
Rates and Determinants of Hospital-Acquired Infection among ICU Patients Undergoing Cardiac Surgery in Developing Countries: Results from EMERGENCY’NGO’s Hospital in Sudan
 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Methods
2.1. Study Design, Patient Selection and End Points
- (1)
- Elective: For clinically stable patients scheduled for cardiac surgery. Ideally, these patients are meant to be admitted on a ward level a few days before undergoing surgery in order to perform a standard pre-operative assessment including laboratory exams, ECG and heart ultrasound. Following surgery, they are initially referred to the ICU and then to the sub-ICU/ward for post-operative care.
- (2)
- Urgent: For patients requiring urgent care as a result of a precipitating condition. These patients receive medical care and, when appropriate, some of them also undergo urgent surgery. In relation to their clinical conditions, at hospital admission, patients are referred either to the ICU, sub-ICU or ward.
2.2. Study Setting
2.3. Definitions
2.4. Microbiological Studies
2.5. Statistical Analysis
2.6. Ethics
3. Results
3.1. Description of Study Population
3.2. Outcomes Evaluation
3.2.1. Infection Prevalence
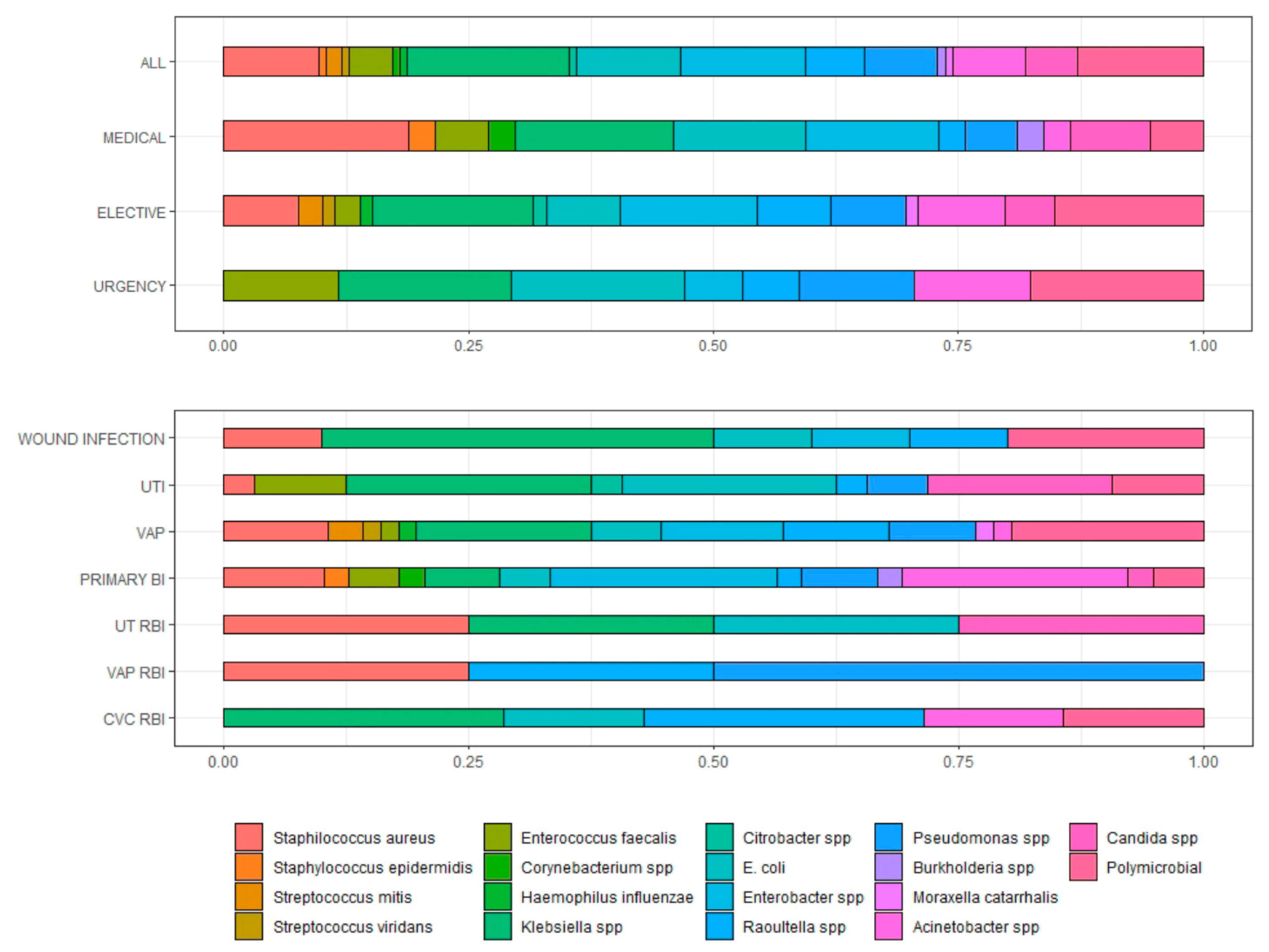
3.2.2. Microbiological and Clinical Characteristics of Infections
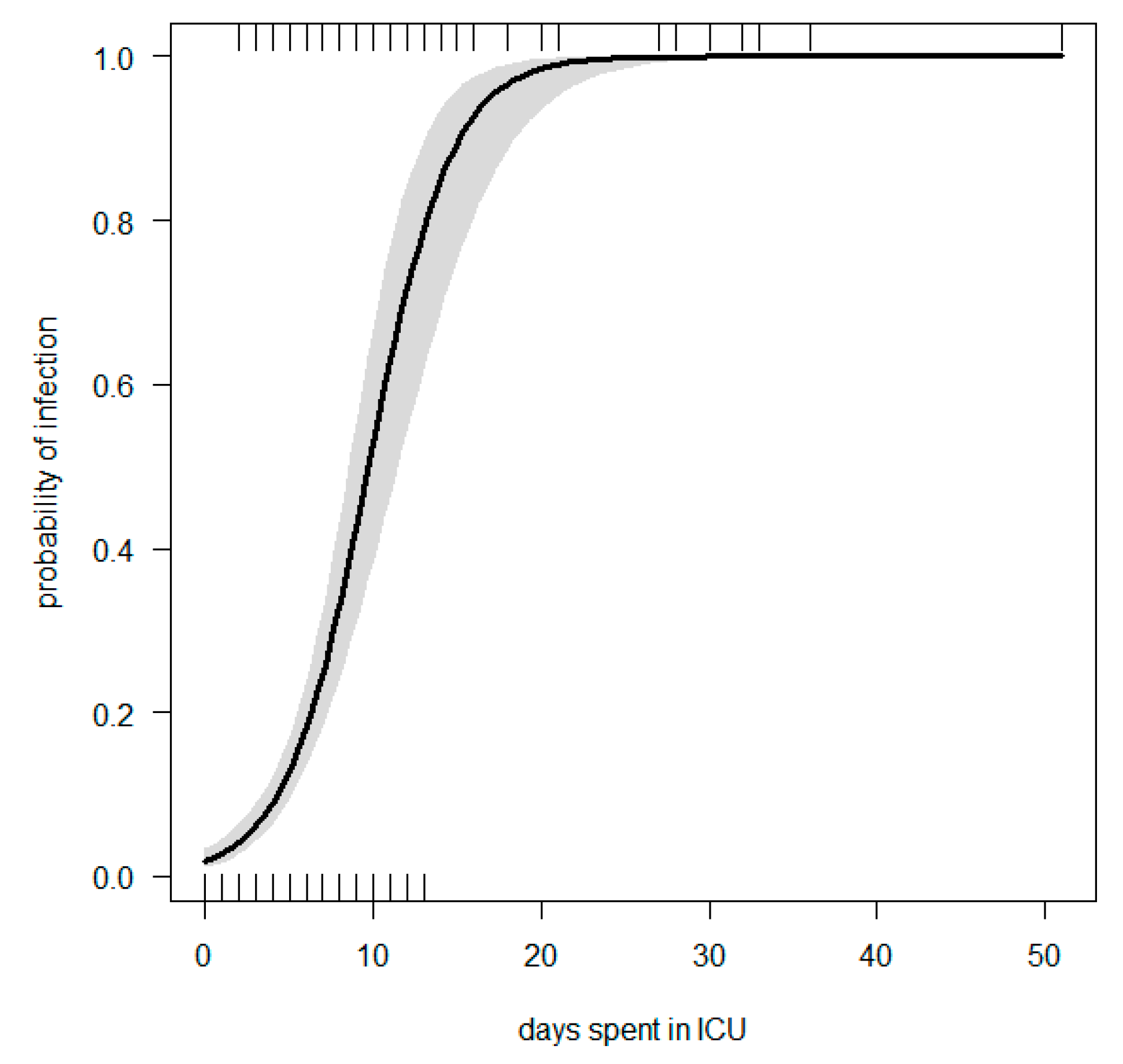
3.2.3. Risk Factors Associated with Development of Infections
3.2.4. Mortality
4. Discussion
5. Conclusions
6. Recommendation
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gelijns, A.C.; Moskowitz, A.J.; Acker, M.A.; Argenziano, M.; Geller, N.L.; Puskas, J.D.; Perrault, L.P.; Smith, P.K.; Kron, I.L.; Michler, R.E.; et al. Management Practices and Major Infections After Cardiac Surgery. J. Am. Coll. Cardiol. 2014, 64, 372–381. [Google Scholar] [CrossRef] [PubMed]
- Toeg, H.; French, D.; Gilbert, S.; Rubens, F. Incidence of sternal wound infection after tracheostomy in patients undergoing cardiac surgery: A systematic review and meta-analysis. J. Thorac. Cardiovasc. Surg. 2017, 153, 1394–1400.e7. [Google Scholar] [CrossRef]
- Massart, N.; Mansour, A.; Ross, J.T.; Piau, C.; Verhoye, J.P.; Tattevin, P.; Nesseler, N. Mortality due to hospital-acquired infection after cardiac surgery. J. Thorac. Cardiovasc. Surg. 2020, 163, 2131–2140.e3. [Google Scholar] [CrossRef]
