
Point-of-Care and Rapid Tests for the Etiological Diagnosis of Respiratory Tract Infections in Children: A Systematic Review and Meta-Analysis


 , ,
, ,  ,
,
Abstract
1. Introduction
2. Results

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Year of Publication | Study Design | Study Location | Study Period | Single or Multi-Center | Age | Care Setting | N° Patients | Type of Test | Outcomes | NIH Tool | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PR | DOT | LOS | COST | PO | |||||||||||
| Nitsch-Osuch et al. [8] | 2017 | QE | POL | January 2015–March 2015 January 2016–March 2016 | Single | <5 years | Inpatient | 115 | RIDT | X | X | FAIR | |||
| Vecino-Ortiz et al. [9] | 2018 | QE | GBR | 2013–2014 2014–2015 | Single | Children | Inpatient | 574 | RIDT, Rapid VRS test | X | X | X | X | FAIR | |
| Abanses et al. [10] | 2006 | RCT | USA | December 2002–March 2003 | Single | 3–36 months | ED | 1007 | RIDT | X | X | X | FAIR | ||
| Diallo et al. [11] | 2019 | OR | FRA | 2013–2015 | Single | 1 month–18 years | ED | 241 | RIDT | X | FAIR | ||||
| Noyola et al. [12] | 2000 | OR | USA | July 1995– June 1997 | Single | Children | ED | 1530 | RIDT | X | X | X | X | GOOD | |
| Özkaya et al. [13] | 2009 | OP | TUR | November 2006–March 2007 | Single | 3–14 years | ED | 97 | RIDT | X | FAIR | ||||
| Bonner et al. [14] | 2003 | RCT | USA | January 2002–March 2002 | Single | 2 months–21 years | ED | 391 | RIDT | X | X | X | GOOD | ||
| Cantais et al. [15] | 2019 | OP | FRA | January 2016–March 2016 | Single | 0–16 years | ED | 514 | RIDT | X | FAIR | ||||
| Iyer et al. [16] | 2006 | Quasi-RCT | USA | January 2003–March 2003 December 2003–January 2004 | Single | 2–24 months | ED | 700 | RIDT | X | X | X | FAIR | ||
| Jacob et al. [17] | 2020 | OR | AUS | August 2017–September 2017 | Single | <16 years | ED | 1451 | RIDT | X | X | FAIR | |||
| Jun et al. [18] | 2016 | QE | KOR | December 2008–January 2009 February 2013–March 2013 | Single | <16 years | ED | 342 | RIDT | X | X | FAIR | |||
| Li-Kim-Moy et al. [19] | 2016 | OR | AUS | 2009 | Single | <18 years | ED | 364 | RIDT | X | X | X | FAIR | ||
| Sharma et al. [20] | 2002 | OR | USA | November 1998–March 1999 November 1999–March 2000 | Single | 2 months–2 years | ED | 72 | RIDT | X | X | FAIR | |||
| Patel et al. [21] | 2020 | QE | USA | November–March of 2014 to 2017 November–March of 2017 to 2018 | Single | 3 months–18 years | ED | 5307 | RIDT | X | X | X | FAIR | ||
| Pierron et al. [22] | 2008 | OP | FRA | January 2007–March 2007 | Single | 1 month–6 years | ED | 177 | RIDT | X | FAIR | ||||
| Benito-Fernandez et al. [23] | 2006 | OP | ESP | November–December 2003 December 2004–February 2005 | Single | 0–14 years | ED | 206 | RIDT | X | X | FAIR | |||
| Poehling et al. [24] | 2006 | RCT | USA | 2002–2004 | Multi-center | <5 years | ED + outpatient | 468 | RIDT | X | GOOD | ||||
| Jennings et al. [25] | 2009 | OP | DEU | January 2007– April 2007 | Multi-center | 1–12 years | Outpatient | 16907 | RIDT | X | X | FAIR | |||
| Nitsch-Osuch et al. [26] | 2013 | OP | POL | 2009/2010–2010/2011 | Multi-center | <5 years | Outpatient | 256 | RIDT | X | X | FAIR | |||
| Van Esso et al. [27] | 2019 | OP | ESP | 2016–2017 | Multi-center | 0–6 years | Outpatient | 1170 | RIDT | X | POOR | ||||
| Cohen et al. [28] | 2007 | OP | FRA | 2004–2005 | Multi-center | Children | Outpatient | 602 | RIDT | X | X | FAIR | |||
| de La Rocque et al. [29] | 2009 | OP | FRA | December 2006–April 2007 | Multi-center | Children | Outpatient | 695 | RIDT | X | X | GOOD | |||
| Keske et al. [30] | 2018 | QE | TUR | January 2015–December 2016 | Single | <16 years | Inpatient | 258 | FA-RP | X | X | FAIR | |||
| Kitano et al. [31] | 2019 | QE | JPN | March 2018 – April 2019 March 2012–March 2018 | Single | nd | Inpatient | 1281 | FA-RP | X | X | X | FAIR | ||
| Lee et al. [32] | 2020 | QE | USA | December 2009–July 2012 August 2012 – June 2016 | Single | <18 years | Inpatient | 5142 | FA-RP | X | X | X | FAIR | ||
| Reischl et al. [33] | 2020 | QE | DEU | February 2016–February 2017 February 2017–April 2018 | Single | 0–2 years | Inpatient | 786 | FA-RP | X | X | X | X | FAIR | |
| Schulert et al. [34] | 2013 | OR | USA | August 2009–December 2010 | Single | 0–14 years | Inpatient | 790 | FA-RP | X | X | FAIR | |||
| Subramony et al. [35] | 2016 | QE | USA | June 2010 – June 2012 October 2012–May 2014 | Single | 0–18 years | Inpatient | 4779 | FA-RP | X | FAIR | ||||
| Walls et al. [36] | 2016 | OR | NZL | Winter months 2012–2015 | Single | 3 months–5 years | Inpatient | 237 | FA-RP | X | X | FAIR | |||
| Yoshida et al. [37] | 2021 | QE | JPN | December 2017–November 2018 March 2019–February 2020 | Single | 0–18 years | Inpatient | 181 | FA-RP | X | X | X | FAIR | ||
| McCulloh et al. [38] | 2013 | OR | USA | October 2009–April 2010 October 2010–April 2011 | Single | 0–18 years | Inpatient | 1727 | FA-RP | X | X | X | FAIR | ||
| McFall et al. [39] | 2017 | OR | USA | November 2012–August 2015 | Single | 1–3 months | Inpatient | 176 | FA-RP | X | X | FAIR | |||
| Iroh Tam et al. [40] | 2017 | OR | USA | January 2011 – April 2015 | Multi-center | <18 years | ED + inpatient | 1625 | FA-RP | X | X | X | FAIR | ||
| Kim et al. [41] | 2021 | QE | KOR | November 2015–June 2016 November 2016–July 2018 | Single | 1 month–18 years | ED + inpatient | 915 | FA-RP | X | X | X | FAIR | ||
| Rogers et al. [42] | 2015 | QE | USA | November 2011–January 2012 November 2012–January 2013 | Single | 3 months–21 years | ED + inpatient | 1136 | FA-RP | X | X | X | FAIR | ||
| Busson et al. [43] | 2019 | QE | BEL | February 2016–March 2016 | Single | Adults and children, separated data | ED | 142 | FA-RP | X | X | X | FAIR | ||
| Byington et al. [44] | 2002 | OR | USA | December 2000–February 2001 December 2001–January 2002 | Single | <19 years | ED | 338 | FA-RP | X | X | FAIR | |||
| Crook et al. [45] | 2020 | QE | USA | January 2011–December 2014 January 2015– April 2018 May 2018– June 2019 | Single | <90 days | ED | 5317 | FA-RP | X | X | X | FAIR | ||
| Dimopoulou et al. [46] | 2020 | OP | GRC | February 2019 | Single | 0–16 years | ED | 80 | FA-RP | X | X | FAIR | |||
| Rao et al. [47] | 2021 | RCT | USA | December 2018–November 2019 | Single | 1 month–18 | ED | 920 | FA-RP | X | X | X | GOOD | ||
| Echavarría et al. [48] | 2018 | RT | ARG | April–November 2016 April–October 2017 | Single | 2 months–6 years | ED | 156 | FA-RP | X | X | X | GOOD | ||
