
Against the Norm: Do Not Rely on Serum C-Reactive Protein and White Blood Cell Count Only When Assessing Eradication of Periprosthetic Joint Infection

 ,
,  ,
,
Abstract
:1. Introduction
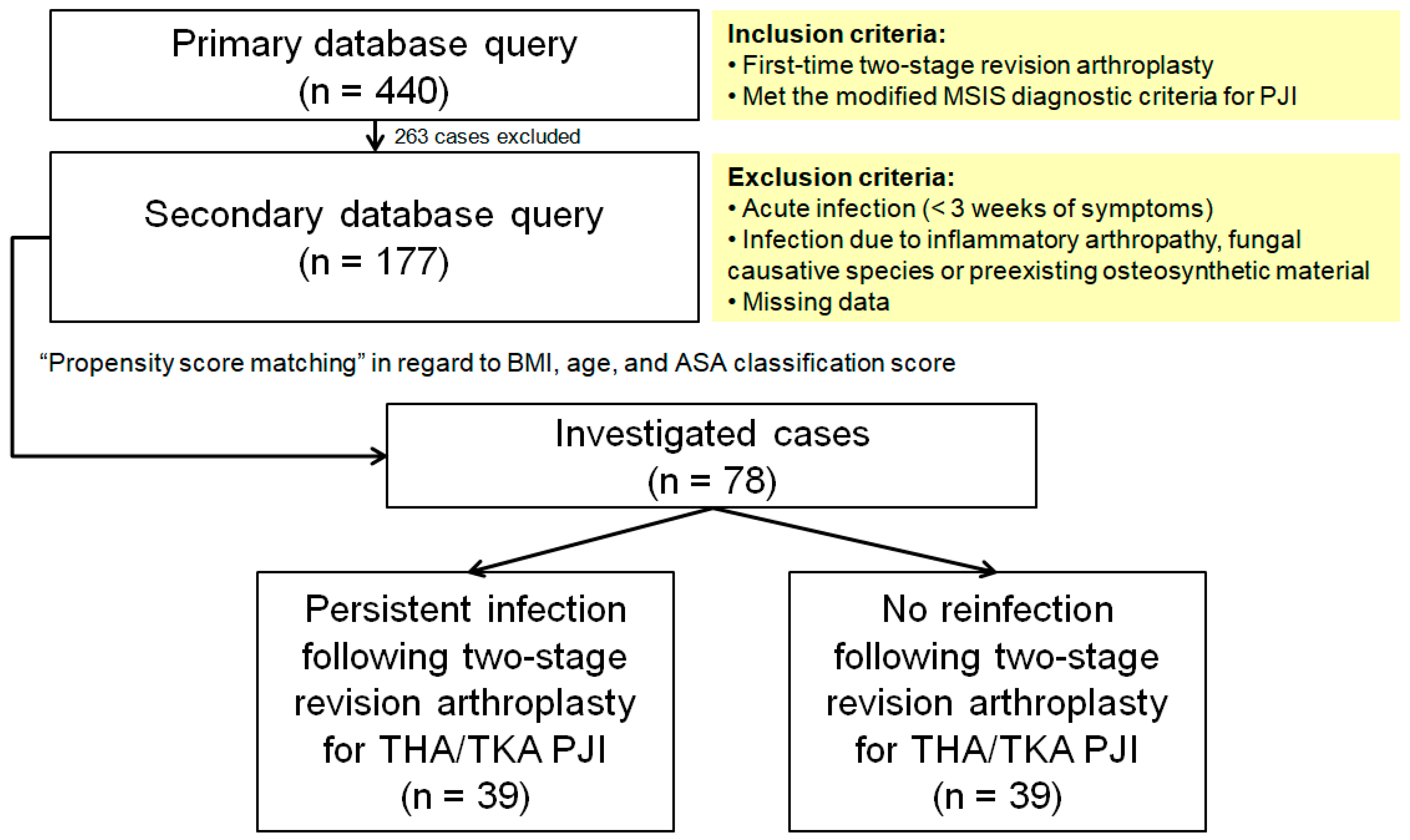
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| PJI | Periprosthetic infections |
| DAIR | Debridement, antibiotics and implant retention |
| CRP | C-reactive protein |
| WBC | White blood cell count |
| ESR | Erythrocyte sedimentation rate |
| BMI | Body mass index |
| ASA | American Society of Anesthesiologists |
| AAOS | American Academy of Orthopaedic Surgeons |
| PMMA | Polymethylmethacrylate |
| MSIS | Musculoskeletal Infection Society |
| 95% CI | 95% confidence interval |
| IQR | Interquartile range |
| SD | Standard deviation |
| ROC | Receiver operator curve |
| AUC | Area under curve |
References
- Kurtz, S.M.; Lau, E.; Watson, H.; Schmier, J.K.; Parvizi, J. Economic burden of periprosthetic joint infection in the United States. J. Arthroplast. 2012, 27, 61–65.e1. [Google Scholar] [CrossRef] [PubMed]
- Lentino, J.R. Prosthetic joint infections: Bane of orthopedists, challenge for infectious disease specialists. Clin. Infect. Dis. 2003, 36, 1157–1161. [Google Scholar] [CrossRef] [PubMed]
- Ong, K.L.; Kurtz, S.M.; Lau, E.; Bozic, K.J.; Berry, D.J.; Parvizi, J. Prosthetic joint infection risk after total hip arthroplasty in the Medicare population. J. Arthroplast. 2009, 24, 105–109. [Google Scholar] [CrossRef]
- Klouche, S.; Sariali, E.; Mamoudy, P. Total hip arthroplasty revision due to infection: A cost analysis approach. Orthop. Traumatol. Surg. Res. 2010, 96, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Parvizi, J.; Della Valle, C.J. AAOS Clinical Practice Guideline: Diagnosis and treatment of periprosthetic joint infections of the hip and knee. J. Am. Acad. Orthop. Surg. 2010, 18, 771–772. [Google Scholar] [CrossRef]
- Faschingbauer, M.; Kappe, T.; Trubrich, A.; Bieger, R.; Reichel, H. Retention of the prosthesis in early periprosthetic infection after total hip arthroplasty. Z. Fur Orthop. Und Unf. 2015, 153, 192–197. [Google Scholar] [CrossRef]