- Gao, Y.; Wang, C.; Wang, Y.; Li, J.; Wang, J.; Wang, S.; Tian, Y.; Liu, J.; Diao, X.; Zhao, W. Establishment and Validation of a Nomogram to Predict Hospital-Acquired Infection in Elderly Patients After Cardiac Surgery. Clin. Interv. Aging. 2022, 17, 141–150. [Google Scholar] [CrossRef]
- He, S.; Chen, B.; Li, W.; Yan, J.; Chen, L.; Wang, X.; Xiao, Y. Ventilator-associated pneumonia after cardiac surgery: A meta-analysis and systematic review. J. Thorac. Cardiovasc. Surg. 2014, 148, e1–e5. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://salamcentre.emergency.it/ (accessed on 30 July 2022).
- Mukaka, M.M. Statistics corner: A guide to appropriate use of correlation coefficient in medical research. Malawi Med. J. 2012, 24, 69–71. [Google Scholar]
- Russo, A.; Carriero, G.; Farcomeni, A.; Ceccarelli, G.; Tritapepe, L.; Venditti, M. Role of oral nystatin prophylaxis in cardiac surgery with prolonged extracorporeal circulation. Mycoses 2017, 60, 826–829. [Google Scholar] [CrossRef] [PubMed]
- Kitai, T.; Kirsop, J.; Tang, W.H. Exploring the Microbiome in Heart Failure. Curr. Heart Fail Rep. 2016, 13, 103–109. [Google Scholar] [CrossRef]
- Wang, D.S.; Huang, X.F.; Wang, H.F.; Le, S.; Du, X.L. Clinical risk score for postoperative pneumonia following heart valve surgery. Chin. Med. J. 2021, 134, 2447–2456. [Google Scholar] [CrossRef]
- Wang, D.; Huang, X.; Wang, H.; Le, S.; Yang, H.; Wang, F.; Du, X. Risk factors for postoperative pneumonia after cardiac surgery: A prediction model. J. Thorac. Dis. 2021, 13, 2351–2362. [Google Scholar] [CrossRef]
- Bouza, E.; Pérez, A.; Muñoz, P.; Jesús Pérez, M.; Rincón, C.; Sánchez, C.; Martín-Rabadán, P.; Riesgo, M.; Cardiovascular Infection Study Group. Ventilator-associated pneumonia after heart surgery: A prospective analysis and the value of surveillance. Crit. Care Med. 2003, 31, 1964–1970. [Google Scholar] [CrossRef]
- Xu, F.; Li, W.; Zhang, C.; Cao, R. Performance of Sequential Organ Failure Assessment and Simplified Acute Physiology Score II for Post-Cardiac Surgery Patients in Intensive Care Unit. Front. Cardiovasc. Med. 2021, 8, 774935. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Liu, F.; Gong, S.; Liao, B.; Liu, H.; Yuan, J.; Yu, D.; Qin, H.; Wu, M.; Dong, S. Validity of SOFA score as a prognostic tool for critically ill elderly patients with acute infective endocarditis. Rev. Cardiovasc. Med. 2021, 22, 967–973. [Google Scholar] [CrossRef] [PubMed]