| May et al. [49] | 2019 | RCT | USA | December 2016–April 2018 | Single | 1–17 years | ED | 71 | FA-RP | X | X | X | GOOD | ||
| Wishaupt et al. [50] | 2011 | RCT | NLD | November 2007–May 2008 October 2008–March 2009 | Single | 0–12 years | ED + outpatient | 583 | FA-RP | X | X | GOOD | |||
| Beal et al. [51] | 2020 | QE | USA | January 2018–January 2019 | Multi-center | <21 years | Outpatient | 430 | FA-RP | X | X | X | FAIR | ||
| Thibeault et al. [52] | 2007 | OR | CAN | Winter 2001–2002 and 2002–2003 | Multi-center | 0–3 years | Inpatient | 448 | Rapid RSV test | X | X | FAIR | |||
| Schnell et al. [53] | 2017 | OR | USA | November–March of 2008–2013 | Single | 2 months–2 years | ED | 713 | Rapid RSV test | X | X | FAIR | |||
| O’ Callaghan et al. [54] | 2019 | QE | AUS | May 2017– August 2017 May 2018–August 2018 | Single | Children | ED | 642 | Rapid PCR for influenza and RSV | X | X | FAIR | |||
| Mitchell et al. [55] | 2018 | QE | USA | November 2014–March 2015 | Single | <18 years | ED | 2171 | Rapid PCR for influenza and RSV | X | FAIR | ||||
| Schneider et al. [56] | 2018 | OP | DNK | February 2018–July 2018 | Multi-center | 0–18 years | ED | 180 | Rapid PCR for influenza and RSV | X | X | FAIR | |||
| Hayashi et al. [57] | 2018 | OP | JPN | May 2016– April 2017 | Single | <18 | Inpatient | 375 | Mycoplasma PCR | X | FAIR | ||||
| Ayanruoh et al. [58] | 2009 | QE | USA | September 2005–September 2007 | Single | 3–18 years | ED | 8280 | RSTs | X | FAIR | ||||
| Bird et al. [59] | 2021 | QE | GBR | October–November 2014 August–November 2015 September–November 2016 | Single | 6 months–16 years | ED | 605 | RSTs | X | FAIR | ||||
| Halverson et al. [60] | 2011 | QE | USA | October 2006–December 2009 | Multi-center | nd | ED | nd | RSTs | X | POOR | ||||
| Kose et al. [61] | 2016 | QE | TUR | February 2012–May 2014 | Single | 3–14 years | ED | 223 | RSTs | X | X | FAIR | |||
| Małecki et al. [62] | 2017 | QE | POL | October 2013– April 2014 | Multi-center | 2–15 years | Outpatient | 1307 | RSTs | X | X | X | X | FAIR | |
| Maltezou et al. [63] | 2008 | OP | GRC | December 2005–June 2006 September 2006–June 2007 | Multi-center | 2–14 years | Outpatient | 820 | RSTs | X | X | X | X | FAIR | |
| Rao et al. [64] | 2019 | OP | USA | Fall-winter 2016–2017 | Single | 3–18 years | Outpatient | 275 | RSTs and PCR Strep A test | X | FAIR | ||||
| Authors and Year of Publication | N° Patients | Type of Test | Outcomes | NIH Tool | ||||
|---|---|---|---|---|---|---|---|---|
| PR | DOT | LOS | COST | PO | ||||
| Nitsch-Osuch et al., 2017 [8] | 115 | RIDT | Antibiotic therapy was statistically more frequently administered when RIDT was not available (93% vs. 64%; p < 0.05) | Oseltamivir was statistically more prescribed when RIDT was available (64% of patients with influenza received an antiviral, none of the children received an antiviral without RIDT) | FAIR | |||
| Vecino-Ortiz et al., 2018 [9] | 574 | RIDT, rapid VRS test | No significant differences in the antibiotic prescription rate between periods in those positive for influenza and negative for both influenza and RSV | There was no significant difference between the periods for the total length of stay (median = 2 days for both periods, p = 0.23) | Reductions in the average reimbursement charge for patients with a negative influenza and RSV test. No change in reimbursement for patients with proven influenza or RSV infection | Small but significant increase in the cost of drugs between periods 1 and 2 for admissions in which the patients were positive for influenza and/or RSV | FAIR | |
| Abanses et al., 2006 [10] | 1007 | RIDT | Significant reduction in antibiotic prescription in those testing positive for influenza (215 vs. 102, RR 0.85, CI 95% 0.7–1.02) | Time in ED was significantly less in the intervention group (195 vs. 156 min; 95% CI for the difference, 19–60) | Total medical charges were significantly less in the intervention group (USD 666 vs. USD 393; 95% CI for the difference, 153–392) | FAIR | ||
| Diallo et al., 2019 [11] | 241 | RIDT | The mean length of stay in the PED was significantly lower in the positive RDT group: 4.0 h vs. 7.4 h (p < 10−6) | FAIR | ||||
| Noyola et al., 2000 [12] | 1530 | RIDT | Patients discharged from the ED with a positive influenza test were less likely to receive antibiotics than those with a negative test (20% vs. 53%; p < 0.04) Patients admitted to the hospital with a positive EIA test were as likely to receive antibiotics as those without a rapid diagnosis | Duration of antibiotic administration was significantly shorter in the group with a positive influenza test (3.5 vs. 5.4 days; p = 0.03) | Patients with a positive influenza test were more likely to have a shorter duration of admission than the control group (4.3 mean days versus 7.4; p = 0.02) | Patients with a positive influenza test were more likely to receive antiviral therapy than the control group (25% vs. 0 and 1.8%; p < 0.001) | GOOD | |
| Özkaya et al., 2009 [13] | 97 | RIDT | Patients in group testing prior to prescription were less likely to be prescribed antibiotics when compared to those in the group in which rapid testing was not considered for prescription (32% vs. 100%, respectively, p < 0.0001) | FAIR | ||||
| Bonner et al., 2003 [14] | 391 | RIDT | Reduction in antibiotic prescription in the group in which the results of the rapid test was known in comparison to the group of unknown (7/96 vs. 26/106, p < 0.001); no difference between negative test and negative unaware test (27/97 vs. 27/92, p = 0.0818) | Reduction in the length of stay in the group in which the results of the rapid test were known in comparison to the group of unknown (25 min vs. 49 min, p < 0.001); no difference between the negative test and negative unaware test (45 min vs. 42 min, p = 0.549) | Increase in antiviral prescription in the group in which the results of the rapid test were known in comparison to the group of unknown (18/96 vs. 7/106, p = 0.02); no difference between negative test and negative unaware test (0/97 vs. 2/92, p = 0.236) | GOOD | ||
| Cantais et al., 2019 [15] | 514 | RIDT | Reduction in antibiotic prescriptions, 60 of 245 patients (24.5%) received antibiotics in the DIA negative group, versus 25 of 262 (9.5%) in the positive one (p < 0.001) | FAIR | ||||