- Choi, H.R.; Von Knoch, F.; Zurakowski, D.; Nelson, S.B.; Malchau, H. Can implant retention be recommended for treatment of infected TKA? Clin. Orthop. Relat. Res. 2011, 469, 961–969. [Google Scholar] [CrossRef]
- Azzam, K.A.; Seeley, M.; Ghanem, E.; Austin, M.S.; Purtill, J.J.; Parvizi, J. Irrigation and debridement in the management of prosthetic joint infection: Traditional indications revisited. J. Arthroplast. 2010, 25, 1022–1027. [Google Scholar] [CrossRef]
- Haddad, F.S.; Sukeik, M.; Alazzawi, S. Is single-stage revision according to a strict protocol effective in treatment of chronic knee arthroplasty infections? Clin. Orthop. Relat. Res. 2015, 473, 8–14. [Google Scholar] [CrossRef]
- Kendoff, D.; Gehrke, T. Surgical management of periprosthetic joint infection: One-stage exchange. J. Knee Surg. 2014, 27, 273–278. [Google Scholar] [CrossRef]
- Gehrke, T.; Kendoff, D. Peri-prosthetic hip infections: In favour of one-stage. HIP Int. 2012, 22, 40–45. [Google Scholar] [CrossRef]
- Van Thiel, G.S.; Berend, K.R.; Klein, G.R.; Gordon, A.C.; Lombardi, A.V.; Della Valle, C.J. Intraoperative molds to create an articulating spacer for the infected knee arthroplasty. Clin. Orthop. Relat. Res. 2011, 469, 994–1001. [Google Scholar] [CrossRef]
- Freeman, M.G.; Fehring, T.K.; Odum, S.M.; Fehring, K.; Griffin, W.L.; Mason, J.B. Functional advantage of articulating versus static spacers in 2-stage revision for total knee arthroplasty infection. J. Arthroplast. 2007, 22, 1116–1121. [Google Scholar] [CrossRef]
- Fehring, T.K.; Odum, S.; Calton, T.F.; Mason, J.B. Articulating versus static spacers in revision total knee arthroplasty for sepsis. The Ranawat Award. Clin. Orthop. Relat. Res. 2000, 380, 9–16. [Google Scholar] [CrossRef]
- Izakovicova, P.; Borens, O.; Trampuz, A. Periprosthetic joint infection: Current concepts and outlook. EFORT Open Rev. 2019, 4, 482–494. [Google Scholar] [CrossRef]