- Pitiriga, V.; Kanellopoulos, P.; Bakalis, I.; Kampos, E.; Sagris, I.; Saroglou, G.; Tsakris, A. Central venous catheter-related bloodstream infection and colonization: The impact of insertion site and distribution of multidrug-resistant pathogens. Antimicrob. Resist. Infect. Control. 2020, 9, 189. [Google Scholar] [CrossRef] [PubMed]
- Toor, H.; Farr, S.; Savla, P.; Kashyap, S.; Wang, S.; Miulli, D.E. Prevalence of Central Line-Associated Bloodstream Infections (CLABSI) in Intensive Care and Medical-Surgical Units. Cureus 2022, 14, e22809. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Sun, G.; Cheng, Z.; Mei, C.; Liao, X.; Li, J.; Yuan, Y. Analysis of Nosocomial Infections in Post-Cardiac Surgery Extracorporeal Membrane Oxygenation Support Therapy. Heart Surg. Forum. 2018, 21, E387–E391. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wang, L.; Jia, M.; Du, Z.; Hou, X. Extracorporeal Membrane Oxygenation-Related Nosocomial Infection after Cardiac Surgery in Adult Patients. Braz. J. Cardiovasc. Surg. 2021, 36, 743–751. [Google Scholar] [CrossRef]
- Parienti, J.J.; Dugué, A.E.; Daurel, C.; Mira, J.P.; Mégarbane, B.; Mermel, L.A.; Daubin, C.; du Cheyron, D. Members of the Cathedia Study Group. Continuous renal replacement therapy may increase the risk of catheter infection. Clin. J. Am. Soc. Nephrol. 2010, 5, 1489–1496. [Google Scholar] [CrossRef]
- Ding, W.; Liu, J.; Zhou, X.; Miao, Q.; Zheng, H.; Zhou, B.; Dou, G.; Tong, Y.; Long, Y.; Su, L. Clinical Multi-Omics Study on the Gut Microbiota in Critically Ill Patients After Cardiovascular Surgery Combined With Cardiopulmonary Bypass With or Without Sepsis (MUL-GM-CSCPB Study): A Prospective Study Protocol. Front. Med. 2020, 7, 269. [Google Scholar] [CrossRef] [PubMed]
- Byarugaba, D.K. A view on antimicrobial resistance in developing countries and responsible risk factors. Int. J. Antimicrob. Agents. 2004, 24, 105–110. [Google Scholar] [CrossRef]
- Ayukekbong, J.A.; Ntemgwa, M.; Atabe, A.N. The threat of antimicrobial resistance in developing countries: Causes and control strategies. Antimicrob. Resist. Infect. Control. 2017, 6, 47. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.L.; Rello, J.; Marshall, J.; Silva, E.; Anzueto, A.; Martin, C.D.; Moreno, R.; Lipman, J.; Gomersall, C.; Sakr, Y.; et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA 2009, 302, 2323–2329. [Google Scholar] [CrossRef] [PubMed]