| Iyer et al., 2006 [16] | 700 | RIDT | No significant differences were demonstrated between the POCT and standard test groups with respect to antibiotic prescription | No significant differences were demonstrated between the POCT and standard test groups with respect to lengths of stay | No significant differences were demonstrated between the POCT and standard test groups with respect to visit-associated costs | FAIR | ||
| Jacob et al., 2020 [17] | 1451 | RIDT | Antibiotics were used more in patients with ILI with no RIDT (15.2% in the ILI group vs. 2.7% in the laboratory RIDT group and 11.2% in the ED RIDT group; p < 0.0001) | Patients for whom RIDT was performed at the laboratory had a shorter length of stay when compared to patients for whom RIDT was performed bedside in the ED (4.7 and 5.3 h, respectively; p < 0.0001), | FAIR | |||
| Jun et al., 2016 [18] | 342 | RIDT | Reduction in antibiotic prescription in RAT-positive patients, after the 2009 influenza pandemic (none of the pediatric patients received antibiotics) | The duration of ER stay in discharged patients was 268.9 ± 144.2 min in patients with the use of a RAT kit and 210.5 ± 205.3 min in patients with no use of a RAT kit after the 2009 influenza pandemic | FAIR | |||
| Li-Kim-Moy et al., 2016 [19] | 364 | RIDT | Compared with standard testing (n = 65), children diagnosed by positive POCT (n = 236) had a reduction in antibiotic use (odds ratio 0.42, p = 0.003) | Compared with standard testing, children diagnosed by positive POCT had a shorter median hospital LOS by 1 day (p = 0.006). POCT did not decrease LOS in ED | Compared with standard testing, children diagnosed by positive POCT had increased antiviral prescription (odds ratio 3.1, p < 0.001) | FAIR | ||
| Sharma et al., 2002 [20] | 72 | RIDT | Fewer patients in the early diagnosis group received ceftriaxone sodium compared with the late diagnosis group (2% vs. 24%, p = 0.006) | No significant differences were demonstrated between the POCT and standard test groups with respect to lengths of stay | FAIR | |||
| Patel et al., 2020 [21] | 5307 | RIDT | There was no significant difference in rates of antibiotics used | The median LOS decreased from 239 min in the pre-POC period to 232 min in the post-POC period (p < 0.05) | There were increased rates of oseltamivir used in the post-POC period (21.2% vs. 13.3%, p < 0.05 | FAIR | ||
| Pierron et al., 2008 [22] | 177 | RIDT | There was not any significant difference concerning antibiotic prescriptions | FAIR | ||||
| Benito-Fernandez et al., 2006 [23] | 206 | RIDT | There was a significant reduction in the use of antibiotics (38.5% vs. 0%, p < 0.01) | There was a significant reduction in the mean length of stay in the ED (192.9 versus 116.2 min) (p < 0.01) | FAIR | |||
| Poehling et al., 2006 [24] | 468 | RIDT | There was no difference in antibiotic prescribing | GOOD | ||||
| Jennings et al., 2009 [25] | 16907 | RIDT | Antibiotics were less commonly prescribed for children who were influenza positive by rapid test (3.5% (271/7685) versus 17.2% (125/725) for symptom assessment alone) | The antiviral oseltamivir was prescribed for 24.6% (178/725) of children who were influenza positive by symptom assessment alone and 60.1% (4618/7685) of children who were influenza positive by rapid test | FAIR | |||
| Nitsch-Osuch et al., 2013 [26] | 256 | RIDT | Antibiotics were administered more often in the control group compared with the rapid test group (respectively, for 16% vs. 7%). No child with a positive result of RIDT was prescribed an antibiotic | The antiviral treatment (oseltamivir) was prescribed only for four children with positive results of RIDT | FAIR | |||
| Van Esso et al., 2019 [27] | 1170 | RIDT | Influenza-confirmed patients received fewer antibiotics during the 10 days after influenza diagnosis but not statistically significant compared with the groups with a clinical diagnosis of influenza without a microbiologic confirmation | POOR | ||||
| Cohen et al., 2007 [28] | 602 | RIDT | The antibiotic prescription was overall low (9.5% with RIDT vs. 3.9% without RIDT, p = 0,008), and primarily when the result of RIDT was negative (15.7% if RIDT– vs. 4.3% if RIDT+, p = 0.0003) | The pediatricians using RIDT prescribed with positive tests more oseltamivir (68.5 vs. 1.9%, p < 0.0001) | FAIR | |||
| de La Rocque et al., 2009 [29] | 695 | RIDT | The RIDT+ group received antibiotics in 7.6% of cases, RIDT− in 18.5% (p < 0.0001) | The RIDT+ group received an antiviral in 64.7% and the RIDT− group received no antiviral (p < 0.0001) | GOOD | |||
| Keske et al., 2018 [30] | 258 | FA-RP | Significant decrease in antibiotic use (44.5% in 2015 and 28.8% in 2016, p = 0.009) | The duration of antibiotic use after the detection of virus was significantly decreased in children (p < 0.001) | FAIR | |||
| Kitano et al., 2019 [31] | 1281 | FA-RP | The DOT/case was 12.82 vs. 8.56 (p < 0.001), in the rapid antigen test and mPCR groups, respectively | The LOS was 8.18 vs. 6.83 days (p = 0.032) in the rapid antigen test and mPCR groups, respectively | The total costs during admissions were 258,824 (USD 2331.7) and 243,841 (USD 2196.8)/case, in the rapid antigen test and mPCR groups, respectively | FAIR | ||
| Lee et al., 2020 [32] | 5142 | FA-RP | Patients tested with RP were less likely to receive empiric antibiotics (OR: 0.45; p < 0.001; 95% CI: 0.39, 0.52) compared to RVP patients | Patients tested with RP had a shorter duration of empiric broad-spectrum antibiotics (6.4 h vs. 32.9 h; p < 0.001) compared to RVP patients | RP influenza patients had increased oseltamivir use post-test compared to RVP influenza patients (OR: 13.56; p < 0.001; 95% CI: 7.29, 25.20). | FAIR | ||
| Reischl et al., 2020 [33] | 786 | FA-RP | The binary logistic regression analysis shows no significant (p = 0.784) impact of the FA-RP or the multiplex RT-PCR on the antibiotic treatment | The diagnostic method, FA-RP (8.6 days) or multiplex RT-PCR (9.1 days), showed no significant (p = 0.592) impact on the duration of antibiotic treatment in the linear logistic regression analysis | The mean hospital length of stay for both study groups was 4.7 days. The diagnostic method, FA or multiplex RT-PCR, showed no significant impact on the length of hospital stay in the linear regression analysis. | No significant difference in antiviral prescriptions | FAIR | |
| Schulert et al., 2013 [34] | 790 | FA-RP | The median duration of IV antibiotics for patients with a positive RVP was 55 h, compared with 96 h for patients with a negative RVP (p = 0.03) | The median length of stay for patients with a positive RVP was 3 days, compared with 4 days for patients with a negative RVP (p = 0.057) | FAIR | |||