- Kraay, M.J.; Goldberg, V.M.; Fitzgerald, S.J.; Salata, M.J. Cementless two-staged total hip arthroplasty for deep periprosthetic infection. Clin. Orthop. Relat. Res. 2005, 441, 243–249. [Google Scholar] [CrossRef]
- Burnett, R.S.; Kelly, M.A.; Hanssen, A.D.; Barrack, R.L. Technique and timing of two-stage exchange for infection in TKA. Clin. Orthop. Relat. Res. 2007, 464, 164–178. [Google Scholar] [CrossRef]
- Mont, M.A.; Waldman, B.J.; Hungerford, D.S. Evaluation of preoperative cultures before second-stage reimplantation of a total knee prosthesis complicated by infection. A comparison-group study. J. Bone Jt. Surg. Am. 2000, 82, 1552–1557. [Google Scholar] [CrossRef]
- Bian, T.; Shao, H.; Zhou, Y.; Huang, Y.; Song, Y. Tests for predicting reimplantation success of two-stage revision for periprosthetic joint infection: A systematic review and meta-analysis. Orthop. Traumatol. Surg. Res. 2018, 104, 1115–1123. [Google Scholar] [CrossRef]
- Hirakawa, K.; Stulberg, B.N.; Wilde, A.H.; Bauer, T.W.; Secic, M. Results of 2-stage reimplantation for infected total knee arthroplasty. J. Arthroplast. 1998, 13, 22–28. [Google Scholar] [CrossRef]
- Mortazavi, S.M.J.; Vegari, D.; Ho, A.; Zmistowski, B.; Parvizi, J. Two-stage exchange arthroplasty for infected total knee arthroplasty: Predictors of failure. Clin. Orthop. Relat. Res. 2011, 469, 3049–3054. [Google Scholar] [CrossRef]
- Kusuma, S.K.; Ward, J.; Jacofsky, M.; Sporer, S.M.; Della Valle, C.J. What is the role of serological testing between stages of two-stage reconstruction of the infected prosthetic knee? Clin. Orthop. Relat. Res. 2011, 469, 1002–1008. [Google Scholar] [CrossRef]
- Ghanem, E.; Azzam, K.; Seeley, M.; Joshi, A.; Parvizi, J. Staged revision for knee arthroplasty infection: What is the role of serologic tests before reimplantation? Clin. Orthop. Relat. Res. 2009, 467, 1699–1705. [Google Scholar] [CrossRef]
- Stambough, J.B.; Curtin, B.M.; Odum, S.M.; Cross, M.B.; Martin, J.R.; Fehring, T.K. Does Change in ESR and CRP Guide the Timing of Two-stage Arthroplasty Reimplantation? Clin. Orthop. Relat. Res. 2019, 477, 364–371. [Google Scholar] [CrossRef]