- Adhikari, N.K.; Fowler, R.A.; Bhagwanjee, S.; Rubenfeld, G.D. Critical care and the global burden of critical illness in adults. Lancet 2010, 376, 1339–1346. [Google Scholar] [CrossRef]
- Zante, B.; Reichenspurner, H.; Kubik, M.; Kluge, S.; Schefold, J.C.; Pfortmueller, C.A. Base excess is superior to lactate-levels in prediction of ICU mortality after cardiac surgery. PLoS ONE 2018, 13, e0205309. [Google Scholar]
- Watson, G.; Jallow, B.; Le Doare, K.; Pushparajah, K.; Anderson, S.T. Acute rheumatic fever and rheumatic heart disease in resource-limited settings. Arch. Dis. Child. 2015, 100, 370–375. [Google Scholar] [CrossRef]
- Kumar, R.K.; Tandon, R. Rheumatic fever & rheumatic heart disease: The last 50 years. Indian J. Med. Res. 2013, 137, 643–658. [Google Scholar]
- Seckeler, M.D.; Hoke, T.R. The worldwide epidemiology of acute rheumatic fever and rheumatic heart disease. Clin. Epidemiol. 2011, 3, 67–84. [Google Scholar] [CrossRef]
- Mirabel, M.; Grimaldi, A.; Freers, J.; Jouven, X.; Marijon, E. Access to cardiac surgery in sub-Saharan Africa. Lancet 2015, 385, 606. [Google Scholar] [CrossRef]
- Chavez-Lindell, T.; Kikwe, B.; Gikonyo, A.; Odoi, A. Patient characteristics and cardiac surgical outcomes at a tertiary care hospital in Kenya, 2008–2017: A retrospective study. PeerJ 2021, 9, e11191. [Google Scholar] [CrossRef]
- Yangni-Angate, K.H.; Meneas, C.; Diby, F.; Diomande, M.; Adoubi, A.; Tanauh, Y. Cardiac surgery in Africa: A thirty-five year experience on open heart surgery in Cote d’Ivoire. Cardiovasc. Diagn. Ther. 2016, 6 (Suppl 1), S44–S63. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| All (n = 611) | Medical (n = 86) | Surgical (n = 525) | p-Value | |
|---|---|---|---|---|
| Age, mean (SD) | 22.05 (12.6) | 26.03 (13.2) | 21.39 (12.45) | 0.0024 |
| Male, n (%) | 299 (48.94) | 40 (46.51) | 259 (49.33) | 0.7122 |
| Aged less than 15 years, n (%) | 200 (32.73) | 20 (23.25) | 180 (34.28) | 0.05787 |
| BMI, mean (SD) | 17.86 (3.99) | 18.41 (4.18) | 17.77 (9.95) | 0.06234 |
| CHD, n (%) | 497 (83.67) | 3 (3.66) | 94 (17.9) | 0.00146 |
| Patients with previous surgery, n (%) | 10 (1.64) | 1 (1.18) | 9 (1.71) | 1 |