| Subramony et al., 2016 [35] | 4779 | FA-RP | Subjects in the mPCR group received fewer days of antibiotics than subjects in the non-mPCR group (4 vs. 5 median antibiotic days, p < 0.01) | FAIR | ||||
| Walls et al., 2016 [36] | 237 | FA-RP | A significantly larger proportion of children who had an NPS sample taken (42/146, 36%) received no empiric antibiotics compared to children who did not have a sample taken (7/91, 7.7%, p < 0.001) | Of those who did have an NPS sample taken, 17 of 146 (11.6%) had their antibiotics discontinued prior to or at the time of discharge compared with only 3 of 91 (3.3%) of those who did not have an NPS sample (p < 0.025) | FAIR | |||
| Yoshida et al., 2021 [37] | 181 | FA-RP | We did not observe differences in the use of antibiotics between the pre- and post-mPCR periods (p = 0.14) | We did not observe differences in the duration of antibiotic usage between the pre- and post-mPCR periods (p = 0.45) | We did not observe differences in the length of stay between the pre- and post-mPCR periods (p = 0.94) | FAIR | ||
| McCulloh et al., 2013 [38] | 1727 | FA-RP | Children with a positive RVP test result received antibiotics less often (363 of 703 (51.6%) vs. 71 of 106 (67.0%); p = 0.003) | In total, 21 of 348 (6.0%) children who were positive for a viral pathogen by RVP had antibiotics discontinued within 24 h after RVP test results were available, but no children with negative RVP results had antibiotics subsequently stopped | Children with a positive RVP test result received oseltamivir more often (76.9% vs. 18%; p < 0.001) | FAIR | ||
| McFall et al., 2017 [39] | 176 | FA-RP | Duration of antimicrobial consumption was significantly decreased in patients with a positive FA-RP compared to infants with a negative test (mean rank 2.8 vs. mean rank 5.2 days), p < 0.001) | For all infants with a positive FA-RP result, LOS was significantly decreased compared with infants with a negative FA-RP result (5.7 vs. 10.4 days, p = 0.017) | FAIR | |||
| Iroh Tam et al., 2017 [40] | 1625 | FA-RP | No difference in antibiotic prescription for all types of antibiotics | Patients with a positive test from RVPP had shorter LOS (p = 0.0503) | Hospital charges for patients with a positive test from RVPP were lower, but not significantly so | No difference in antiviral prescription (p = 0.76) | FAIR | |
| Kim et al., 2021 [41] | 915 | FA-RP | FA-RP reduced intravenous (IV) antibiotic use (p = 0.002) | FA-RP reduced the duration of intravenous (IV) antibiotic use, for pediatric patients (p < 0.001) | FA-RP reduced the lead time, waiting time, turnaround time, and length of hospital stay (p = 0.004) | FAIR | ||
| Rogers et al., 2015 [42] | 1136 | FA-RP | The number of patients receiving antibiotics and the inpatient LOS did not differ in the 2 groups | Duration of antibiotic use decreased for patients in the post-FA-RP group by 0.4 days (p = 0.003) | The LOS in the ED increased by 26 min in the post-RRP group (p = 0.002) | FAIR | ||
| Busson et al., 2019 [43] | 142 | FA-RP | Results from the FilmArray Respiratory Panel do not appear to impact antibiotic prescription | The mean length of stay was not significantly different between the two groups (3.9 days for the group with a positive FA result vs. 5.2 days for the group with a negative FA result; p = 0.286) | No difference in oseltamivir prescription | FAIR | ||
| Byington et al., 2002 [44] | 338 | FA-RP | Test-positive patients had fewer discharge prescriptions for oral antibiotics (37% vs. 52%, p = 0.02) when compared with test-negative patients. Intravenous antibiotics were initiated less often for test-positive patients during the second winter season than during the first (26% vs. 44%, p = 0.008) | Test-positive patients had fewer days using intravenous antibiotics (2.4 vs. 4, p = 0.04), fewer days using oral antibiotics (0.25 vs. 2.5, p = 0.04), when compared with test-negative patients | FAIR | |||
| Crook et al., 2020 [45] | 5317 | FA-RP | Following introduction of mPCR testing, the percentage of patients who did not receive antimicrobials increased from 32.4% to 43.1% (difference, 10.8%; 95% CI, 6.5–15%) | Median antibiotic duration decreased by 0.47 days (95% CI, 0.16–0.51) | There was a significant reduction in LOS (p < 0.001) | FAIR | ||
| Dimopoulou et al., 2020 [46] | 80 | FA-RP | The implementation of a rapid molecular test had no impact on antibacterial prescription (10% vs. 13.3%). | The implementation of a rapid molecular test had no impact on antiviral prescription | FAIR | |||
| Rao et al., 2021 [47] | 920 | FA-RP | In the intention-to-treat intervention group (result known), children were more likely to receive antibiotics (relative risk (RR), 1.3; 95% CI, 1.0–1.7) compared to the control group (result not known) | No significant differences in length of stay between the two groups | No significant differences in antiviral prescribing between the two groups | GOOD | ||
| Echavarría et al., 2018 [48] | 156 | FA-RP | Diagnosis with FA-RP was associated with significant changes in medical management including withholding antibiotic prescriptions (OR:12.23, 95%CI:1.56–96.09) | The median LOS was lower for the FA-RP group (4 days) than the control group (10 days) although the difference was not statistically significant (p = 0.382) | Oseltamivir usage was very low and no significant changes in treatment with the drug were observed between the two study groups | GOOD | ||
| May et al., 2019 [49] | 71 | FA-RP | In total, 20 (22%) RP patients and 33 (34%) usual-care patients received antibiotics during the ED visit (–12%; 95% confidence interval, –25% to 0.4%; p = 0.06/0.08) | There was no significant difference in length of ED stay, or hospital stay among admitted patients between the 2 groups | No significant difference in antiviral prescription (+3% (–5% to –10%) 0.53/0.61) | GOOD | ||
| Wishaupt et al., 2011 [50] | 583 | FA-RP | Mean durations of antibiotic treatment, if antibiotic treatment was started, did not differ significantly between the groups | There was a trend toward a shorter length of hospital stay in the intervention group, but the difference was not statistically significant | GOOD | |||