- Lindsay, C.P.; Olcott, C.W.; Del Gaizo, D.J. ESR and CRP are useful between stages of 2-stage revision for periprosthetic joint infection. Arthroplast. Today 2017, 3, 183–186. [Google Scholar] [CrossRef]
- Ghani, R.; Hutt, J.; Mitchell, P.; Granger, L.; Sandiford, N.A. Serial C-reactive Protein Monitoring in Prosthetic Joint Infection: A Powerful Predictor or Potentially Pointless? Cureus 2020, 12, e6967. [Google Scholar] [CrossRef]
- Shukla, S.K.; Ward, J.P.; Jacofsky, M.C.; Sporer, S.M.; Paprosky, W.G.; Della Valle, C.J. Perioperative testing for persistent sepsis following resection arthroplasty of the hip for periprosthetic infection. J. Arthroplast. 2010, 25, 87–91. [Google Scholar] [CrossRef]
- George, J.; Jawad, M.; Curtis, G.L.; Samuel, L.T.; Klika, A.K.; Barsoum, W.K.; Higuera, C.A. Utility of Serological Markers for Detecting Persistent Infection in Two-Stage Revision Arthroplasty in Patients With Inflammatory Arthritis. J. Arthroplast. 2018, 33, S205–S208. [Google Scholar] [CrossRef]
- Cha, M.S.; Cho, S.H.; Kim, D.H.; Yoon, H.K.; Cho, H.S.; Lee, D.Y.; Lee, S.H.; Hwang, S.C. Two-Stage Total Knee Arthroplasty for Prosthetic Joint Infection. Knee Surg. Relat. Res. 2015, 27, 82–89. [Google Scholar] [CrossRef]
- Parvizi, J.; Tan, T.L.; Goswami, K.; Higuera, C.; Della Valle, C.; Chen, A.F.; Shohat, N. The 2018 Definition of Periprosthetic Hip and Knee Infection: An Evidence-Based and Validated Criteria. J. Arthroplast. 2018, 33, 1309–1314. [Google Scholar] [CrossRef]
- Greidanus, N.V.; Masri, B.A.; Garbuz, D.S.; Wilson, S.D.; McAlinden, M.G.; Xu, M.; Duncan, C.P. Use of erythrocyte sedimentation rate and C-reactive protein level to diagnose infection before revision total knee arthroplasty. A prospective evaluation. J. Bone Jt. Surg. Am. 2007, 89, 1409–1416. [Google Scholar] [CrossRef]
- Spangehl, M.J.; Masri, B.A.; O’Connell, J.X.; Duncan, C.P. Prospective analysis of preoperative and intraoperative investigations for the diagnosis of infection at the sites of two hundred and two revision total hip arthroplasties. J. Bone Jt. Surg. Am. 1999, 81, 672–683. [Google Scholar] [CrossRef]