| SOFA, mean (SD) | 4.7 (2.7) | 6.06 (3.63) | 4.49 (2.40) | <0.001 |
| Time from hospital to ICU admission (days), mean (SD) | 7.26 (9.43) | 4.24 (10.1) | 7.76 (9.23) | <0.001 |
| ICU length of stay (days), mean (SD) | 3.89 (4.79) | 4.53 (5.5) | 3.78 (4.66) | 0.0617 |
| Reintubation, n (%) | 16 (2.62) | 2 (2.32) | 14 (2.67) | 1 |
| Tracheostomy, n (%) | 5 (0.82) | 1 (1.16) | 4 (0.77) | 1 |
| Foley, n (%)—at least one | 606 (99.18) | 85 (98.84) | 521 (99.24) | 1 |
| n. of Foley, mean (SD) | 1.03 (0.24) | 1.05 (0.26) | 1.02 (0.23) | 0.1946 |
| Time with Foley (days), mean (SD) | 4.06 (4.83) | 5.07 (5.73) | 3.89 (4.65) | 0.0065 |
| CVC, n (%)—at least one | 604 (98.85) | 81 (94.19) | 523 (99.62) | <0.001 |
| n. of CVC, mean (SD) | 1.14 (0.57) | 1.23 (0.81) | 1.13 (0.52) | 0.1534 |
| Time with CVC, mean (SD) | 4.02 (5.48) | 4.96 (6.55) | 3.87 (5.28) | 0.07185 |
| CVVH, n (%)—at least one session | 31 (5.07) | 6 (6.98) | 25 (4.76) | 0.5468 |
| Time on CVVH (days), mean (SD) | 0.2 (1.25) | 0.22 (0.9) | 0.2 (1.30) | 0.39 |
| Blood Transfusion, n (%)—at least one | 245 (40.1) | 25 (29.07) | 220 (41.9) | 0.033 |
| Surgical (n = 525) | p-Value | ||
|---|---|---|---|
| Elective Group (n = 491) | Urgent Group (n = 34) | ||
| Age, mean (SD) | 21.31 (12.5) | 22.65 (11.9) | 0.5334 |
| Male, n (%) | 244 (49.69) | 15 (44.12) | 1 |
| Aged less than 15 years, n (%) | 170 (34.62) | 10 (29.41) | 0.6655 |
| BMI, mean (SD) | 17.82 (3.98) | 17.09 (3.43) | 0.3755 |
| CHD, n (%) | 93 (19.37) | 1 (3.12) | 0.0391 |
| Patients with previous surgery, n (%) | 9 (1.83) | 0 (0) | 0.9099 |
| SOFA, mean (SD) | 4.33 (2.34) | 6.71 (2.22) | <0.001 |
| Time from Hospital to ICU admission (days), mean (SD) | 7.98 (8.85) | 4.59 (13.4) | <0.001 |
| Time from Hospital to OT (days), mean (SD) | 8.03 (8.94) | 6.65 (13) | 0.03824 |
| ICU length of stay (days), mean (SD) | 3.43 (4.33) | 8.82 (6.19) | <0.001 |
| Reintubation, n (%)—at least one | 13 (2.65) | 1 (2.94) | 1 |
| Tracheostomy, n (%) | 3 (0.61) | 1 (2.94) | 0.6231 |
| Foley, n (%)—at least one | 487 (99.18) | 34 (100) | 1 |
| n. of Foley, mean (SD) | 1.02 (0.23) | 1.09 (0.29) | 0.0177 |
| Time with Foley (days), mean (SD) | 3.52 (4.36) | 9.32 (5.29) | <0.001 |
| CVC, n (%)—at least one | 489 (99.59) | 34 (100) | 1 |
| n. of CVC, mean (SD) | 1.1 (0.46) | 1.56 (0.99) | <0.001 |
| Time with CVC, mean (SD) | 3.48 (4.8) | 9.47 (8.14) | <0.001 |