| Beal et al., 2020 [51] | 430 | FA-RP | Appropriate treatment occurred for 93.6% of patients when the FA-RP was performed (Clinic A) versus 87.9% of patients who had only antigen tests performed (Clinic B, p = 0.0445) | Utilization of FA-RP testing also significantly reduced appointment duration time (48.0 versus 54.9 min, p = 0.0009) | Patients tested with FA-RP received less oseltamivir compared to children tested with an antigen test (p = 0.0018) | FAIR | ||
| Thibeault et al., 2007 [52] | 448 | Rapid RSV test | There was no significant difference between children with positive and negative RSV RADT results in the percentage receiving IV antibiotics only (10% versus 7%, p = 0.61); PO antibiotics only (38% versus 28%, p = 0.17); or both PO and IV antibiotics (52% versus 65%, p = 0.12) | At 24, 48, or 72 h, stopping or switching of IV antibiotics was not influenced by the RADT result in any of the four strata combining age and presence of pneumonia (<3 months and no pneumonia; <3 months without pneumonia; ≥3 months with pneumonia; ≥3 months with- out pneumonia) | FAIR | |||
| Schnell et al., 2017 [53] | 713 | Rapid RSV test | Antibiotic administration within the ED did not differ between those testing positive for RSV versus those testing negative | The mean time in the department was not statistically significant between the 2 groups at 174.1 (SD, 89.8) minutes for the RSV-negative group and 165.2 (SD, 84.6) minutes for the RSV-positive group | FAIR | |||
| O’ Callaghan et al., 2019 [54] | 642 | Rapid PCR for influenza and RSV | 26.3% of positive influenza A/B RSV patients were treated with antibiotics in 2017, whereas 21.3% were treated with antibiotics in 2018 (p = 0.45) | According to time to discharge in the ED, there were no differences between positive and negative patients (p = 0.85) | FAIR | |||
| Mitchell et al., 2018 [55] | 2171 | Rapid PCR for influenza and RSV | Analysis of the post-implementation period revealed a significantly lower percentage (14.3%, p < 0.001) of negative patients receiving antiviral therapy compared to the pre-implementation period, with no difference in prescription of oseltamivir in those testing positive | FAIR | ||||
| Schneider et al., 2018 [56] | 180 | Rapid PCR for influenza and RSV | A positive POCT result significantly reduced antibiotic prescription (p < 0.0011) | A positive POCT result significantly reduced median hospitalization time by 14.2 h for children | FAIR | |||
| Hayashi et al., 2018 [57] | 375 | Mycoplasma PCR | Antimicrobial agents for atypical pathogens (macrolides, tetracyclines, or quinolones) were prescribed in 97.3% (217/223) at the initial evaluation, and their prescription rates increased to 99.1% (221/223) during management | FAIR | ||||
| Ayanruoh et al., 2009 [58] | 8280 | RSTs | Rapid strep testing was associated with a lower antibiotic prescription rate for children with pharyngitis (41.38% for those treated in the pre-RST phase versus 22.45% for those treated in the post-RST phase; p < 0.001) | FAIR | ||||
| Bird et al., 2021 [59] | 605 | RSTs | The baseline prescribing rate was 79%, whereas rates after intervention were 24% in 2015 and 28% in 2016 | FAIR | ||||
| Halverson et al., 2011 [60] | nd | RSTs | Implementation of POCT was shown to provide a statistically significant drop in LOS of patients who had group A strep testing performed on them, discharging them 25–30 min faster than other patients on average | POOR | ||||
| Kose et al., 2016 [61] | 223 | RSTs | Antibiotic prescription decreased by 42.6% after learning RST results | Antibiotic costs in non-Group A streptococcus pharyngitis, Group A streptococcus pharyngitis, and all subjects’ groups decreased by 80.8%, 48%, and 76.4%, respectively | FAIR | |||
| Małecki et al., 2017 [62] | 1307 | RSTs | Reduction in antibiotic use by 5.1%. | The anticipated cost of treatment decreased by 17% | FAIR | |||
| Maltezou et al., 2008 [63] | 820 | RSTs | Pediatricians without access to laboratory tests were more likely to prescribe antibiotics compared with pediatricians with access to tests (72.2% versus 28.2%, p < 0.001) | FAIR | ||||
| Rao et al., 2019 [64] | 275 | RSTs and PCR Strep A test | The use of POC PCR resulted in the appropriate use of antibiotics in 97.1% of cases compared with 87.5% of cases for the standard of care, RST plus confirmatory bacterial culture (p = 0.0065) | FAIR | ||||
2.1. Implementation Setting
2.1.1. Hospital Setting: Inpatient—Emergency Department
2.1.2. Outpatient—Primary Care
2.2. Implementation of Rapid Tests or POCTs and Outcomes
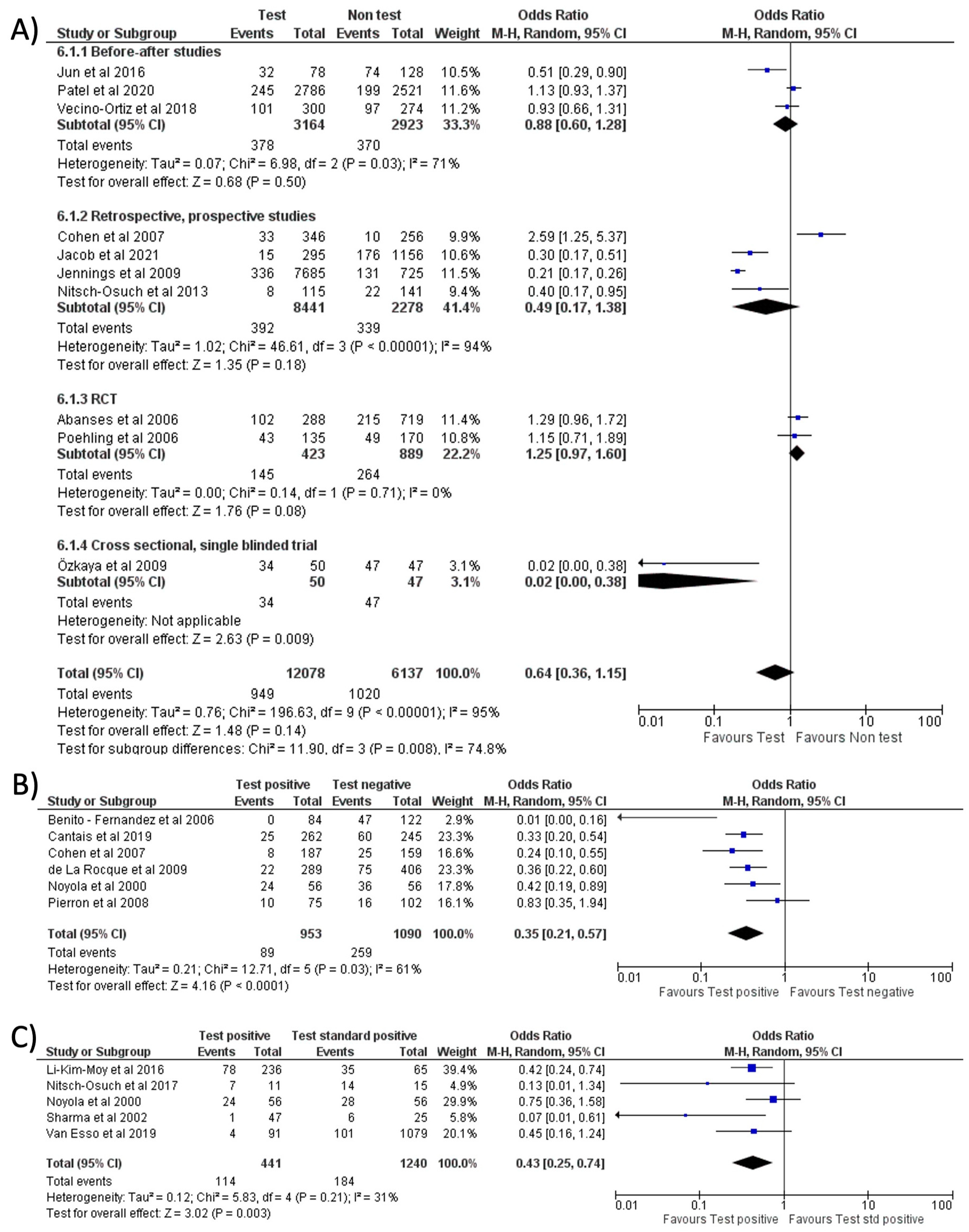
2.2.1. Antibiotics Prescription
2.2.2. Oseltamivir Prescription
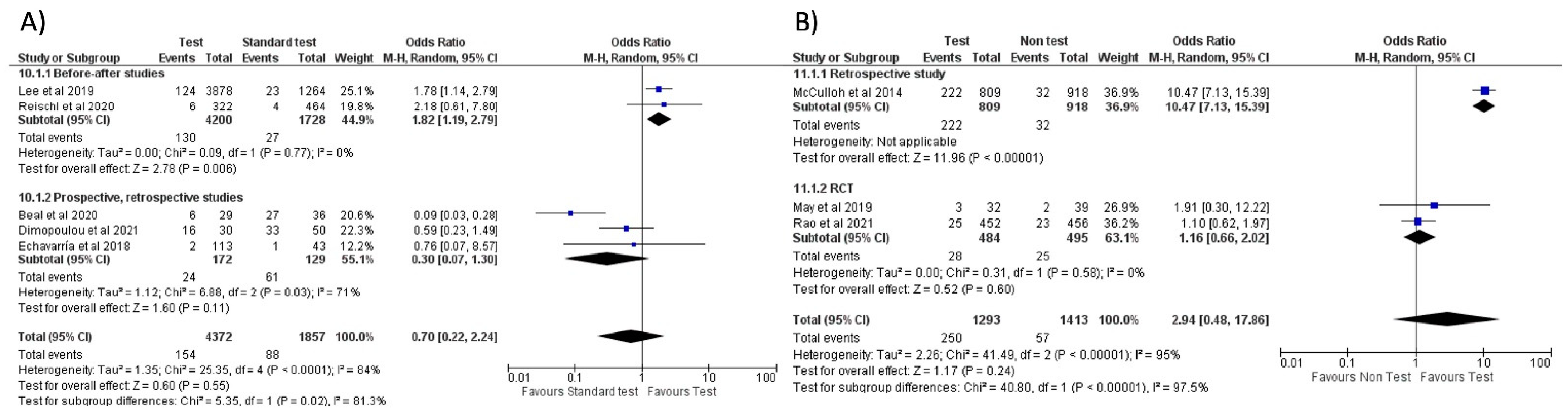
2.2.3. Length of Stay
2.2.4. Days of Therapy
2.2.5. Healthcare Cost
2.3. Quality Assessment of Studies
3. Discussion
Limitations
4. Materials and Methods
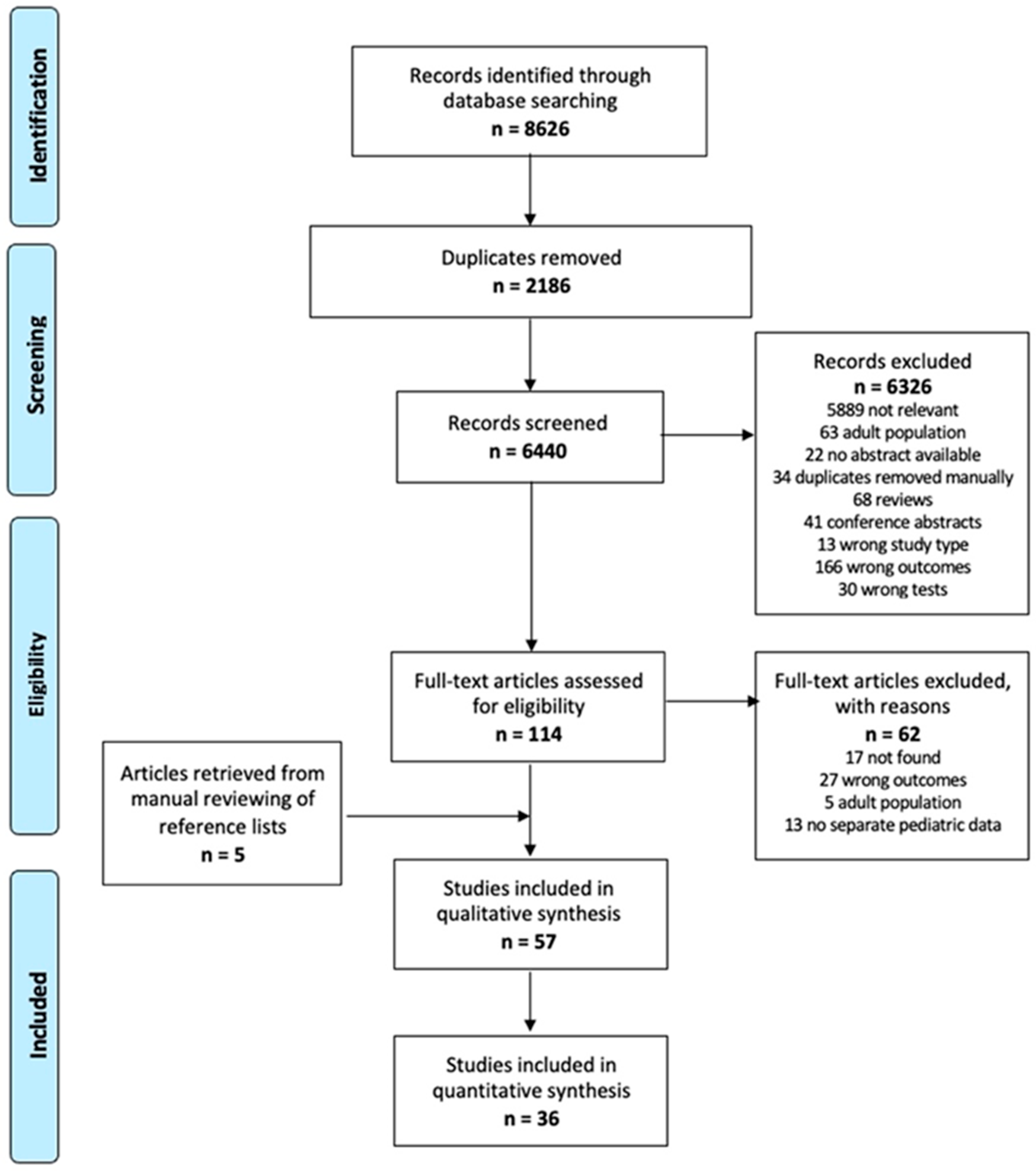
4.1. Study Design and Search Strategy
4.2. Inclusion Criteria and Outcomes
4.3. Exclusion Criteria
4.4. Study Selection
4.5. Data Collection
4.6. Risk of Bias in Individual Studies
4.7. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Sands, R.; Shanmugavadivel, D.; Stephenson, T.; Wood, D. Medical problems presenting to paediatric emergency departments: 10 Years on. Emerg. Med. J. 2012, 29, 379–382. [Google Scholar] [CrossRef]
- Dellit, T.H.; Owens, R.C.; McGowan, J.E.; Gerding, D.N.; Weinstein, R.A.; Burke, J.P.; Huskins, W.C.; Paterson, D.L.; Fishman, N.O.; Carpenter, C.F.; et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America Guidelines for Developing an Institutional Program to Enhance Antimicrobial Stewardship. Clin. Infect. Dis. 2007, 44, 159–177. [Google Scholar]
- Hecker, M.T.; Aron, D.C.; Patel, N.P.; Lehmann, M.K.; Donskey, C.J. Unnecessary Use of Antimicrobials in Hospitalized Patients. Arch. Intern. Med. 2003, 163, 972–978. [Google Scholar] [CrossRef]
- Messacar, K.; Gaensbauer, J.T.; Birkholz, M.; Palmer, C.; Todd, J.K.; Tyler, K.L.; Dominguez, S.R. Impact of FilmArray meningitis encephalitis panel on HSV testing and empiric acyclovir use in children beyond the neonatal period. Diagn. Microbiol. Infect. Dis. 2020, 97, 115085. [Google Scholar] [CrossRef]
- Samuel, L. Point-of-Care Testing in Microbiology. Clin. Lab. Med. 2020, 40, 483–494. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- New World Bank Country Classifications by Income Level: 2021–2022. Available online: https://blogs.worldbank.org/opendata/new-world-bank-country-classifications-income-level-2021-2022 (accessed on 22 February 2022).