- Ryu, D.J.; Kang, J.S.; Moon, K.H.; Kim, M.K.; Kwon, D.G. Clinical Characteristics of Methicillin-resistant Staphylococcus aureus Infection for Chronic Periprosthetic Hip and Knee Infection. Hip Pelvis 2014, 26, 235–242. [Google Scholar] [CrossRef]
- Aali Rezaie, A.; Goswami, K.; Shohat, N.; Tokarski, A.T.; White, A.E.; Parvizi, J. Time to Reimplantation: Waiting Longer Confers No Added Benefit. J. Arthroplast. 2018, 33, 1850–1854. [Google Scholar] [CrossRef]
- Fu, J.; Ni, M.; Li, H.; Li, X.; Chai, W.; Zhou, Y.; Hao, L.; Chen, J. The proper timing of second-stage revision in treating periprosthetic knee infection: Reliable indicators and risk factors. J. Orthop. Surg. Res. 2018, 13, 214. [Google Scholar] [CrossRef]
- Nelson, C.L.; Jones, R.B.; Wingert, N.C.; Foltzer, M.; Bowen, T.R. Sonication of antibiotic spacers predicts failure during two-stage revision for prosthetic knee and hip infections. Clin. Orthop. Relat. Res. 2014, 472, 2208–2214. [Google Scholar] [CrossRef] [PubMed]
- Mariconda, M.; Ascione, T.; Balato, G.; Rotondo, R.; Smeraglia, F.; Costa, G.G.; Conte, M. Sonication of antibiotic-loaded cement spacers in a two-stage revision protocol for infected joint arthroplasty. BMC Musculoskelet. Disord. 2013, 14, 193. [Google Scholar] [CrossRef]
- Lonner, J.H.; Siliski, J.M.; Della Valle, C.; DiCesare, P.; Lotke, P.A. Role of knee aspiration after resection of the infected total knee arthroplasty. Am. J. Orthop. 2001, 30, 305–309. [Google Scholar]
- Boelch, S.P.; Roth, M.; Arnholdt, J.; Rudert, M.; Luedemann, M. Synovial Fluid Aspiration Should Not Be Routinely Performed during the Two-Stage Exchange of the Knee. BioMed Res. Int. 2018, 2018, 6720712. [Google Scholar] [CrossRef]
- Schulz, P.; Dlaska, C.E.; Perka, C.; Trampuz, A.; Renz, N. Preoperative synovial fluid culture poorly predicts the pathogen causing periprosthetic joint infection. Infection 2020, 49, 427–436. [Google Scholar] [CrossRef]
- McPherson, E.J.; Woodson, C.; Holtom, P.; Roidis, N.; Shufelt, C.; Patzakis, M. Periprosthetic total hip infection: Outcomes using a staging system. Clin. Orthop. Relat. Res. 2002, 403, 8–15. [Google Scholar] [CrossRef]