| CVVH, n (%)—at least one | 19 (3.87) | 6 (16.67) | 0.0012 |
| Time on CVVH (days), mean (SD) | 0.17 (1.27) | 0.68 (1.65) | <0.001 |
| Blood Transfusion, n (%)—at least one | 197 (40.12) | 23 (67.65) | 0.003 |
| Number of valves repaired, mean (SD) | 1.36 (0.95) | 1.79 (0.91) | 0.0084 |
| ECC (minutes), mean (SD) | 96.61 (46.61) | 116.51 (49.27) | 0.0097 |
| Delayed chest closure | 10 (2.04) | 2 (5.88) | 0.391 |
| Reopening/reintervention | 21 (4.28) | 2 (5.88) | 0.9928 |
| All | Medical Group | Surgical Group | p-Value | ||
|---|---|---|---|---|---|
| Total number of infected patients, n (%) | 87 (14.2) | 22 (25.6) | 65 (12.4) | 0.004 | |
| Median number of isolates per patient (min–max) | 1 (1–9) | 1 (1–8) | 1 (1–9) | 1 | |
| Patient with one isolate (%) | 53 (60.9) | 13 (59.1) | 40 (61.5) | 1 | |
| Number of infected patients with at least one MDR, n (%) | 32 (36.8) | 9 (40.9) | 23 (35.4) | 0.8347 | |
| Total of isolates and rate for patient | 156 (1.8) | 41 (1.9) | 115 (1.8) | 0.8361 | |
| Types of infections | |||||
| Catheter-associated urinary tract infection | 34 (21.8) | 11 (26.8) | 23 (20) | 0.4908 | |
| Wound infection (surgical site) | 10 (6.4) | 5 (12.2) | 5 (4.35) | 0.1645 | |
| VAP | 57 (36.5) | 6 (14.6) | 51 (44.3) | 0.0013 | |
| Primary bloodstream infection | 39 (25) | 16 (39) | 23 (20) | 0.0274 | |
| CVC-related bloodstream infection | 7 (4.49) | 1 (2.44) | 6 (5.22) | 0.7653 | |
| Urinary tract-related bloodstream infection | 5 (3.21) | 2 (4.88) | 3 (2.61) | 0.8478 | |
| VAP-related bloodstream infection | 4 (2.56) | 0 | 4 (3.48) | 0.5258 | |
| Infection due to MDR isolates, n (%) * | 48 (30.8) | 15 (36.6) | 33 (28.7) | 0.4576 | |
| Elective | Urgent | p-Value | |||
| Total number of infected patients, n (%) | - | - | 55 (11.2) | 10 (29.4) | 0.0044 |
| Median number of isolates per patient (min–max) | 1 (1–9) | 2 (1–4) | 0.1651 | ||
| One isolate (%) | 36 (65.4) | 4 (40) | 0.2425 | ||
| Number of infected patients with at least one MDR, n (%) | 20 (36.4) | 3 (30) | 0.7789 | ||
| Total of isolates and rate per patient | 94 (1.7) | 21 (2.1) | 0.1193 | ||
| Types of Infections | |||||
| Catheter-associated urinary tract infection | - | - | 20 (21.3) | 3 (14.3) | 0.6727 |
| Wound infection (surgical site) | 3 (3.2) | 2 (9.5) | 0.4872 | ||
| VAP | 42 (44.7) | 9 (42.9) | 1 | ||
