2 | 1.31 ± 10 | 22.1 | 24.6 | 28.4 | 36.4 |
| Volume of distribution, L/kg | 0.07–0.7 | 0.2–0.7 | |||
| Elimination half-life, h | 0.5–2.5 | 2.0–9.0 | |||
| % excreted in urine | 85–95% | First dose 65–85% in 24 h; steady-state 85–95% | |||
| Aminoglycosides | β-lactams | Glycopeptides | |||||
|---|---|---|---|---|---|---|---|
| Gentamicin | Amikacin | Tobramycin | Penicillins | Carbapenems | Cephalosporins | Vancomycin | |
| PK/PD parameters | Cmax/MIC | fT > MIC (%) | 24 h AUC/MIC | ||||
| PK/PD efficacy target values | ≥8 | 8–10 | 8–12 | T > MIC >50–60% | T > MIC >40–60% | T > MIC >60–70% | 400 |
| TDM reference intervals | Cmin 0.5–2.0 mg/L | Cmin <5 mg/L | Cmin <1.0 mg/L | Cmin 10–20 mg/L | |||
| TDM reference intervals | Cmin 0.5–2.0 mg/L | Cmin <5 mg/L | Cmin <1.0 mg/L | Cmin 10–20 mg/L | |||
| Cmax 5–10 mg/L | Cmax 20–60 mg/L | Cmax >10 mg/L | Cmax 30–40 mg/L | ||||
| PK/PD properties | Concentration-dependent killing and prolonged persistent effects | Time-dependent killing and minimal persistent effects | Time- and conc.-dependent killing and moderate to prolonged persistent effects | ||||
| Drug | No. of Pts | PN Age Days | Software | Covariables Used to Estimate Clearance | Covariables Used to Estimate Volume of Distribution | Bibliography |
|---|---|---|---|---|---|---|
| Amikacin | 131 | 1 | NPEM2 | GA, Weight | GA, Weight | [49] |
| Amoxicillin | 150 | 1 | MW/PHARM | GA, PNA, Weight | Weight | [50] |
| Cefepime | 55 | 14.5 | NONMEM | SCr | PCA | [51] |
| Cefepime | 31 | 21.8 | NONMEM | ASC, CLcr | ASC | [52] |
| Ceftixozime | 50 | 5 | NONMEM | Weight | Weight | [53] |
| Gentamicin | 30 | 7 | NONMEM | Weight | Weight | [54] |
| Gentamicin | 79 | 4.2 | NONMEM | Weight, GA | Weight | [55] |
| Gentamicin | 200 | 5.5 | NONMEM | Weight, Clcr, PNA | Weight | [56] |
| Gentamicin | 61 | 20 | NONMEM | Weight, GA, PNA | Weight, GA | [57] |
| Meropenem | 37 | 40 | NONMEM | Scr, PCA | Weight | [58] |
| Vancomycin | 49 | 2.3 | NONMEM | PNA, Weight | Weight | [59] |
| Vancomycin | 214 | 12 | NONMEM | Weight, PMA | Weight | [60] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Regazzi, M.; Berardi, A.; Picone, S.; Tzialla, C. Pharmacokinetic and Pharmacodynamic Considerations of Antibiotic Use in Neonates. Antibiotics 2023, 12, 1747. https://doi.org/10.3390/antibiotics12121747
Regazzi M, Berardi A, Picone S, Tzialla C. Pharmacokinetic and Pharmacodynamic Considerations of Antibiotic Use in Neonates. Antibiotics. 2023; 12(12):1747. https://doi.org/10.3390/antibiotics12121747
Chicago/Turabian StyleRegazzi, Mario, Alberto Berardi, Simonetta Picone, and Chryssoula Tzialla. 2023. "Pharmacokinetic and Pharmacodynamic Considerations of Antibiotic Use in Neonates" Antibiotics 12, no. 12: 1747. https://doi.org/10.3390/antibiotics12121747
APA StyleRegazzi, M., Berardi, A., Picone, S., & Tzialla, C. (2023). Pharmacokinetic and Pharmacodynamic Considerations of Antibiotic Use in Neonates. Antibiotics, 12(12), 1747. https://doi.org/10.3390/antibiotics12121747