- Nitsch-Osuch, A.; Kuchar, E.; Gołębiak, I.; Kanecki, K.; Tarka, P.; Brydak, L.B. Rapid influenza diagnostic tests improve suitability of antiviral treatment in hospitalized children. Adv. Exp. Med. Biol. 2017, 968, 1–6. [Google Scholar]
- Vecino-Ortiz, A.I.; Goldenberg, S.D.; Douthwaite, S.T.; Cheng, C.-Y.; Glover, R.E.; Mak, C.; Adams, E.J. Impact of a multiplex PCR point-of-care test for influenza A/B and respiratory syncytial virus on an acute pediatric hospital ward. Diagn. Microbiol. Infect. Dis. 2018, 91, 331–335. [Google Scholar] [CrossRef]
- Abanses, J.C.; Dowd, M.D.; Simon, S.D.; Sharma, V. Impact of rapid influenza testing at triage on management of febrile infants and young children. Pediatr. Emerg. Care 2006, 22, 145–149. [Google Scholar] [CrossRef]
- Diallo, D.; Hochart, A.; Lagree, M.; Dervaux, B.; Martinot, A.; Dubos, F. Impact of the Sofia® Influenza A+B FIA rapid diagnostic test in a pediatric emergency department. Arch. Pediatr. 2019, 26, 6–11. [Google Scholar]
- Noyola, D.E.; Demmler, G.J. Effect of rapid diagnosis on management of influenza A infections. Pediatr. Infect. Dis. J. 2000, 19, 303–307. [Google Scholar] [CrossRef]
- Özkaya, E.; Cambaz, N.; Çoşkun, Y.; Mete, F.; Geyik, M.; Samanci, N. The effect of rapid diagnostic testing for influenza on the reduction of antibiotic use in paediatric emergency department. Acta Paediatr. Int. J. Paediatr. 2009, 98, 1589–1592. [Google Scholar] [CrossRef]
- Bonner, A.B.; Monroe, K.W.; Talley, L.I.; Klasner, A.E.; Kimberlin, D.W. Impact of the Rapid Diagnosis of Influenza on Physician Decision-Making and Patient Management in the Pediatric Emergency Department: Results of a Randomized, Prospective, Controlled Trial. Pediatrics 2003, 112, 363–367. [Google Scholar] [CrossRef]
- Cantais, A.; Mory, O.; Plat, A.; Bourmaud, A.; Giraud, A.; Costille, M.; Pozzetto, B.; Pillet, S. Impact of bedside diagnosis of influenza in the paediatric emergency ward. Clin. Microbiol. Infect. 2018, 25, 898–903. [Google Scholar]
- Iyer, S.B.; Gerber, M.A.; Pomerantz, W.J.; Mortensen, J.E.; Ruddy, R.M. Effect of Point-of-care Influenza Testing on Management of Febrile Children. Acad. Emerg. Med. 2006, 13, 1259–1268. [Google Scholar]
- Jacob, R.; White, B.; McCaskill, M.E. Does location of rapid influenza diagnostic testing influence treatment time and ancillary testing in a paediatric emergency department? EMA-Emerg. Med. Australas. 2021, 33, 88–93. [Google Scholar] [CrossRef]
- Jun, S.H.; Kim, J.Y.; Yoon, Y.H.; Lim, C.S.; Ch, H.J.; Choi, S.H. The effect of the rapid antigen test for influenza on clinical practice in the emergency department: A comparison of periods before and after the 2009 H1N1 influenza pandemic. Signa Vitae 2016, 11, 74–89. [Google Scholar]
- Li-Kim-Moy, J.; Dastouri, F.; Rashid, H.; Khandaker, G.; Kesson, A.; McCaskill, M.; Wood, N.; Jones, C.; Zurynski, Y.; Macartney, K.; et al. Utility of early influenza diagnosis through point-of-care testing in children presenting to an emergency department. J. Paediatr. Child Health 2016, 52, 422–429. [Google Scholar]
- Sharma, V.; Dowd, M.D.; Slaughter, A.J.; Simon, S.D. Effect of rapid diagnosis of influenza virus type A on the emergency department management of febrile infants and toddlers. Arch. Pediatr. Adolesc. Med. 2002, 156, 41–43. [Google Scholar] [CrossRef][Green Version]
- Patel, P.; Laurich, V.M.; Smith, S.; Sturm, J. Point-of-care influenza testing in the pediatric emergency department. Pediatr. Emerg. Care 2020, 36, 515–518. [Google Scholar] [CrossRef]
- Pierron, S.; Haas, H.; Berlioz, M.; Ollier, L.; Albertini, M. Impact of rapid influenza test during influenza epidemic in all febrile children less than 6 years old in a pediatric emergency departmentl. Arch. Pediatr. Organe Off. Soc. Fr. Pediatr. 2008, 15, 1283–1288. [Google Scholar] [CrossRef]
- Benito-Fernández, J.; Vázquez-Ronco, M.A.; Morteruel-Aizkuren, E.; Mintegui-Raso, S.; Sánchez-Etxaniz, J.; Fernández-Landaluce, A. Impact of rapid viral testing for influenza A and B viruses on management of febrile infants without signs of focal infection. Pediatr. Infect. Dis. J. 2006, 25, 1153–1157. [Google Scholar] [CrossRef]
- Poehling, K.A.; Zhu, Y.; Tang, Y.W.; Edwards, K. Accuracy and impact of a point-of-care rapid influenza test in young children with respiratory illnesses. Arch. Pediatr. Adolesc. Med. 2006, 160, 713–718. [Google Scholar] [CrossRef]
- Jennings, L.C.; Skopnik, H.; Burckhardt, I.; Hribar, I.; del Piero, L.; Deichmann, K.A. Effect of rapid influenza testing on the clinical management of paediatric influenza. Influenza Other Respi. Viruses 2009, 3, 91–98. [Google Scholar] [CrossRef]
- Nitsch-Osuch, A.; Stefańska, I.; Kuchar, E.; Brydak, L.B.; Pirogowicz, I.; Życińska, K.; Wardyn, K. Influence of rapid influenza test on clinical management of children younger than five with febrile respiratory tract infections. Adv. Exp. Med. Biol. 2013, 755, 237–241. [Google Scholar] [PubMed]
- van Esso, D.L.; Valente, A.M.; Vilà, M.; Casanovas, J.M.; de Quixano, M.; Rodrigo, C.; Anton, A.; Pumarola, T. Rapid Influenza Testing in Infants and Children Younger than 6 Years in Primary Care: Impact on Antibiotic Treatment and Use of Health Services. Pediatr. Infect. Dis. J. 2019, 38, E187–E189. [Google Scholar] [CrossRef] [PubMed]
- Cohen, R.; Thollot, F.; Lécuyer, A.; Koskas, M.; Touitou, R.; Boucherat, M.; D’Athis, P.; Corrard, F.; Pecking, M.; de La Rocque, F. Impact des tests de diagnostic rapide en ville dans la prise en charge des enfants en période de grippe. Arch. Pediatr. 2007, 14, 926–931. [Google Scholar] [CrossRef]
- de La Rocque, F.; Lecuyer, A.; Wollner, C.; d’Athis, P.; Pecking, M.; Thollot, F.; Cohen, R. Impact des tests de diagnostic rapide de la grippe dans la prise en charge des enfants en période d’épidémie en pédiatrie de ville. Arch. Pediatr. 2009, 16, 288–293. [Google Scholar] [CrossRef]
- Keske, Ş.; Ergönül, Ö.; Tutucu, F.; Karaaslan, D.; Palaoğlu, E.; Can, F. The rapid diagnosis of viral respiratory tract infections and its impact on antimicrobial stewardship programs. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 779–783. [Google Scholar] [CrossRef]
- Kitano, T.; Nishikawa, H.; Suzuki, R.; Onaka, M.; Nishiyama, A.; Kitagawa, D.; Oka, M.; Masuo, K.; Yoshida, S. The impact analysis of a multiplex PCR respiratory panel for hospitalized pediatric respiratory infections in Japan. J. Infect. Chemother. 2019, 26, 82–85. [Google Scholar] [CrossRef]
- Lee, B.R.; Hassan, F.; Anne, M.; Selvarangan, R. Impact of multiplex molecular assay turn-around-time on antibiotic utilization and clinical management of hospitalized children with acute respiratory tract infections. J. Clin. Virol. 2018, 110, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Reischl, A.T.; Schreiner, D.; Poplawska, K.; Kidszun, A.; Zepp, F.; Gröndahl, B.; Gehring, S. The clinical impact of PCR-based point-of-care diagnostic in respiratory tract infections in children. J. Clin. Lab. Anal. 2020, 34, e23203. [Google Scholar] [CrossRef] [PubMed]
- Schulert, G.S.; Lu, Z.; Wingo, T.; Tang, Y.W.; Saville, B.R.; Hain, P.D. Role of a respiratory viral panel in the clinical management of pediatric inpatients. Pediatr. Infect. Dis. J. 2013, 32, 467–472. [Google Scholar] [CrossRef] [PubMed]
- Subramony, A.; Zachariah, P.; Krones, A.; Whittier, S.; Saiman, L. Impact of multiplex polymerase chain reaction testing for respiratory pathogens on healthcare resource utilization for pediatric inpatients. J. Pediatr. 2016, 173, 196–201.e2. [Google Scholar] [CrossRef] [PubMed]