| Primary bloodstream infection | 20 (21.3) | 3 (14.3) | 0.6727 | ||
| CVC-related bloodstream infection | 4 (4.3) | 2 (9.5) | 0.6608 | ||
| Urinary tract-related bloodstream infection | 3 (3.2) | 0 | 0.9423 | ||
| VAP-related bloodstream infection | 2 (2.1) | 2 (9.5) | 0.3107 | ||
| Infection due to MDR isolates, n (%) * | 28 (29.8) | 5 (23.8) | 0.7789 | ||
| OR (95% CI) | p-Value | VIF | |
|---|---|---|---|
| No. of days spent in ICU | 1.5 (1.36–1.65) | 0.0302 | 1.06 |
| Medical group compared to surgical group | 2.23 (1.08–4.61) | <0.001 | 1.07 |
| SOFA | 1.18 (1.05–1.31) | 0.002 | 1.08 |
| pseudo R2 = 0.37 | AIC = 321.24 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spagnolello, O.; Fabris, S.; Portella, G.; Raafat Shafig Saber, D.; Giovanella, E.; Badr Saad, M.; Langer, M.; Ciccozzi, M.; d’Ettorre, G.; Ceccarelli, G. Rates and Determinants of Hospital-Acquired Infection among ICU Patients Undergoing Cardiac Surgery in Developing Countries: Results from EMERGENCY’NGO’s Hospital in Sudan. Antibiotics 2022, 11, 1227. https://doi.org/10.3390/antibiotics11091227
Spagnolello O, Fabris S, Portella G, Raafat Shafig Saber D, Giovanella E, Badr Saad M, Langer M, Ciccozzi M, d’Ettorre G, Ceccarelli G. Rates and Determinants of Hospital-Acquired Infection among ICU Patients Undergoing Cardiac Surgery in Developing Countries: Results from EMERGENCY’NGO’s Hospital in Sudan. Antibiotics. 2022; 11(9):1227. https://doi.org/10.3390/antibiotics11091227
Chicago/Turabian StyleSpagnolello, Ornella, Silvia Fabris, Gina Portella, Dimiana Raafat Shafig Saber, Elena Giovanella, Manahel Badr Saad, Martin Langer, Massimo Ciccozzi, Gabriella d’Ettorre, and Giancarlo Ceccarelli. 2022. "Rates and Determinants of Hospital-Acquired Infection among ICU Patients Undergoing Cardiac Surgery in Developing Countries: Results from EMERGENCY’NGO’s Hospital in Sudan" Antibiotics 11, no. 9: 1227. https://doi.org/10.3390/antibiotics11091227
APA StyleSpagnolello, O., Fabris, S., Portella, G., Raafat Shafig Saber, D., Giovanella, E., Badr Saad, M., Langer, M., Ciccozzi, M., d’Ettorre, G., & Ceccarelli, G. (2022). Rates and Determinants of Hospital-Acquired Infection among ICU Patients Undergoing Cardiac Surgery in Developing Countries: Results from EMERGENCY’NGO’s Hospital in Sudan. Antibiotics, 11(9), 1227. https://doi.org/10.3390/antibiotics11091227