- Cierny, G., 3rd; DiPasquale, D. Periprosthetic total joint infections: Staging, treatment, and outcomes. Clin. Orthop. Relat. Res. 2002, 403, 23–28. [Google Scholar] [CrossRef]
- Peersman, G.; Laskin, R.; Davis, J.; Peterson, M. Infection in total knee replacement: A retrospective review of 6489 total knee replacements. Clin. Orthop. Relat. Res. 2001, 392, 15–23. [Google Scholar] [CrossRef]
- Pradhan, A.D.; Manson, J.E.; Rifai, N.; Buring, J.E.; Ridker, P.M. C-reactive protein, interleukin 6, and risk of developing type 2 diabetes mellitus. Jama 2001, 286, 327–334. [Google Scholar] [CrossRef]
- Goodman, S.M.; Springer, B.; Guyatt, G.; Abdel, M.P.; Dasa, V.; George, M.; Gewurz-Singer, O.; Giles, J.T.; Johnson, B.; Lee, S.; et al. 2017 American College of Rheumatology/American Association of Hip and Knee Surgeons Guideline for the Perioperative Management of Antirheumatic Medication in Patients With Rheumatic Diseases Undergoing Elective Total Hip or Total Knee Arthroplasty. J. Arthroplast. 2017, 32, 2628–2638. [Google Scholar] [CrossRef]
- Pincus, T.; Sokka, T. Laboratory tests to assess patients with rheumatoid arthritis: Advantages and limitations. Rheum. Dis. Clin. 2009, 35, 731–734. [Google Scholar] [CrossRef]
- Pulido, L.; Ghanem, E.; Joshi, A.; Purtill, J.J.; Parvizi, J. Periprosthetic joint infection: The incidence, timing, and predisposing factors. Clin. Orthop. Relat. Res. 2008, 466, 1710–1715. [Google Scholar] [CrossRef] [PubMed]
- Mittal, Y.; Fehring, T.K.; Hanssen, A.; Marculescu, C.; Odum, S.M.; Osmon, D. Two-stage reimplantation for periprosthetic knee infection involving resistant organisms. J. Bone Jt. Surg. Am. 2007, 89, 1227–1231. [Google Scholar] [CrossRef]
- Ueng, S.W.N.; Lee, C.-Y.; Hu, C.-C.; Hsieh, P.-H.; Chang, Y. What is the success of treatment of hip and knee candidal periprosthetic joint infection? Clin. Orthop. Relat. Res. 2013, 471, 3002–3009. [Google Scholar] [CrossRef]