- Walls, T.; Stark, E.; Pattemore, P.; Jennings, L. Missed opportunities for antimicrobial stewardship in pre-school children admitted to hospital with lower respiratory tract infection. J. Paediatr. Child Health 2017, 53, 569–571. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Hatachi, T.; Okamoto, Y.; Aoki, Y.; Kyogoku, M.; Miyashita, K.M.; Inata, Y.; Shimizu, Y.; Fujiwara, F.; Takeuchi, M. Application of Multiplex Polymerase Chain Reaction for Pathogen Identification and Antibiotic Use in Children With Respiratory Infections in a PICU. Pediatr. Crit. Care Med. 2021, 22, e644–e648. [Google Scholar] [CrossRef]
- McCulloh, R.J.; Andrea, S.; Reinert, S.; Chapin, K. Potential utility of multiplex amplification respiratory viral panel testing in the management of acute respiratory infection in children: A retrospective analysis. J. Pediatr. Infect. Dis. Soc. 2014, 3, 146–153. [Google Scholar] [CrossRef]
- McFall, C.; Salimnia, H.; Lephart, P.; Thomas, R.; McGrath, E. Impact of Early Multiplex FilmArray Respiratory Pathogen Panel (RPP) Assay on Hospital Length of Stay in Pediatric Patients Younger Than 3 Months Admitted for Fever or Sepsis Workup. Clin. Pediatr. 2018, 57, 1224–1226. [Google Scholar] [CrossRef]
- Tam, P.Y.I.; Zhang, L.; Cohen, Z. Impact of a transition from respiratory virus shell vial to multiplex PCR on clinical outcomes and cost in hospitalized children. Children 2017, 4, 3. [Google Scholar]
- Kim, Y.K.; Lee, J.H.; Kim, S.Y.; Ahn, J.Y.; Choi, K.H.; Lee, Y.H.; Jang, K.M.; Hau, Y.S.; Lee, J.M. Rapid Molecular Tests for Detecting Respiratory Pathogens Reduced the Use of Antibiotics in Children. Antibiotics 2021, 10, 283. [Google Scholar] [CrossRef] [PubMed]
- Rogers, B.B.; Shankar, P.; Jerris, R.C.; Kotzbauer, D.; Anderson, E.J.; Watson, J.R.; O’Brien, L.A.; Uwindatwa, F.; McNamara, K.; Bost, J.E. Impact of a Rapid Respiratory Panel Test on Patient Outcomes. Arch. Pathol. Lab. Med. 2014, 139, 636–641. [Google Scholar] [CrossRef] [PubMed]
- Busson, L.; Bartiaux, M.; Brahim, S.; Konopnicki, D.; Dauby, N.; Gérard, M. Contribution of the FilmArray Respiratory Panel in the management of adult and pediatric patients attending the emergency room during 2015–2016 influenza epidemics: An interventional study. Int. J. Infect. Dis. 2019, 83, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Byington, C.L.; Castillo, H.; Gerber, K.; Daly, J.A.; Brimley, L.A.; Adams, S.; Christenson, J.C.; Pavia, A.T. The Effect of Rapid Respiratory Viral Diagnostic Testing on Antibiotic Use in a Children’s Hospital. Arch. Pediatr. Adolesc. Med. 2002, 156, 1230–1234. [Google Scholar] [CrossRef] [PubMed]
- Crook, J.; Xu, M.; Slaughter, J.C.; Willis, J.; Browning, W.; Estrada, C.; Gay, J.; Thomas, G.; Benton, A.; Quinn, C.; et al. Impact of clinical guidance and rapid molecular pathogen detection on evaluation and outcomes of febrile or hypothermic infants. Infect. Control Hosp. Epidemiol. 2020, 41, 1285–1291. [Google Scholar] [CrossRef]
- Dimopoulou, D.; Vourli, S.; Douros, K.; Pournaras, S.; Papaevangelou, V. Use of point-of-care molecular tests reduces hospitalization and oseltamivir administration in children presenting with influenza-like illness. J. Med. Virol. 2021, 93, 3944–3948. [Google Scholar] [CrossRef]
- Rao, S.; Lamb, M.M.; Moss, A.; Mistry, R.D.; Grice, K.; Ahmed, W.; Santos-Cantu, D.; Kitchen, E.; Patel, C.; Ferrari, I. Effect of Rapid Respiratory Virus Testing on Antibiotic Prescribing among Children Presenting to the Emergency Department with Acute Respiratory Illness: A Randomized Clinical Trial. JAMA Netw. Open 2021, 4, e2111836. [Google Scholar] [CrossRef]
- Echavarría, M.; Marcone, D.; Querci, M.; Seoane, A.; Ypas, M.; Videla, C.; O’Farrell, C.; Vidaurreta, S.; Ekstrom, J.; Carballal, G. Clinical impact of rapid molecular detection of respiratory pathogens in patients with acute respiratory infection. J. Clin. Virol. 2018, 108, 90–95. [Google Scholar] [CrossRef]
- May, L.; Tatro, G.; Poltavskiy, E.; Mooso, B.; Hon, S.; Bang, H.; Polage, C. Rapid Multiplex Testing for Upper Respiratory Pathogens in the Emergency Department: A Randomized Controlled Trial. Open Forum Infect. Dis. 2019, 6, ofz481. [Google Scholar] [CrossRef]
- Wishaupt, J.O.; Russcher, A.; Smeets, L.C.; Versteegh, F.G.A.; Hartwig, N.G. Clinical Impact of RT-PCR for Pediatric Acute Respiratory Infections: A Controlled Clinical Trial. Pediatrics 2011, 128, e1113–e1120. [Google Scholar] [CrossRef]
- Beal, S.G.; Posa, M.; Gaffar, M.; Reppucci, J.; Mack, J.A.; Gurka, M.J.; Rand, K.; Houck, H.; Kelly, M.N. Performance and Impact of a CLIA-waived, Point-of-care Respiratory PCR Panel in a Pediatric Clinic. Pediatr. Infect. Dis. J. 2020, 39, 188–191. [Google Scholar] [CrossRef]
- Thibeault, R.; Gilca, R.; Côté, S.; de Serres, G.; Boivin, G.; Déry, E.P. Antibiotic use in children is not influenced by the result of rapid antigen detection test for the respiratory syncytial virus. J. Clin. Virol. 2007, 39, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Schnell, J.; Schroeder, L.; Sinclair, K.; Patel, L.; Dowd, D. The Effect of Early Knowledge of Respiratory Syncytial Virus Positivity on Medical Decision Making and Throughput Time within the Pediatric Emergency Department. Pediatr. Emerg. Care 2020, 36, 134–137. [Google Scholar] [CrossRef] [PubMed]
- O’Callaghan, K.; Jones, K. Rapid testing for respiratory viruses: Impact on antibiotic use and time to patient discharge. Infect. Dis. Health 2019, 24, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, S.L.; Chang, Y.C.; Feemster, K.; Cárdenas, A.M. Implementation of a rapid influenza A/B and RSV direct molecular assay improves emergency department oseltamivir use in paediatric patients. J. Med. Microbiol. 2018, 67, 358–363. [Google Scholar] [CrossRef]
- Schneider, U.V.; Holm MK, A.; Bang, D.; Petersen, R.F.; Mortensen, S.; Trebbien, R.; Lisby, J.G. Point-of-care tests for influenza A and B viruses and RSV in emergency departments-indications, impact on patient management and possible gains by syndromic respiratory testing, Capital Region, Denmark, 2018. Eurosurveillance 2020, 25, 1900430. [Google Scholar]
- Hayashi, D.; Akashi, Y.; Suzuki, H.; Shiigai, M.; Kanemoto, K.; Notake, S.; Ishiodori, T.; Ishikawa, H.; Imai, H. Implementation of Point-of-Care Molecular Diagnostics for Mycoplasma pneumoniae Ensures the Correct Antimicrobial Prescription for Pediatric Pneumonia Patients. Tohoku J. Exp. Med. 2018, 246, 225–231. [Google Scholar] [CrossRef]
- Ayanruoh, S.; Waseem, M.; Quee, F.; Humphrey, A.; Reynolds, T. Impact of rapid streptococcal test on antibiotic use in a pediatric emergency department. Pediatr. Emerg. Care 2009, 25, 748–750. [Google Scholar] [CrossRef]
- Bird, C.; Winzor, G.; Lemon, K.; Moffat, A.; Newton, T.; Gray, J. A Pragmatic Study to Evaluate the Use of a Rapid Diagnostic Test to Detect Group A Streptococcal Pharyngitis in Children with the Aim of Reducing Antibiotic Use in a UK Emergency Department. Pediatr. Emerg. Care 2021, 37, E249–E251. [Google Scholar] [CrossRef]
- Halverson, K.A.; Milner, D. Implementation of Point-of-Care Testing in the Emergency Department. Point Care J. Near-Patient Test. Technol. 2011, 10, 116–119. [Google Scholar] [CrossRef]
- Kose, E.; Kose, S.S.; Akca, D.; Yildiz, K.; Elmas, C.; Baris, M.; Anil, M. The Effect of Rapid Antigen Detection Test on Antibiotic Prescription Decision of Clinicians and Reducing Antibiotic Costs in Children with Acute Pharyngitis. J. Trop. Pediatr. 2016, 62, 308–315. [Google Scholar] [CrossRef][Green Version]
- Małecki, M.; Mazur, A.; Sobolewski, M.; Binkowska-Bury, M.; Marć, M.; Januszewicz, P. Rapid strip tests as a decision-making tool about antibiotic treatment in children–A prospective study. Pediatr. Polska 2017, 92, 149–155. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Tsagris, V.; Antoniadou, A.; Galani, L.; Douros, C.; Katsarolis, I.; Maragos, A.; Raftopoulos, V.; Biskini, P.; Kanellakopoulou, K.; et al. Evaluation of a rapid antigen detection test in the diagnosis of streptococcal pharyngitis in children and its impact on antibiotic prescription. J. Antimicrob. Chemother. 2008, 62, 1407–1412. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Rao, A.; Berg, B.; Quezada, T.; Fader, R.; Walker, K.; Tang, S.; Cowen, U.; Duncan, D.; Sickler, J. Diagnosis and antibiotic treatment of group a streptococcal pharyngitis in children in a primary care setting: Impact of point-of-care polymerase chain reaction. BMC Pediatr. 2019, 19, 24. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, K.V. Advances in Diagnostic Testing that Impact Infection Prevention and Antimicrobial Stewardship Programs. Curr. Infect. Dis. Rep. 2019, 21, 6. [Google Scholar] [CrossRef]
- Martínez-González, N.A.; Keizer, E.; Plate, A.; Coenen, S.; Valeri, F.; Verbakel, J.Y.J.; Rosemann, T.; Neuner-Jehle, S.; Senn, O. Point-of-care c-reactive protein testing to reduce antibiotic prescribing for respiratory tract infections in primary care: Systematic review and meta-analysis of randomised controlled trials. Antibiotics 2020, 9, 610. [Google Scholar] [CrossRef]
- Lippi, G.; Nocini, R.; Mattiuzzi, C.; Henry, B.M. FebriDx for rapid screening of patients with suspected COVID-19 upon hospital admission: Systematic literature review and meta-analysis. J. Hosp. Infect. 2022, 123, 61–66. [Google Scholar] [CrossRef]
- Egilmezer, E.; Walker, G.J.; Bakthavathsalam, P.; Peterson, J.R.; Gooding, J.J.; Rawlinson, W.; Stelzer-Braid, S. Systematic review of the impact of point-of-care testing for influenza on the outcomes of patients with acute respiratory tract infection. Rev. Med Virol. 2018, 28, e1995. [Google Scholar] [CrossRef]
- Marrie, T.J.; Lau, C.Y.; Wheeler, S.L.; Wong, C.J.; Vandervoort, M.K.; Feagan, B.G. A controlled trial of a critical pathway for treatment of community-acquired pneumonia. CAPITAL Study Investigators. Community-Acquired Pneumonia Intervention Trial Assessing Levofloxacin. JAMA 2000, 283, 749–755. [Google Scholar] [CrossRef]
- Asiimwe, C.; Kyabayinze, D.; Kyalisiima, Z.; Nabakooza, J.; Bajabaite, M.; Counihan, H.; Tibenderana, J.K. Early experiences on the feasibility, acceptability, and use of malaria rapid diagnostic tests at peripheral health centres in Uganda-insights into some barriers and facilitators. Implement. Sci. 2012, 7, 5. [Google Scholar] [CrossRef]
- Schito, M.; Peter, T.F.; Cavanaugh, S.; Piatek, A.S.; Young, G.J.; Alexander, H.; Coggin, W.; Domingo, G.; Ellenberger, D.; Ermantraut, E.; et al. Opportunities and Challenges for Cost-Efficient Implementation of New Point-of-Care Diagnostics for HIV and Tuberculosis. J. Infect. Dis. 2012, 205, S169–S180. [Google Scholar] [CrossRef]
- Pai, N.P.; Vadnais, C.; Denkinger, C.; Engel, N.; Pai, M. Point-of-Care Testing for Infectious Diseases: Diversity, Complexity, and Barriers in Low- and Middle-Income Countries. PLoS Med. 2012, 9, e1001306. [Google Scholar] [CrossRef] [PubMed]
- Uyeki, T.M.; Bernstein, H.H.; Bradley, J.S.; Englund, J.A.; File, T.M., Jr.; Fry, A.M.; Gravenstein, S.; Hayden, F.G.; Harper, S.A.; Hirshon, J.M.; et al. Clinical Practice Guidelines by the Infectious Diseases Society of America: 2018 Update on Diagnosis, Treatment, Chemoprophylaxis, and Institutional Outbreak Management of Seasonal Influenza. Clin. Infect. Dis. IDSA Guidel. 2019, 30, 97–98. [Google Scholar]
- Tse, J.; Near, A.M.; Cheng, M.; Karichu, J.; Lee, B.; Chang, S.N. Outpatient Antibiotic and Antiviral Utilization Patterns in Patients Tested for Respiratory Pathogens in the United States: A Real-World Database Study. Antibiotics 2022, 11, 1058. [Google Scholar] [CrossRef] [PubMed]
- Cheysson, F.; Brun-Buisson, C.; Opatowski, L.; Le Fouler, L.; Caserio-Schönemann, C.; Pontais, I.; Guillemot, D.; Watier, L. Outpatient antibiotic use attributable to viral acute lower respiratory tract infections during the cold season in France, 2010–2017. Int. J. Antimicrob. Agents 2021, 57, 106339. [Google Scholar] [CrossRef]
- Thompson, P.L.; Spyridis, N.; Sharland, M.; Gilbert, R.; Saxena, S.; Long, P.; Johnson, A.P.; Wong, I.C.K. Changes in clinical indications for community antibiotic prescribing for children in the UK from 1996 to 2006: Will the new NICE prescribing guidance on upper respiratory tract infections just be ignored? Arch. Dis. Child. 2009, 94, 337–340. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, T.; Malcolm, W.; McMenamin, J.; Reynolds, A.; Guttmann, A.; Hardelid, P. Community-Based Antibiotic Prescribing Attributable to Respiratory Syncytial Virus and Other Common Respiratory Viruses in Young Children: A Population-Based Time-series Study of Scottish Children. Clin. Infect. Dis. 2021, 72, 2144–2153. [Google Scholar] [PubMed]
- Harris, M.; Clark, J.; Coote, N.; Fletcher, P.; Harnden, A.; Mckean, M.; Thomson, A.; on behalf of British Thoracic Society Standards of Care Committee. British Thoracic Society guidelines for the management of community acquired pneumonia in children: Update 2011. Thorax 2011, 66 (Suppl. S2), ii1–ii23. [Google Scholar] [CrossRef]
- Gonzalez-Gonzalez, C.; López-Vázquez, P.M.; Vazquez-Lago, J.; Piñeiro-Lamas, M.; Herdeiro, M.T.; Arzamendi, P.C.; Figueiras, A.; GREPHEPI Group. Effect of Physicians’ Attitudes and Knowledge on the Quality of Antibiotic Prescription: A Cohort Study. PLoS ONE 2015, 10, e0141820. [Google Scholar]
- Borg, M.A.; Camilleri, L. Broad-spectrum antibiotic use in Europe: More evidence of cultural influences on prescribing behaviour. J. Antimicrob. Chemother. 2019, 74, 3379–3383. [Google Scholar] [CrossRef]
- Zeitler, K.; Narayanan, N. The Present and Future State of Antimicrobial Stewardship and Rapid Diagnostic Testing: Can One Ideally Succeed Without the Other? Curr. Treat. Options Infect. Dis. 2019, 11, 177–187. [Google Scholar] [CrossRef]
- Machowska, A.; Lundborg, C.S. Drivers of irrational use of antibiotics in Europe. Int. J. Environ. Res. Public Health 2019, 16, 27. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- NIH Tool for Bias Assessment. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 3 February 2022).
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Cochran, W.G. The Combination of Estimates from Different Experiments. Biometrics 1954, 10, 101–129. [Google Scholar] [CrossRef]
- Der Simonian, N.; Lair, R. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brigadoi, G.; Gastaldi, A.; Moi, M.; Barbieri, E.; Rossin, S.; Biffi, A.; Cantarutti, A.; Giaquinto, C.; Da Dalt, L.; Donà, D. Point-of-Care and Rapid Tests for the Etiological Diagnosis of Respiratory Tract Infections in Children: A Systematic Review and Meta-Analysis. Antibiotics 2022, 11, 1192. https://doi.org/10.3390/antibiotics11091192
Brigadoi G, Gastaldi A, Moi M, Barbieri E, Rossin S, Biffi A, Cantarutti A, Giaquinto C, Da Dalt L, Donà D. Point-of-Care and Rapid Tests for the Etiological Diagnosis of Respiratory Tract Infections in Children: A Systematic Review and Meta-Analysis. Antibiotics. 2022; 11(9):1192. https://doi.org/10.3390/antibiotics11091192
Chicago/Turabian StyleBrigadoi, Giulia, Andrea Gastaldi, Marco Moi, Elisa Barbieri, Sara Rossin, Annalisa Biffi, Anna Cantarutti, Carlo Giaquinto, Liviana Da Dalt, and Daniele Donà. 2022. "Point-of-Care and Rapid Tests for the Etiological Diagnosis of Respiratory Tract Infections in Children: A Systematic Review and Meta-Analysis" Antibiotics 11, no. 9: 1192. https://doi.org/10.3390/antibiotics11091192
APA StyleBrigadoi, G., Gastaldi, A., Moi, M., Barbieri, E., Rossin, S., Biffi, A., Cantarutti, A., Giaquinto, C., Da Dalt, L., & Donà, D. (2022). Point-of-Care and Rapid Tests for the Etiological Diagnosis of Respiratory Tract Infections in Children: A Systematic Review and Meta-Analysis. Antibiotics, 11(9), 1192. https://doi.org/10.3390/antibiotics11091192