- Westhuyzen, J.; Healy, H. Review: Biology and relevance of C-reactive protein in cardiovascular and renal disease. Ann. Clin. Lab. Sci. 2000, 30, 133–143. [Google Scholar]
- Fehring, K.A.; Abdel, M.P.; Ollivier, M.; Mabry, T.M.; Hanssen, A.D. Repeat Two-Stage Exchange Arthroplasty for Periprosthetic Knee Infection Is Dependent on Host Grade. J. Bone Jt. Surg. Am. 2017, 99, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Trampuz, A.; Hanssen, A.D.; Osmon, D.R.; Mandrekar, J.; Steckelberg, J.M.; Patel, R. Synovial fluid leukocyte count and differential for the diagnosis of prosthetic knee infection. Am. J. Med. 2004, 117, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Karczewski, D.; Winkler, T.; Renz, N.; Trampuz, A.; Lieb, E.; Perka, C.; Müller, M. A standardized interdisciplinary algorithm for the treatment of prosthetic joint infections. Bone Jt. J. 2019, 101, 132–139. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sex | Age | BMI | ASA Grade | DM | AH | PAD | RA | CAD | HF | CKD | COPD | ||
| Infection status | −0.135 | 0.047 | −0.125 | −0.019 | −0.217 | −0.127 | −0.200 | 0.000 | −0.109 | −0.104 | −0.186 | −0.224 | |
| CRP | Preexplantation | 0.173 | 0.081 | −0.036 | 0.307 | 0.274 | 0.091 | 0.074 | 0.216 | 0.006 | 0.005 | 0.318 | 0.056 |
| Prereimplantation | 0.102 | 0.063 | 0.035 | 0.295 | 0.241 | −0.152 | 0.070 | 0.116 | −0.062 | −0.051 | 0.160 | 0.129 | |
| WBC | Preexplantation | 0.185 | 0.046 | 0.120 | 0.197 | 0.123 | 0.182 | 0.110 | 0.293 | 0.138 | 0.146 | 0.270 | 0.130 |
| Prereimplantation | −0.025 | 0.009 | −0.038 | −0.037 | −0.091 | 0.033 | −0.064 | 0.374 | 0.089 | 0.056 | −0.046 | 0.131 | |
| Parameter | Status | Time Point | Mean | Minimum | Maximum | Standard Deviation |
|---|---|---|---|---|---|---|
| CRP (mg/L) | Infection-free | Preexplantation | 45.4 | 0.1 | 298.4 | 74.8 |
| Prereimplantation | 11.1 | 0.01 | 171 | 28.3 | ||
| Reinfection | Preexplantation | 18 | 0.1 | 202.3 | 37.3 | |
| Prereimplantation | 2.8 | 0.01 | 16.2 | 3.7 | ||
| WBC (109/L) | Infection-free | Preexplantation | 8.6 | 5 | 17 | 10.1 |
| Prereimplantation | 6.6 | 3.5 | 11.4 | 2.9 | ||
| Reinfection | Preexplantation | 7.5 | 3 | 13 | 5.4 | |
| Prereimplantation | 6.5 | 3.4 | 12.6 | 3.5 | ||
| Interim interval (weeks) | 13.7 | 4 | 35 | 5.3 | ||
| Infection-free | 13.6 | 5 | 35 | 4.7 | ||
| Reinfection | 13.8 | 4 | 33 | 5.6 | ||
| Parameter | Status | Median | IQR for Median | Mean | 95% CI for Mean | AUC | p-Value |
|---|---|---|---|---|---|---|---|
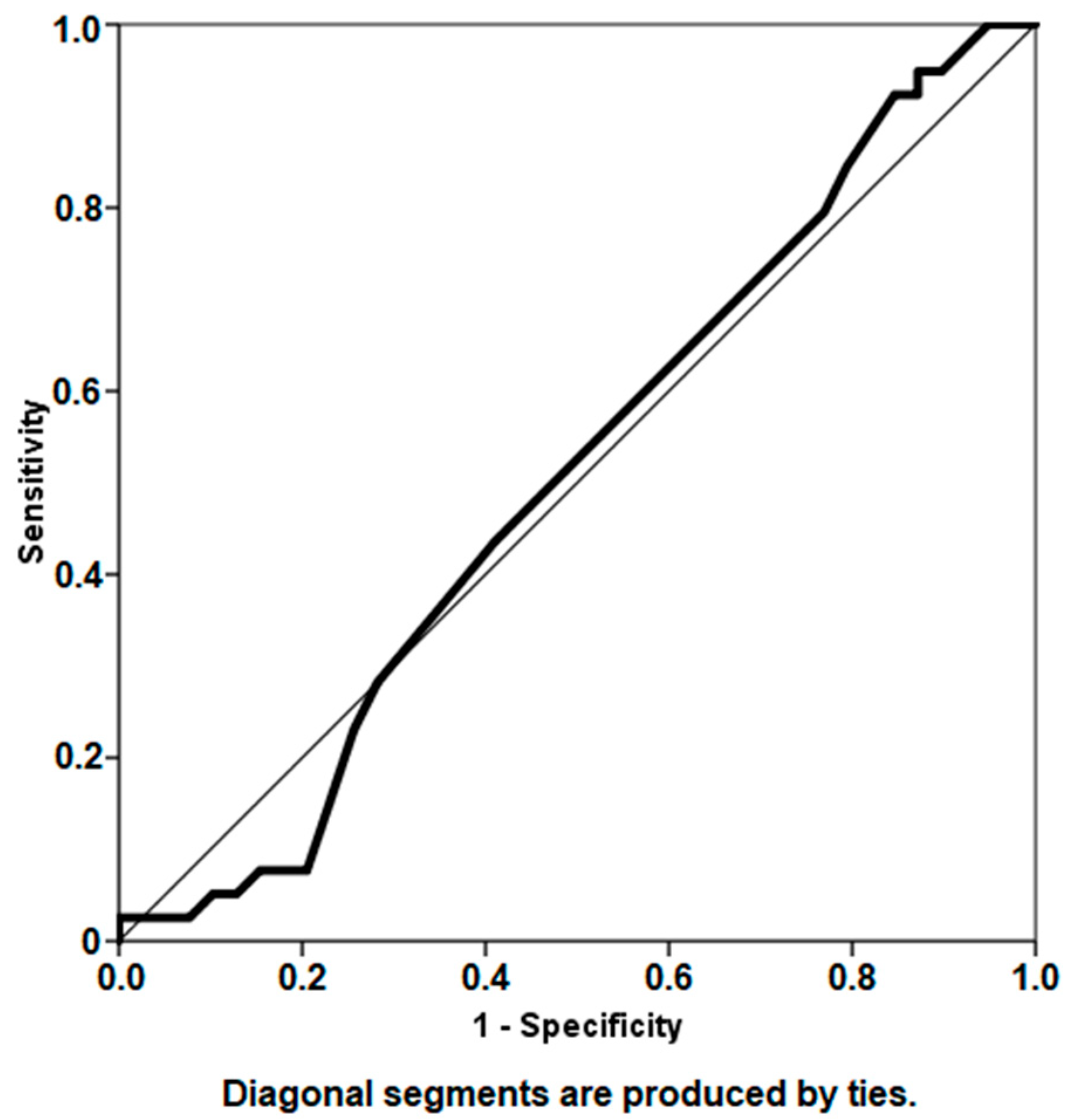
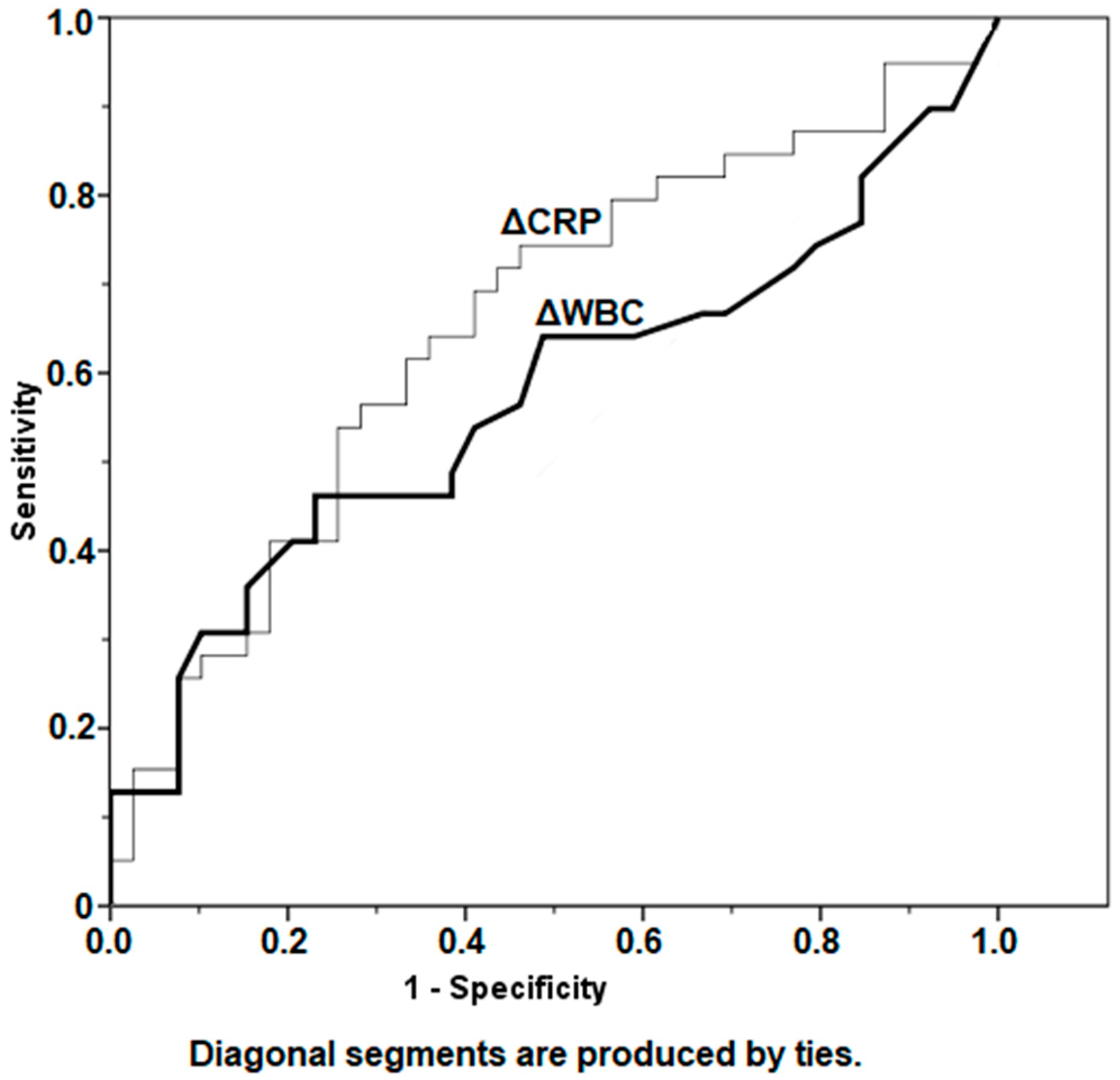
| ΔCRP (mg/L) | Infection-free | 9.48 | 2.3–36.6 | 38.1 | 16.5–59.7 | 0.654 | 0.069 |
| Reinfection | 2.74 | 1.4–14.2 | 15.5 | 3.6–27.4 | |||
| ΔWBC (109/L) | Infection-free | 1.5 | 0.6–4.0 | 2.5 | 1.7–3.3 | 0.573 | 0.072 |
| Reinfection | 1.2 | 0.8–2.2 | 1.7 | 1.2–2.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khury, F.; Oltmanns, M.; Fuchs, M.; Leiprecht, J.; Reichel, H.; Faschingbauer, M. Against the Norm: Do Not Rely on Serum C-Reactive Protein and White Blood Cell Count Only When Assessing Eradication of Periprosthetic Joint Infection. Antibiotics 2022, 11, 1174. https://doi.org/10.3390/antibiotics11091174
Khury F, Oltmanns M, Fuchs M, Leiprecht J, Reichel H, Faschingbauer M. Against the Norm: Do Not Rely on Serum C-Reactive Protein and White Blood Cell Count Only When Assessing Eradication of Periprosthetic Joint Infection. Antibiotics. 2022; 11(9):1174. https://doi.org/10.3390/antibiotics11091174
Chicago/Turabian StyleKhury, Farouk, Moritz Oltmanns, Michael Fuchs, Janina Leiprecht, Heiko Reichel, and Martin Faschingbauer. 2022. "Against the Norm: Do Not Rely on Serum C-Reactive Protein and White Blood Cell Count Only When Assessing Eradication of Periprosthetic Joint Infection" Antibiotics 11, no. 9: 1174. https://doi.org/10.3390/antibiotics11091174
APA StyleKhury, F., Oltmanns, M., Fuchs, M., Leiprecht, J., Reichel, H., & Faschingbauer, M. (2022). Against the Norm: Do Not Rely on Serum C-Reactive Protein and White Blood Cell Count Only When Assessing Eradication of Periprosthetic Joint Infection. Antibiotics, 11(9), 1174. https://doi.org/10.3390/antibiotics11091174